
Abstract
Background
Moral distress is a phenomenon that can lead to an imbalance of the mind and body. There are many coping strategies to overcome the obstacles that lead the subject to this condition. Some coping strategies are capable of being achieved through the cultivation of moral resilience.
Aim
The aim is to identify the strategies of moral resilience in the nursing management of University Hospitals in Brazil.
Research design
The research design is the qualitative study with discursive textual analysis.
Participants and research context
: 44 nurse managers and nurses in leadership positions participated in a total of 30 University Hospitals in Brazil. Data were collected online, using a questionnaire with open questions.
Ethical considerations
The Ethics Committee approved the study. Participants received information about the research, agreed to respond to the questionnaire, and were guaranteed anonymity.
Findings
Personal adaptive strategies (intrapersonal and interpersonal) and organizational collaborative strategies (intrinsic and transformational management) emerged from this process. The intrapersonal strategies involved elements of rationality, flexibility, rebalancing practices, moral courage, and detachment. The interpersonal strategies addressed support networks, team involvement, and dialog. Organizational strategies dealt with actions which reorient ethical infrastructure, ethical education, and psychological protection, as well as fostering dialogical relationships, empowerment, and cooperation.
Conclusion
From the perspective of social historical construction, it is understood that developing personal and organizational strategies is essential to cultivating moral resilience.
Introduction
In the work process of the hospital context, nurse managers face numerous challenges related to complex organizational practices, asymmetries of freedom and autonomy, fragmentations of care, and power microspaces.1,2 Coping with these challenges can lead to moral distress (MD). As a process, MD can appear from moment the professional recognizes their ethical responsibility in the face of a conflict situation, their reflections on possible actions until identifying a morally correct decision, however, feel prevented from acting in accordance with their conscience and values, due to different types of barriers. 3
Many studies are aimed at recording the frequency, sources, and consequences of MD, and others are dedicated to highlighting possible interventions aimed at reducing its effects on professionals and their physical and emotional health.4,5 Among the strategies for coping with MD, the concept of moral resilience (MR) stands out. Moral resilience is the ability to preserve or recover moral integrity through the development of skills that strengthen the connection and commitment to the primary intentions of individuals, in the face of morally complex, ambiguous, or conflicting situations. Moreover, MR approaches the human experience in an interconnected way, in its moral, biological, psychological, cognitive, spiritual, and relational aspects. 6
As it is a complex phenomenon, multidimensional approaches are needed to understand MD within the health area, with research that contributes to expanding resources aimed at helping professional cope with it.8,9 From the perspective of individual or collective MR, possibilities are opened up in the fields of psychology (reason and emotion), biophysics (structure and body performance), spirituality (transcendent connection), cognition (learning), pedagogy (knowing and doing), and human interaction (intra and intersubjective). 10
Work experiences in the health area are characterized as challenging, not only due to the aspects involved in caring for others but also for relational and environmental issues that influence the self-care of professionals. There are numerous factors related to the contexts of the health work process capable of stressing or protecting. Therefore, environmental, personal, and relational factors must be highlighted, discussed, and understood in order to become protective tools instead of becoming triggers for suffering. 11
The scientific literature on MR considers the production of knowledge from different areas and contexts.6,12 Autonomy and moral courage are two elements strongly associated with the ethical dimension of health work, evidenced in literature review studies, and especially important for the categories of this study. Low levels of autonomy as a personal characteristic or in service management that do not promote the empowerment of professionals are aspects correlated to MD. 13 The perception of MD and its confrontation can be associated with the moral courage required in ethical conflicts according to personal principles, the profession, and health institutions. Thus, moral courage is also influenced by individual and organizational factors.13,14
Specifically regarding nurse managers, studies emphasizes fostering and supporting leaders, such as engaging in dialog, promoting ethical education, triage of MD manifestations, and providing the necessary resources to intervene in suffering.15–17 Therefore, it is understood that it is necessary to examine promising coping practices when addressing the process of MD experienced by nurse managers in hospital organizations, in order to promote their integrity and moral well-being.
The present study aims to identify the strategies of moral resilience in nursing management in University Hospitals in Brazil, with a view to supporting organizations in the creation of a culture of ethical practice.
Research methods
This is a descriptive and exploratory study, with a qualitative approach, 18 performed with the participation of nurse managers in University Hospitals in Brazil.
The sample was randomly selected by drawing lots, and 55 nurse managers were invited. From this possible universe, a final sample of 44 participants was obtained, distributed by 30 University Hospitals in Brazil. From the analysis of this sample, it was possible to confirm the saturation of the data. 18
Data were collected via an online form, and access links were sent to participants’ emails, between December 2019 and March 2020. The questionnaire contained two open questions: When you experience moral suffering, what are your strategies to reduce this suffering? How has your institution contributed or could it contribute to the development of moral resilience in work environments and relationships? In addition to the questions, the participants also had access to MD and MR concepts, to situate them on the objects of the study. This guide was previously tested with two nurse managers in one of the hospitals and who were not included in the study sample.
Discursive textual analysis was supported by the Nvivo software (version 11), from the researcher’s interpretative perspective and by empirical-theoretical approximation in three steps: unitarization of data (fragmentation of interviews in units of meanings); categorization of the corpus (theoretical and thematic agglutination); and communication, with the recording and presentation of productions (metatexts). 19
In the unitarization stage, the elementary units of meaning were identified based on the strategies for coping with the MD process and the possibilities of intervention by institutions in the cultivation of MR. From the units established in the first stage, similar components were grouped by theoretical and thematic agglutination. The principle of homogeneity guided the formulation of emerging categories, allowing new understandings of MR cultivation strategies. Finally, the strategies adopted by nurse managers during the MD process and the development of MR in work environments and relationships were theorized and understood based on the emerging categories.
Ethical considerations
The study was approved by the Ethics Committee on Research with Human Beings, in compliance with Brazilian legislation. All participants were instructed on the research and signed the informed consent form (ICF).
The questionnaires were saved on the principal investigator’s computer in anonymous folders. To preserve the anonymity of the participants, the term “NM” was used, which means nurse manager (NM) followed by a sequential ordinal number assigned according to the receipt of the forms (NM1, NM2, NM3 to NM44…).
Results
Two subcategories emerged from the corpus of the managers’ reports about the coping strategies regarding MD, conceived as personal strategies: “intrapersonal strategies” and “interpersonal strategies.” Two subcategories emerged from the participants' imagination or expectation regarding the institution contribution to a culture of ethical practice and cultivation of MR, perceived as organizational strategies or collaborative possibilities: “intrinsic management” and “transformational management.” Figure 1 summarizes and illustrates these results. Summary of categories, subcategories, and associated elements results of the discursive textual analysis of the study.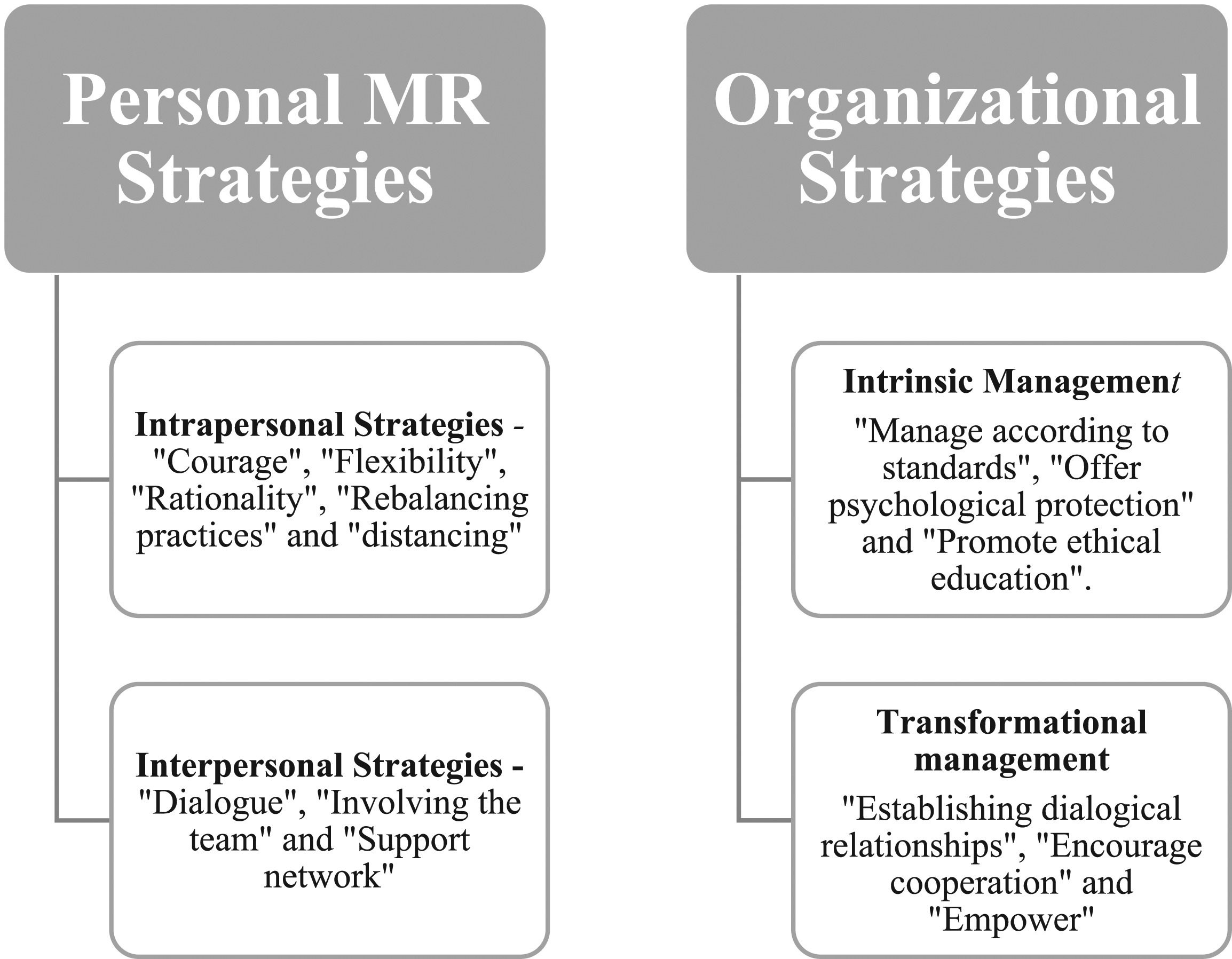
Personal MR strategies
In the unitarization process, 105 textual fragments (units of meaning) were coded, of which 61 (58%) were related to “intrapersonal strategies” and 44 (42%) to “interpersonal strategies.”
Intrapersonal strategies
The “intrapersonal strategies” reflect individual devices and are related to the practices of connection or interaction with the internal subject (the “I"), involving access to an internal repertoire of coping methods and resources, potentially related to the process of development of the moral agent. This subcategory integrated five elements: “courage,” “flexibility,” “rationality,” “rebalancing practices,” and “distancing.”
The element “courage” referred to the search for an action with ethical conviction, determination, and persistence, defending what it believes to be “correct,” dedicating all efforts in situations of MD. […] As a principle, I believe that the best way to do something is the right way and I do not give up […]. (NM1)
First, I try to keep track and assimilate the situation, but I do n't give up my ethical position […]. (NM5)
The element “flexibility” emerges as a strategy to deal with MD giving new meaning to their experiences, with cognitive ability, adaptability, and overcoming moral problems. […] Changing the perspective of the problem can generate new ways of justifying the decision still in line with our moral precepts, even though we know that we practice flexibility, a redesign, that it is justified as the possible or least harmful factor for the whole in the face of real situations over which we do not have complete control (NM2)
The element “rationality” is related to techniques in the use of objective standards to cultivate MR. In this case, the manager deals with the MD process through a methodical, analytical, and tactical behavior, seeking the best time to act. It depends on the situation: sometimes I retreat and I wait for the best time to try to resolve the issue with those involved and/or senior management […]. (NM38)
Also from the perspective of reason, the nurse manager believes that he can cultivate MR through the development of self-control, seeking to support and sustain his conduct on theoretical and legal bases, as well as using your experiences, the result of individual historical constructions. I immediately try to control myself and speak as little as possible, so I believe that I can also avoid situations in which the people involved often try to establish forced or psychological agreements […]. (NM3) […] I like to study a little about ethics and bioethics; it helps me to understand situations and to deal with these issues with people better […]. (NM4)
The element “rebalancing practices” includes reports of reflexive practices for self-control and self-awareness (body, mind, and spirit) as a personal routine. […] Personal and regular strategies that I take are: prayer, exercise practices, massages and therapy. I think they make me more aware of my role, because my attitudes in the workplace interfere with other people’s lives. (NM11)
Reflection, prayer (as I am religious, I understand it as an essential factor to maintain balance), and planning actions that minimize the impact of the fact that cause suffering. (NM6)
The “distancing” is mentioned when the manager faces the MD process, remaining in a position of removal and relative omission. […] I prefer not to confront some situations and keep to myself […]. (NM8) […] I always try to avoid clashes that increase any suffering. (NM9)
Interpersonal strategies
The “interpersonal strategies” are associated with the relational practices of interaction of the internal agent with the external agent (the “I and the other”). This subcategory converges three elements: “dialog,” “involving the team,” and “support network.”
The element “dialog” cultivates MR when the manager seeks to interact with the other through discussion, providing moments of active listening and applying clarity and transparency in communication. Investigate the reasons related to the situation, promote dialogue and build strategies so that the event does not happen again. (NM39) Establish dialogical relationships to highlight confrontation and defend the ethical aspect, aiming to ensure and guarantee human value. (NM10)
The element “involving the team” emerges as an intentional and directed MR practice, when the manager seeks to interact with the team beyond the dialog, with the purpose of gaining the support and collaboration necessary to deal with the MD process, uniting and mobilizing people in the solution of the problem (moral). […] I seek to discuss the problems with the team as a way to face ethical situations together […]. (NM4) […] in the team meeting, I address the situation, without identifying the origin or parties involved, I look for alternatives for a resolution together with the team. (NM31)
With the element “support network,” the nurse manager faces the MD process seeking support in the available support network. These relationships can be represented by friendship bonds or formal contacts in this network, without necessarily involving an institutional (formal) figure. […] I often share problems with people close to me that help me see better the alternatives […]. (NM5) I try to share this suffering with trusted colleagues or even with superiors. It helps me to understand the situation better and get through it. (NM12)
On the other hand, the nurse manager also seeks to face the MD process using the resources available in their institutional (formal) support network. In this case, it is an interaction between individual and institution, and, in this perspective, represented and materialized by a formal subject. Whenever possible, I seek to access the Organizational Psychology sector to record the fact and further guidance. (NM13) I seek to talk openly with my immediate leadership about the discomfort. Even if he offers me an answer that does not solve the problem, saying the nuisance is already very good […]. (NM2)
Organizational strategies
Seventy-seven fragments were coded in the unitarization process from the corpus of the reports, where 41 (53%) were related to “transformational management” and 36 (47%) to “intrinsic management.”
Intrinsic management
The “intrinsic management” deals with the reorientation of ethical infrastructure from the strengthening of responsibilities and fundamental aspects of the organization. Based on the participants' ideas about the institution’s expectation of collaborating for the development of MR, this subcategory exposes three elements, “manage according to standards,” “offer psychological protection,” and “promote ethical education.”
The element “manage according to standards” indicates that the institution would promote the cultivation of MR by assuming its intrinsic responsibilities (normative structure and directive/strategic), acting ethically, fairly, and transparently, in line with legal practices. Assuming the responsibilities inherent to the positions, without the concern to meet desires. Exposing the rules and acting according to them […]. (NM14) […] Standardization of the guidelines between the various sectors, in order to apply the same conduct to all […]. (NM15)
The element “offer psychological protection” refers to the structuring and organization of mental health support resources (individual or collective), especially clinical psychology and organizational psychology. Through […] psychological care to professionals who hold managerial positions. (NM38) […] Another way to contribute is to form support groups with the involvement of organizational psychologists, providing a space for discussion and exchange of experiences. (NM16)
The element “promoting ethical education” represents to intention to offer of courses on ethics and MR, for learning of leaders and team, to minimize the generating sources of ethics conflicts and the development MD. With leadership strategies and courses that focus on this issue, that clarify the real meaning of these terms and how to work with them. (NM30) I believe that training is welcome, in order to support/sustain the conducts that must be taken […]. (NM15)
Transformational management
“Transformational management” brought to light the elements of interaction between the hospital (the “structure”) with the institution’s living organism (the “me and the other”), referring to the relational dimensions with the moral agents, modifying its moral structure, giving new meaning to their experiences, and the inspiring way they deal with ethical issues. This subcategory has a collaborative meaning, due to the possibility of the institution producing an organic transformation in the dynamics of nursing management relations. In this case, the resources are “dialogical relationships,” political awareness about the collective interest (“encouraging cooperation”), and fostering autonomy for nurse managers (“empowerment”).
With the element “establishing dialogical relationships,” the nurse manager expects greater approximation with managers of other levels, establishing an effective communication channel (tuned and transparent), as well as dynamics and practices of integration between leaders, to share experiences and solutions about the (moral) problems experienced. I believe that the simple dialogue with the higher levels and more moments of integration between the different leaders could be important to assist in this process. (NM17) Implementation of conflict mediation committees and interpersonal relationship workshops, with the involvement of managers in open discussions on ethics in the work environment and the moral commitment for all […]. (NM12)
The element “encourage cooperation” highlights the desire for strategies to nourish the feeling of cooperation among workers, generating commitment and co-responsibility. […] Further clarification to employees in the sense of respect for hierarchy and remembering that the main objective of the institution is work and assistance aimed at the collective and not personal needs […]. (NM18) Strategies that promote personal change using creative activities, reflection through meetings where the collective strengthens interpersonal relationships, space for socialization and listening, and intensification of the recognition of human value. (NM10)
The element “empower” presupposes that the institution should support it, giving it power and autonomy and offer the necessary support for nursing management. […] a manager needs to be well informed, analyze situations from more than one point of view and also have the support of the areas of people management and human resources, so that they feel more confident in the face of confrontations. (NM3) […] Have autonomy to lead the nursing team in a very calm, humane way, seeking to practice justice and equity, with a voice in the collegiate, among others. (NM10)
Discussion
The results showed that nurse managers at university hospitals rely on personal and organizational strategies to deal with the MD process, especially from the perspective of promoting MR.
In the practice of these nurse managers, these potential MR-promoting strategies reflect the singular (personal) and systemic (institutional) alternatives that can provide them in coping with MD and its main generating sources. Considering that MD is related to intrinsic and intra-organizational factors, potentially promoting aspects can be enumerated, such as conflicts of interest and power, identity crisis, violation of autonomy, insufficient resources, coercive management models, insecurity in the care environment, inappropriate working conditions, and precarious ethical climate.20–23
Intrapersonal strategies were the resources most used by nurse managers in the university hospitals and in this regard they are associated with individual, cognitive, and behavioral approaches as demonstrated in other studies. 21 In this set of adaptive response and overcoming the adversities and burnouts that are involved in MD, it is understood that resilience goes far beyond the quality or innate characteristic but arises as a result of a dynamic process of development and learning.24,25 Thus, it can be considered that resilience is not a state but a personal condition. 26
Yet, from this perspective, nurses are confronted with numerous and different moral problems, requiring a clear ethical positioning, consistent with their moral judgment for ethical decision making. 3 In this process of deliberation, the professional seeks to find concrete solutions and prudent courses of action, involving an analysis that considers the subjective (intuitive) aspects of professional experience and objectives (reason), deontology, and foundations of ethics as science. 27 The rationality of professionals expresses the adoption of theoretical-legal standards and management techniques to support deliberation in the face of a widely standardized, regulated, and multi-liability system. In institutions similar to those studied, there was a strong use of rationality in decision-making, especially at the top of the organization, often attributed to the complexity of the hospital environment and its formal relations. 28
The critical positioning of determination and defense of the ethically correct, highlighted by the participants, refers to the concept of moral courage. The moral courage connects to moral sensitivity for their recognition of morally relevant aspects and mobilizes for taking action and making ethical decisions.29–31 Moral courage relates organizational and individual factors, such as sensitivity and commitment to ethical principles, supportive work environment, and team work. 32
Situations of ethical conflicts, ethical deliberations, or moral suffering require nurses to demonstrate cognitive flexibility, with the ability to reassess perceptions and experiences of suffering, recognizing meanings, negative or painful aspects, and coping alternatives. 33 This resignification found in the reports represents transformational learning, in which the resilient learn from their experiences and change their responses in subsequent events, confronting forces and limitations, reexamining assumptions and justifications, and reconnecting with purposes of the moral structuring. 30
Other studies agree with the results of this study regarding intrapersonal strategies. They are behavioral forces which strengthen moral integrity, mindfulness, self-regulation, emotional intelligence, and moral self-awareness. Performing physical activities and spiritual practices are examples of personal self-care actions that can help in the development of harmonious connections and internal capacities to defend moral principles, transmitting calm, well-being, firmness, and stability in the midst of challenging circumstances.4,5,7,14,30 Maintaining positive beliefs about oneself and its role in the world results in adaptive thoughts, with the potential to prevent hopelessness and encourage resilience. 34
Distancing from the ethical conflict is another intrapersonal strategy identified. Although adaptive coping presupposes some experience with adversity, other reactions can be produced: the individual does not show interest in an ethical issue, adopting a posture of moral indifference 35 ; conformist attitudes, closing our eyes to possible conflicts, or ethical dimensions 36 ; or remaining in moral uncertainty, without deliberating on the problem. 4
Regarding interpersonal strategies, from the perspective of relational ethics, we highlight the element “support network,” which offers support (formal and informal) to the nurse manager of the university hospitals to cope with MD and promote MR. It consists of reciprocity, guided by empathy, cooperation, trust, and even friendship. This ability to cultivate interconnections with others is a crucial point of MR. 29 Seeing yourself as part of a larger moral community provides a safety net in response to morally complex or distressing situations. Establishing interpersonal relationships to cope with the ethical complexities diminishes the sense of despair and isolation that often accompanies MD.6,37 The external support offers access to formal and informal structures to support the professional and the construction of a healthy practice environment. 5
The search for clarity and transparency in communication could also be verified by the interpersonal element “dialog.” The healthcare professionals capable of speaking with confidence and clarity about insidious threats to their integrity promote moral resilience in themselves. Efficient dialog allows action and provides a moment of approximation with team members and active listening brings up reflective issues that go beyond protests and help to cope with MD.6,37,38
In interpersonal relationships and their innumerable ethical challenges, the nurse manager of the university hospitals seeks to involve the team to find a solution for the moral problem, in an intentional process of co-creation.22,39 This confrontation aims to preserve relational integrity and develop team moral efficacy, based on solidarity and professional responsibility, promoting moral agency and confidence in the ability to overcome adversities effectively and assertively. 40
From the perspectives of nurses participating in this study, the collaborative strategies of organizations for the promotion of MR in environments and personal relationships depend on the reorientation of their intrinsic management structures. The ethical foundation of an organization must be solid, promote ethical education, offer essential resources for the psychological protection of professionals, and develop a strong policy of cooperation and empowerment. The ethical practice requires the establishment of norms and responsibilities, which aligns priorities to create an environment where ethical, individual, and organizational values are references to the shared commitment to quality care, safe, and ethically grounded. 39
In this way, it promotes the ethical climate in the organization which develops relational skills and ethical competencies essential in the moderation of ethical conflicts.4,17,41 All this context through which ethical education permeates ethical education is a powerful ally to strengthen MR, influencing ethical decision-making, reasoning, and moral sensitivity.21,42–45
Also in the category of organizational strategies intrinsic to management, although the nurse managers of the university hospitals seek to preserve psych emotional health and develop relational skills through personal strategies, there is a strong desire for the restructuring of the organizational psychology service. In fact, there is a significant correlation between psychological health and resilience, both acting as protection variables.46,47
In relation to transformational strategies, the organization is also responsible for guiding ethical practices, above all, based on its exemplary role and mainly through dialogical practices. This involves the establishment of a policy of open dialog, with respect to differences of opinion and free thinking, spaces of integration, and methods to cultivate moral reflection.44,48 In addition, it is essential to establish an effective communication interface with professionals, which is synchronized, clear and transparent, structured and universal, with the greatest possible scope to enable interactions and understanding about the transformations of the environment. 49
The organization has the role of promoting the autonomy of nurses in management, supporting their empowerment in the conduction of moral issues. Nurse managers work with a greater number of workers in the institution and, as morally sensitive agents, based on ethical standards, moderate the different interests and values of the nursing structure and professionals. In this complex relationship of fragile reciprocity, the restriction of power and the precarious ethical climate tend to hinder ethical decision-making and thus increase MD.50–52
Moral well-being requires the organization to enhance the feeling of cooperation and collectiveness in personal relationships. And this can go beyond the individual’s formal duties, it is voluntary and citizenship behavior that represent the basis for the development of an ethical climate and ethical leadership.47,53 This solidarity perceived by nurses managers of the university hospitals can strengthen relationships of mutual respect and empathy, especially when each one recognizes their roles and perceives themselves as an integral part of the nursing work process.
Conclusion
With this study, it was possible to identify the strategies of moral resilience in the nurse managers of the university hospitals. In order to deal with MD, nurse managers adopt personal strategies (intrapersonal and interpersonal) and highlight organizational strategies (intrinsic and transformational management) as essential collaborative possibilities in the cultivation of MR.
Organizations should be based on strategies to reorient their ethical infrastructure and transform relations with agents, aimed at building a culture of ethical practice and solidarity as an exercise of citizenship. Thus, it is necessary to direct resources for the development of ethical skills and abilities, the structuring of a psychological protection network, as well as establish an unpretentious and assertive dialogical relationship, expanding the power and autonomy of the nurse manager.
Limitations
The use of qualitative methodology does not allow generalization. The inferences regarding moral resilience are related to the single sample of this study. However, the research provides an important and in-depth scope of knowledge on the subject. Their findings contribute to the discussions and foster further studies which can explore this object in other scenarios and different populations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Academic Excellence Program of the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Brazil.