
Abstract
Healthcare is vital for the overall well-being of an individual. The service quality in healthcare is a matter of great importance for health institutions across the world. With increasing patient awareness and rising competition among hospitals, patient perception of healthcare quality has become very relevant. This study aims to review the literature to explore the concepts of perceived service quality, customer satisfaction, and behavioural intentions. The study has attempted to look into the relationship between perceived healthcare service quality, patient satisfaction, and behavioural intentions of patients. Healthcare service quality is measured using SERVQUAL dimensions as well as other dimensions specific to the healthcare sector. The findings clearly show that perceived healthcare service quality, patient satisfaction, and behavioural intentions are closely related to each other, and high-quality services lead to satisfied patients who further exhibit positive behavioural intentions.
Keywords
Introduction
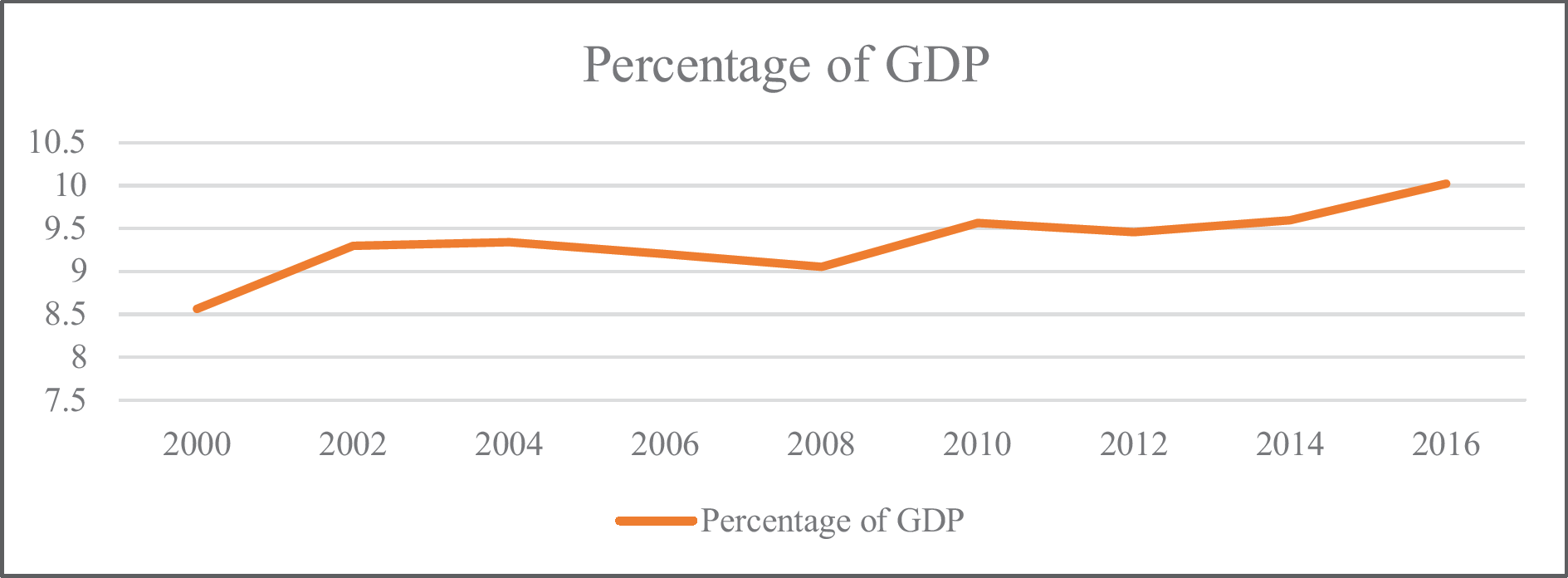
The service sector is an essential contributor to the GDP of a country. It makes a significant contribution in terms of creating employment and investment opportunities critical to the overall development of a nation. The share of the service sector in the world’s GDP is more than 50 per cent (OECD, 2008). The service sector provides ample opportunities for both developed and developing countries, even amid trade barriers and escalating tensions (United Nations, 2019). Healthcare is the most complex, exorbitant, and universally used service, which has a massive impact on a country’s economy and the quality of day-to-day lives of people (Berry & Bendapudi, 2007). The global spending in the healthcare sector is around 10 per cent of the world’s GDP, and the rate of growth of the industry is faster than the growth of the economy. The global healthcare spending between 2000 and 2017 grew by 3.9 per cent, whereas the global GDP grew by 3 per cent. Notably, the growth in the health spending of low-income countries was the fastest between the same period (WHO, 2019). Figure 1 shows the current health expenditure as a percentage of GDP over the period from 2000 to 2016.
With multiple ranges of options available across all products and services, quality is one of the most important parameters that distinguishes one offering from the other. People are always on the lookout for right quality products and services. This desire has caused the organisations across the world to work towards achieving competitive advantage by delivering high-quality products and services (Mosadeghrad, 2013). Long-term profitability of an organisation is dependent on the quality of services it provides. Service quality directly affects the repurchase intentions of its existing and potential customers (Ghobadian et al., 1994). Healthcare services involve high risk for the life of a patient dependent on the care process. Even a small amount of error can have deadly consequences. Thus, paying attention to healthcare service quality becomes crucial (Ahmed et al., 2017). Patients choose the healthcare provider whom they can trust and who they believe can cure them. Patients are likely to exhibit positive behavioural intentions when providers meet their service expectations, whereas dissatisfied customers avoid revisiting the healthcare facility. Thus, understanding patient expectations helps the service providers to better cure and satisfy them (Ramsaran-Fowdar, 2005). Patient satisfaction is achieved by continuous improvement in the healthcare service delivery, understanding patients’ needs, and responding to their views and enhancing the interpersonal relationship between the patient and the provider. Patient’s perception towards healthcare is affected by functional and technical factors, understanding of society, technological factors, and political environment. Assessment of all these factors is imperative for healthcare managers to understand how patient perceptions are formed (Talib et al., 2015).
A review of literature has been carried in this work to understand and explore the concepts of perceived service quality, perceived healthcare service quality, patient satisfaction, and behavioural intentions. The article identifies the different dimensions used to measure healthcare service quality and enlists the studies that have used SERVQUAL dimensions. The work also includes the studies measuring healthcare service quality in the Indian context. Finally, the article presents a link between perceived healthcare service quality, patient satisfaction, and behavioural intentions.
Perceived Service Quality
Quality is subjective and is defined differently by various stakeholders. Every stakeholder may be viewing quality from a different perspective, context, and interest. The definition may be different for customers, managers, suppliers, accreditation agencies, policymakers, etc. (Mosadeghrad, 2013).
Service quality helps the customer form an opinion about an entity. High-quality products help in building an excellent reputation for the organisation, which further leads to enhanced customer satisfaction. Providers must focus on four critical characteristics of service to satisfy customers:
Intangibility: Cannot be felt, touched, or seen. Perishability: Produced and consumed simultaneously and cannot be stored like products. Inseparability: Cannot be detached from the service provider, and their production and consumption take place at the same time. Heterogeneity: Services delivered cannot be identical, and their quality also varies depending upon factors such as provider, time, and place of service (Ahmed et al., 2017).
Service quality means meeting the consumer requirements and the level to which the service matches the customers’ service expectation level. It can be defined as providing a service that exceeds customers’ expectations by giving them what they want and how they want. Perceived service quality is a consumer attitude which is formed by interactions with a company, word of mouth (WOM), evaluating the expectations met by company’s products, marketing mix, and comparisons with offerings of competitor (Lewis, 1989). The ultimate aim of any business is to please the customer and to establish long-term engagements. Service quality plays a crucial role in meeting customer expectations and maintaining relationships. The author represented perceived service quality on a continuum with unacceptable quality on one end and perfect quality on the other. The provider aims to keep the delivery levels close to the ideal condition (Ghobadian et al., 1994).
Two important questions about service quality are: how is the service delivered and what is the outcome of service. The entire process of service delivery depends on these two questions. Human element is the most important factor while determining the quality of service delivered as the customer and provider are continuously in touch throughout the service delivery process. Human involvement adds variability to the service quality, and thus, it is imperative to monitor it regularly (Prakash, 2019).
Multiple dimensions are used to measure service quality, which is defined as the difference between service expectations and perceptions. The customer evaluates the quality of service based on how closely the provider meets his/her service expectations (Bloemer et al., 1999). Even though SERVQUAL is an established instrument to measure quality, it has often drawn criticism due to its dimensional structure, which varies across different contexts and industries. The inclusion of expectations is another area of contention in the model, with critiques questioning its utility and relevance (Vinagre & Neves, 2008). Since service is intangible in nature and service quality is an attitude, it is more appropriate to use a performance-based approach to measure customer attitudes (Butt & Run, 2010).
Service quality measurement is dependent on factors such as the type of service used, its need, expectations from it, and service setting. The changing expectations of people from a service further add to its complex nature. These expectations change concerning factors such as competitive offerings, time of using service, and number of times the service was availed. The concept of service quality and its measures must be continuously updated to meet customer expectations (Seth et al., 2005).
Dimensions of Perceived Service Quality
Service quality is considered crucial for the success and excellence of any service. The importance of service quality has motivated several researchers to identify its underlying dimensions. Several authors have proposed service quality dimensions depending on the sector and the context.
According to Kang and James (2004), while evaluating service quality, researchers either refer to the American or the European perspectives of service quality. The American view of service quality primarily focusses on the functional aspect of quality, whereas the European perspective includes the functional, technical, and the image aspects of quality. Dimensional approach to service quality is widely used and occupies a dominant share in the service review literature. Some of the industry-specific service quality measurement models are HEALTHQUAL, which is for measuring service quality in the healthcare sector, and LibQUAL, which is to measure the quality of services of the public library (Ladhari & Morales, 2008; Lee, 2016). The essential features of the dimensional approach to service quality are as follows:
The focus is on the features and delivery of the service. Industry-specific service quality instrument. Quality dimensions differ across services, sectors, firms, and cultures (Sultan & Wong, 2010).
The original SERVQUAL instrument proposed 10 dimensions to measure service quality, which were later reduced to 5. Across all service sectors, reliability was considered the most critical aspect, and tangibility the least important one. SERVQUAL, which is a reliable and valid scale, has provided the basis for many studies in service quality (Johnston, 1995). The model, however, was found to be of poor fit across some studies where its original five-factor structure was not supported. Thus, even though the model is prevalent in the service quality literature, its universality is often questioned. Service quality constructs differ across cultures and countries, and therefore, the factors relevant in the Western context may not apply to the Asian context (Pai & Chary, 2016).
Cronin and Taylor (1992) proposed the SERVPERF model comprising 22 items; the number of statements is half the number as compared to the SERVQUAL model. The model uses only customer perceptions to measure service quality. SERVPERF explains more variations in service quality than the SERVQUAL model, which makes it superior to the latter. Kang and James (2004) mentioned several models of service quality to emphasise its multidimensional nature. The Lehtinen and Lehtinen model proposed physical quality, interactive quality, and corporate quality. The Grönroos model proposed functional, technical, and corporate image. The hierarchical model of service quality gives three primary quality dimensions, namely interaction, environment, and outcome.
Healthcare Perceived Service Quality
Characteristics of Healthcare Services

Relationship Between Healthcare Service Quality Dimensions, Patient Satisfaction, and Behavioural Intentions
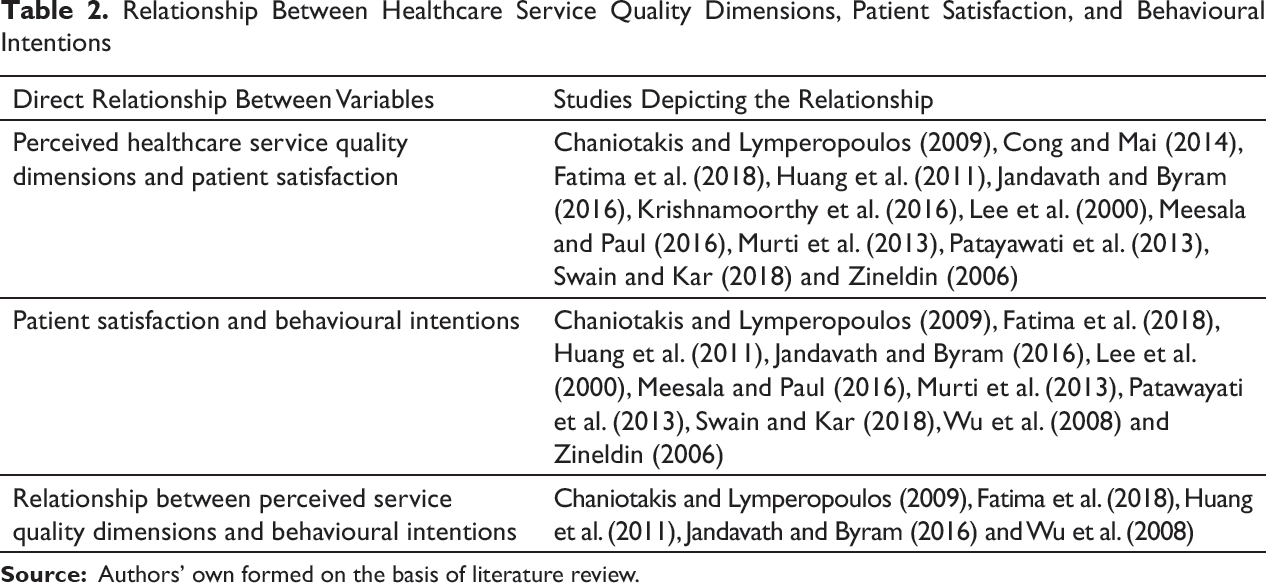
Healthcare services impose a big challenge on economies due to new diagnoses and treatments, the ever-increasing demand for quality services, and an aging population. Therefore, studying healthcare quality and patient satisfaction is vital for healthcare organisations. Customer is the direct recipient of healthcare services, which makes understanding patient’s perception highly crucial. Healthcare quality has two aspects, technical and functional. Patients find it difficult to understand the technical aspects of care such as correct diagnosis, line of treatment, and instruments used and find it easy to judge the functional aspects of care (Butt & Run, 2010). Technical quality incorporates the accuracy of diagnosis and adeptness of the skills of doctors, nurses, and other healthcare staff. Functional quality refers to how the service is delivered and relies on the human element of service delivery. Due to limited medical expertise, a patient may not be able to assess the technical part of healthcare and relies on functional quality to form his/her perceptions (Rashid & Jusoff, 2009) (Table 2).
Healthcare quality must be defined by integrating the views of all the stakeholders involved in the service delivery process. The supply side of healthcare quality focuses on meeting the prior decided standards and specifications of service, whereas the demand side looks at the service characteristics which satisfy the customer (Mosadeghrad, 2013). Healthcare service quality can be measured scientifically by using tools called measures. Consumer ratings are the patient-oriented measures that focus on the patient’s perception of quality, like the doctor’s behaviour and performance of the healthcare staff. Clinical performance is a technical measure that centres on the service outcome. It provides information on the performance of the healthcare organisation, for example, treatment or prevention of the illness (Zineldin, 2006). According to the World Health Organization (2006), healthcare systems should make efforts in six areas of quality: effectiveness, accessibility, the efficiency of care, delivery of equitable care, safety procedures, and patient-oriented care process.
Dimensions of Healthcare Perceived Service Quality
Many models of healthcare service quality have been formed over the past several years. Constructs developed in one country or culture may not be replicated at other places. Even though SERVQUAL is often criticised for its reliability and validity, it is still widely used and has immensely contributed to healthcare literature (Aagja & Garg, 2010; Purcărea et al., 2013).
Studies Using SERVQUAL Instrument to Measure Perceived Healthcare Service Quality
Prabhu A. and Iyer (2018) attempted to find the impact of information systems on patient satisfaction and service quality by noting their experience with the usage of information systems in hospitals. The users perceived the system as outdated and challenging to use. The respondents perceived reliability, followed by tangibility, as the most crucial factor while evaluating service quality.
Shafiq et al. (2017) adapted the original SERVQUAL scale to measure the quality perception of patients in Pakistan. The high gap scores on all dimensions revealed the need for an extensive scope of improvement in hospitals. It was observed that private hospitals provided better services than public hospitals.
Kansra and Jha (2016) used the SERVQUAL model to measure service quality in hospitals in Jalandhar city. They used exploratory factor analysis to organise the items under four dimensions, thus rejecting the five-dimensional approach of the original instrument. The study has successfully validated the tool in the Indian context, and the results can help the managers to assess the medical services in their hospitals.
Turan and Bozaykut-Bük (2016) observed a maximum gap between patient expectation and perception of the ‘tangible’ dimension in gynaecological and paediatric hospitals in Turkey. ‘Prompt service by staff during discharge’ was the only item that registered a positive gap score. Perceived service quality positively affected patient satisfaction, buying intentions, and WOM.
Al-Neyadi et al. (2016) pointed out that assurance was the most important dimension of service quality, while responsiveness was the least essential dimension for patients in the UAE. There were no significant differences in patients’ perception of quality between public and private hospitals. All the quality dimensions were interrelated with each other, except for the responsiveness dimension, which was only related to empathy.
Mečev and Goleš (2015) investigated hospital service quality in primary healthcare centres in Croatia. The expectations were found to be higher than the perceptions of all dimensions, thus indicating poor quality of care. The patients had maximum expectations with the cleanliness of the equipment, followed by the need to feel safe during the examination. Patients were least satisfied with the long waiting time and the lack of modern types of equipment.
Peprah and Atarah (2014) added the ‘communication’ dimension to the original five dimensions to measure the patient perception of services in a public hospital in Ghana. The gap scores on the six dimensions revealed negative scores for responsiveness, reliability, communication, and assurance. The hospital performed well on the tangibility and empathy dimensions.
Mahapatra (2013) assessed patient’s preferences for choosing public and private hospitals in Delhi. Patients who visited public and private hospitals reported poor quality of service at both public and private hospitals. They found poor maintenance of medical facilities and instruments, low cleanliness, improper directional sign, no privacy during treatment, long waiting hours, no proper feedback system, unempathetic staff and doctors showing no respect in the hospitals.
In their study, Purcărea et al. (2013) found that the expectations of female patients exceeded their perception levels. The hospital could invest in modern-looking instruments and work towards improving the overall appearance of the facility and its employees.
Ramez (2012) concluded that reliability was the most critical dimension, and assurance the least to the patients admitted in Bahrain. Responsiveness exerted the most significant influence on service quality, followed by empathy and tangibility. There were strong substantial and positive associations between behavioural intentions, satisfaction, and overall service quality.
Papanikolaou and Zygiaris (2012) investigated that the patients visiting public healthcare centres in Greece reported a negative gap between expectation and perception on all dimensions of the instrument, with the centres performing the worst on empathy dimensions and the best on reliability and responsiveness dimensions.
Ramanujam (2011) found that the patients admitted in corporate hospitals of Hyderabad were content with the services provided. The tangibles at the hospital were excellent, and the reliability and responsiveness shown by the staff were satisfactory. However, the assurance dimension of quality was worrying.
Butt and Run (2010) found a vast difference between the expectation and perception levels of patients. Reliability and responsiveness dimensions had the highest gap, which indicated that the patients did not trust the medical personnel at the hospitals.
In their study, Lee (2005 failed to confirm the original five-factor solution of SERVQUAL. He instead gave a four-factor model, revealing that service quality factors are not the same across all cultures and settings. ‘Convenience to access service’ emerged as a new factor in the study. Adequate support to employees, trust in doctors, keenness to help the patients, modern facilities, and being dependable were the most important factors listed by the patients.
Sohail (2003) evaluated the service quality in Malaysian hospitals and found that it exceeded the patients’ expectation levels. Private medical care in Malaysia is highly trusted, and the country is a popular destination for medical tourism. Excellent medical facilities discouraged the citizens from going abroad for treatment, thus saving foreign exchange.
Studies Using Other Instruments to Measure Perceived Healthcare Service Quality
Akdere et al. (2018) compared the SERVQUAL and SERVPERF instruments to conclude that the perceptions only instrument (SERVPERF) showed higher construct, discriminant, and convergent validity. Responsiveness and reliability were the most important, and tangibility the least essential dimension for patients. All the measures of the SERVPERF instrument significantly predicted the overall service quality in the hospital.
Fatima et al. (2018) explored the relationship between hospital service quality, satisfaction, and loyalty variables. They operationalised healthcare quality using the constructs such as, physical environment, communication, safety and privacy, responsiveness, and customer friendliness. Patients visit private hospitals because of the polite behaviour of staff, confidentiality of information, modern technology and equipment, and attentiveness of doctors towards patients. Healthcare quality was positively related to satisfaction and patient loyalty.
Shabbir et al. (2017) conducted a gap analysis to compare the expected and perceived healthcare service quality in public and private hospitals located in two cities of Pakistan. Eight dimensions used to obtain patient responses are doctor’s medical service, nursing medical service, diagnostic service, employee service, admission service, meal service, housekeeping, room service, and discharge. The overall services provided by private hospitals were better than the public hospitals.
Lee (2016) developed the ‘HEALTHQUAL’ instrument to measure the healthcare service quality in a hospital in South Korea. It has two parts, the processes, and the results. The process part of the instrument comprises empathy, tangibles, safety, and efficiency aspects, whereas the results part degree of improvement in service.
Shafei et al. (2015) developed a comprehensive model to measure healthcare quality in Egypt. The dimensions identified are doctor service, nurse service, diagnostic service, admission, discharge, hospital premises, rooms, and meals. The researchers confirmed the relationship between overall perceived quality and the identified dimensions. Room and housekeeping, staff courtesy, nursing tangibles, hospital premises, and employees exerted a significant impact on service quality.
Abuosi (2015) developed a six-dimensional structure to measure the quality of medical care using the dimensions: financial access, the fairness of care, adequacy of resources, effective treatment, professional care, and interpersonal care. The findings show stark contrasts between the perceptions of the patients and providers on the service quality dimensions. Lack of direct contact between patients and providers can be one reason for such gaps in the perception levels.
Kondasani and Panda (2015) revealed an eight-dimensional framework as loyalty, satisfaction, privacy, responsiveness, communication, customer-friendly staff, physical environment, and reliability. Except for privacy and reliability, all constructs of quality had a significant relationship with patient loyalty.
Le and Fitzgerald (2014) examined the service quality in two public hospitals in Vietnam. Reliability, tangibility, assurance, empathy, responsiveness, and administrative procedures were the six dimensions used to gather the perceptions of patients. Due to the high correlation found between satisfaction and the factors, empathy, and assurance, it is of utmost importance that the hospitals focus on these items.
Ritu Narang (2010) evaluated the service quality using four dimensions: access to services, delivery of services, adequacy of resources, and healthcare personnel. The author suggested that policymakers should address the requirements of the patients by addressing urgent concerns such as access to the facility, number of rooms, availability of drugs and doctors, and patient follow-up.
Duggirala et al. (2008) used seven dimensions to model service quality: infrastructure, health personnel quality, the process of care, administrative procedures, safety indicators, overall experience, and social responsibility. This instrument showed several similarities with the SERVQUAL framework.
Zineldin (2006) proposed a model to study the factors affecting satisfaction by integrating both the technical and functional aspects of healthcare quality. Quality of object, quality of processes, quality of infrastructure, quality of interaction, and quality of atmosphere were the five quality dimensions developed in the study. The biggest hurdle found in public hospitals was contacting staff, parking space, and less concern for patients. In the semi-public hospital, the responsiveness and politeness of healthcare providers were not satisfactory. Parking space and waiting time to see the doctor were the significant areas of concern for the private hospital.
Andaleeb (2001) believed that in developing countries, the perception of patients is often ignored and not accounted for in the decisions regarding hospital facility improvement. The five-factor solution to measure the quality of medical service comprises of responsiveness, assurance, communication, discipline, and baksheesh. The discipline factor had the most significant impact on satisfaction , followed by the assurance factor.
Haddad et al. (1998) used the inductive process to develop the content of the scale, which focusses on the perceptions of people visiting primary healthcare centres in the Upper Guinea region. The three quality dimensions used are facilities, personnel, and healthcare delivery. Cronbach’s alpha coefficient and consistency ascertained the reliability of the scale.
Healthcare Service Quality in India
In India and other developing countries, there is an apparent mismatch between the demand and supply of healthcare services. To effectively fulfil the healthcare needs of the ever-growing population, it is vital to establish a sound health infrastructure that is easily accessible to everyone. Today, the patients are more aware of healthcare than ever before due to the ease of availability of online and offline data. Hence, it has become necessary for service providers to deliver high-quality healthcare services (Padma et al., 2010). Due to the focus on increasing healthcare service coverage, service quality and the needs of the patients are often ignored. The services are usually delivered, based on the provider’s perception of quality instead of the patients’ perceptions (Narang, 2010).
Jandavath and Byram (2016) conceptualised the quality of care using the five SERVQUAL dimensions. Acceptable service quality levels positively affected patients’ willingness to recommend and their revisit intentions. The impact of empathy, assurance, and responsiveness was significant on patient’s revisit intentions.
Padma et al. (2014) used the importance performance analysis technique to find the difference between the performance of service quality dimensions and the importance attached to those dimensions by patients and attendants. The service quality dimensions used in the study are the trustworthiness of hospital, social responsibility, image, safety, administrative process, clinical care, quality of staff, and infrastructure. Safety indicators and clinical care process are the most critical dimensions for both patients and attendants.
Murti et al. (2013) attempted to measure service quality, behavioural intentions, and customer satisfaction and explore the relationship between the three variables. The scale developed to evaluate service quality uses eight dimensions, namely tangibles, reliability, responsiveness, assurance, empathy, safety, discharge, and management of medicine quality. The aspects of quality significantly explain satisfaction, with assurance, reliability, empathy, responsiveness and tangibility playing a dominant role.
Narang (2011) adapted the scale developed by Haddad et al. (1998) to suit the cultural context of the study. The five factors to measure the quality of service revealed are facility, availability of drugs and conduct of personnel, interpersonal and diagnostic aspects, healthcare delivery, and physical and financial accessibility. The overall service quality was found to be unfavourable by the patients. However, patients gave positive responses to the dimensions, physical and financial accessibility and healthcare delivery.
Padma et al. (2010) measured service quality perceptions of both patients and attendants using infrastructure, personnel quality, image, safety, social responsibility, trustworthiness, administration, and care process. It was noted that the patients and attendants of government and private hospitals are satisfied with different dimensions of service quality.
Aagja and Garg (2010) developed PUBHOSQUAL instrument to measure service quality from the perspective of patients in public hospitals of India. Overall service, medical service, admissions, social responsibility, and discharge are the five dimensions of the instrument. The PubHosQual scale was found to be more superior to the original SERVQUAL scale in terms of the reliability of the aspects and its content validity.
Chahal and Kumari (2010) modified the hierarchical model to include interaction quality, physical environment quality, and outcome quality to evaluate service quality. Physical environment quality has three dimensions, of which, tangibility, followed by the ambient atmosphere and social responsibility, affects service quality. The three aspects of interaction quality are process, attitude and behaviour of staff, skill, and expertise. The expertise of the hospital team is most significant for overall quality, followed by the attitude of employees and process quality.
Rao et al. (2006) developed a 16-item scale with medicine availability, information related to medical services, staff and doctor behaviour, and infrastructure to measure service quality perceptions of inpatients and outpatients. The outpatients are most satisfied with the doctors’ conduct, whereas the inpatients with the staff conduct. The overall quality at public hospitals was found marginally favourable, thereby suggesting a massive scope of improvement in the healthcare system.
Swain and Kar (2018) conceptualised service quality into a 6Q framework: technical (core medical service), procedural (administrative procedures), personnel (skills of staff), infrastructure (physical facilities), social support (ethical and societal orientation) and interactional (interactions and communication between the staff and patients).
Pai and Chary (2016) modelled service quality as a nine-dimensional construct. The dimensions are Healthscope, personnel, image, trustworthiness, clinical care, communication, relationship, personalisation, and administrative procedures. The model shows the causal linkage between service quality, satisfaction, and behavioural intentions.
Customer Satisfaction
Customer satisfaction provides information about the needs and expectations of customers. The firms which measure customer satisfaction and regularly incorporate changes in their policies based on the results can outperform other players. Satisfaction is the evaluation of a customer’s service experience, and it represents his/her feelings about the output of that service experience (Jandavath & Byram, 2016). It is the function of features and characteristics of the service and the incidents that take place during a service encounter. It evaluates whether the service experience was pleasurable or not (Mehta, 2011). Customer satisfaction is dependent on the expectations and perceived performance of the patients. A match between the customer expectations and perceptions results in a satisfied customer, whereas a mismatch leads to a dissatisfied customer (Andaleeb, 1998).
Patient Satisfaction from Healthcare Services
Cure is a basic expectation of every patient treatment. Satisfaction is the evaluation of patient expectations on all the dimensions of service quality, and it is the desired result of any treatment process. Patient satisfaction enhances the overall image of the hospital and is favourable for the reputation of the hospital (Naidu, 2009). The feedback received from patient satisfaction surveys is used by hospital management to improve their facilities. The ever-increasing competition in the healthcare sector has made it significant for hospitals to keep track of all factors affecting satisfaction (Al-Neyadi et al., 2016).
Patient satisfaction determines the standard of performance of a hospital and the quality of services delivered. Quality is a cognitive component, whereas satisfaction is an affective construct, which makes it difficult to define. It can be summed up as the patients’ experience at the hospital and the extent of fulfilment of their expectations (Geletta, 2018). Satisfaction determines the utilisation of healthcare services by the patients. It helps to allocate resources effectively by thoroughly understanding the priorities of patients. Patients play a significant role in spreading a positive image of the hospital. Therefore, their feedback is an essential yardstick to design programmes aimed at enhancing their satisfaction levels (Rajguru 2018).
There are several theories proposed on patient satisfaction. The discrepancy and transgression theories underline that a patient is satisfied when the provider’s service conditions and patients’ preferences are congruent with each other. According to the discrepancy theory, satisfaction is mediated by customer’s expectations from service, values, and beliefs. Determinant theory highlights that satisfaction is the response to the service experienced and is mediated by the customer’s feelings and likings. The healthcare quality theory propounds that satisfaction is the product of the interpersonal aspect of care (Gill & White, 2009).
Vinagre and Neves (2008) put forward that the relational aspect between the patient and provider is as important as imparting high-quality services in a hospital. Mismanaged patient emptions may cause satisfaction levels to dip, even when there are high healthcare quality levels.
Ahmed et al. (2017) found that the patients in Bangladesh were more satisfied with the services provided by private hospitals than public hospitals. People did not mind the high cost of treatment in return for reliable and quality healthcare services. Patient satisfaction was affected by the care provided by hospital staff and the ease of the information supplied.
Andaleeb et al. (2007) introduced factors such as doctor service, nursing service, tangibles, access to services, treatment cost, and baksheesh to measure satisfaction levels of patients. Doctor and nurse service orientation most significantly affected the level of satisfaction. People are willing to pay a higher cost for quality treatment, suggesting price is not a significant indicator of satisfaction.
According to Priporas et al. (2008), patients were concerned not only about the healthcare components but also their overall experience at the service facility. The patient’s education level, the situation at the time of admission, and the type of insurance affect patient satisfaction levels. Males and young people were more satisfied as compared to females and older people.
Naidu (2009) identified dimensions affecting satisfaction as access, care, the output of healthcare, tangibles, and communication. Paying attention to customer satisfaction improves the image and performance of hospital services, which results in increased service usage and market share.
Mehta (2011) found satisfaction to be determined by the healthcare service features and the experiences of patients during a service episode. It should be scientifically measured and managed to retain the patients. Amenities, clinical services, and physical facilities were the three most important factors which influenced patient satisfaction.
Abiodun (2010) examined the satisfaction level of patients at a primary level using quality attributes. ‘Empathy’ was perceived as an essential attribute for healthcare providers, along with the facilities at the healthcare facility. The healthcare providers must explain the technical aspects of care to the healthcare seeker to ensure maximum service utilisation.
Bernhart et al. (1999) found that in Indonesia, patients ranked ‘getting cured’ as the most important parameter of satisfaction followed by medicine administration and privacy. The factors regarded less significant by patients were the cost of care, interaction with the provider, and waiting time. Men and women had different opinions on the relative ranking of satisfaction parameters.
Kuttichira and Rejani (2011) conducted a satisfaction survey at a government tertiary care hospital. The patients were satisfied with the registration process, accommodation, cleanliness, availability of medicines, and the services provided by doctors. The patients were dissatisfied with the support and security staff, and the food quality at the hospital.
Zhang et al. (2016) observed that patient satisfaction in Chinese public hospitals was influenced by the attitude of hospital staff, physical environment, and the cost of treatment. The level of satisfaction varied with demographic factors like gender and occupation, whereas income and marital status did not influence it.
Kamra et al. (2016) found that non-clinical factors had more influence on patients than clinical factors. Convenience and affordability of treatment is the factor which affects satisfaction the most. Other factors such as staff care, behaviour of doctor, admin procedures, and facilities at the hospital also significantly influence the satisfaction levels of patients.
According to Zinn et al. (2016), satisfaction is the evaluation of various aspects of a health system. The four-factor solution established shows doctor care, nurse care, facilities, and support facilities as the determinants of inpatient satisfaction in Germany. With the exception of Opthalmology department, the factor structure was identical across all other medical departments.
Reddy Aileni (2003) examined the satisfaction levels of patients at various stages in a hospital. The significant steps which a patient goes through in a hospital are reception stage, examination process, pathology stage, and X-ray and other scanning processes.
Chahal et al. (2004) used technical and non-technical aspects of care to measure the satisfaction levels. Below average satisfaction levels were found in patients at government health services. The patients were dissatisfied with the hospital atmosphere, behaviour of staff, quality of administration, waiting time, and grievance handling. A considerable gap emerged between patient perception and expectation levels.
Radad et al. (2016) emphasised the importance of measuring patient satisfaction to find loopholes in the healthcare system in Palestine. Overall satisfaction of patients was measured using the accessibility of health centre, waiting time, health insurance and treatment cost, atmospherics, and quality of services offered. Patients gave maximum importance to waiting time and health centre accessibility.
Behavioural Intentions
Behavioural intentions are a person’s inclination to perform a particular behaviour. The propensity to perform a specific action emerges from the attitude towards a behaviour, perceived control, and subjective principles. WOM, revisit intentions, and willingness to pay a premium were the three items used to study the behavioural inclination of tourists (Lee et al., 2000). The indicators of consumer intentions used by Cronin et al. (2000) are (a) willingness to recommend services, (b) repurchase, and (c) positive WOM. In a study to measure the behavioural intentions of passengers on a cruise ship, Petrick (2004) used repurchase intentions and word-of-mouth constructs. Wu et al. (2008) measured behavioural intentions using the willingness to recommend, compliance with healthcare provider’s instructions, and repurchase intentions. Bloemer et al. (1999) measured service loyalty using the dimensions: purchase intentions, sensitivity towards price change, WOM, and complaining behaviour of customers.
Service Quality Customer Satisfaction and Behavioural Intentions
Lee et al. (2000) found that service quality leads to customer satisfaction. Satisfaction influenced purchase intentions more than service quality. Customers opt for services that provide them maximum satisfaction rather than the ones that offer high-quality services. In their empirical study, Chaniotakis and Lymperopoulos (2009) found that satisfied new mothers spread positive WOM about their treatment. Out of the service quality dimensions, only empathy directly impacted WOM recommendations. Tangibles, assurance, and responsiveness affected WOM indirectly via satisfaction. Swain and Kar (2018) used the 6Q quality framework to show that the six aspects of quality impact patient satisfaction levels, which then determine the behavioural intentions of patients in terms of their repeat usage, recommendations, and WOM. Cong and Mai (2014) established a direct relationship between the quality perception of patients in Vietnamese public hospital and their satisfaction levels. Tangibles such as dimension of quality exerted the maximum impact on satisfaction, followed by the attitude of staff and accessibility of services. Meesala and Paul (2016) found that responsiveness and reliability impacted patient satisfaction directly, which further is directly related to the loyalty of patients visiting private hospitals.
Wu et al. (2008) empirically verified the influence of patient’s perception of quality on patient satisfaction level. The quality perceptions exerted a direct impact on the patient’s behavioural intentions and also an indirect effect via patient satisfaction. A positive relationship existed between perceived value and patient’s intention and perceived value and patient satisfaction. Jandavath and Byram (2016) conducted an empirical study to show that high-quality services lead to satisfied patients, which in turn encourages them to revisit and recommend the healthcare facility. Patient’s loyalty and quality dimensions such as empathy, assurance, and responsiveness share a direct relationship. Fatima et al. (2018) developed a model to show that the five quality dimensions positively affect patient satisfaction. High satisfaction levels make patients loyal to healthcare services. A positive relationship exists between the quality dimensions and the loyalty of patients. Huang et al. (2011) confirmed the direct positive impact of perceived quality dimensions on satisfaction levels of patients. Satisfaction plays two roles between loyalty and quality dimensions. Satisfaction plays the role of both a moderator and a mediator between the service quality dimensions and purchase intentions of patients.
Patayawati et al. (2013) established a direct relationship between the patient’s perception of quality and their satisfaction level with the service, which further has a positive correlation with patient commitment and trust. There exists an indirect relationship between loyalty and satisfaction, mediated by patient trust and commitment. Zineldin (2006) showed that high technical and functional quality services lead to satisfied patients. These patients are also willing to recommend the hospital to others. Murti et al. (2013) found a direct correlation between quality and satisfaction, and an indirect relationship mediated by satisfaction between a patient’s behavioural inclinations and quality variables. Krishnamoorthy et al. (2016) empirically established that dimensions of quality such as trust, reliability, the process of admission, infrastructure, and care in the hospital, all affect the level of patient satisfaction.
Conclusion
Low quality of services may discourage patients from using healthcare facilities. This trend can be harmful to the productivity of an individual and for the country as a whole. Health is among the most salient concerns, and, therefore, delivering high-quality services should be a priority for all healthcare organisations. The study elucidates that effective management of service quality demands attention to healthcare quality dimensions as well as management of daily operations. Physical environment, professional care by hospital personal, interpersonal aspects of care, safety and security, the process of care delivery, facilities available, and accessibility are the broad dimensions of patient perception of quality identified from the literature. The rising competition in the healthcare sector and increasing patient awareness make patient perceptions a valuable healthcare quality indicator. Researchers and practitioners of healthcare institutions must pay attention to these aspects and use this work to better understand the three essential concepts of healthcare: patient satisfaction, healthcare perceptions, and behavioural intentions. These three concepts are interwoven with each other and are extremely useful to ensure the effective and efficient delivery of healthcare services. Negative perceptions of quality lead to dissatisfied customers who further choose to discontinue the medical services and spread negative WOM.
SERVQUAL is one of the most popular instruments to measure service quality in the service industry and has been used extensively in the healthcare setting (Al-Neyadi et al., 2016; Lee, 2005; Papanikolaou & Zygiaris, 2012; Peprah & Atarah, 2014; Turan & Bozaykut-Bük, 2016). However, no model has been developed for the healthcare industry, which is as established as SERVQUAL. The broad set of dimensions available in the healthcare literature is enriching. However, there is a need to develop an instrument that can serve as a benchmark in the healthcare literature.
The management should assess the provider’s performance based on both their technical adeptness and their ability to connect with the patients and attendants. In-service training programmes and regular feedback mechanisms in the form of satisfaction surveys can also help the providers understand the specific needs of their patients. Healthcare has several stakeholders, such as patients, service providers, healthcare administrators, and society. Every stakeholder values quality but perceives it differently. It is thus essential to form a broad and comprehensive healthcare model by accommodating the perceptions of all the stakeholders. The study can also be carried out separately at primary, secondary, and tertiary levels of healthcare as the quality indicators may vary for the services provided at these three levels.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.