
Abstract
Keywords
Introduction
Ethical decision-making is one of the main components of nursing care. According to Kohlberg’s theory of moral development, its’ four components include moral sensitivity, moral judgment, moral motivation, and moral character. 1 In this schema, moral sensitivity is the first step and cornerstone of ethical decision-making.2,3 Moral sensitivity is the ability to enable one to recognize moral conflicts, make sensory and perceptual perceptions of vulnerable situations, and be aware of ethical outcomes of deciding for others. 4 It is the mechanism whereby “morals,” as beliefs about the nature of right and wrong, are translated or applied to situations in which decisions are required about what to do in a given situation.
Moral sensitivity therefore, prepares the ground for nurses to provide effective and ethical care, and in making nurses sensitive to ethical issues in the professional environment, can provide assurance to patients about professional ethical standards in nursing care.5,6 Moral sensitivity also contributes to the acquisition of problem-solving skills by enabling the health professional to better recognize moral problems and improve moral decision-making capabilities.7,8 The application of moral sensitivity in ethical decision-making therefore contributes to prevention of avoidable damage imposed on the patient and the health care system due to non-compliance with moral principles in nursing. 9
The particularities of the intensive care unit (ICU), invites a high level of attention to patient rights and moral decision-making. 10 ICUs are high-pressure work environments in which healthcare personnel provide high-quality, intensive care services to patients with critical needs.10,11 Advances in life-saving technology and improvements in nursing care practices in ICUs have increased the patient’s chances of survival, while at the same time, increasing the chance of survival creates a stressful environment for the healthcare team, patients, and their families. The unpredictable nature of care provision in ICUs means that to prevent potential harmful consequences, treatment and care decisions need to be made within a shorter time frame. Thus, caregiving stress in ICU is intrinsic and a scientific-based decision as an answer to “what to do,” may not necessarily provide an answer to the question of whether it really “should” be done or not. 12
Numerous factors, such as age and gender, spiritual, cultural, and religious values, work experience, level of education, work environment, and quality of training in ethical principles and practices, have been found to affect the development of moral sensitivity in nurses and healthcare team members.4,7 It has been argued that the teaching of ethical principles, especially awareness of patients’ rights, is one of the main ways to form moral sensitivity, in order for nurses to make appropriate ethical decisions to protect patients’ rights. 10
There has long been debate about the most effective method for teaching ethics in health care settings. 2 Methods include case study, scenario writing, lecture-based methods, group discussion, small group work, and e-learning for this purpose.13,14 With advancements in the Internet and computer technology, new challenging and interactive teaching methods, such as e-learning and simulation, have emerged and developed as a teaching approach to healthcare education over the past decade.15,16 Simulators create a high-quality environment similar to real-world environments that is safe and enjoyable for learners and it deals with learning, practicing, and making mistakes without direct contact with patients and the risk of injury.13,15 Thus, during the simulation, it is possible for nurses to participate in trial and error without harming a living patient 17 and receive virtual training before actual interacting with the real patient. There are different types of simulation techniques such as written simulation, 3D models, screen based simulators or computer simulation such as videos, software or virtual reality and surgical simulators, standardized patient with real or simulated roles (trained actors), intermediate fidelity simulators with programmable full body size patient simulators that are computer controlled, and high fidelity simulators that are interactive and computer controlled. 18 Following the implementation of procedures that can endanger the patient’s safety, the tendency to use virtual patient simulations before the student enters the clinic has increased. 19 Ethics virtual patients are computerized and interactive simulators of real-life scenarios that have moral components 20 and provide a virtual environment for improving patient interaction techniques that enables the user to query the patient and receive the patient’s response and help users in clinical reasoning and decision making. 15 Among these different instruction techniques, written simulation has long been considered. This includes paper-based simulations in which a patient and their health management issues are written and used for a variety of purposes across medical disciplines. 18 Despite the easy and widespread use of written simulations, the clinical judgments made using these may not reflect clinical and behavioral realities as they do not sufficiently simulate the cognition required in clinical settings. 21
Miller’s assessment pyramid, has four levels of evaluation including knows, knows how, shows how (competence) and does (performance). Written simulation and computer simulation can perform the assessment at the “knows” and “knows how” levels. 22
Objective
Arising from questions about the most appropriate methods of instruction, the present study aimed at determining and comparing the effect of written and virtual patient computer simulation approaches on the moral sensitivity of ICU nurses. The following hypotheses were examined: (1) Virtual patient computer simulation was effective in increasing nurses’ moral sensitivity. (2) Written simulation was effective in increasing nurses’ moral sensitivity.
Method
Participants
Study participants included 204 (n = 68 in each group) eligible nurses working in the ICUs of hospitals affiliated to the Tehran University of Medical Sciences, Tehran, Iran, from 2019 to 2021. The participants were randomly assigned to the three groups of control, written simulation, and computer simulation using a random block sampling method. Concealment was performed with sealed envelopes. A letter was placed in the specified order inside each envelope (by the corresponding author), and then was given to the first author.
Inclusion criteria were: working in ICU for at least 1 year; Willingness to participate in the study; holding a bachelors’ degree in nursing.
Exclusion criteria included: a history of attending an ethics seminar or workshop in the last 2 months; moving to another department during data collection.
Materials
In the present study, demographic and Lützén moral sensitivity questionnaires were used as data collection instruments.
Demographic questionnaire: Included items on demographic characteristics-i e, age, gender, marital status, years of working in ICU.
Lützén moral sensitivity questionnaire: This 30-item questionnaire measures the status of moral sensitivity in nurses when delivering clinical services. Items are scored based on a seven-point Likert scale from strongly agree 7 to strongly disagree 1. The scale includes the six areas of interpersonal orientation, structuring moral meaning, benevolence, modifying autonomy, experiencing moral conflict, and trust in medical knowledge and principles of care. The scores range from 30 to 210, and higher scores indicate more moral sensitivity. In Iran, the psychometrics of a modified instrument were confirmed in the study by Hassanpoor et al., with a Cronbach’s alpha coefficient of 0.81, using 25 items. 23 The items were scored based on a five-point Likert scale as strongly agree (4), relatively agree (3), relatively disagree (2), strongly disagree (1), and no idea (0). The scores ranged from zero to 100. Accordingly, scores 0–50 were considered low, 51–75 moderate, with 76–100 indicating high moral sensitivity. The questionnaire had six dimensions of respect for the client’s independence (items 10, 12, 13), knowledge of communication with the patient (items 1, 2, 3, 4, 17), professional knowledge (items 16 and 24), experiences in moral problems and conflicts (items 9, 11, 15), utilization of ethical concepts in moral decision making (items 6, 8, 14, 18, 20) and honesty and benevolence (items 5, 7, 19, 21, 22, 23, 25).
Procedure
The present randomized, controlled trial was conducted with nurses working in the ICUs of hospitals affiliated to Tehran University of Medical Sciences, Tehran, Iran. After obtaining ethics approval from the Ethics Committee of Tehran University of Medical Sciences, eligible participants (ICU nurses) were enrolled in the study using the block sampling method. After explaining the study objectives to participants and obtaining informed consent, before the study onset, the demographic and Lützén moral sensitivity questionnaires were completed. In the virtual patient computer simulation group, the educational content was presented in five scenarios. Since ethical guidelines are developed in many countries as patient rights codes of practice based on the ethical values of professionals, these consider performance based on such values. 24 The Declaration on Rights of Patients was first developed by the National Nursing Union (NNU) in 1948 in response to patients’ expectations, the legal principles of informed consent, the confidentiality of information, respect and dignity for patients, and admission without discrimination. 25 Therefore, patients, as the target group of healthcare services, have rights that should be observed by the healthcare team. These rights are regulated In Iran as the Patients’ Rights Charter, according to high level human values and Islamic-Iranian culture, as well as the principle of equality and the inherent dignity of healthcare recipients. 26 The application of this Charter is designed to lead to comprehensive consideration of patients’ rights provision and movement towards maintaining, promoting, and strengthening the relationship between healthcare providers and recipients. 27 Ethical education, especially in patients’ rights, plays a pivotal role in promoting moral sensitivity, in terms of nurses’ professional behavior. 28
Accordingly, the researcher first conducted a survey of nurses and patients, and in this survey, the content of the patient’s charter was assigned the highest score for the content to be taught; hence, its education was considered as the main educational content in this study. On completion, the scenarios were placed at the disposal of medical ethics and nursing experts, who assessed their and their content validity. After finalizing the scenarios, the virtual patient was designed by a team consisting of a graphical designer, software engineer, e-learning expert, and medical education expert. It was then given to five experts who fixed a number of bugs such as color combinations, design, hardware and software troubles. It was then given to 10 nurses as a pilot program with the opportunity to resolve any further errors and problems. The nurses enrolled in the pilot program did not participate in the main study.
After developing the scenarios and designing the virtual patient, training on the Patient’s Rights’ Charter was provided by a mentor that was a computer character in the form of an ICU nurse, and then five stimulation scenarios were presented, which focused on compliance with the Patients’ Rights’ Charter, including items on management and compliance with ethical principles, including observation of patients’ rights. Participants had to choose a response, and if the nurse chose the wrong item, that is, selected an incorrect answer, the computer character provided the necessary hints and recommendations and asked participant to choose another one. If the correct item was chosen, the participant was encouraged and the reason for the correctness of the selected option was explained to the participant by the computer character according to the provisions of the Patients’ Rights’ Charter and the participant went to the next scenario. If the correct response was not selected, the process was continued until the correct one was selected (Figure 1). Research process.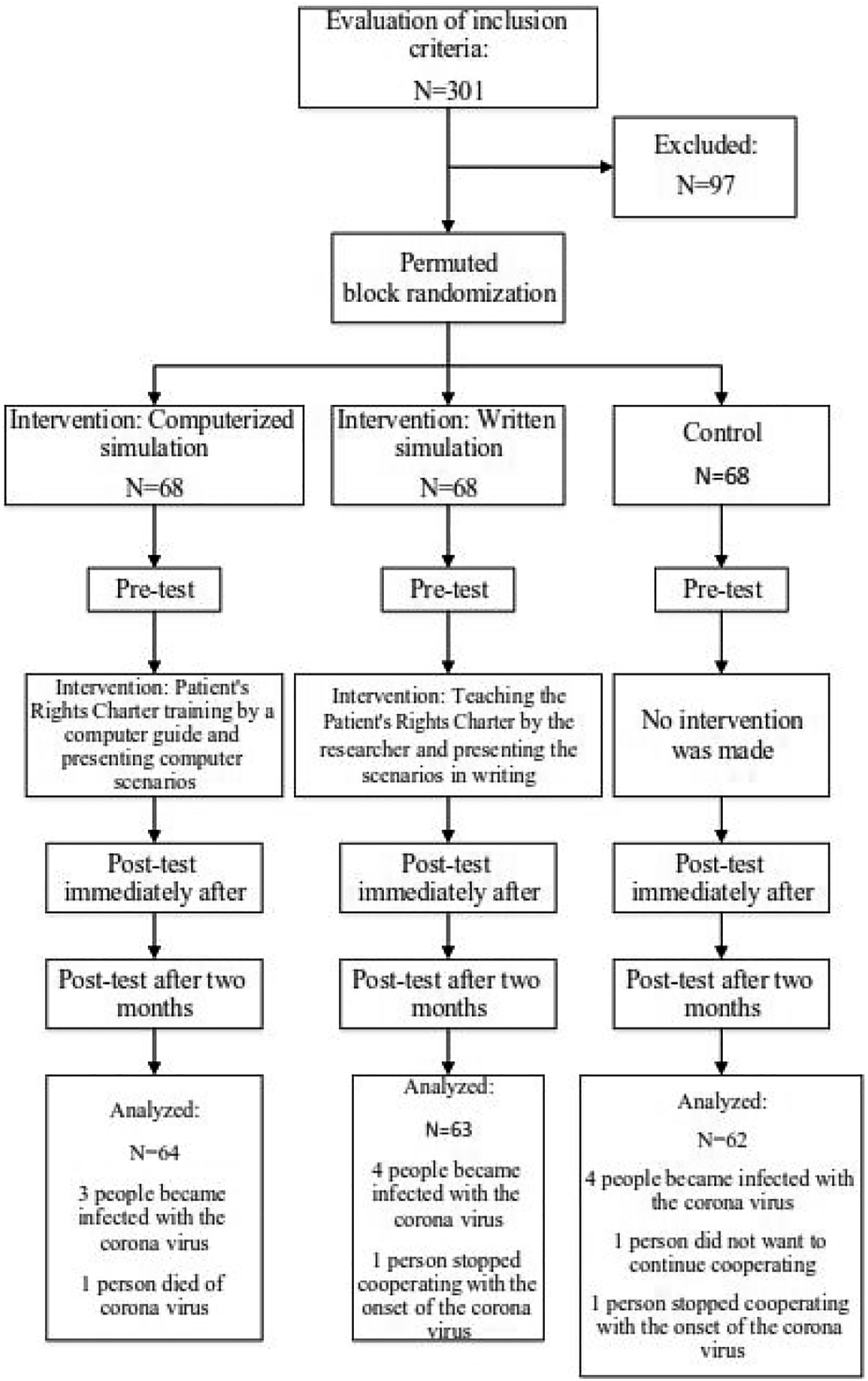
In the written simulation group, first, training on the Patients' Rights Charter was provided by the researcher, and then the same five scenarios presented as in the virtual patient simulation group with the same items were given as text to them. Again, in the case of the wrong response being selected, the necessary hints and recommendations were given to the participants by the researcher (facilitator), and when a correct response was made, the participants were encouraged and the reason for the correctness of the selected option was explained to the participant by the researcher according to the provisions of the Patients’ Rights’ Charter, and the next scenario, as a text, was presented to them. The full text of training was provided to this group.
Post-training, and 2 months after training in the intervention groups, the Lützén moral sensitivity questionnaire was completed by the participants. The control group did not receive any training, and the participants were asked to complete the Lützén moral sensitivity questionnaire before the intervention, as well as immediately and 2 months after it.
Ethical considerations
The study protocol was approved by the Ethics Committee of Tehran University of Medical Sciences (ethical code: IR.TUMS.FNM.REC.1398.062). The study was registered in the Iranian Registry of Clinical Trials at www.irct.ir (Reg. No. IRCT20111203008286N6). The study objectives were explained to the participants and informed consent was obtained for participation in the study. The contents trained for the intervention groups were also provided for the control group with written or computer simulation methods after study.
Data analysis
The Shapiro-Wilk test was used to examine the normal distribution and the Levene test to evaluate the homogeneity of variance in research groups, as prerequisites for parametric ANOVA. Repeated measures were used to evaluate the interaction of repeated measures in different groups and the effectiveness of the interventions. The Chi-square test was used to evaluate the ratios in the groups. One-way ANOVA was utilized to evaluate numerical variables and moral sensitivity scores in the study groups. All tests in the study were two-tail, and p-values < 0.05 were considered significant. SPSS version 16 was used for data analysis.
Sensitivity analysis showed that dropouts had no role in determining the significance of results. There was a significant difference between marital status and work experience in ICU in the study groups. To evaluate the degree of interference of these variables in the effectiveness of the intervention, the effect size (mean differences) of marital status and work experience in ICU was evaluated in the study groups using ANOVA, and no differences were found between the groups (marital status; p = 0.83, f = 6.5, df = 1(187)); work experience (p = 0.76, f = 2.1, df = 2(186)). Also, since there was a significant difference in moral sensitivity score among the study groups before the intervention using repeated measure ANOVA, the moral sensitivity scores were adjusted based on pre-intervention scores. These results are shown in Figure 2. Linear diagram of moral sensitivity adjusted values based on pre-intervention values in the study groups before, immediately after, and 2 months after the intervention.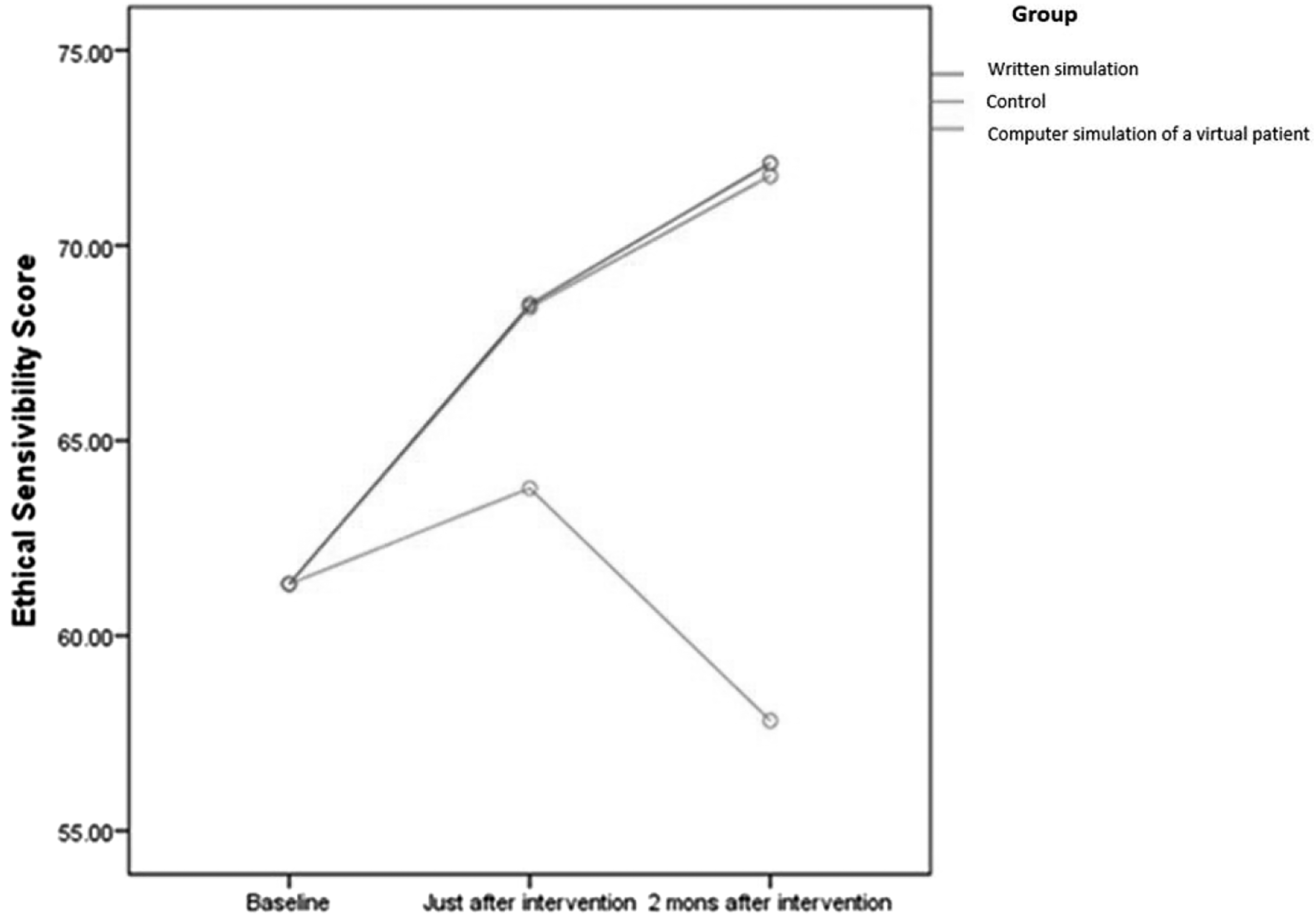
Results
Demographic characteristics of the study participants
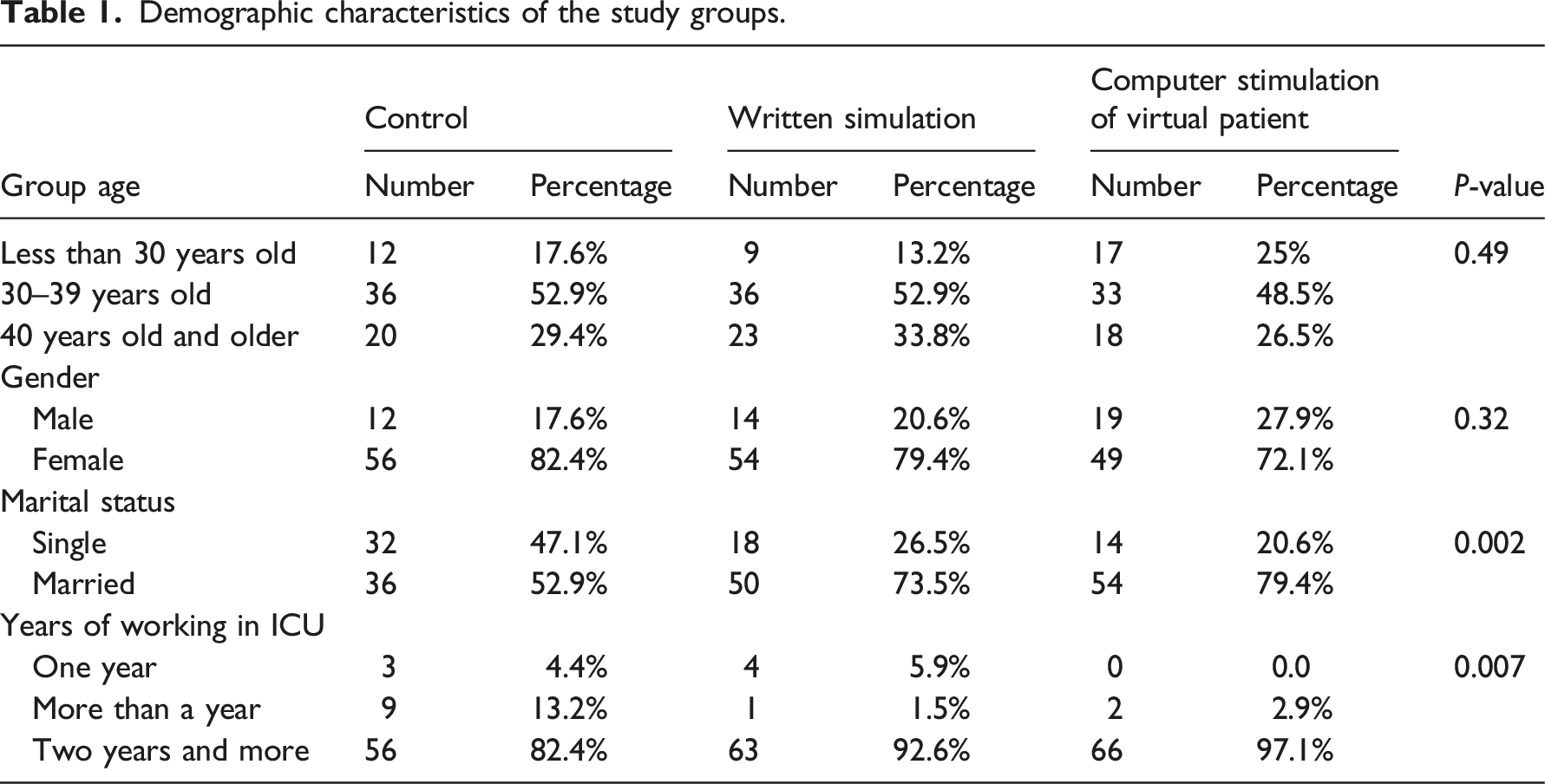
Demographic characteristics of the study groups.
The effect of training Patients’ Rights Charter through two methods of written simulation and computer simulation of a virtual patient on the moral sensitivity of ICU nurses
Comparison of mean moral sensitivity score among the control, written simulation, and computer simulation groups before, immediately after, and 2 months after the intervention.
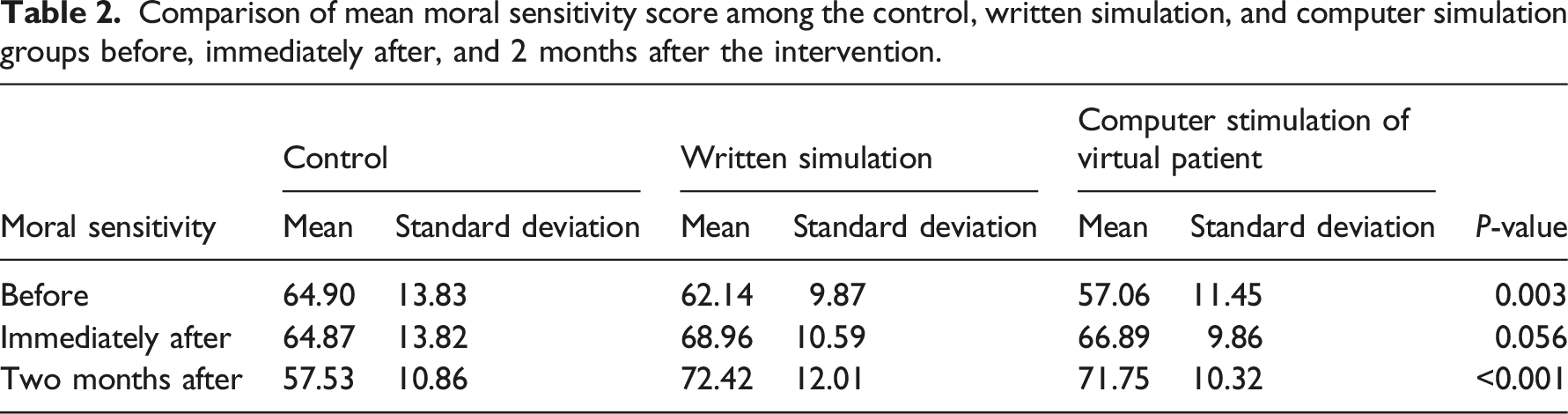
Immediately after the intervention, a slight increase was observed in the number of subjects with high moral sensitivity in the written stimulation (89.7%) and computer stimulation (74.2%) groups however there was also no significant difference in the moral sensitivity among the three groups immediately after the intervention (p = 0.232). Two months after the intervention, the moral sensitivity score decreased in the control group so that 4.5% of the subjects had low moral sensitivity (while none of them had low moral sensitivity before the intervention), and the frequency of subjects with high moral sensitivity dropped to 81.8% 2 months after the intervention in this group; in the written stimulation group, the mean moral sensitivity score decreased 2 months after the intervention compared to pre-intervention (24.1%), and the frequency of subjects with high moral sensitivity decreased 2 months after the intervention, compared to pre-intervention (79.9%).
Discussion
The comparison of the normalized mean scores of moral sensitivity among the computer simulation, written simulation, and control groups showed a significant difference between the baseline measurement and the 2-month post intervention measure in all the study groups. There was no significant difference among the three groups immediately after the intervention despite the increase in the mean score of moral sensitivity in the written and computer stimulation groups. Given that moral sensitivity is one of the ethical decision-making components, by increasing the moral sensitivity of nurses, their ethical decision-making might be improved. For this purpose, attention should also be paid to improving other ethical decision-making components-i e, moral judgment, moral motivation, and moral character. In line with the present study’s results, Kucukkelepce et al., 29 showed that the simulation method could improve moral sensitivity. The results of the study by Chao et al., 30 showed that the study population and educational topic can both have an influence on the effectiveness of the teaching method. In their study, unlike the present study, on the immediate evaluation of subjects, the intervention was found to be effective, which may be due to differences between the two studies in the study population (nursing students vs nurses in the present study) and particularly the continuation of training for 18 weeks for the student cohort, which led to greater effectiveness of their training in the assessment of moral sensitivity, at the post-intervention point. A further explanation for differences between the present study and the Chao et al. 30 study may be due to the fact that running an ethics training program as a mandatory course in nursing education, which has a final exam and requires a passing score may encourage students to put more effort into acquiring the content which is retrievable in the short term, at least. A further study 31 has indicated the importance of the appropriateness of the simulation method to the participants being taught and the target audience, which has been reinforced by the Jawaid et al. 32 study which used paper-based and computer simulation methods for moral reasoning development in medical students, and found that computer simulation performed better.
Study limitations
One of the study limitations was the concurrence of some stages of the intervention with the COVID-19 pandemic. Hence, some participants could not continue to participate and unfortunately in some cases lost their lives. The nature of COVID-19 and changes in the ICU context also affected nurses’ moral sensitivity. The researchers were unaware of the number of times the training file of the Patients’ Rights Charter was reviewed as part of their usual work practices by participants during the 2-month follow-up, which may have affected the final assessment of moral sensitivity.
Conclusion
The results of the present study confirm hypothesis #1 -i e, computer simulation of a virtual patient affects nurses’ moral sensitivity, and hypothesis #2 -i e, written simulation affects nurses’ moral sensitivity. Work pressure, psychologically and physically, is imposed on nurses by patients, colleagues, and the organization, which can lead to the exacerbation and even creation of new ethical conflicts in nurses. Moral tension is a given in these circumstances. Since intensive care unit nurses spend most of their time in patients' bedsides and are in close contact with patients and their families, they are constantly dealing with ethical decision-making, which requires appropriate moral sensitivity. E-learning methods, such as simulation, are safer ways for nurses and students to achieve their intended academic goals without compromising their health, due to advantages of stimulation of the clinical setting and treatment conditions, without the need for risking themselves by the necessity of a physical presence for their learning.
Although more realistic simulation methods are often costly in terms of design, execution and delivery, considering the potential costs of hospitalized in the intensive care unit, it may be, at this time, a smarter and more logical solution rather than traditional teaching methods to train nurses and paramedical students, where appropriate. Due to the sensitivity of ethical decision-making by medical staff and different moral sensitivity levels of healthcare team members, interprofessional training should also be considered in future studies. As there are few studies in this field, it is recommended to do more studies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.