
Abstract
Background
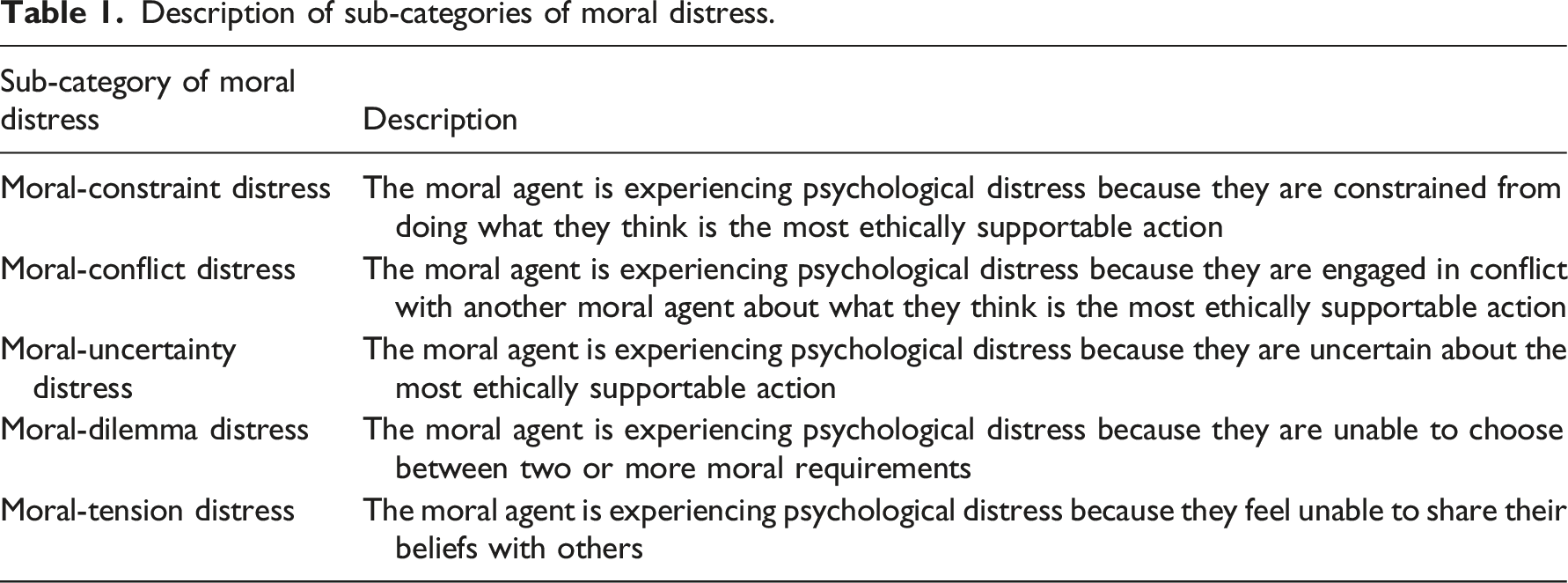
There is ongoing debate regarding how moral distress should be defined. Some scholars argue that the standard “narrow” definition overlooks morally relevant causes of distress, while others argue that broadening the definition of moral distress risks making measurement impractical. However, without measurement, the true extent of moral distress remains unknown.
Research aims
To explore the frequency and intensity of five sub-categorizations of moral distress, resources used, intention to leave, and turnover of nurses using a new survey instrument.
Research design
A mixed methods embedded design included a longitudinal, descriptive investigator-developed electronic survey with open-ended questions sent twice a week for 6 weeks. Analysis included descriptive and comparative statistics and content analysis of narrative data.
Participants
Registered nurses from four hospitals within one large healthcare system in Midwest United States.
Ethical considerations
IRB approval was obtained.
Results
246 participants completed the baseline survey, 80 participants provided data longitudinally for a minimum of 3 data points. At baseline, moral-conflict distress occurred with the highest frequency, followed by moral-constraint distress and moral-tension distress. By intensity, the most distressing sub-category was moral-tension distress, followed by “other” distress and moral-constraint distress. Longitudinally, when ranked by frequency, nurses experienced moral-conflict distress, moral-constraint distress, and moral-tension distress; by intensity, scores were highest for moral-tension distress, moral-uncertainty distress, and moral-constraint distress. Of available resources, participants spoke with colleagues and senior colleagues more frequently than using consultative services such as ethics consultation.
Conclusions
Nurses experienced distress related to a number of moral issues extending beyond the traditional understanding of moral distress (as occurring due to a constraint) suggesting that our understanding and measurement of moral distress should be broadened. Nurses frequently used peer support as their primary resource but it was only moderately helpful. Effective peer support for moral distress could be impactful. Future research on moral distress sub-categories is needed.
Introduction
Description of sub-categories of moral distress.
Research aims and objectives
The aims of this research were to examine hospital-based registered nurses (1) perceptions of frequency and intensity of sub-categories of moral distress; (2) personal and work characteristics and their association with each sub-category of moral distress; (3) resources used and their usefulness when addressing moral distress; and (4) associations between moral distress, resource utilization, intention to leave, and turnover.
Methodology
Research design
A mixed methods embedded design included longitudinal, descriptive electronic surveys, and free-text (open ended) responses to explore sub-categories of moral distress, resources used during morally distressing experiences, intention to leave, and turnover. Participants were also invited to participate in interviews and these data will be reported elsewhere.
Sample size calculations were performed based on the ability to detect moderate correlations between frequencies of different moral distress sub-categories, and to detect associations between categorized groups of moral distress frequency with other factors that included hospital site, intention to leave, and actual turnover. Since actual participation was unknown for this novel project, calculations assumed that 100 nurses would be willing to participate. With a sample size of 100, there would be 80% power to detect small to moderate correlations of at least 0.28 between frequencies of moral distress and similar power to detect absolute percentage differences of at least 28% in intention to leave and turnover between groups defined by moral distress response frequency. With our observed sample size of 80 participants with 3 or more surveys, there was similar power to detect correlations of at least 0.31 and absolute percentage differences of 31% or more for similarly defined groups. Power calculations were performed using G*Power14, and assumed use of two sided tests with significance level of 0.05.
Data collection
Registered nurses were recruited from a large, academic quaternary care medical center and three small to mid-size regional acute-care hospitals within the health system. Nursing units within each hospital were designated as sites (purposive sampling) based on nurse manager support of the research project. Registered nurses were recruited from within the designated nursing units. Potential participants received an email with an IRB approved research information sheet and information about the research at nursing unit huddles. Potential participants could ignore email requests and once recruited, could drop out of the study at any time by ignoring email requests to complete surveys or requesting to no longer receive email reminders. There were no exclusion criteria; all clinical nurses in direct patient care were included if their unit was selected for inclusion in the study. Non-clinical nurses were excluded.
Ethical considerations
This study was approved by the healthcare system institutional review board (IRB number 19-1025). Completion of surveys signified consent to participate.
Survey development
Moral distress sub-categorizations were examined using the Moral Distress Sub-Categorization Survey (MD-SCS), an investigator-developed survey. The instrument was designed with the aim of capturing the different sub-categories of moral distress longitudinally so the goal was to keep the survey as brief as possible to decrease nurses’ response burden. Each of the moral distress questions were developed to reflect the five different sub-categories that were identified in empirical research conducted by Morley et al.8,13 in the United Kingdom which followed an in-depth review of the literature. 14 For example, to capture the sub-category of moral-conflict distress, participants could choose the option “I am engaged in conflict with the team or family because of disagreement about what is right.”
Content validity was evaluated using the Lynn method. 15 Eight content experts were given information about the aim of the survey and the different sub-categories of moral distress. Content experts consisted of one professor of nursing ethics, two professors of nursing, one clinical nurse with ethics expertise and four bioethicists. They individually rated each item based on relevance, clarity and importance. The original survey contained 23 items. Following feedback on clarity and importance, the survey was reduced to 11 items. The same eight content experts provided feedback on the 11-item version. The content validity index was 0.969 which exceeded the acceptable content relevance threshold of 0.78. To assure all eleven items were clear and understandable, cognitive interviewing was completed with a clinical nurse specialist with ethics and moral distress knowledge to ensure that the questions were clear and understandable. 16 The MD-SCS was not compared to previous moral distress instruments such as the Moral Distress Scale-Revised and the Moral Distress Measure for Healthcare Professionals because the aim was to capture the different sub-categories of moral distress over time rather than the various constraints that cause distress.
Moral distress sub-categorization-survey
The final MD-SCS consisted of 11 items designed to understand themes of interest (8 items related to moral distress sub-categories and resources, and 3 items related to intention to leave and turnover). Depending on how participants responded, the survey could have been as short as 1 item or it could have encompassed the full 11 items. Questions were tiered with participants first asked to reflect upon the most recent 72 hours of work (the last 1–3 shifts of work) and state whether they experienced distress using a dichotomous yes/no checkbox. Participants were asked to recall the last 72 hours or 1–3 shifts to minimize recall bias of the phenomenon. 17 If participants selected yes, they were asked if the distress was due to clinical work using a yes/no checkbox. If participants selected no, they would be presented with demographic questions and the survey ended. If yes, participants were asked to describe the cause of moral distress. They were presented with 5 options that represented the sub-categorizations or “other.” Participants were able to choose all that applied to capture the possibility that different sub-categories of moral distress occurred simultaneously. A free text option allowed for individualization of the cause of distress. The fourth item requested that participants provide the intensity of each sub-category of moral distress on a scale from 0 (no distress at all) to 100 (most distress imaginable). A 0–100 scale was utilized to capture breadth in responses. Two items of the survey captured healthcare system resources that participants might seek to use when experiencing different sub-categories of moral distress. Participants were provided with a checklist of resouces (for example, speaking with colleagues, using an employee assistance program, consulting the ethics consultation service (ECS) or palliative medicine) that could be used to address each cause of moral distress they selected. A free text option was provided to allow for resources that were not prepopulated. After participants selected a resource or support service, they rated it based on how helpful it was in mitigating moral distress, on a scale of 0 (not helpful at all) to 100 (extremely helpful). The final two items on resources and support services were free text that asked participants to explain why they didn’t access support services (when applicable) and if another service could have helped.
Intention to leave and turnover
Three items were developed by investigators to address intention to leave and also the influence of moral distress on turnover. Participants used fill-in-the-blank to show how long they saw themselves working on their current unit, hospital and in the nursing profession. Then, participants were asked about whether they were considering leaving the unit because of moral distress (dichotomous yes/no checkbox) and they used free text, as desired, to describe their reasons for intending to leave.
Turnover was captured in follow-up surveys. Participants completed a 2-item survey at 3, 6, and 12 months that asked if they worked on the same or a different unit and they were able to explain why via a fill-in-the-blank box. If a participant’s email was no longer active, the participant was no longer an active employee, as email addresses are removed immediately after service departure.
Participant demographics
Six nurse characteristics were collected at baseline, midpoint, and in the final survey using fill-in-the-blank or a drop down option list: highest nursing degree; length of time as a nurse (overall), on the current unit and within the healthcare system; gender; work shift; and if the ethics team rounded on the unit.
Data collection
Data were collected and stored using the REDCap database system, a secure, HIPAA compliant web-based program designed for building and managing web-based projects that is password protected. A research information sheet was emailed electronically to nurses who met the inclusion criteria. The information sheet contained a direct link to the electronic survey. At the end of the initial survey, participants were asked to provide their email address to receive surveys longitudinally, twice a week for six weeks. When nurses supplied their email via REDCap, longitudinal surveys were automatically emailed at the scheduled time point. Participants had the option to ignore requests or complete one or more surveys during the 6 weeks follow-up period. Participants could opt-out by sending an email request to the principal investigator. Survey responses were connected to each email address; and emails were visible to the principal investigator but not to other investigators; thus, participants’ identities were confidential. Data were collected from November 2019–January 2020.
Data analysis
Categorical variables were described using frequencies and percentages, and continuous variables were described using means, standard deviations, medians, minimum and maximum values. In analysis, data were grouped based on the causes of moral distress and resources used, and frequencies and percentages were calculated. Comparisons between groups were assessed using Kruskal–Wallis tests for ordered variables, or Fisher’s exact tests. When overall comparisons were significant, pairwise comparisons were run. Analyses of non-free text responses were completed using SAS® Software (version 9.4; Cary, NC).
Free text responses were analyzed using content analysis, guided by Vaismoradi et al. 18 This approach provided a process for legitimately quantifying qualitative data without requiring close attention to context to build understanding, since context for responses is not available in short free text survey responses. 18 This approach required reading and re-reading the data, creating groupings and categories and identifying themes. 18
Results
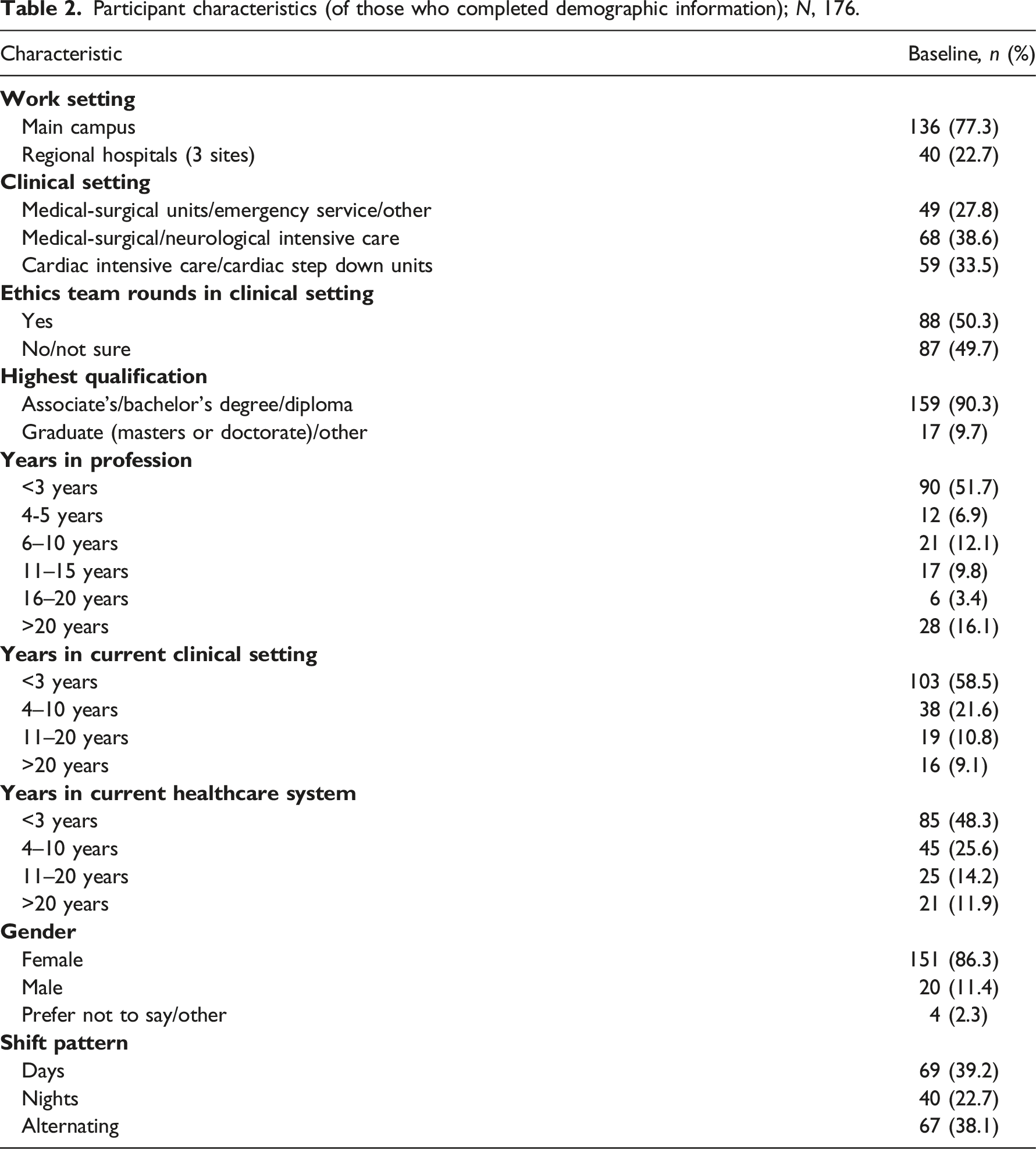
In total, 246 nurses completed the baseline survey and 176 (71.0%) participants provided demographic data. Of baseline responders, 86.3% were female and the majority worked at the quaternary care hospital (77.3%); 38.6% worked in medical-surgical or neurosurgical ICU. Other characteristics of baseline survey responders were that most had a bachelor’s degree (90.3%) and around one-half had 3 years’ experience as a nurse on their current unit and in the health system. Most nurses rotated shifts and one-half reported that the ethics team rounded on their unit.
Participant characteristics (of those who completed demographic information); N, 176.
Moral distress frequency and intensity by sub-categories
Sub-categories of moral distress, distress frequency, and intensity at baseline and 3 of more surveys completed*.

*Intensity was measured on a 0–100 scale.
In total, 80 participants completed 3+ surveys over the 6 weeks data collection period. By frequency, moral-conflict distress occurred the most often (51.3%), followed by moral-constraint distress (42.5%), and moral-tension distress (36.3%). Moral-uncertainty distress (15.2%) and moral-dilemma distress were experienced with the same frequency (31.3%). By intensity, moral-tension distress and moral-uncertainty distress ranked highest (see Table 3).
Resources used when experiencing moral distress
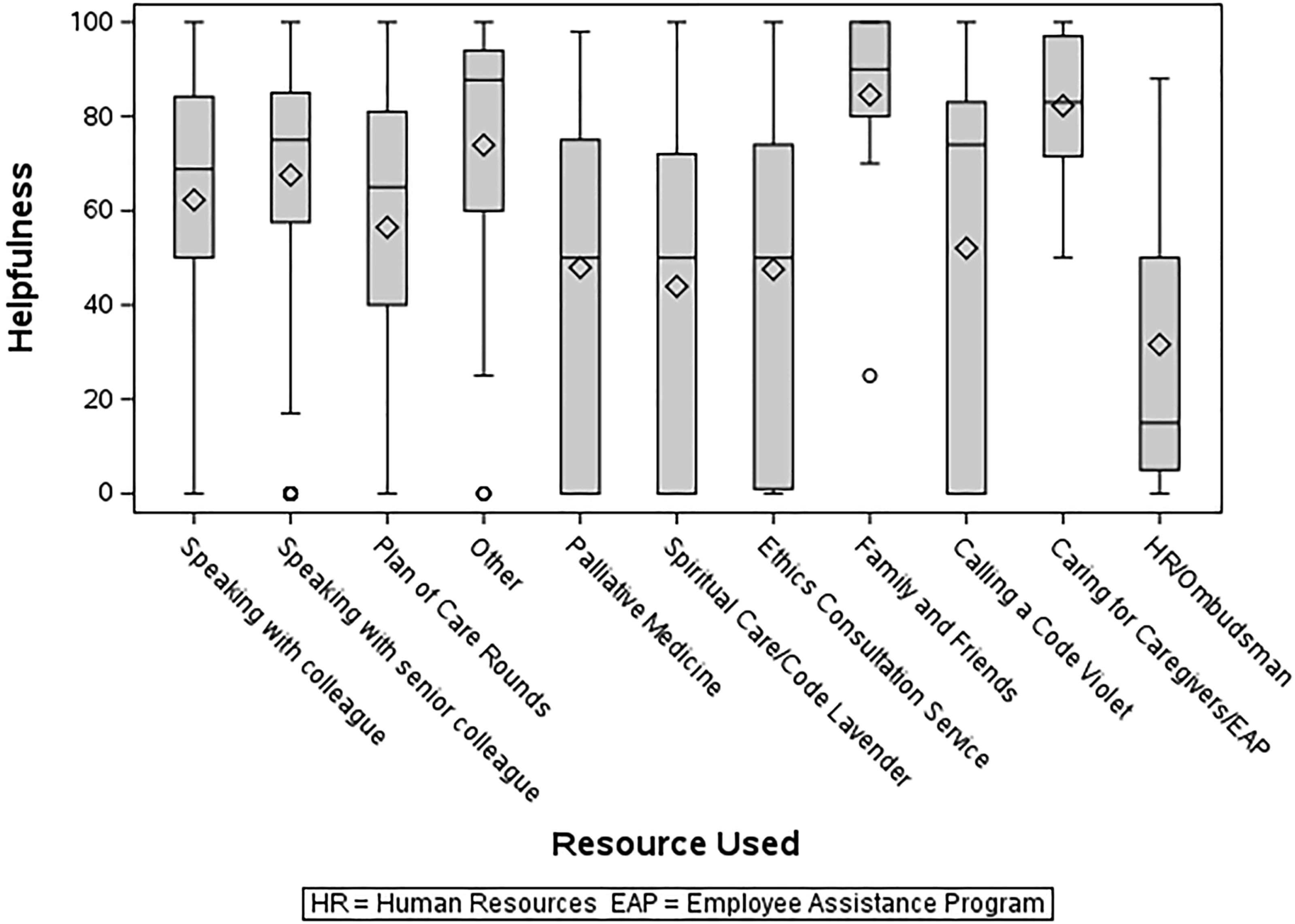
Of the overall sample of participants, 12 resources including an “other” free-text response were utilized to different degrees by participants. Of resources selected, speaking with a colleague or a senior colleague occurred most often. Services that involved communicating with non-collegial personnel such as the employee assistance program were used less often (see Figure 1). Of resources selected, ratings of helpfulness varied (see Figure 2). For example, although the employee assistance program was rarely used, participants rated it as highly helpful. Among nurse participants who experienced moral-uncertainty distress, the most frequent resource was speaking to family and friends (14%), followed by plan of care visits (7%). Nurse participants who experienced moral-constraint distress and moral-tension distress most frequently reported not using any resource (8.7%; 16.9%). Half of the sample indicated that ethics rounded on their units, and half stated no/not sure with free text responses stating that they worked predominantly night shift. Given that all of these rounds occur during day shift, this suggests that many participants were aware of ethics round. Frequency of Resources Used at Baseline (N, 176). Helpfulness of Resources Used at Baseline (N,176).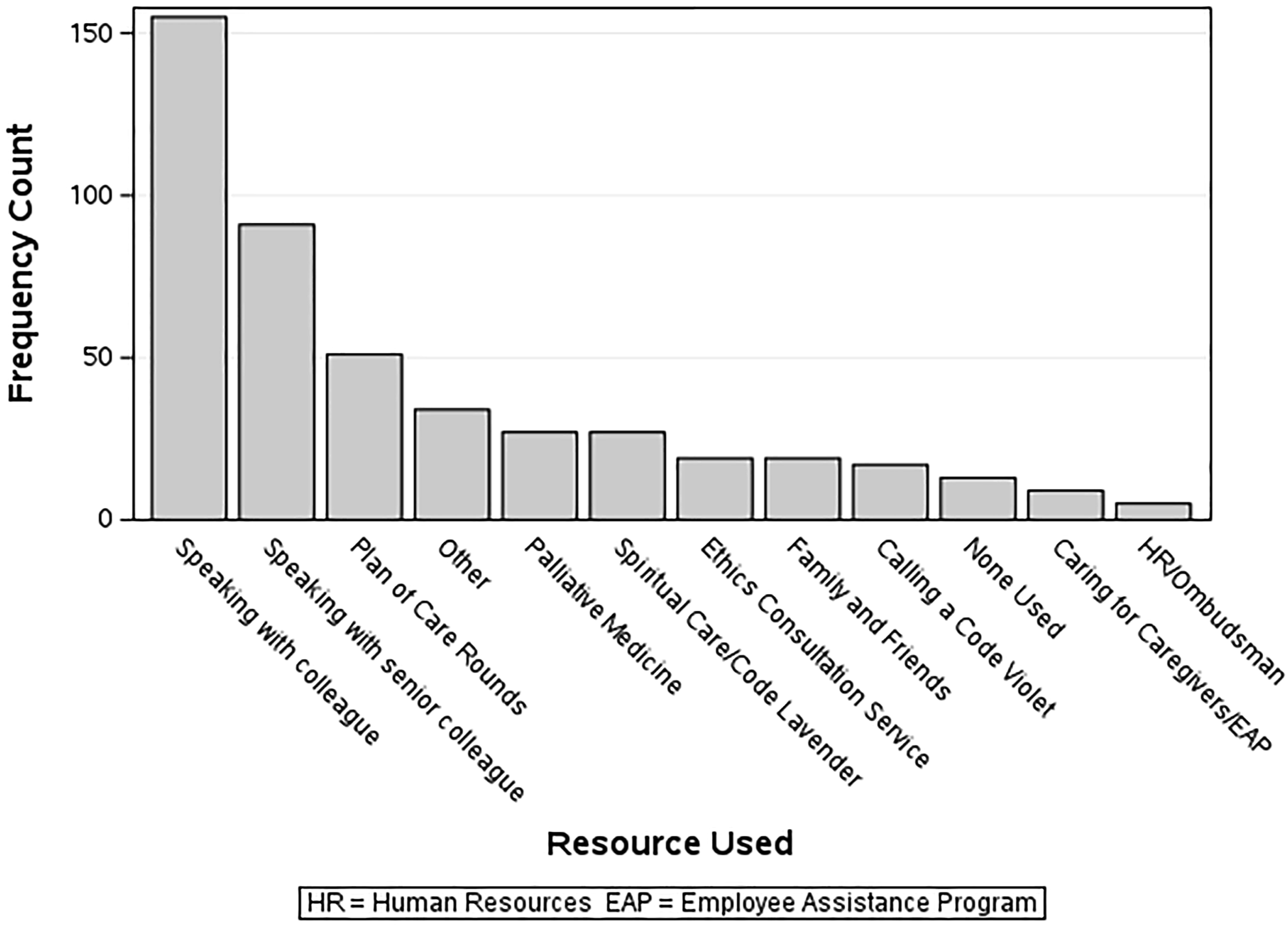
Moral distress sub-categories and resources used based on nurse and unit characteristics
There were three statistically significant findings when conducting stratified analysis of moral distress sub-categories, resources used, and nurse and unit characteristics. During moral distress episodes, participants who spoke with a colleague or senior colleague were less likely to work at the hospital system’s main campus (p = 0.048), in the surgical ICU (p = 0.013) and night shifts (p = 0.014). Within the moral distress sub-category, those who spoke with a colleague or senior colleague when experiencing moral-dilemma distress were more likely to identify as female (p = 0.019). After adjusting for multiple responses per subject, female gender continued to be associated with using colleagues or senior colleagues when experiencing moral-dilemma distress (p = 0.019).
Intention to leave and actual turnover based on moral distress sub-categories, resources used, and support services
Intention to leave and actual turnover.
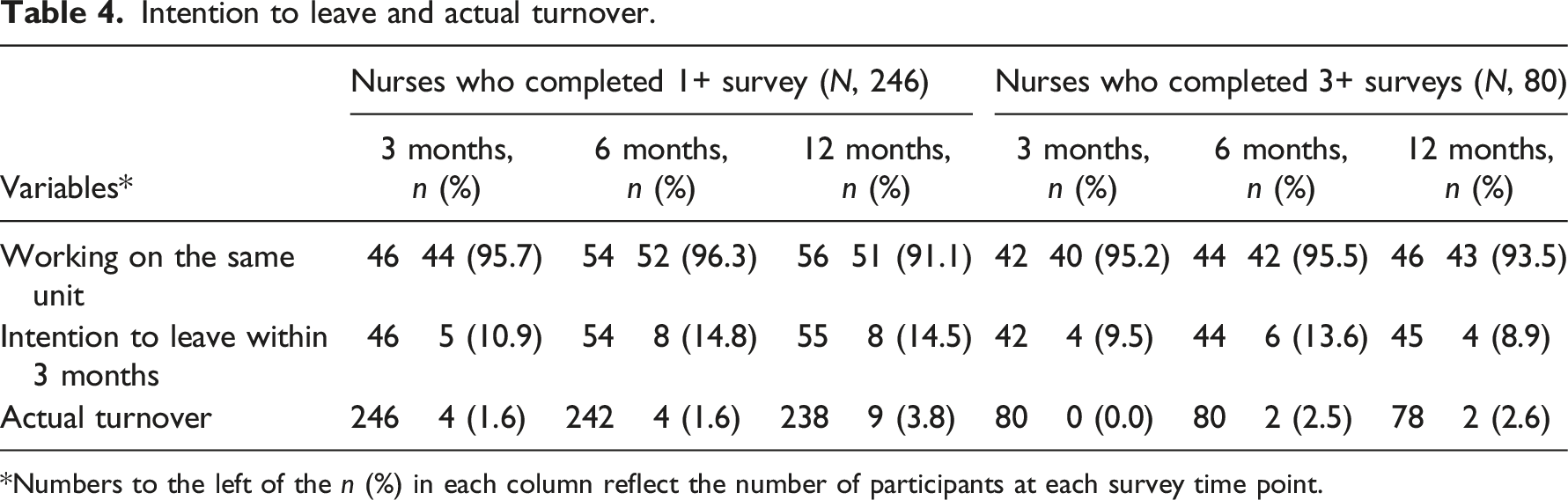
*Numbers to the left of the n (%) in each column reflect the number of participants at each survey time point.
Free text responses
Themes from free-text responses.
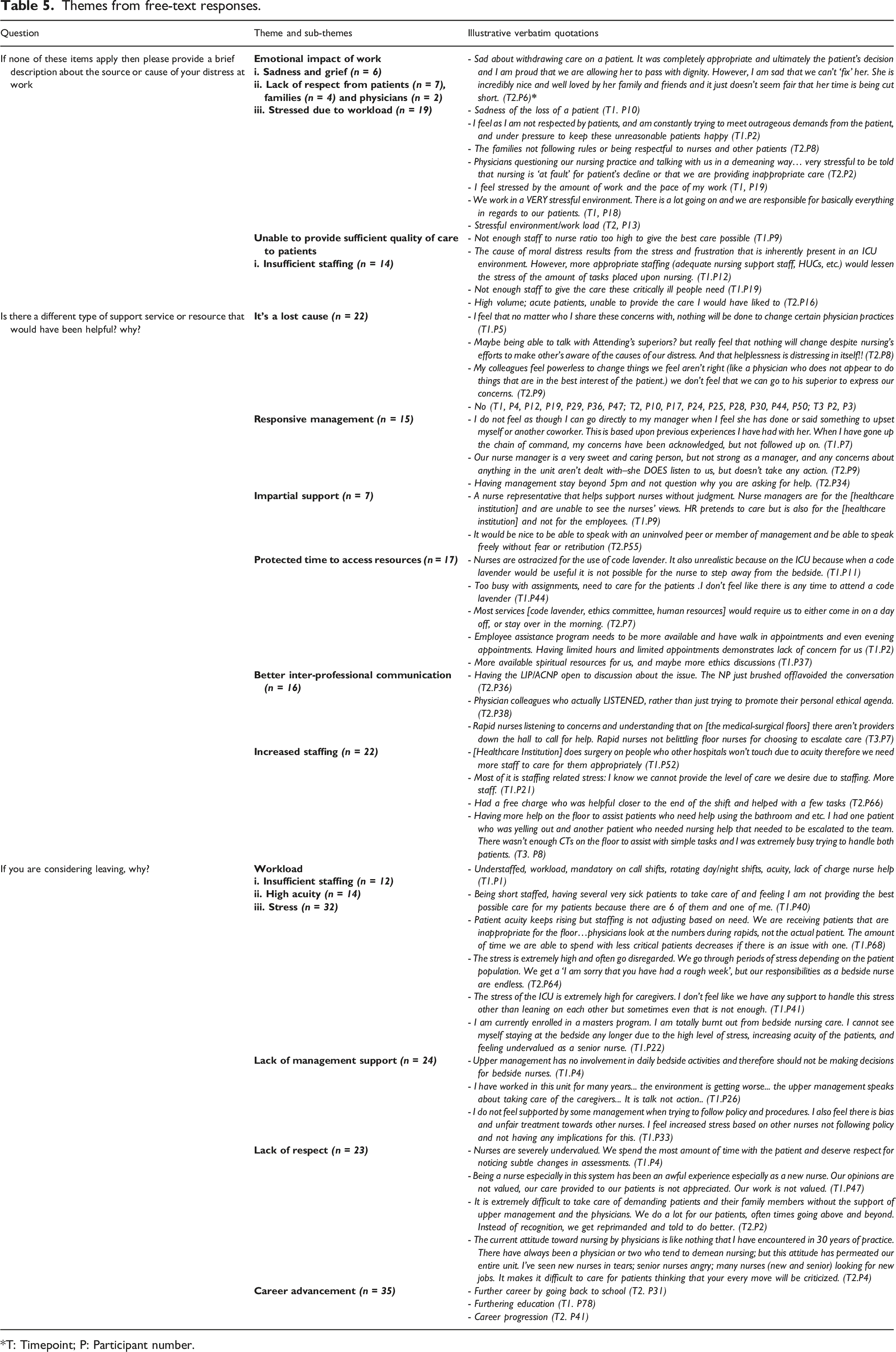
*T: Timepoint; P: Participant number.
Discussion
The primary focus of this research was to understand the frequency and intensity of sub-categories of moral distress that were previously identified in qualitative research. 8 Nearly one-half of nurse participants reported experiencing moral-conflict distress at baseline and this sub-category also ranked as the most frequent type of moral distress among nurses who completed three or more surveys. The second most frequent sub-category of moral distress at baseline was moral-constraint distress and this sub-category ranked as the second most frequent among nurses who completed three or more surveys. These results were important since moral-constraint distress represents the traditional narrow description of moral distress. Our findings substantiated that some sub-categories of moral distress had a high prevalence and were more prominent than is represented by the narrow definition. Importantly, in our survey, participants did not need to know the right thing to do when experiencing a constraint, rather, they responded if they felt unable to do what they believed, thought, or felt to be right. We intentionally utilized this wording because it was previously suggested that knowledge of the right thing is too high of an epistemic threshold for moral-constraint distress to occur. 19
At baseline and among participants who completed three or more surveys, moral-tension distress was the sub-category that was the most intensely felt, even though it occurred less frequently. This is an interesting finding since this sub-category of moral distress was first identified by Morley et al. 8 Moral-tension distress occurs when an individual feels unable to share their beliefs with others. It is therefore likely to be important to nurture an environment in which nurses feel more able to articulate their moral perspective in order to mitigate this sub-category of moral distress.
There were wide standard deviations among mean moral distress sub-category scores indicating variability of occurrence. This finding was not surprising given that moral distress is a subjective phenomenon that impacts individuals differently. The subjectivity of moral distress makes it a challenging phenomenon to capture and a clear limitation of this survey is that participants could have different scenarios in mind when responding to the moral distress questions. Free text responses provided insight into the morally distressing scenarios that participants did not think were captured in the sub-categories of moral distress proposed. Some of the free text responses mapped onto items already listed in existing moral distress measures. For example, feeling unable to provide high quality care due to insufficient staffing could reflect the item “Working with unsafe staffing levels” on the Moral Distress Scale-Revised, 20 or “Experience compromised patient care due to lack of resources/equipment/bed capacity” on the Measure of Moral Distress for Healthcare Professionals (MMD-HP). 22 Some scholars may question, therefore, whether a new moral distress measure is needed when the Moral Distress Scale-Revised is valid, reliable and has been used internationally,20,23,24 and the newer MMD-HP shows promising validity and reliability. 22 There are three significant critiques of current moral distress scales: that they fail to generate participant responses representative of the clinical and ethical situation25,26; perpetuate the assumption morally distressed individuals have correctly assessed the ethically supportable pathway 12 ; and scale items do not prompt the ethical reflection required to address moral distress.25,26 In addition, these scales focus on constraint-based moral distress only. The approach used in this study to capture five sub-categories of moral distress may enhance diagnostic capability and lead to more specific testing of interventions. In our findings, some free-text responses could have been re-categorized as moral-constraint distress, but others were representative of moral-conflict distress, such as conflicts about the plan or care, and improvements in inter-professional communication. Kolbe and Melo-Martin 25 argued that moral distress measures and tools would have more utility if they took a diagnostic approach that provoked participants to critically consider the current constraints in place. One future direction for the MD-SCS is to repurpose it as a database repository of real-time, longitudinal morally distressing situations that can be assessed. Alternatively, the questions could provide real-time capture with prompts for reflection or identification of next steps.
Other scholars developed surveys designed to capture moral distress in real-time that have utility for pre-post intervention testing, such as Wocial and Weaver’s Moral Distress Thermometer. 27 However, use of real-time surveys that measure the intensity of sub-categories of moral distress can raise questions about the possibility of a threshold point that requires response or intervention. In our study, the “other” sub-category of moral distress tended to have a high intensity when it occurred; thus, a real-time approach may create recognition of situations that require immediate attention, such as a high workload and feeling unable to provide sufficient quality of care to patients.
With regard to specific resources, participants indicated utilizing peer supports (colleagues/senior colleagues) most frequently, which were moderately helpful. If peer support were optimized, it could be a more effective resource. Though peer support is gaining popularity as a support mechanism for healthcare professionals experiencing second victim phenomenon and other stressful experiences, 28 it has not been well studied in relation to moral distress. Recently, ethics education programs emerged that combined elements of peer support into their curriculum,29–32 but the peer support element needs to be directly explored in future research.
About a third of participants described using daily, multidisciplinary “plan of care rounds” as a resource. During rounding, the plan of care should be discussed and formulated in partnership with the patient, family and nurse. Patient and healthcare team-focused rounds have the potential to increase inter-professional communication and decrease epistemic injustices between team members that occur when nurses are not involved in formulating the plan of care, or informed of the reasoning behind specific plans. 33 Epistemic injustice has been recognized as a cause of moral distress that occurs when nurses are not recognized as credible sources of knowledge (testimonial injustice) or when nurses are prevented from understanding their own social experiences (hermeneutical injustice).33,34 Optimization of daily rounds, via collaboration of all parties involved, may mitigate occurrences of sub-categories of moral distress.
Since about 50% of participants reported that professional clinical ethicists rounded on their ICU during the data collection period, it was surprising that so few nurses stated that they contacted the ECS when they experienced moral distress, and also, that the ECS ranked low in helpfulness. In a quality survey, over 90% of ECS users (n = 84; physicians, nurses, social workers, case managers) found the guidance they received to be helpful in addressing ethical issues in patient care. 35 Our research findings raise questions about nurses’ perceptions of the utility of ECS to address moral distress. Future research might provide new insights and interventions surrounding ECS structures, systems or processes. In a national survey of ethics practitioners, Fox et al. 36 reported that ethics consultation was effective to reduce moral distress expressed by staff, patients, and family members involved in ethics consultation. Fox et al. 36 acknowledged substantive limitations of recall bias and perceived impact on another person’s experience. Based on nurses’ perspectives of the ECS from our research, it will be important to learn if some practitioners have an over-inflated sense of their ability to mitigate moral distress or if there are common practices that all ECS should adopt to more effectively address the sub-categories of moral distress.
Once sub-categories of moral distress have been identified, interventions can be assessed for their value. In one report, authors built a Moral Distress Consultation Services (MDCS), separate to their ECS, based on the work of Hamric and Epstein. 37 The American Society for Bioethics and Humanities 38 recommends an ethics facilitation approach to ECS in which an ethics consultant (usually an individual consultant) follows a number of process steps to clarify the ethical issue, identify a range of ethically appropriate options and provide supporting rationale, which is often provided in the electronic medical record. In contrast, MDCS is a form of ethics support offered to a group of individuals who are provided with a safe space to share their experiences of moral distress. Two individuals, a facilitator and scribe lead the consult session. The facilitator promotes discussion of the patient or system issue with the group, and the scribe makes notes and produces a report that is shared internally, not in the medical record. Advantages of MDCS is that nurses and other stakeholders who may not have an opportunity to engage in ethics consultation can share their experience of moral distress, and systems issues that contribute to moral distress can be addressed. However, the creation of two distinct consult services may create confusion for stakeholders. Morally distressed individuals may believe that there is no mechanism to address their moral distress outside of a group process and discussion of moral distress that is not constraint-based 39 may not be recognized since some sub-categories of moral distress identified in this study are not typically included. Based on resources, an ECS that is well-integrated into the clinical setting, responsive to stakeholders, and that integrates additional mechanisms and approaches into consultation to address moral distress may be better positioned than a separate consult service. The approach selected will most likely depend upon current institutional structures. Regardless of the approach selected, the impact on sub-categories of moral distress will require more research.
Of resources used by clinical nurses in this study, the Employee Assistance Program was seldom used but it was the most helpful resource. Conceptualizing moral distress as the psychological distress that is causally related to a moral event may enable individuals to more clearly disentangle their emotional response from the underlying cause of distress. Mitigating moral distress may require focused support that addresses the psychological distress (such as mental health support) and the moral event (such as ethics support). To better understand if this is a promising approach, more research is needed.
Actual turnover of clinical nurses was not reported in other papers that assessed moral-constraint distress; however, our findings on intention to leave were similar to that of Whitehead et al. 20 and Epstein et al. 22 who reported that 20% or fewer nurses considered leaving their workplace and under 17% reported leaving a previous position. It is unknown if our low actual turnover was due to nurses being personally committed to their hospital and unit, the large number of potential work opportunities available across the health system, employee benefits, work-related friendships, or other reasons, despite the prevalence and intensity of moral distress. Further research is needed to understand the relationship between the different sub-categories of moral distress and actual nurse turnover.
Study limitations
This research was conducted in a single healthcare system so more research utilizing this survey in other contexts is needed to better understand the generalizability of the results. Nursing units included in the study had a significant likelihood of nurse moral distress since the sample included high acuity areas such as critical care and emergency departments, which have previously been units in which moral distress occurs. 40 Therefore, findings related to the frequency and intensity of moral distress may be higher than would be found if other, potentially less acute units were included. Participants could indicate that they had experienced more than one sub-category of moral distress and had used more than one resource to address their distress during each occurrence. The survey was designed in this way since the sub-categories and resources are not mutually exclusive but this prevented us from conducting analysis to understand if specific resources were more or less helpful in relation to specific sub-categories of moral distress. Furthermore, the ability to check multiple moral distress sub-categories and resources led to wide standard deviations around the mean scores. We did meet our minimal sample size expectations but a larger sample size would allow for more responses in each category and provide more detail about characteristics of nurses and their work sites in relation to moral distress sub-categories. Finally, because we sent out the survey and electronic information sheet via email there is no way to know how many potential participants actually opened the email and saw the opportunity to participate making it impossible to know the response rate.
Conclusion
Among nurses who participated in this study, they indicated experiencing distress due to morally relevant causes beyond constraint. In free-text comments, nurses described a number of issues that might be considered to cause moral-conflict distress such as feeling disrespected by various stakeholders. Nurse participants indicated the need for more support to improve inter-professional communication. There is a need to put interventions in place that reduce moral-conflict distress experienced by nurses; especially programs that enhance communication between healthcare professionals and assure that all providers of patient care have the same understanding related to patients’ plans of care. Further research is needed to understand whether findings of this study are replicated outside of one healthcare system and also, by healthcare professionals in different healthcare settings, especially related to the frequency of moral distress by sub-category. Future research is also needed to understand whether nurses experiencing the different sub-categories of moral distress regard specific interventions to be more, or less, useful.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was Internally funded.