
Abstract
Abstract
Most studies pertaining to the returns to education literature focus on estimating benefits of education that accrue to the individual who spends more years in school. However, from a public policy perspective it is crucial to understand the gains of education to the society at large. This study is an attempt to estimate these social returns to education, that is, the impact of an increase in average education on individual health outcomes. In particular, we try to assess if (above and beyond individual educational attainment), average years of schooling at a district level has an impact on individual health. We obtain individual level data from two rounds of the India Human Development Survey (IHDS) and calculate district level average education using data from the National Sample Survey Organisation (NSSO) surveys for the same years. We use a logit model to estimate the probability of suffering from short-term morbidity and find that there is a strong negative association between short-term morbidity and average education. We also study the impact of average education on health seeking outcomes such as consumption of cigarettes and tobacco. We find that after accounting for individual education and income, the average education at the district level has a strong positive influence on better health seeking behaviour. The results from our study lend support to the notion that in addition to policies aimed at improving healthcare, an increase in average education can potentially lead to improvement in health outcomes.
Keywords
Introduction
Returns to education measure the monetary and non-monetary benefits earned due to increased years of schooling. While most studies look at private returns to education, that is, benefits from education that accrue to the individual who spends more years in school, there is now a growing interest in estimating the social returns to education. These are benefits that accrue to society at large as a result of individuals spending more years in school. This article contributes to this strand of literature by focusing on a relatively less explored dimension of social returns to education, which is the impact of average education on individual health. Research has shown that increase in average education can benefit societies over and above the direct effects of individual education. Since Indian independence, several central government initiatives like the District Primary Education Programme, Sarva Shiksha Abhiyan and more recently the Right to Education Act have targeted increasing accessibility to schools, especially for children aged 6–14 years, thereby contributing to a long-term increase in average education. However, identifying the magnitude and form of the social return to education is crucial for determining optimum public investment in education.
Social returns to education typically study the increase in monetary or non-monetary outcomes caused due to an increase in the average level of education in a community. Average education could either be a simple mean of years of schooling (Acemoglu & Angrist, 1999) or a share of college graduates in a given population (Moretti, 2004). Both studies use the US census data to study the increase in individual wages caused by an increase in average education. Among studies that estimate social non-monetary returns to education, Lochner and Moretti (2004) find that an increase in education has a negative impact on crime rates. Similarly, Dee (2004) and Milligan, Moretti, and Oreopolous (2004) show that increase in education generates substantial increase in likelihood of voting. Surprisingly, despite large potential gains, only few papers explore the issue of social returns to education in the context of developing economies (see Fan, Ma, & Wang, 2015; Liu, 2007).
Returns to Education in India
In the Indian context, Tilak (1989) finds that individuals from higher income groups earn a higher rate of return to any level of education. He suggests that investments in education targeted specifically towards the poor, may be preferred to overall investment in education. More recently, Duraisamy (2002) estimates the returns to education by age-cohort, gender and location using the data from the National Sample Survey Organisation (NSSO) surveys. He finds that there is considerable inequality in returns to education between male and female, lower caste and upper caste workers in India. Singari and Madheswaran (2016) use the first round of the India Human Development Survey (IHDS) and find that income levels increase with educational level.
Using 25 years of national sample surveys, Fulford (2014) is one of the first papers to estimate social as well as private monetary returns to education in India. Deviating from the standard literature, 1
Returns to education are typically estimated as increase in income levels caused due to increase in education.
This article is one of the first attempts to study health as a form of social non-monetary return to education. A person’s education has been theoretically and empirically established to be one of the strongest determinants of individual health. An individual who is highly educated earns higher wages, works in a secure environment and is aware of factors that contribute to better health outcomes (Zimmerman, Woolf, & Haley, 2015). Similarly, at a household level there are studies that show (Currie & Moretti, 2003) that mother’s education is a significant determinant of a child’s health. However, is there any relationship between individual health and average education? Can the community you live in influence your health outcomes?
There are two channels through which average education can influence individual income (Moretti, 2004): (a) knowledge sharing and skill formation through formal and informal interactions may generate positive externalities across workers (Lucas, 1988) and (b) spillovers from education may arise through search externalities, that is, firms will make hiring decisions based on average education of the workers in an economy (Acemoglu, 1996). In the context of health outcomes, increase in average education could facilitate the sharing of knowledge on type of treatment, tips to avoid illnesses or information on health insurance. A higher average education would also lead to higher ability among the population at large to follow prescriptions, or use small-scale devices such as nebulisers or blood pressure machines within the household, thus improving health outcomes.
Health as a Form of Social Non-monetary Return to Education
Using this theoretical background, we try to understand if there is any relationship between average education and individual health. Average education in this context has been defined as the mean of years of education of the population in a district. This indirectly influences the type of schools, shops, infrastructural facilities and public spaces that come up in an area. In a community with higher average education, we would expect parents to be motivated in vaccinating their children and children being taught to maintain basic hygiene standards. On the other hand, in a society where literacy rates are poor and awareness is low, mothers are not necessarily competent enough to provide the right nutrition for their children. However, if there is indeed an association between average education and individual health, we expect an illiterate mother to ensure good health of her children as she sees her neighbours doing the same.
To test our hypothesis empirically, we pool information from the IHDS, a nationally representative survey conducted during 2004–2005 and 2011–2012. The survey covered 41,554 households during the first and 42,152 households during the second round with 150,988 individuals being interviewed across both the waves. Pooling the surveys together yields 301,976 observations. From the individual component of the data, we extract information on individual health, income, education levels and other demographic details. The survey categorises individual health condition into (a) short-term morbidity (STM), (b) major morbidity, (c) daily activities and (d) health behaviour. Of these, we study the impact of average education on incidence of short-term morbidity 2
The respondents were asked whether they suffered from a particular STM in the last 30 days. The responses were coded by a binary variable which we use as the key outcome variable.
Health behaviour is represented by questions asked on whether anyone in a household smokes or chews tobacco, or drinks alcohol. The responses are ordered as: never, sometimes and daily. We transformed each health-related variable into a binary variable while calculating the corresponding probability of occurrence of that outcome variable.
We derive average education levels from the NSSO surveys and combine this with health-related information from the IHDS, at the district level. 4
We have used the standard measure for average years of education, whereby we denote each level of education by the following years of education and then compute the average across individuals in every district: not literate = 0; literate without formal schooling = 0; literate but below primary = 0; primary = 3; middle = 7; secondary = 10; higher secondary = 12; diploma/certificate course = 15; graduate = 16 and postgraduate and above = 18. We compute average education levels for 517 districts.
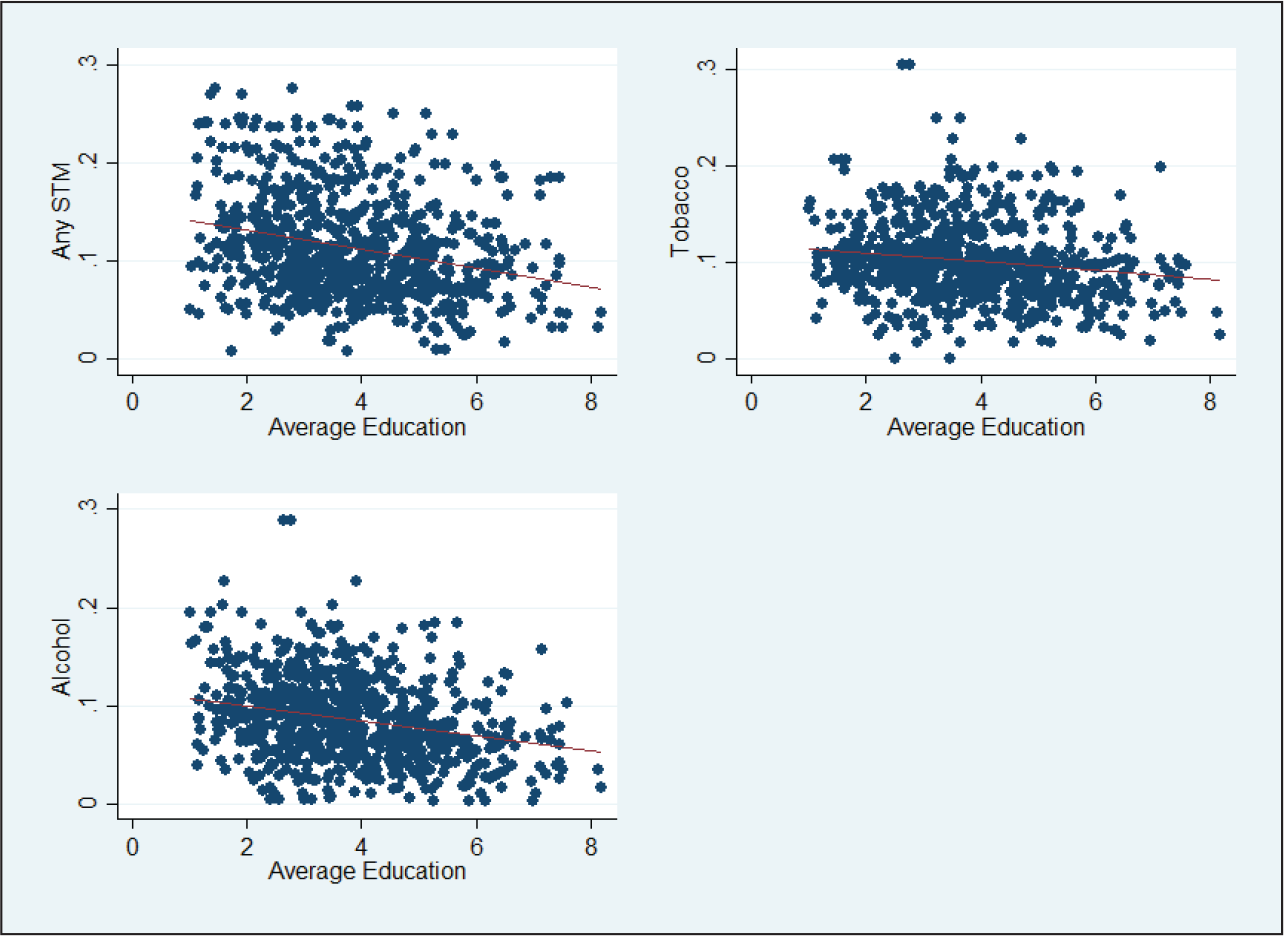
We define social non-monetary return to education as the impact of average education on short-term morbidity and health behaviour. Simply eyeballing the data, we see a negative relationship between average education and health outcomes in both survey rounds (Figure 2), which is in line with our expectations. To test the relationship empirically, we estimate a logit model. The primary challenge in addressing this causality is isolating the impact of average education on health, given the myriad list of other factors that may simultaneously influence health conditions. To address this issue, we control for factors such as income, caste, religion and availability of health infrastructure.
Our logit model results establish statistically significant positive effects of the district level average education on individual health conditions (Table 1). We find that holding other factors constant, the odds of suffering from short-term morbidity are lower if the average education in the district is high. Our models with robustness checks show that after controlling for all relevant factors, a year increase in the average years of schooling in a district, the expected change in suffering from short-term morbidity reduces by about 28 per cent for diarrhoea, 16 per cent for cough with short breath and 13 per cent for fever. Similarly, a year increase in the average years of schooling in a district is likely to reduce the tendency of an individual’s smoking tobacco by about 7 per cent, chewing tobacco by about 6 per cent and drinking alcohol by about 5 per cent. We test the robustness of our findings by controlling for health infrastructure variables also.
The potential effects on health behaviour appear less than the effects on short-term morbidity. This could be attributed to the links with behavioural aspects which take time to change. Irrespective of the magnitude of the potential effects, our estimates reconfirm the fact that not only individual education but also community level educational attainment can directly affect health outcomes of individuals.
Logit Regression Results Using Short-term Morbidity and Health Behaviour
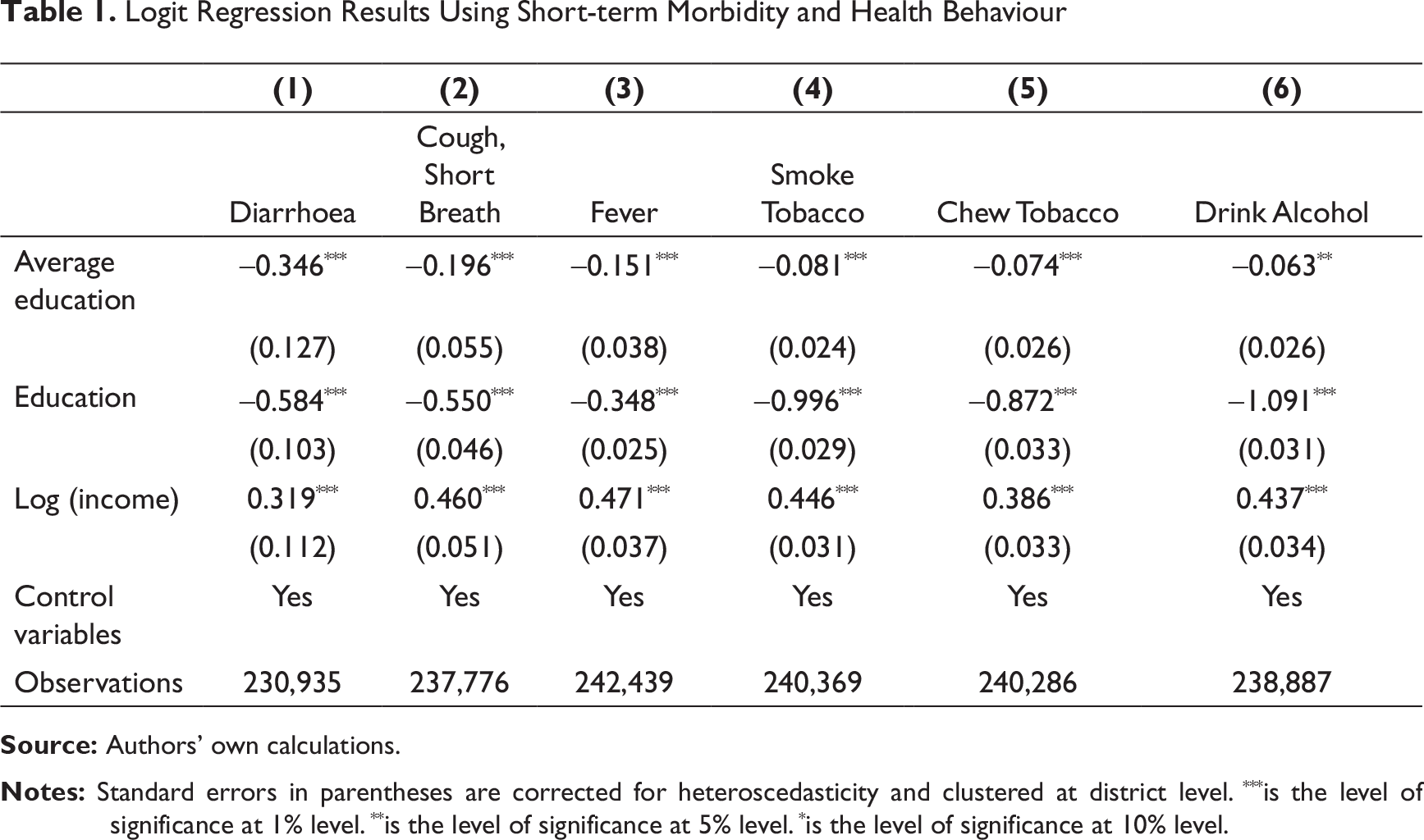
The dependent variables in columns (1)–(3) take a value of 1 if the respondent suffered from any of the corresponding diseases in the past month and 0 otherwise. In columns (4)–(6), the dependent variable takes a value of 1 if the respondent smokes or chews tobacco or drinks alcohol, and 0 otherwise. Average education represents the district level mean years of education, computed from the 61st and 68th NSS surveys. All variables have been weighted using appropriate sample weights as derived from the sample rounds. The other covariates are extracted from the IHDS. Education represents whether an individual is literate or not. Income is the annual household income in logarithmic terms. We also control for caste/religion (Brahmin, OBC, high caste, Dalit, Muslim, Sikh, Jain and others), rural/urban areas, gender of the individual access to toilet, exposure to chulha and survey dummies. We further carry out robustness checks by introducing measures for health infrastructure (number of primary and community health centres)—average education still has significant negative effects (results available on request).
Discussion and Conclusion
The existing literature primarily focuses on understanding and quantifying the relationship between individual education and health. While it is difficult to say whether better education leads to better health or vice versa, there is ample evidence to confirm that good education and better health go hand in hand. Yet, academicians have paid very little attention to studying the relationship between average education and health outcomes.
Average education is an important indicator of awareness within a community. A locality with more educated or literate individuals may have more adults who are able to read instructions on medication, vaccine or health camps and can hence help children attain better health. Using data in a developing country context (from the IHDS and NSSO), our study shows that increased average education is associated with a decrease in the likelihood of suffering from short-term mortality and also reduces the chances of individuals consuming alcohol or tobacco.
However, given that the impact of education takes years to trickle down, our study would have benefited greatly if we had access to a longitudinal data with more number of years between surveys and more waves to compare the growth in average education with respect to improvement in health outcomes. Second, IHDS allows us to identify the location of the individual only up to the district level, forcing us to aggregate average education data at the district level as well. This prevents us from accounting for heterogeneity in average education within a district.
Despite these caveats, we believe that our article brings to light an important aspect that an improvement in educational level is not an end in itself but has implications for the society at large. Given that there are very few studies that estimate social returns to education especially in the context of developing economies, we believe that the results presented in this article are of relevance to public policy.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.