
Abstract
The concept of technological catch-up can be used as a theoretical platform to design policies for the management of the healthcare sector in developing countries. In this article, initially, the factors affecting a technological catch-up process were collected through a conceptual literature review and prioritised using a fuzzy Delphi survey. The interdependences among important contributory factors were investigated as well. They were then used to create some policy recommendations for the management of the healthcare sector in developing countries through an interdisciplinary integration of the literature of technological catch-up and healthcare. Some exemplary projects/initiatives using these policies were collected too. The quality of human resources, a comprehensive knowledge management system, interactive learning and innovation-encouraging culture were rated as the most important contributing factors to an effectual technological catch-up in the healthcare sector in developing countries. Also, the creation of distributed health social networks, development of systematic knowledge management systems, forming strategic partnerships and designing path-creating technological catch-up processes by focusing on indigenous innovation were the final policy recommendations. All in all, the healthcare sector in developing countries should stop chasing frontiers, should try taking detours and flying a balloon by adopting a strategy of differentiation.
Introduction
In today’s world, health has gained profound significance for three reasons: (a) the role of health in world security, effective governance and promotion of human rights; (b) the significant yet insufficient budget dedicated to health; and (c) the proliferation of innovations and technological advancements to improve the condition of national healthcare systems (Frenk, 2010). Nonetheless, in terms of ‘goodness’ and ‘fairness’ (World Health Organization, 2000a), ‘the current rate of change is insufficient to reach the 2030 Sustainable Development Goals (SDG) targets’ (World Health Organization, 2020).
In both technological and non-technological, low- and middle-income countries suffer from severe deficiencies compared to their high-income counterparts due to numerous constraints on various levels of the healthcare system (Mills, 2014). Furthermore, historical emphasis on quantity over quality (Peabodyet al., 2006), ‘budget limitations, conflicting values of stakeholders, the high rate of financial circulation and the low morale of medical personnel’ (Zurn et al., 2004), the ratio of medical staff to total population (Benyoussef & Christian, 1977), ‘government stewardship within a pluralistic health landscape’ (World Health Organization, 2003a) and, last but not least, ‘gross underutilization of effective health care’ (O'Donnell, 2007) have a debilitating effect on the healthcare sector in developing countries.
Considering the technological transformation, one possible approach to bridge this gap is to use theoretical assumptions and successful projects of ‘technological catch-up’ and ‘successes experienced by industrialized nations’(Alexander, 2004). In this regard, we have used the concept of ‘technological catch-up’ to address the following question: How can the theoretical assumptions and practical examples of ‘technological catch-up’ enhance policies and practices in the healthcare sector of developing countries? To answer this question, first, some of the factors influencing the process of technological catch-up were collected from the literature and prioritised using a fuzzy Delphi study. The result was then used to create some policy recommendations for the healthcare sector in developing countries through interdisciplinary integration of the literature of technological catch-up and healthcare.
The Concept of Technological Catch-Up
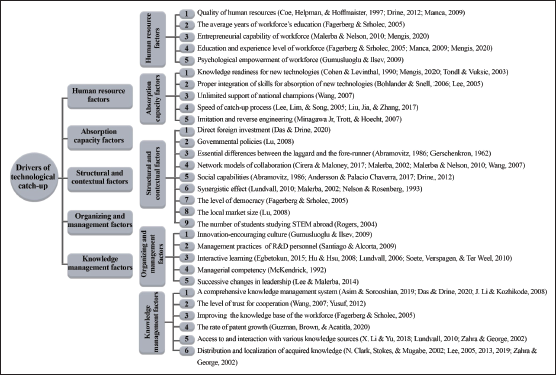
Miao et al. (2018) define ‘technological catch-up’ as a noticeable improvement of technological capabilities by ‘the laggard’ trying to bridge their gap with the forerunners and even leapfrogging over incumbents (Miao et al., 2018; Wong, 1999). As for the driving forces of technological catch-up, studies have emphasised the role of institutions (Manca, 2009), macroeconomic stability and trade openness (Sachs & Warner, 1997; Wong, 1999), potential of human capital (Barro, 2001), local absorptive capacity (Miao et al., 2018), ‘assimilation and mastering of imported technologies’ (Clark, 2002), historical/local condition of technology regime (Miao et al., 2018) indigenous innovation (Miao et al., 2018), open innovation platforms (Lu, 2008), cross-border inventions (Miao et al., 2018), direct foreign investment (Lu, 2008), access to international knowledge and networks (Lu, 2008), deployment of path-following, stage-skipping or path-creating catch-up (Lee, 2005), having ‘a holistic view of rather than focusing on isolated aspects of the process’ (Schrempf et al., 2013), open culture and politics towards technology and science (Fagerberg & Godinho, 2004), development of national innovation systems (NISs) (Cirera & Maloney, 2017) and interdependencies between various components of the system (Nelson & Rosenberg, 1993), affecting the ‘possibility of poor countries catching. Figure 1 summarises important factors affecting technological catch-up collected from the pertinent literature.
Methods
This study has been conducted as a survey using the fuzzy Delphi method. Two conceptual literature reviews have been conducted too—one to collect factors affecting the process of technological catch-up and the other to integrate the results of the survey with the literature of healthcare in an interdisciplinary fashion.
The Delphi method is a semi-structured decision-making method that is based on iterative sequences, anonymity of voters and feedback (Rowe & Wright, 1999). Since its inception at Rand, the Delphi method has been criticised for its ambiguity, necessity of sequential repetitions, declining response rates, and high cost and time of execution (Ishikawa et al., 1993).
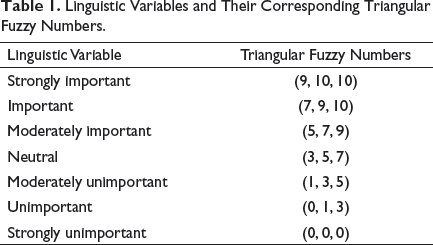
Linguistic Variables and Their Corresponding Triangular Fuzzy Numbers.
Second, suppose that

Next, the fuzzy weighting

where
And finally, the important factors can be chosen by determining a threshold value of
If
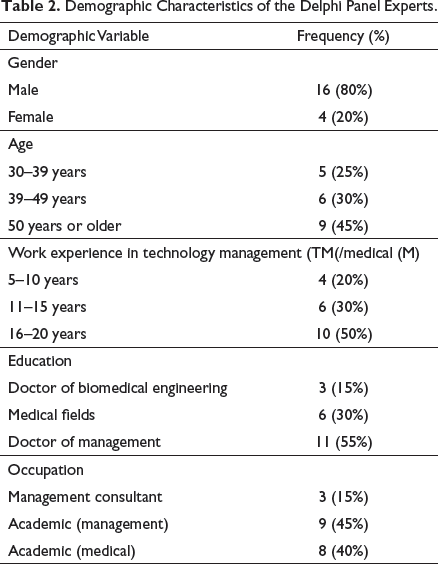
Demographic Characteristics of the Delphi Panel Experts.
Results and Discussion
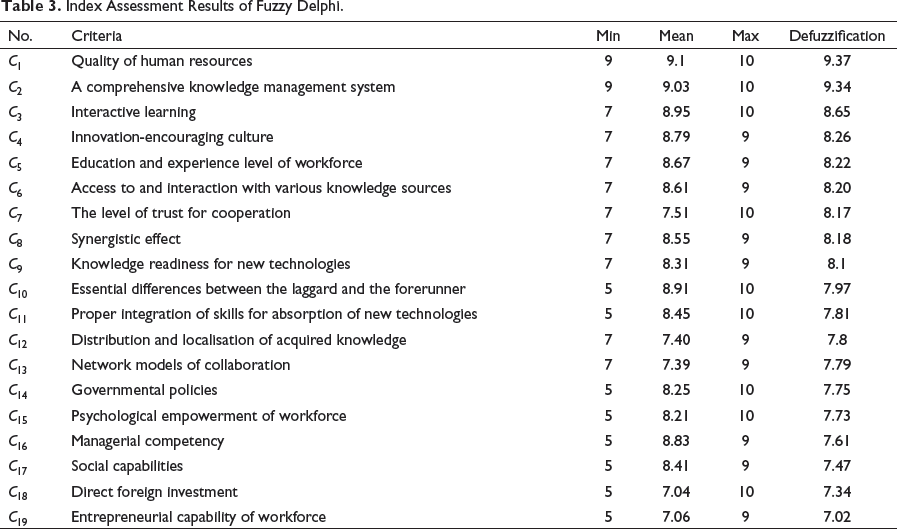
Having applied the fuzzy Delphi, factors effective in technological catch-up (Figure 1) were prioritised. Table 3 shows the contributory factors that passed the threshold of 7. The lowest, highest and geometric mean of experts’ estimations and the importance of each criteria after application of the defuzzification principle are given too.
In what follows, we have tried to discuss the underlying rationale behind the most important criteria in Table 3, cross-check them with the existing literature of healthcare and debate interdependencies among them to create policy recommendations for reinforcement of the healthcare sector in developing countries. We will use the notation of (C i ) to keep track of the criteria in Table 3 and discuss interdependencies among them.
‘Quality of human resources’ (C1) has been chosen as the most important factor. Mengis (2020) suggests that individuals can affect the catch-up process because of their ‘education (C5), industry experience (C5), technological know-how (C9), experience abroad, culture, entrepreneurial skills (C19), and power’. In developing countries, lack of adequate knowledge concerning the nature, scope, composition and needs of healthcare human resources (HHR) is a tremendous hindrance, despite the fact that HHR plays a more important role in healthcare systems in these countries (Sander, 2017; Zurn et al., 2004). Rural and remote communes are reported to be under-staffed, the geographically unbalanced distribution of manpower—beside their talent and skilfulness—is a ‘chief bottleneck’ (Noya et al., 2020; Van Lerberghe et al., 2002), and the emigration of high-skilled professionals and the effect of demand-supply imbalance exacerbates the crisis (Francis & Hoefel, 2018). Despite the obvious significance of HHR, ‘management of HHR is often absent from health reform processes’ (Inga-Berrospi & Rodríguez, 2019; World Health Organization, 2003b).
Index Assessment Results of Fuzzy Delphi.
The ‘right minds’ can also play a significant role in times of fundamental technological changes with their timely strategic recognitions (Mengis, 2020). Technological paradigm-shift intervals can provide the laggard with a ‘window of opportunity’ (Lee, 2005; Lee et al., 2005). Healthcare is facing an unprecedented wave of emerging technologies such as mHealth and the Internet of things (Aamir et al., 2018; World Health Organization, 2011), telehealth (Dorsey & Topol, 2016; Smith et al., 2020; Suzuki et al., 2020), big data (Bates et al., 2018), artificial intelligence (Becker, 2019; Jiang et al., 2017; Yu et al., 2018) and blockchain technology (Hölbl et al., 2018; Pandey & Litoriya, 2020), to name a few. As for mHealth, the number of mobile phones is expected to reach 17.72 billion by 2024 (O'Dea, 2020); these ubiquitous gadgets—which can easily be transformed into medical kits with the help of software development kits and novel applications (Latif et al., 2017)—and the swift rise of mobile penetration can ‘enable’ citizens in developing nations via short message services, web-based data entries and learning, social networking and data transmission (Fourtané, 2018; Kahn et al., 2010; Mousavi & Takian, 2020); provide them with mobile-assisted awareness; and accelerate the catch-up cycle of the healthcare sector in terms of fairness and goodness of services. Also, mHealth can assist healthcare workers in ‘data collection and reporting (C2), training and decision support, emergency referrals, work planning through alerts and reminders, an improved supervision and communication’ (Agarwal et al., 2015). According to data collected from 10 developing countries, governmental policies (C14) play a major role in eHealth adoption and acceptance (laGrange, 2006). Telemedicine likewise can be used for remote diagnostics, monitoring, and training and education (Combi et al., 2016), and its role in the management of the coronavirus disease is concrete proof of this (Kleinschmit, 2019). In Africa, for instance, integration of telemedicine solutions with local programmes such as African Home-based Care (AHC) and African Traditional Medicine (ATM) can offer both conventional and modern health services in rural areas (Kamsu-Foguem & Foguem, 2014). Moreover, artificial intelligence can compensate for lack of health-work personnel in rural areas of developing countries and can improve professionals’ ‘efficiency and quality of medical services’ and help physicians systematically analyse electronic health records (Guo & Li, 2018). The paradigm shift caused by nascent technologies can provide developing countries with an opportune moment to ride the next wave, ‘seize the window of opportunity’ (Balabanova et al., 2013) and bridge the chasm.
As a final comment on HHR, ‘local absorptive capacity’ (C12) for catch-up and ‘learning’ are inextricably linked to the availability of ‘human resources’, their mobilisation and strengthening (Chen et al., 2004), and the social capabilities (C17) of the country, and these factors can improve as fast as education (C5) flourishes (Abramovitz, 1986). To create a local absorptive capacity in developing countries, a distributed social health network should be created; human resource for health should go beyond classical definitions and should not only include doctors and nurses (Kruk et al., 2009); and community health workers should not be considered as an ‘extra pair of hands’ because, over time, they accumulate social capacity (C17) and contribute to equitable health development (Kane et al., 2020). At a broader level, the management of HHR should focus on (a) coverage by focusing on numeric adequacy, proper worker skill mixes (C11), and social outreach; (b) motivation by providing sufficient remuneration (C15), positive work environment and supportive health systems; and (c) competence through ensuring appropriate skill portfolio (C11), constant learning, and encouraging entrepreneurship and innovation (C4 & C19) (Chen et al., 2004). A holistic solution is to include ‘human resource impact assessment’ as a fundamental element of any reform project and to create evidence-based knowledge for improving the management of HHR (Van Lerberghe et al., 2002). Also, conventional models of recruitment, education, employment and deployment of health professionals needs to be revised altogether (World Health Organization, 2003b). Continuing medical education in the forms of targeted education, case-based learning and multi-model teaching techniques can contribute to HHR (Peabody et al., 2006).
The healthcare industry is a ‘knowledge-intensive’ and ‘knowledge-driven industry’ (Karamat et al., 2019; Shahmoradi et al., 2017). As our study shows, the development and implementation of a comprehensive knowledge management system (KMS) (C2) is paramount in the healthcare sector, without which the spiral of socialisation-externalisation-combination-internalisation (C12) as the heart of the technological catch-up process cannot occur. For instance, inefficiency of KMS in Iran’s healthcare system (Hojabri et al., 2014). and insufficiency of knowledge of nascent issues (C9) among health community workers in Pakistan have been reported (Haq & Hafeez, 2009). KMS is also the prerequisite condition for evidence-based interventions that can be metallised if only ‘systematic reviews and appropriate, usable evidence-based information for the developing world’ and for ‘all’ are produced and given to frontline health workers at the point-of-care using appropriate technology (Chen et al., 2004; Pearson & Jordan, 2010).
According to Shahmoradi et al. (2017), communities of practice, sufficient attention to the complementarity of tripartite subdivisions of KMS (people, process and technology), application of information and virtual technologies, and motivating actors of the network to share (C12 & C13) can facilitate the development and implementation of KMS (Shahmoradi et al., 2017). Moreover, knowledge acquisition diversity and management of a portfolio of knowledge sourcing—access to various external sources of knowledge and technology (C6)—(Li & Yu, 2018; Park, 2011) and geographic localisation of knowledge (C12) flows (Park, 2011) are other contributing factors. Using a quantitative model for Pakistan’s healthcare, Karamat et al. (2019) studies barriers, enablers and drivers of knowledge management (KM) and concludes that it can be (Karamat et al., 2019) negatively affected by organisational barriers including lack of management commitment (C16) and unsupportive organisational culture and structure, negatively impacted by strategic barriers such as divided definitions of KM and positively influenced by governmental enablers (C14) (Karamat et al., 2019).
As countries become relatively successful in primary healthcare, due to economic development, ageing, urbanisation and sedentary lifestyle. an ‘epidemiological transition’ towards non-communicable disease occurs. As a result, developing nations face a ‘dual burden’ (Kahn et al., 2010) and different types of knowledge bases such as Prospective Epidemiological Research Studies in IrAN (PERSIAN), which collect longitudinal information based on cohort and regional differences and make evidence-based practices possible (Eghtesad et al., 2017). gain importance. In the case of non-communicable diseases, social media can help developing countries tackle this ‘dual burden’ by spreading information, educating people and launching campaigns (Islam et al., 2019).
Interactive learning (C3) is the next important criteria. As emphasised by a sectoral interpretation of innovation, far from isolation, innovation and thus catch-up occurs in ‘an ecosystem of actors, knowledge and institutions’. The role of complementary capacities and synergistic ‘collaboration of various actors’ (C8 & C13) in high-achieving healthcare systems in developing countries has been documented (Balabanova et al., 2013).
At the intersection of HHR, KMS and interactive learning (C1, C2 & C3), the linguistic repertoire of the workforce to communicate their knowledge (Azadegan & Wagner, 2011) is key due to the fact that it has a direct impact on the externalisation of knowledge (C12) and the process of interactive learning both intra-organisationally and with frontiers. ‘Benefits emanating from interactive learning’ (Lundvall, 1990) between healthcare personnel, workforces and patients, and healthcare providers from different regions and countries are noteworthy. To materialise interactive learning, healthcare can be equipped with interactive KMS (IKMS) using Web 2.0 platforms and open innovation platforms in the form of participatory virtual communities that ‘unleash passion for engaging in knowledge sharing’ (C12 & C13) (Paroutis & Al Saleh, 2009) and create a spirit of collegiality. In this regard, patient-system interaction plays a role as well. Healthcare delivery can only be fully achieved in a bidirectional process—affected by healthcare literacy, cultural competency and linguistic repertoire— between providers and patients (Ratna, 2019). The transition from authoritarian and paternalistic healthcare delivery to proactive patient-focused care (Cramm & Nieboer, 2015) is indicative of a different dimension of interactive learning that has aptly been dubbed as ‘relational coproduction’ (Gittell, 2002). To achieve this, in Abu Dhabi, for example, it is recommended that clinical guidelines be translated to the patient’s native language based on their health literacy (Paulo et al., 2019).
Another factor is innovation-encouraging culture. Innovative individuals can be regarded as the greatest asset of healthcare systems (Wickramasinghe, 2007). At the organisation level, organisational culture and climate (C4)—via goal emphasis, means emphasis, reward orientation, task support and socio-emotional support (C15)—have a direct impact on individual creativity (Tesluk et al., 1997).
At the intersection of innovation and interactive learning (C3 & C4), it is noteworthy to mention that the healthcare sector cannot complete a catch-up cycle in isolation (IEEE, 2018) or in the presence of poor inter and intra-sectoral collaboration (Kristinsson & Rao, 2008; Lundvall, 2010). Therefore, national, regional and sectoral interpretations of innovation policy as well as the interplay between them (C8 & C13) (Malerba, 2002), international reinforcement of effective local strategies (Chen et al., 2004) and as strong action-coalitions via engagement of all stakeholders (Chen et al., 2004) are significant parameters through which health can be placed ‘at the center of the broader development agenda’ (World Health Organization, 2000b), and ‘systematic strengthening’ can be achieved instead of overconcentration on a specific programmer or problem. which is typical of vertical approaches in developing countries (Travis et al., 2004). Beyond this, Plum et al. (2020) argue that global health innovation platforms can be created to facilitate indigenous innovation. Information integration and knowledge coordination C2) as well as a multi-stakeholder engagement (C13 & C17) are at the core of this platform (Plum et al., 2020).
Regional considerations, for instance, are vital in developing countries due to heterogeneity within countries, resulting in spatially recognised boundaries and geographically formed gradients in terms of availability of workforce, infrastructures, equipment and pattern of disease. The central dictum of regional perspective declares that ‘there is no single one-size-fits-all policy’ (Schrempf et al., 2013). This also has a bearing on ‘engagement of private sector in healthcare’ and seeking ‘flexible models of public-private collaboration’ (Balabanova et al., 2013), which can be considered a pragmatic strategy due to ‘concentration of human resources in private sector’ (Mills, 2014).
In a catch-up process, indigenous innovation is a game-changer because success depends in part on gaining a local understanding of the dimensions and determinants of access (C10) to health services (World Health Organization, 2000b). Actually, any ‘meaningful reform in healthcare depends on innovation’ (Hinchliffe, 2000). Innovation leads to the development of local/context-specific solutions (C10)path-creating catch-up—via interactive learning with frontiers and ‘bi-directional flow of knowledge, ideas, skills and innovation’, internalises both tacit and implicit knowledge, provides the network with the underlying vocabulary and fabricates a common context-specific language (Kristinsson & Rao, 2008; Syed et al., 2013). One of the reasons a ‘primary health model’ failed is because developed countries did not allow communities to design and implement their ‘own’ (C10) health services (Hall & Taylor, 2003); their predominant mental model of health development was through path-following catch-up. To guarantee sustainable health growth, developing countries should nurture ‘local innovation capacity’ that imports not only finished products and technologies but also associated ‘knowledge, processes, and cultural mindset’ (Moses, 2020). Therefore, the allocation of sufficient financial resources to fund health-system research and building research capacity in developing countries in order to find patch-creating catch-up solutions and induce indigenous innovation should be given high priority. An analysis by the Alliance for Health Policy and Systems Research reported that health-system research may attract only 0·007% of the total health expenditure in low-income countries (Travis et al., 2004).
So far, we have discussed the underlying rationale behind the most important criteria in Table 3 and have debated interdependencies among them by providing examples and evidence from both healthcare and technology catch-up literature. Box 1 provides policy recommendations for reinforcement (or possibly catching up) of the healthcare sector in developing countries plus some exemplary initiatives/projects.
Policy Recommendations for Catch-Up of Healthcare Sector in Developing Countries and Exemplary Initiatives/Projects.
Nurse-based scale-up of antiretroviral therapies in Zambia (Stringer et al., 2006)
Joint Learning Initiative (Chen et al., 2004)
Distance education targeting diarrhoea and cholera in Guatemala (Peabody et al., 2006)
Framing the Future: The Second 100 Years of Education for Public Health (Petersen et al., 2015)
The Bangladesh Rural Advancement Committee programme to reduce morbidity from diarrhoea (Chowdhury & Cash, 1996)
Chipatala cha pa Foni programme in Malawi (World Health Organization, 2013)
Translation of clinical guidelines to the patient’s native language based on their health in Abu Dhabi (Paulo et al., 2019)
Task shifting and variation in skill mix in Thailand (Balabanova et al., 2013)
Inception of ‘health houses’ in the 1980s staffed by behvarzes and data collection by them through the ‘vital horoscope (KMS)’ in Iran (World Health Organization, 2003b)
General Electric’s low-cost MACi EKG machine (DePasse & Lee, 2013)
Collaboration of community health workers and ‘Partners In Health’ in rural Haiti (Jerome & Ivers, 2010)
Ecobank innovative financial strategies in TriSave and MuttiCard (netFWD, 2019)
Application of the eRanger in Malawi (Howitt et al., 2012)
Salauno eye-screening project using blended finance, big data and multisectorial collaboration in Mexico (Mignano, 2017)
Using a micro-credit system to support the provision of motivated healthcare workers in Bangladesh (MacBeath, 2012)
The Global Initiative on Health Technologies (Howitt et al., 2012)
AI-powered Chabots in China (Guo & Li, 2018)
ICT-enabled mobile application to assist healthcare delivery for infants and young children under 5 years in Nigeria (Eze et al., 2019)
Low-cost telecommunication systems for rural primary healthcare personnel such as ‘Hispano-American Health Link’ (Martínez et al., 2004)
Pan Africa Project providing Tele-consultation services in Egypt and India (Combi et al., 2016)
Malnutrition screening in under 5-years children in Ghana (Sarma et al., 2018)
Mobile Alliance for Maternal Action in South Africa (Coleman et al., 2020)
The e-NABLING future project providing 3D printing of prosthetics (Elmansy, 2015)
SIMpill for improvement of treatment adherence among TB patients in Cape town (Barclay, 2009)
Digital Health Programme of Aga Khan Development Network in South-Central Asia (netFWD, 2019)
Uniform web-based platforms for clinical terminology (such as SNOMED for problem, LOINC for laboratory tests and ICD-9 for billing) (Shahmoradi et al., 2017)
The Lancet’s Who Counts? Series (Okonjo-Iweala & Osafo-Kwaako, 2007)
‘Mapping’ the knowledge shortage concerning the diagnosis and management of common disease by collecting ‘killer facts’ in Africa to support evidence-base practices (Pakenham-Walsh & Bukachi, 2009)
Conducting cohort studies and collecting longitudinal information Prospective Epidemiological Research Studies in IrAN (PERSIAN) (Eghtesad et al., 2017)
Handhelds for Health in India and Alerta DISAMAR in Peru—platforms to collect data for epidemic outbreak tracking (Latif et al., 2017)
Teeko and Tibbi vaccination data-collecting mobile apps in Pakistan (netFWD, 2019)
An mHealth system to mitigate gaps in reproductive health reporting in Kerala, India (Thomas et al., 2012)
Public-private partnership led by Pfizer Global Health Fellows programme (Vian et al., 2007)
Carabayllo project in Peru (Berwick, 2004)
The Millennium Villages Project: a multisectoral, rural development project (Mitchell et al., 2018)
The South-South Initiative in tropical diseases research (Holt et al., 2012)
Collaboration of four sub-Saharan countries to design and run a joint Master Programme with a focus on health workforce (Amde et al., 2014)
Capacity building among hospital managers of Iran in collaboration with World Health Organization (Doshmangir & Takian, 2019)
The Observatory of Human Resources in Health Sector Reforms for the Americas (World Health Organization, 2003a)
The project from the Italian association Patologi Oltre Frontiera for cancer prevention in Zambia (Combi et al., 2016)
Many of these exemplary projects apply policies presented in Box 1, criteria presented in Figure 1 and Table 3 in an eclectic fashion at the heart of their design. For instance, the Carabayllo project in Peru (Berwick, 2004), as a successful project in combating multidrug-resistant tuberculosis in a poor neighbourhood in Peru, was born as a path-creating catch-up model through a strategic partnership of Partners in Health, based in Boston, and Socios en Salud, its sister organisation in Lima. They tried to create distributed health social networks by forming 41 multidisciplinary teams, empowering community health workers, setting ambitious goals, and benefiting from a number of indigenous innovations thereby creating magnificent results that ‘compare favorably with those achieved in similar collaborative improvement projects’ in developed countries (Berwick, 2004). This is an outstanding example of a catch-up success related to healthcare in a developing country innovation paradox.
Conclusion
In developing countries, ‘Prometheus remains bound’ and the innovation paradox is prevalent (Cirera & Maloney, 2017). These countries try to bridge the gap with developed countries in the best possible way. The healthcare sector is no exception here and is even more in need of such a development—the raison d’être of this article.
In this article, first, drivers of technological catch-up were gathered and prioritised in a fuzzy-Delphi survey. The quality of human resources, a comprehensive KMS, interactive learning and innovation-encouraging culture were chosen as the most significant drivers for the catch-up of the healthcare sector in developing countries.
The resultant analysis was then used to offer some policy recommendations for ‘the improvement of the healthcare sector by interdisciplinary integration of the literature of technological catch-up healthcare. Needless to say, there is no fixed and magical formula for an ideal healthcare system, and the process of reform should be considered as a long-term development process (Mills, 2014). Keun Lee (2019), considers technological catch-up processes based on chasing frontiers ineffective and argues that ‘one cannot catch up if s/he continues to work on catching up’. Instead, he recommends that latecomers should forget algorithmic/scientific imitation, ‘kick the ladder away’, follow a strategy of differentiation, and master the art of ‘taking detours and flying a balloon (Cobby, 2020; Lee, 2019). The creation of distributed health social networks, developing comprehensive KMS, riding the wave of emerging technologies and forging synergistic strategic partnerships can be some effectual policies in designing a path-creating catch-up process and building a local capacity based on continuous indigenous innovation for the healthcare sector in developing countries.
Footnotes
Declaration of Conflicting Interests
Funding
The authors received no financial support for the research, authorship and/or publication of this article.