
Abstract
Background:
Moral distress is recognized as a problem affecting healthcare professionals globally. Unaddressed moral distress may lead to withdrawal from the moral dimensions of patient care, burnout, or leaving the profession. Despite the importance, studies related to moral distress are scant in Thailand.
Objective:
This study aims to describe the experience of moral distress and related factors among Thai nurses.
Design:
A convergent parallel mixed-methods design was used. The quantitative and qualitative data were collected in parallel using the Measure of Moral Distress for Healthcare Professionals and interview guide. The analysis was conducted separately and then integrated.
Participants:
Participants were Thai nurses from two large tertiary care institutions in a Southern province of Thailand.
Ethical considerations:
This study was approved by our organization's Institutional Review Board for Health Sciences Research, and by the Institutional Review Boards of the two local institutions in Thailand. Permission from the publisher was received to translate and utilize the Measure of Moral Distress (MMD-HP) under the license number: 4676990097151.
Results:
A total of 462 participants completed the survey questions. The top 7 causes of moral distress were related to system-level root causes and end-of-life care situations. Hierarchical multiple regression showed that work units, considering leaving position, and number of moral distress episodes in the past year were significant predictors of moral distress. Twenty interviews demonstrated three main themes of distressing causes: (1) powerlessness (at patients/family-, team-, and organizational-levels), (2) end-of-life issues, and (3) poor team function (poor communication and collaboration, incompetent healthcare providers, and inappropriate behavior of colleagues). The integration of data from both components indicated that the qualitative interviews enrich the quantitative findings, especially as related to the top 7 causes of moral distress.
Discussion:
Although the experience of moral distress among Thai nurses is similar to studies conducted elsewhere, the patient’s and family’s religious perspective that ties into the concept of moral distress needs to be explored.
Conclusions:
Although the root causes of moral distress are similar among different cultures, the experience of Thai nurses may vary according to culture and context.
Introduction
Moral distress is a global phenomenon, causing serious negative outcomes for healthcare providers and organizations. This concept was first identified among nurses as an event involving the clinician knowing or believing to know the ethically right course of action but feeling unable to pursue that course of action due to organizational and other constraints. 1 Moral distress affects the moral integrity of the agent, which distinguishes it from other concepts such as stress, emotional distress, or compassion fatigue. 2
Although initially described among critical care nurses, moral distress has also been found among medical-surgical, 3 oncology,4,5 and mental health nurses6–8 and among other healthcare providers as well.9–16 Focusing on nurses, several studies demonstrate higher levels of moral distress in critical nurses than nurses in non-critical care settings.13,14,16–19 This could be due in part to the high stress, high-stakes environment where there is high risk for patient mortality and morbidity, and daily confrontations with ethical dilemmas. 20
Common and problematic causes of moral distress occur at the patient level, unit level, and system level.2,21 Often, a morally distressing situation involves causes at two or more levels. For example, a situation in which a dying patient continues to receive painful, unnecessary treatments due to a family’s demands (patient-level cause) may also involve powerful team hierarchies that inhibit relevant input from some clinicians (team-level cause) and a lack of policy-guiding clinicians in situations of family demands for inappropriate treatment (system-level cause). Recurrent experiences of moral distress can lead to the “crescendo effect,” with buildup of moral residue and moral distress in care providers. 22 Inadequate attention to moral distress can lead to burnout or leaving a position as evidenced by several studies indicating that high levels of moral distress are associated with intention to leave a position.6,10,12,13,16,18,19,23–26
Moral distress has been studied internationally in an increasing number of non-western countries including Iran,27–29 Israel, 30 Japan,8,31 Taiwan, 32 China, 33 Korea, 34 and India 35 and African countries including Malawi, 36 South Africa, 37 and Uganda. 38 However, the literature on moral distress in Thailand is limited.
Some unique factors in Thailand create stressors for healthcare providers that could contribute to moral distress. First, the healthcare system is in transition in that there are simultaneous advances in both palliative care practice and healthcare technology.39,40 Studies by Krongyuth et al. 41 and Nilmanat 39 found that nurses and physicians perceived that they had inadequate skills and were insufficiently trained in palliative care practices. Second, in 2002, Thailand adopted a universal healthcare coverage system (UHCS), but the utilization of out-of-network services is still high, which could imply a lack of universal access to services provided under the UHCS policy. 42 Third, Thailand is a member of the Association of Southeast Asian Nations (ASEAN) economic community (AEC), established in 1967 to promote regional peace, economic growth, and collaboration in various fields such as science, economics, and technology. 43 While many outcomes of this agreement have been beneficial, some challenges are being realized such as a large influx migrant population, financial healthcare constraints, medical supply-side constraints, ongoing epidemiological transitions, and increasing workloads for healthcare providers. 44 Finally, approximately 50% of Thai nurses report high levels of burnout and 10%–60% intend to leave their job in the next 6–12 months.45,46 A plausible explanation for these concerning statistics is high levels of moral distress, yet our understanding of moral distress among Thai nurses is largely unknown.
Aims
The aims of this study were to describe the phenomenon of moral distress among Thai nurses, to investigate the relationships between moral distress and selected demographic and practice factors, and to identify predictors of moral distress.
Methods
Design
A convergent parallel mixed-methods design was used in which quantitative and qualitative data were collected in parallel, analyzed separately, and then integrated to yield a richer and more nuanced understanding of the experiences of moral distress among Thai nurses. 47 In the cross-sectional quantitative study, self-administered online questionnaires were used to assess the level of moral distress and key demographic characteristics. Concurrently, the qualitative descriptive design with semi-structured interview was conducted to explore the phenomenon of moral distress among Thai nurses in depth.
Setting and participants
Participants were Thai nurses from two large tertiary care institutions in a Southern province in Thailand. Combined, these institutions have 31 acute care units and 17 critical care units and approximately 1000 nurses in employment. The nurses were recruited based on inclusion and exclusion criteria. The inclusion criteria were the following: (1) licensed as a registered nurse (RN), (2) working on an inpatient unit, and (3) have worked in the current hospital for at least 1 year. They were excluded if they were (1) head nurse or nurse administrator, or (2) working in private units (units in which nurses do not provide direct patient care in the same way as other inpatient units). A target sample size for the quantitative aspect of the study was 200, based on the communalities and the number of strong factor loadings, the primary goal of overall study not reported here. 48
In qualitative phase, the participants who completed the online survey and are interested to participate in the interview provided their email or cell phone number, which the first author used to arrange the interview. Although the data were saturated with 15 interviews, the first author interviewed five more cases to make sure that there was no other new information.
Instruments
Two instruments, a sociodemographic questionnaire and the Measure of Moral Distress for Healthcare Professionals (MMD-HP), as well as a semi-structured interview were used.
The MMD-HP is a 27-item scale developed by Epstein et al. 13 which aims to measure moral distress among healthcare professions in any clinical setting. The MMD-HP offers five ordinal-level, Likert-type response choices scored by participants in terms of how often the situation arose in the past year (frequency: 0 = never, 4 = very frequently) and how disturbing the situation is when it arises (intensity: 0 = none, 4 = great extent). A composite score was computed by multiplying the frequency score by the disturbance score of each item, creating a new variable (“fxd”) with possible ranges of 0–16. A composite (fxd) score allows for a more accurate reflection of a participant’s experience than if either frequency or disturbance were calculated alone. For example, if a participant experiences the pressures of understaffing very frequently (4) but finds this to be not morally distressing (0), fxd = 0 because it is not morally distressing. Similarly, if a participant never experiences short staffing (0) but if he or she did it would be greatly disturbing (4), the fxd would still be 0 because it never happens. Next, an overall score was obtained by summing each item’s fxd score, with scores ranging from 0 to 432. Higher scores indicate higher levels of moral distress. The MMD-HP includes two additional categorical items about current and past intention to leave a position due to moral distress. Forward–backward translation of the English MMD-HP to Thai MMD-HP was accomplished according to an adaptation of Brislin’s translation model. 49 Thai version MMD-HP demonstrated a good instrument reliability, with Cronbach’s alpha of .94 and validity through exploratory factor analysis which will be published elsewhere.
The interview guide was developed according to the aims of this study using open-ended questions. Then the internal testing and field testing were done to confirm the coverage and relevance of the content of the formulated. Face-to-face semi-structured interviews were conducted and digitally audiotaped. The author also used verbal and non-verbal probing techniques as follow-up questions to expand on some particular point that came up during the interview. Maximum variation sampling was used to identify and expand the range of variation of moral distress experience in nurses.50,51
Procedures
An online consent form, translated MMD-HP, and demographic survey were distributed via electronic chat group (Line app) using Qualtrics, paper flyers, and study invitation cards with a quick response (QR) code linked to the study survey. One week after initial distribution, the first author sent a reminder to the Line app group. The survey was closed 1 week later. At the end of the Qualtrics survey, participants who completed the survey were invited to participate in an interview. The interviews were arranged based on email or cell phone number that they provided at the end of the survey. The written consent for qualitative interview has been waived; however, the participants have read an information sheet and understood clearly about the study.
Data analysis
Quantitative and qualitative data were analyzed separately. Quantitative data were analyzed using SPSS 23. The statistical assumptions (normality, homogeneity of variance, linearity, non-collinearity, homoscedasticity) are met. Descriptive statistics were used to evaluate demographic data, MMD-HP scores, and intention to leave. T-tests, one-way analysis of variance (ANOVA), and Pearson’s correlations were used to examine relationship variables. Predictive factors of MMD-HP scores were analyzed using hierarchical multiple regression.
For qualitative data, all interviews were transcribed verbatim and translated from Thai to English by the first author. Data analysis was conducted simultaneously with data collection. 51 Thematic analysis was conducted to describe patterns and identify themes within data using Dedoose version 8.2.14 and manual evaluation. Analysis occurred in three phases: data expansion, data limitation, and thematic integration.51,52 Data expansion consisted of open-coding interview transcripts, giving labels to concepts or ideas in the data without regard to relative importance. Data limitation involved combining codes into higher order, more abstract thematic categories and making decisions about relative salience of the categories. The most salient themes represented by the categories were conceptually defined, illustrated with data excerpts, and integrated to best achieve the aims of this study.51,52 Analytic memos were also used to help with future directions, unanswered questions, frustrations with the analysis, and insightful connections. 53
Trustworthiness of the study was accomplished across four domains as described by Lincoln and Guba. 54 Credibility or confidence in the findings was established through explicit probes to get participants’ responses with greater precision and reflexivity to eliminate researcher’s bias. Transferability was maintained by heterogeneous sampling to see the difference in experiences of the participants. Dependability or audit-ability was established throughout the analytic process, detailing decision rules and justifications via memo and reflexivity. Finally, for confirmability, the translation of transcripts was validated by a bilingual translator who had experience in qualitative research, and peer check was also conducted by the research team.
Ethical considerations
This study was approved by our organization’s Institutional Review Board (IRB) for Health Sciences Research and by the IRBs of the two local institutions in Thailand. Prior to the questionnaire and interview, all participants were informed about the purpose and procedures of the study. Interview participants provided verbal consent; the consent of survey respondents was assumed by return of survey.
Results
Quantitative results
A total of 510 participants accessed the Qualtrics survey. Four hundred sixty-two completed all the survey questions and were included in the analysis. Participant characteristics are provided in Table 1.
Participant characteristics.

SD: standard deviation; EOL: end of life.
Root causes of moral distress
The mean score for the composite, summed MMD-HP was 104.80 (SD = 65.32, range 0–369). The top 7 causes of moral were related to system-level root causes and end-of life care situations. These are the only items that demonstrated the mean score greater than 5 (Table 2).
Ranked root causes.
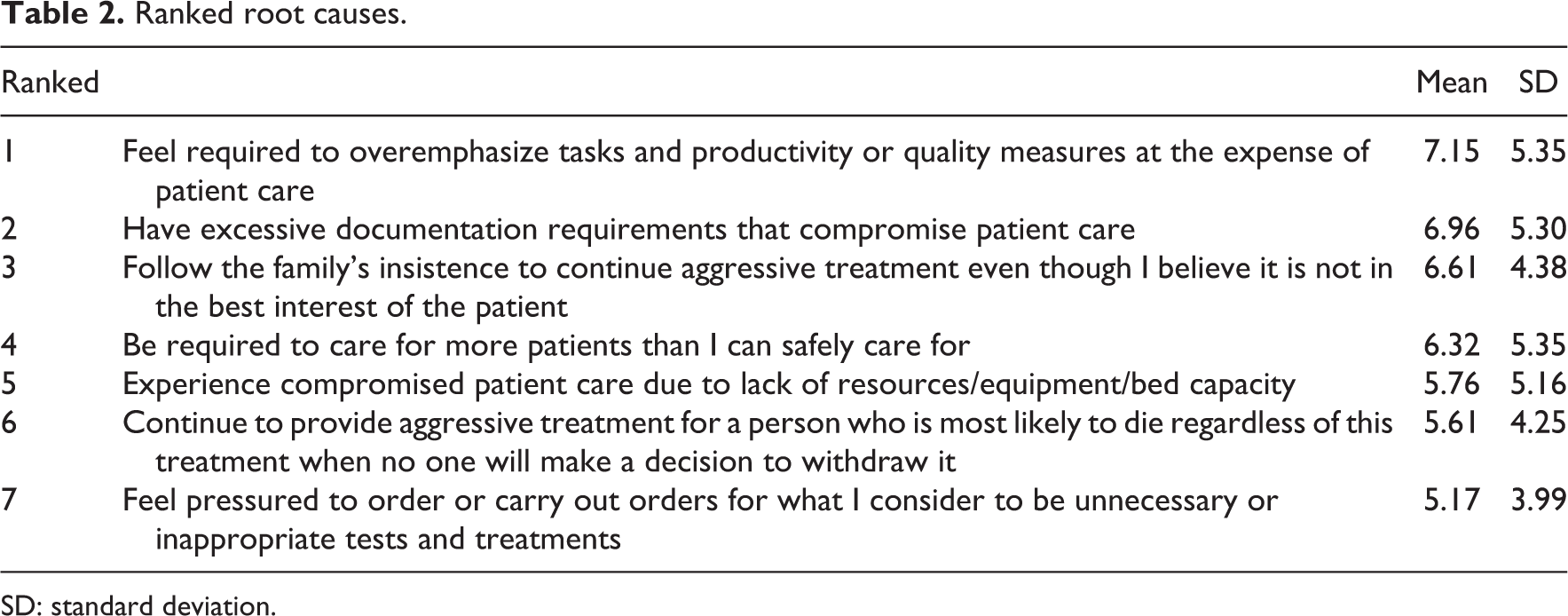
SD: standard deviation.
Moral distress and associated factors
Analysis of the relationships between MMD-HP scores and participant demographic variables indicated a non-significant difference between MMD-HP scores and age, years of working, and end-of-life training. Work unit (acute and critical care) was associated with moral distress in which acute care nurses demonstrated significantly higher moral distress scores than critical care nurses (T(460) = 2.16, p = 0.03). In addition, nurses who provided care for adult patients had significantly higher moral distress scores than those who provided care for pediatric patients (T(460) = 2.15, p = 0.03). Besides working unit, MMD-HP scores were significantly positively correlated with the number of reported moral distress episodes in the past year (r = 0.42, p < 0.001). MMD-HP scores were significantly higher for participants considering leaving their positions now due to moral distress than for those not considering leaving now (T(460) = 6.88, p < 0.001). Furthermore, those who had considered leaving the position in the past due to moral distress and either had left or had not left had significantly higher MMD-HP scores than those who had not considered leaving (Welch’s F(2, 58) = 24.35, p < 0.001).
Predictors of moral distress scores
Hierarchical multiple regression models were conducted to identify predictors of moral distress. The initial models consisted of two variables significantly associated with MMD-HP scores, namely, number of moral distress episodes in the past year and considering leaving position (Table 3). The second model included two additional variables; unit type (acute, critical care) and patient type (adult, pediatric), which were significantly associated with MMD-HP scores in this study. The last model included three demographic variables: institution, years of work experience, and end-of-life training. Among these three models, adjusted R2, root mean square error (RMSE), and incremental F-test were compared. Although the adjusted R2 and RSME were not much different among the three, the second model was chosen for interpretation due to the significance in F statistic change (F(2, 457) = 6.29, p = 0.002), which indicates that meaningful variables are included in the model.
Hierarchical multiple regression analysis predicting moral distress.
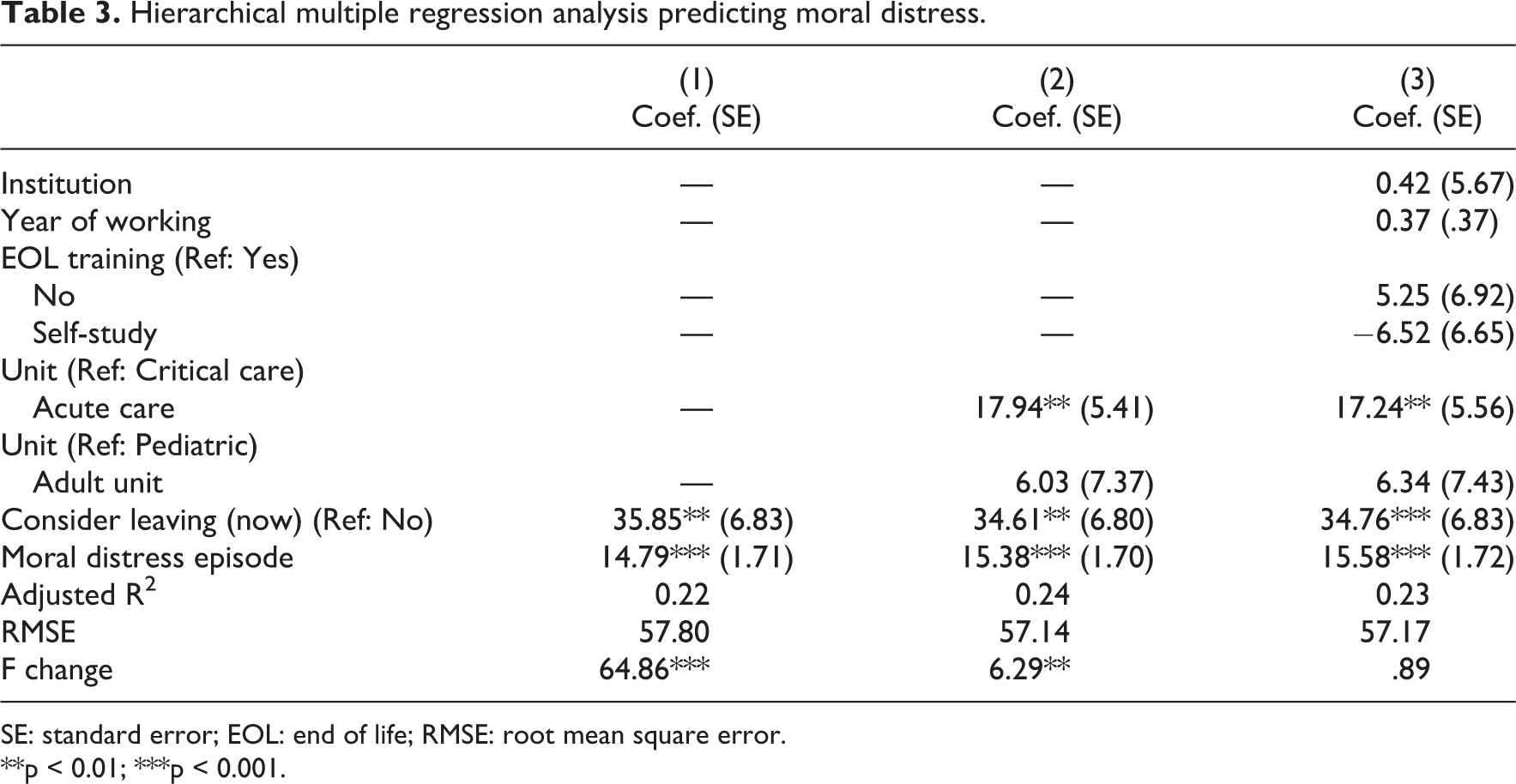
SE: standard error; EOL: end of life; RMSE: root mean square error.
**p < 0.01; ***p < 0.001.
Thus, 24% of the variance in MMD-HP scores is explained by four variables, three of which, number of moral distress episodes in the past year, considering leaving a position, and unit type (critical and acute care unit), are the significant predictors of moral distress. The result showed that an increase in one unit of number of moral distress episodes in the past year is associated with 15.38 points increase in MMD-HP score, holding the other six demographic variables. Relative to nurses who do not consider leaving position, the nurses who are considering leaving had 34.61 higher MMD-HP scores, holding other variables. The non-critical care nurses had 17.94 higher MMD-HP scores than the critical care nurses, controlling for other variables.
Qualitative results
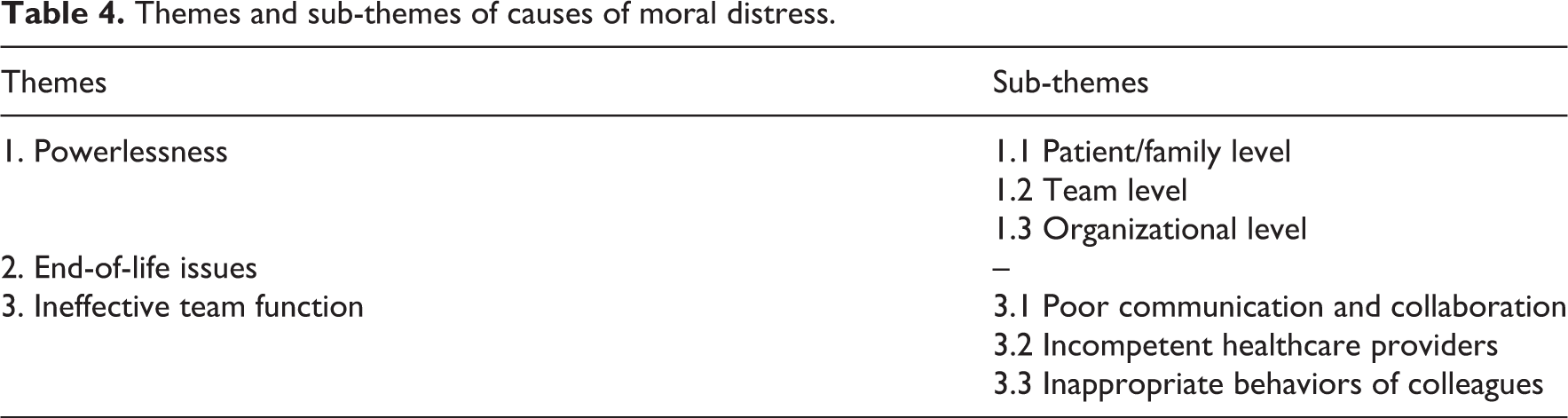
Twenty participants who completed the survey were interviewed, and these interviews were used for the thematic analysis. Eleven participants worked in critical care units and nine worked in acute care units. Participants included adult (15) and pediatric (5) nurses. Years of work experience ranged from 1 to 22 years. Three major themes regarding root causes of moral distress were identified including (1) powerlessness, (2) end-of-life issues, and (3) poor team function (Table 4). The three themes are not entirely distinct from one another. For example, several instances of powerlessness involved end-of-life situations. However, the three themes have enough differences to be described separately and they represent the three most problematic areas for this sample of Thai nurses.
Themes and sub-themes of causes of moral distress.
Theme 1: Powerlessness
Most participants (n = 15) expressed that moral distress occurred when they were unable to meet the standard of nursing care and adhere to their professional ethical values. They felt powerless when they believed they had failed to advocate for patients. Nurses are responsible not only to patients but also to families, physicians, co-workers, and the healthcare organization; therefore, sources of powerlessness were evident at the patient/family level, the team level, and the organizational level.
Sub-theme 1.1: Patient/Family Level
Ten participants experienced moral distress because inappropriate or unnecessary treatments were directed by patients’ family members. In Thailand, surrogates are powerful decision makers when patients are incapable and they are able, as in other countries, to sue healthcare providers. Thus, some participants expressed moral distress when they thoroughly knew that the chosen treatment or decision was not appropriate for a patient but they had to follow the surrogate’s decision because of the power surrogates have (five participants): For end-of-life patients, they used to tell their children like, if I [patient] am severely ill, please don’t intubate me, please don’t place me on surgery, or please don’t give me any hurt, and please take me home. However, that is the oral living will, not an official one. When the patients are unconscious, their children are decision makers. They requested the aggressive treatment, no matter we tried to convince them. (N6) Most patient in my unit are elderly. Some patients are older than 100 years old. The patients always complain that they were on medical treatment for more than half of their life. They stayed in the hospital longer than their home. Some patients told their children that if they get worse, don’t take them to the hospital and please let them die peacefully. When the time comes, they couldn’t see their parents pass away in front of them without any action, so, they took the patients to the hospital and requested full treatment that could save the patients’ life. (N9) ……They want us to perform CPR and other aggressive treatments that could prolong the patient’s life. The prognosis was so poor. I truly knew that CPR was not going to extend the patient’s life. The patient was going to die in 24 hr. Anyway, when the family requested the CPR, we [doctor and nurse] need to follow the request. If we rejected the request, they would sue us. That’s why we had to follow. (N18) Mostly the child who lived far away was the decision maker. Although they didn’t look after the patient, they paid for the hospital cost. So, other children won’t make decisions because they didn’t have money to pay. Let’s say if they decided on the treatment, they would be responsible for its cost. So, the key person was the one who paid. When the decision was made by the one who didn’t live with the patient, he/she didn’t know the patient’s wishes. They had not seen how the patient suffered. Of course, he/she decided on his/her wish.…. Because he was guilty that he didn’t take care his parent [patient] and some might feel that this will be the last chance that he can pay back his parent. (N9) For this case, the patient passed the critical period. Although she couldn’t sit or eat by herself, her condition was better and better. She just needed time to recover. No matter how much we explain to them [patient’s family], they still insisted to take the patient home.….. We could only accept their decision; we had no choice. Their decision is final. (N7)
Sub-theme 1.2: Team Level
From participants’ responses, it was clear that a strong hierarchy among healthcare providers existed. Participants experiencing moral distress felt powerless and helpless to stop treatment that they thought was ethically wrong or involved sub-standard nursing care (seven participants). One nurse who witnessed a medical error in a pediatric patient said, The doctors requested that we stay quiet…I was trying to avoid facing the mother [of the child] which is not me at all. Everyone knows I love talking with the parents, I love to talk with those kids. I was very happy when I talked with them, but now I couldn’t. While I was talking with the mom, I had to look at the floor, I was scared to look at her eyes. When she asked about the patient’s condition, I could only say that I didn’t know much and please wait for the doctor. This is not me at all, I never said this to the parents. I felt like I was not a nurse. (N5) Nurses couldn’t take much action when we saw one’s unethical behavior because we have less power…. I had tried to do [advocate for patient] but I was hurt by his word like “you are just only a nurse; you never know better than me.” I cried inside after listening to him. (N15) ……Anyway, we need the doctors to sign on the consult form. The consultation needed an agreement from the doctors. If they don’t agree, we couldn’t consult. The patient would be treated aggressively. We are under them, we depended on them. Our profession was sometimes controlled by others. (N16)
A hierarchy existed not only between professions but also within professions based on seniority, both in nursing and medicine. This was seen as a barrier by three nurses: ……I was forced to inject adrenaline instead of starting CPR. She [a senior nurse] was in charge of the team, so nursing care was under her decision. Although she had more experience than me, she was putting the patient in risk……(N8)
Sub-theme 1.3: Organizational Level
The organization was perceived as strongly hierarchical and can be considered as an influential moral factor for nurses. Organizational support is one of the important indices of nursing work environment. However, sometimes organizational policies did not align with standards of practice (four participants).
A participant noted that In the ICU, we need immediately respond to the doctor. We couldn’t wait, 1 or 2 minutes is meaningful for the patient. But you know about the regulation, right? When we notify the doctor, we couldn’t jump to the resident or staff. We had to start with the extern or intern. In a hard case, they needed to report to the resident and then treatment was delayed. Some patients were in vegetative stage because of this. (N8)
A nurse said, I felt that the cardiogenic shock patient wouldn’t die if he got into our unit. In the general unit, there was no equipment. Everything was manual which was time consuming. We couldn’t measure arterial blood pressure there. If we had one more bed in the ICU, the patient would survive. (N20) ……When we transferred the patient to their unit [NICU]. They [nurses] were trying to blame us. They looked at our nurses’ note and questioned us. Although, we got 1:4 but when we had 1 or 2 very sick patients, we couldn’t record everything that happened like “the doctor couldn’t insert the central line so the antibiotic was delayed.” We just only wrote down what was the time we administered antibiotic. We had so many documents to be completed before transferring the patient, it diminished our care quality.….. We had tried to raise our issue but we gave up. (N4) I have talked with the head nurse about this situation but it was useless. It became my mistake.….. We never get any support from her. She is on the doctor’s side. No one walks with us. No one fights for us. Sometimes fighting alone is exhausting. (N4) We (nurses) were reported to the administrator that we didn’t complete what they ordered. It became our mistake and we got a punishment.……Yes, they did. They investigated but it was biased. You will never win. See, many of the administrators were doctors. (N19)
Theme 2: End-of-Life Issues
The second theme of this study was end-of-life issues. This theme resonated in the first theme of powerlessness but not all end-of-life situations involved powerlessness. For example, five participants perceived that they had to witness the patients receive aggressive medical interventions at the terminal stage of life because of insufficient knowledge and poor attitudes about palliative care practices: ….. I believed that this situation did not only happen in pediatric units but it also happened in adult units. It seemed to me that the palliative care system is developing. Doctors and nurses lack knowledge in this area. Although we were trained on palliative care, sometimes we don’t incorporate this concept in practice as it should be. (N18) We had an end-stage cancer patient. The cancer metastasized to multiple organs. He developed organ failure. He was place on extracorporeal membrane oxygenation (ECMO) and passed way after 2 days. I could feel how he suffered. He was in pain until the last minute of life. (N17) For a patient with brain death.…he was still treated with full treatment. It was unnecessary to treat the diabetes insipidus, but the doctors still prescribed Minirin and corrected abnormal laboratory eg., high sodium. (N1) A cause behind futile treatment is the information that is given to the patient’s family. In the ICU, we have many end-of-life patients. Their prognosis was so poor. I think, they should not be treated aggressively.….. I felt bad every time that I had to witness the doctor’s providing false hope to patient and family. They talked only one side of the treatment. Of course, the positive side! They would like to convince the family to agree with what they wanted to do. (N11) When we [doctors and nurses] talked with them [Buddhist families] about death, they felt that we were cursing them. I found many cases perceived it in a negative way. So, we invited a palliative care team to make sure that they were prepared about death but we were blamed by the family that we were hastening death. (N3) For Buddhists, some of them believed in a fortune teller more than us [nurses]. A patient’s wife came to us and requested us to do CPR and any treatment that can extend the patient’s life. She said that the fortune teller told her that if the patient was alive until Sunday, he would survive. Sunday was his birthday, she believed he would be born again and get a new life. (N1) Of course, I feel better. At the end of life, a Muslim family is easy to talk with. They accepted the death. They told me that after death they will meet Allah. Life is planned by him. So, when the doctors discussed with them about palliative care, they accepted it easily. At the last minute of life, they will ask to take the patient home. You could see right, there were many family members and neighbors visited the patient, especially when they knew that this gonna be the last time they could meet.…(N3)
Theme 3: Ineffective Team Function
The last theme of this study was ineffective team function. Different from sub-theme of the first theme, source of powerless at the team level, this theme mainly referred to factors that inhibited the effective team work, including poor communication and collaboration, working with incompetent healthcare providers, and inappropriate behaviors of colleagues.
Sub-theme 3.1: Poor Communication and Collaboration
Poor communication and collaboration impacted the quality of patient care in that nurses felt they were excluded as members of the team and could not communicate with patients and families sometimes because they were not sure about the goals of care (12 participants): The collaboration among the team wasn’t bad but it wasn’t good as it should be. We [nurses and doctors] had less discussion. We [nurses] were trying to be a part of team. We joined the morning medical rounds to know the goal and plan of each patient. But when they placed orders, they were totally different from what they had discussed during rounds. They changed the plan without informing us. They might feel that they don’t need to tell us. When the patient asked us about the plan, I could just tell him to discuss it with the doctors. I know I should not say that but I wasn’t really sure about the plan. (N15) When the patient was transferred to our unit, we got so many treatment orders for him that were unnecessary. He was sent here for palliative care. It seemed like the ICU doctor hadn’t cooperated with the doctor in our unit. So, their goal was different. (N19)
Sub-theme 3.2: Incompetent Healthcare Providers
Five participants noted that their colleague’s incompetence threatened the integrity of the patient due to delayed treatment or inappropriate pain management: To me the cause of moral distress was delaying medical treatment. It was delayed because of the doctor’s skill. He was so new. Actually, there was a septic shock care bundle that he could follow. The patient was critical and we need immediate decision on the treatment.….. Finally, the patient went into cardiac arrest and passed away. (N13) They [patients] got fasciotomy which everyone knows causes severe pain. But when we asked the doctor for pain medication, they always refused. They were afraid that the opioid would decrease the patient’s blood pressure. God! This was about knowledge. There were many kinds of medication that we could use.…(N14)
Sub-theme 3.3: Inappropriate Behaviors of Colleagues
Ignoring patients and treating them unequally due to social hierarchy are unethical behaviors of colleagues that four nurses found to be highly morally distressing: I witness the kid was suffering with pain. I notified him [doctor] so many times until I got mad at him. He didn’t even come to visit the patient. He was ignoring the patient. I could give the kid only paracetamol but it didn’t help. I needed more than that but he disappeared. Do you understand right, how I felt at that time? (N5) I notified him [doctor] that the baby’s respiratory rate was 100 bpm. He stood at the bedside and watched the baby breathe and said “it’s fast but shallow breathing,” it was acceptable. He said it was acceptable! I believed if the baby was his daughter or baby of the staff working in this hospital, he would immediately intubate and sent to NICU. It was unfair, life should be equal, no matter who was the parent. (N4)
Integration of the quantitative and qualitative findings
The qualitative data enrich the quantitative findings. Many participants recalled an end-of-life situation as their example of moral distress and this is reflected in the fact that three of the top 7 causes of moral distress were end-of-life-related. In addition, the qualitative data broaden a contextual understanding of moral distress in Thailand where the power/authority from families comes from the person who pays and the religious beliefs of the family can be influential. These stories speak to end of life and give an indication about how powerlessness ties into these end-of-life situations. Furthermore, the nurses provided stories about excessive documentation, inadequate resources (bed availability, equipment availability) and having too many patients—all of which show up in the top seven causes using the MMD-HP.
Discussion
The experiences of moral distress among Thai nurses were quantitatively and qualitatively explored. Of the seven highest ranked causes of moral distress, four addressed system-level workload issues (e.g. excessive documentation requirements, lack of resources) that compromise care quality and three were related to patient-level problems, especially end-of-life issues. In comparison with the most morally distressing root causes reported by Epstein et al., 13 five of the top 7 were the same. Epstein et al. 13 found two team-level root causes: watching patient care suffer because of a lack of provider continuity and witnessing low quality of patient care due to poor team communication, which were not among the most distressing for our Thai nurse sample.
Three of the most morally distressing root causes for Thai nurses such as feeling required to overemphasize tasks and productivity or quality measures at the expense of patient care, having excessive documentation requirements that compromise patient care, and experiencing compromised patient care due to lack of resources/equipment/bed capacity are new items on the MMD-HP, making comparison to other studies using the MDS-R or MDS difficult. However, support for these items comes from the literature. For example, Wilson et al. 55 invited nurses to respond to an open-ended question to describe morally distressing situations beyond the MDS items and found that nurses illustrated that workload made them experience moral distress because it impacted their work performance and made them less empathetic and more careless. Chen et al. 32 applied Q methodology to explore the perspectives of nurses regarding moral distress and found that excessive administrative work and paperwork distracted and prevented nurses from providing quality care to the patient.
End-of-life situations such as providing aggressive treatment due to family decision or because no one will make a decision, and carrying out unnecessary/inappropriate treatments were found to be problematic via the MMD-HP and the interview data were consistent with this and provided additional depth. Approximately 80% of the representative nurses described stories about caring for patients at the end of life. The nurses in this study expressed a sense of powerlessness because they felt compelled to follow a family member’s or a doctor’s decision that they felt caused suffering or prolonged death. They felt forced to participate in aggressive and unnecessary/inappropriate treatments, which is similar to several previous studies.9–12,15–19,23,24,56–58 Varcoe et al. 2 found that feeling powerless was predominantly described by the hierarchical nature of constraints. We found a similar finding in which nurses felt obligated to carry out a physician’s “family-driven” order even when they knew it to be wrong. This study found that families’ cultural and religious beliefs could play an important role in the treatment decision at the end of life. Although Buddhism is the national religion of Thai people, in the southern Thailand where this study was conducted, approximately 28% are Muslim. 59 Nurses express that the religious doctrine that formed the worldview of patients and families was foreign to some nurses’ understanding and sometime inconsistent to medical standard of care. Bressler et al. 60 explored nurses’ experiences of how cultural complexity creates differences between nurses’ and family’s expectations for patient care at the end of life and found that the patients’ faith often conflicts with common healthcare practice and the nurses’ own views, which led to moral distress. They also expressed a desire to learn more on other religious beliefs in order to provide more sensitive care to families and to feel more competent and effective as nurses. Similar to Stanley, 61 the nurses in this study experienced professional moral conflict related to caring for patients with contrary beliefs and culture.
Beyond system-level and patient-level root causes, team-level root causes were also found to be a problem leading to moral distress among Thai nurses. Although team-related items in the MMD-HP did not rank as top causes, analysis of the interview data revealed that poor communication and collaboration and working with incompetent colleagues were frequently described as morally distressing. Several quantitative studies showed that issues related to poor team function were the top cause of moral distress.9–11,13,16,18,19,24,57,58 Poor communication and collaboration are unhealthy for healthcare teams and could affect patient outcomes. 62 Having different goals or being unsure about goals could severely diminish the safety and quality of patient care.28,32,37
With regard to relationships between moral distress and demographic and practice factors, no differences in moral distress scores were found when comparing participating nurses by age, years of working, or end-of-life training. Our findings are consistent with some studies11,17,57,63 but not with others where positive correlations between moral distress and age12,56 or years of experience or years in current position10,12,18,23 were found. One explanation may be that this association demonstrates the crescendo effect in that as clinicians gain years of experience, they also repeatedly confront morally distressing situations causing a rise in moral distress over time. After consideration of the crescendo effect model, we questioned whether it was not the number of years of clinical experience but rather the number of morally distressing situations a provider encounters that triggers a rise in moral distress over time. Thus, in this study, we asked nurses to estimate the number of morally distressing situations they had encountered in the past year and found that this correlated positively with MMD-HP scores. While not an objective measure, the number of episodes of moral distress may be a more reliable indicator of the crescendo effect than years in practice or years in current position. To explore this further, objective measures of episodes are needed.
In this study, acute care nurses’ moral distress levels were significantly higher than those of the critical care nurses. This finding contrasts with several previous studies.13,14,16–19 Contextual differences between Thailand and western countries could offer some explanation although we did not investigate this directly. In some acute care units, nurse: patient ratios can be as high as 1:10–15. And, in these units, widely varying levels of patient acuity are admitted including stable patients, palliative care patients, terminally ill patients, and critically ill patients. The number of intensive care unit (ICU) beds is limited and patients who are critically ill may not be able to be transferred to a higher level of care. In addition, acute care units are mostly manual and lack equipment such as cardiorespiratory monitors, blood pressure monitors, and intravenous pumps. Sometimes, higher technology equipment is used without appropriate training and preparation. Comparison of the narratives from the nine critical care nurses and the nine acute care nurses did not reveal specific or obvious differences. Therefore, this finding calls attention to the need for further exploration, paying particular attention to the context.
Previous studies have found that higher levels of moral distress are significantly and positively correlated with intention to leave a position due to moral distress,10,13,16,18,19,23,24 and our findings were similar. In addition, unit setting, number of moral distress episodes, and intention to leave were significant predictors of MMD-HP scores, controlling for other variables. These consistent findings strongly suggested that moral distress is a substantial threat to employment longevity within the international healthcare community, lending further support to the importance of interventions designed to mitigate moral distress in order to improve staff retention.
Conclusion
This study provides initial evidence that the Thai translation of the MMD-HP captures the root causes of moral distress among Thai nurses. Even if root causes are similar between cultures, the way they are experienced may vary according to culture and context. In this study, three specific findings contribute to a growing body of literature about moral distress in different cultures. First, acute care nurses’ moral distress levels were higher than the critical care nurses, which is rather unique and may be partially attributable to environmental issues such as lack of resources and large nurse: patient ratios. Second, the number of morally distressing episodes, rather than years in practice or in current position, correlated positively with MMD-HP scores and may provide some new insight to the crescendo effect. Finally, the influence of patients’ and family’s religious beliefs on end-of-life care decision is similar to those in the west. However, the understanding of how clinicians approach non-Christian’s decision at the end of life and how the patient’s and family’s religious and cultural perspective ties into the concept of moral distress is not yet clear.
This study was limited in that it has explored moral distress only among Thai nurses. Future studies should measure moral distress among multiple types of healthcare professions so that (1) a clearer picture of moral distress among Thai clinicians is gained, (2) similarities and differences between cultures become better understood, and (3) interventions may be developed that are sensitive to cultural context, which are effective in mitigating moral distress. A large study at the national level might provide more comprehensive findings that may drive healthcare policy development. Studies of coping strategies in nurses and other providers who experience moral distress are needed as interventions may build on these strategies, keeping in mind that moral distress does not indicate a problem with the individual but with the healthcare system in which the individual works.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.