
Abstract
Background:
The COVID-19 pandemic has profoundly impacted the country’s health systems and diminished its capability to provide safe and effective healthcare. This article attempts to review patient safety issues during COVID-19 pandemic in India, and derive lessons from national and international experiences to inform policy actions for building a ‘resilient health system’.
Methods:
Systematic review of existing published articles, government and media reports was undertaken. Online databases were searched using key terms related to patient safety during COVID-19 and health systems resilience. Seventy-three papers were included dependent on their relevance to research objectives.
Findings:
Patient safety was impacted during COVID-19, owing to sub-optimal infection prevention and control measures coupled with reduced access to essential health services. This was largely due to inadequate infrastructure, human and material resources resulting from chronic underinvestment in public health systems, paucity of reliable data for evidence-based actions and limited leadership and regulatory capacity.
Conclusions:
India’s health systems were found ill prepared to tackle large-scale pandemic, which has major implications for patient safety. The shortcomings observed in the COVID-19 response must be rectified and comprehensive health sector reforms should be initiated for building agile and resilient health systems that can withstand future pandemics.
Background
As the pandemic of Coronavirus Disease of 2019 (COVID-19) ravages the countries, the health systems have been largely caught ill prepared to tackle such unprecedented burden. The rising number of COVID-19 cases in India has laid bare the health systems’ capacity to sustain essential health service delivery while coping with additional burden of COVID-19 patients. The decades of chronic underinvestment in public health sector, sub-optimal availability, accessibility, quality and safety of health services has always been a matter of concern, but the pandemic has accentuated these gaps, highlighting safety risks for the patients and healthcare workers (Kaur, 2020).
Patient Safety
Patient Safety—defined as ‘the prevention of adverse events associated with health care to achieve zero avoidable patient harm’ (WHO, 2020d), is a benchmark for the well-functioning health systems and a fundamental element for achieving universal health coverage (UHC). Unless the health services are of good quality and safe, merely making them available is irrelevant, and could rather prove to be harmful. COVID-19 pandemic has also shown that the country health systems that are well prepared, adaptable and agile, are better able to respond and save lives (Quigley et al., 2020).
Resilient Health Systems
Health systems’ performance depends on the interplay of its six ‘building blocks’; Governance and leadership, health financing, health workforce, health information systems, medicines and medical products and the service delivery (Biddle et al., 2020; WHO, 2010). A resilient health system is aware of strengths and vulnerability in each of these building blocks, as well as the spectrum of risks to which it is exposed. More holistically, resilience is about ‘the ability of the health systems to prepare for and effectively respond to health crises while maintaining its core functions when a crisis hits, and to reorganize (adapt and transform) if conditions require it, based on lessons learnt during the crisis’ (Kruk et al., 2015).
Given that the country may witness multiple waves of COVID-19 outbreak as well as future pandemics, it is crucial to assimilate lessons from this pandemic response and work towards building more resilient health systems. Resilience is not only about bouncing back to the pre-crisis stage, but also about evolving into something better for next pandemic waves (Kruk et al., 2017). With this backdrop, this article attempts to review the patient safety issues that emerged during COVID-19 response owing to shortcomings in each of the six building blocks and derive learning from national and international experiences for building future health systems, capable of ensuring patient and health workforce safety and providing effective health services during the crises.
Materials and Methods
A systematic review of existing published and non-published articles and reports was undertaken, using online databases—MEDLINE, EMBASE, PUBMED—and Google Scholar. Besides the existing literature on health systems and systems resilience, the search was conducted covering the period after the first COVID-19 case was reported in, that is, 1 January 2020 to 1 October 2020. The search strategy used variants and combinations of search terms related to patient safety, COVID-19, health systems, resilience and health security. The studies included were in English language that covered patient safety concerns during COVID-19 in India and explored other country responses in strengthening health systems resilience from patient safety perspective over past years. We excluded articles if they covered topics that were not relevant to India. We located 1,187 articles, of which 197 were related to patient safety during COVID-19 and health systems resilience, and of that 73 were considered relevant to this review. The preferred reporting items for systematic reviews and meta-analysis extension for scoping reviews (PRISMA-ScR) guidelines was used to write and report the findings.
Findings
The studies extracted in the literature review did not directly report on levels of patient harm or quantify the adverse patient safety events during COVID-19 pandemic in India, however several studies mentioned potential impact of compromised health service quality and infection prevention and control (IPC) measures, reduced access to essential health services and delay in care seeking by the patients. All these factors make it is plausible that the patient safety incidents would be much higher during the COVID-19 pandemic given the increased patient load and outstretched health systems. Historically too, the patient safety incidence reporting and measurement in India has been weak, but the studies published earlier suggest a high risk of harm for users while seeking routine healthcare in India—for instance nearly, 5.2 million medical errors, and 3 million resulting disabilities and deaths occur annually in India (Jha, 2013), two-thirds of administered injections were unsafe (Arora, 2012) and one-fourth of intensive care unit (ICU) patients get sepsis (Shetty & Thakur, 2014).
The next section elaborates the key gaps identified in each of the health systems building block, which could adversely affect patient safety. We then present the options for building resilient health systems in the subsequent section, which are based on the national and international experiences, as identified in our literature review.
Current Gaps in the Health Systems and Potential Impact on Patient Safety
Service Delivery: Inadequate Infrastructure, Poor IPC and Disruption of Essential Health Services
Numerous issues were identified that could impact patient safety during COVID-19 pandemic, especially related to inadequate public health infrastructure; scarcity of hospital, isolation and ICU beds, inadequate triage and testing facilities, limited physical space and ventilation, lack of separate entry and exit gates. Besides sub-optimal infection and control measures; including facilities for hand washing and hygiene, contributed increased the risk of healthcare associated infections (HAI) amongst patients seeking care (Dwivedi et al., 2020; Kapoor et al., 2020; Sundararaman, 2020).
Furthermore, limited access and disruption in essential health services related to; maternal, newborn and child health (MNCH), nutrition, malaria, HIV/AIDS, tuberculosis (TB) and non-communicable diseases (NCDs) including dialysis, cancer treatment (Dore, 2020; Hebbar et al., 2020; Krubiner et al., 2020) and elective procedures (Goenka et al., 2020) as well as referral delays and service denial (Jain, 2020) have posed the increased risk of patient harm (Rukmini, 2020). There might be resurgence of vaccine-preventable illnesses (as MMR vaccination dropped by 69%, BCG by 50%, OPV by 39%), rise in mortality rates due to preventable chronic illnesses (as treatment of acute heart conditions dropped by 50% and oncology by 70%) and infectious diseases (as treatment and lab testing for TB declined by 80%, Hepatitis by 59% and malaria by 33%) (Sharma, 2020). It is estimated that each month of disruptions in TB treatment in India could cause an additional 40,000 TB deaths over the next five years (London School of Hygiene & Tropical Medicine, 2020; Stop TB Partnership, 2020). Additionally, TB patients, who received intermittent treatment during pandemic, are at increased risk of developing drug resistant disease in the coming years that costs 10 to 100 times more to treat a patient (Gupta et al., 2020). The widespread fear amongst patients and delay in seeking care, also led to psychological distress and potential evolution of mental health issues (Sahoo et al., 2020).
Health Workforce: Shortages, Stressful Work Conditions, Capacity and Communication Gaps
Absence and shortages of the treating health workers (HWs) resulted in delays of key clinical procedures for patients. India with its density of physicians (7.8 per 10,000 population) and nurses (21.1 per 10,000 population) is already far below the WHO threshold of 45 HWs per 10,000 population (WHO, 2016). COVID-19 infections amongst HWs and absence due to fear, quarantine or isolation further exacerbated this shortage, that resulted in work overload and longer duty hours for the remaining HWs, thus leading to burnout and making HWs prone to medical errors. Furthermore, growing incidences of harassment, violence and social stigma against HWs reported during pandemic, resulted in psychological distress and impaired their decision-making capacity for safe patient care (Narwal & Jain, 2020).
Limited staff knowledge and understanding of infection prevention and control (IPC) measures, including the use of personal protective equipment (PPE) was one of the key risk factors that compromised patient safety (Modi et al., 2020). Similarly, a study reported that laboratory staff was unclear about adequate sources for COVID-19 specimen (e.g. endotracheal aspirate) or its proper handling and management, which resulted in specimen collection delay or poor collection technique, false negative or false positive results. Staff failed to communicate patients’ COVID-19-positive or suspected positive status during handover to the other staff, during transfer to other department or hospital, thereby putting other staff and patients at risk (Karthik et al., 2020).
Health Information Systems: Lack of Real Time Surveillance and Patient Safety Information for Decision-Making
Currently there is no systematic mechanism for collecting or reporting data on patient safety incidents, especially in public healthcare system. Only few private hospitals collect such data that too is not widely shared, which limits the scope for cross learning and improving patient safety measures. The existing electronic health records (EHRs) and the digital data captured in public systems is also not adequately used—either to report, or predict, or reduce preventable harm. Moreover, there is no system for patient self-reporting of adverse event related to healthcare. ‘Causes of death’ data is incomplete and in many incidences, the comorbidities have been listed as an underlying cause of death, rather than suspected COVID-19 death (Pulla, 2020).
The lack of robust epidemiological and surveillance mechanisms made it difficult to obtain timely and accurate data and corrective actions, contributed to sustained community transmission of COVID-19 putting populations at risk, especially the people with comorbidities and older populations (The Lancet, 2020). Recently, Government of India has launched National Digital Health Mission (NDHM), which provides good roadmap for future, however the required infrastructure is currently unavailable. Also, concerns related to software and hardware failures, poor user interface, data safety and patient privacy and cyber-attack remain key concerns (Bajpai & Wadhwa, 2020).
Medical Products, Vaccines and Technologies: Shortages and Substandard PPE, Use of Medicines Without Clinical Evidence
Shortages in medical supply and quality of the products especially N95 masks and other PPE and disinfectants was major issue. Similarly lack of enough ventilators, oxygen and ICU medical supplies and poor maintenance of hospital equipment made it difficult to provide safe and effective health services. Laboratory products such a reagents and critical medications were also in short supply, especially during the initial months of pandemic (Garg et al., 2020).
Unauthorised use of medicines such as hydroxychloroquine and anti-retroviral drugs for prophylaxis and treatment of COVID-19 patients not only led to shortages of these drugs for malaria and HIV patients, but also exposed patients to major risk of adverse events (Tripathy, 2020). Unregulated dispensing and irrational use of several other medicines and injectable, also raised patient safety concerns (Ajay & Rathore, 2020).
Health Financing: Poor Financial Protection, Reduced Access to Services and High OOPE
Many patients and their families were forced to pay high costs of health services for emergency conditions as well as for COVID-19 treatment at private healthcare facilities. This led to high out of pocket expenditures (OOPE) and pushed many households into poverty (Thiagarajan, 2020). Public health financing is key to financial protection against OOPE, however the existing public health insurance schemes did not provide adequate safety net (Prinja & Singh, 2020). The public health systems remain chronically underfunded with only 1.6% of Gross Domestic Product (GDP) spent on health in financial year 2020 (FY 2019–2020), in contrast with current global average of 6%. The severity of the situation can be better understood by the fact that India ranks 170 out of 188 countries in government health expenditure as a percentage of its GDP (Tiwari, 2020). Additional Government funding for health during pandemic only had a beneficial effect in emergency health services, but not necessarily for strengthening the public health systems in longer term (The Lancet, 2020).
Leadership and Governance
Health is a ’state subject’ as per the Indian constitution, however the Governance capacity and political commitment for investing in health varies across the states (The Lancet, 2020). The sub-optimal coordination and intersectoral engagement in the COVID-19 response was documented in media reports (John, 2020). Also, there is limited capacity amongst Indian states in regulating the private and informal sectors in maintaining minimum standards for provision of good quality diagnostics, PPE and treatments or curtailing the costs of services (Chetterje, 2020). Similarly, technical capacity in monitoring, analysis of adverse events and quality assurance of health facilities and fraud detection is inadequate, as envisaged under National Patient Safety Implementation Framework (NPSIF). This systemic lack of effective Government stewardship further eroded people’s trust in public health systems that already heavily prefer private health sector due to perception of poor quality, lack of timeliness and responsiveness in the public health systems (Kumar et al., 2020).
Building Resilient Health Systems
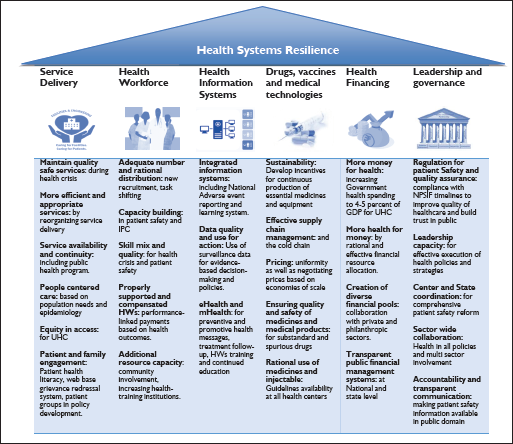
The proposed interventions for strengthening health systems resilience, are based on the WHO’s six building blocks framework, and have been summarised in the Figure 1. The global experience suggests that this menu of interventions will need to be contextualised and prioritised as per the needs, capacity and feasibility at national and sub-national levels. Not all of these interventions can be implemented overnight but would rather require prioritisation, mid to long-term strategic planning (Sundararaman, 2020), sustained investments and high levels of political and institutional commitment.
Improving Service Delivery, Quality and Safety
Building Future Health Workforce
Integrated Digital Health Information and Surveillance Systems
Health Systems Resilience for Patient Safety (WHO Health Systems Building Blocks Framework).
Augment Local Production for Access to Medicines and Medical Products
Investing in Health: More Money for Health, and More Health for Money
Strengthening Stewardship of Health Sector
Discussion
Patient safety concerns during COVID-19 response, were related to, inadequate infrastructure with sub-optimal IPC measures, limited accessibility and continuity of essential health services, scarcity of human and material resources, paucity of timely and reliable data for evidence-based decision-making, and limited leadership capacity which largely emanate from chronic neglect and underinvestment in the public health system.
The patient safety issues during COVID-19 pandemic have illustrated that several prerequisites for resilience were missing in our health systems. The lack of timely, complete and reliable epidemiological and health systems data because of sub-optimal information system and surveillance mechanisms was the major concern. Countries with standardised national electronic health information system can extract routine data on patient harm, real-time disease surveillance, clinical trials, and health system management, beyond early warning and response systems based on alerts and case notification. However, only United Kingdom, Finland, Denmark, Austria, Canada, Slovakia Estonia, Israel, and Singapore, have high technical and operational readiness to generate information from eHIS (Huguet & Kaufmann, 2020). This calls for more efforts in increasing funding for the required infrastructure as envisaged under NDHM for effective implementation of eHIS at point of care that could be utilised for patient safety incident reporting and learning systems, and also to lift technical and data governance barriers that prevent the effective use of such data, while respecting data privacy.
Early response is a defining feature of the health systems of Germany, New Zealand, South Korea, Taiwan and Hubei province of China, as well as in states such as Kerala in India—all of which have managed to provide safe patient care during COVID-19 (Sundararaman, 2020). However, responsiveness requires preparedness, which can take years of planning and investment, long before a pandemic hits. The government in these countries invested heavily on emergency preparedness and elaborate response protocols aligned with dedicated individuals and teams with decision-making autonomy to respond swiftly (Tabish, 2020). However, in India investments in healthcare are chronically low, that hinders its health systems preparedness and rapid response for safe patient care, which have been tested during COVID-19 pandemic. Furthermore India is ranked 57, on Global Health Security Index (2019) which measures countries, pandemic preparedness on their ability to handle the crisis, suggesting that India is more vulnerable to the pandemics and its debilitating impacts—both for lives and economy. The state of Kerala provides useful lessons while successfully managing current COVID-19 and earlier Nipah virus outbreak in 2018, by increasing government investments in public hospitals including the Aardram (Malayalam word for ‘people-friendly’) project, thus improving infrastructure and quality in the government hospitals, as well as winning the public trust (Nambiar et al., 2020; Rahim et al., 2020; Sundararaman, 2020). There is also a need for long-term investment in health infrastructure and a workforce and procedures for emergency procurement and replenishment of medical commodities, in the event of unanticipated shortages.
The crisis has exposed the importance of having adaptable health systems. Lack of any sort of excess capacity can leave countries vulnerable to an unexpected demand surge. However, there is chronic scarcity of resources in Indian health systems. Equipping health systems with reserve capacity will require creative approaches, such as a ‘reserve army’ of health professionals that can be quickly mobilised; storing a reserve capacity of supplies such as PPE; and maintaining care beds that could be quickly transformed into acute care beds. In China, Fangcang (Mandarin word meaning ‘square-cabin hospital’) shelter hospitals were rapidly set up in February 2020—large-scale venues such as stadiums and exhibition centres were converted to temporary hospitals to isolate and care for people with mild to moderate COVID-19 symptoms and reduce the burden on hospitals (Fang et al., 2020). The current crisis has offered huge opportunity for transformational change to address health systems strengthening activities. The resources dedicated in COVID-19 response to create organisational infrastructure, capacity and networks could be leveraged simultaneously in strengthening health systems for its resilience to cope with future epidemics and pandemics from the patient safety perspective.
Conclusion
The COVID-19 pandemic has exposed the need for our health systems to be more resilient to withstand crisis of such gravity while keeping patients and health workforce safe. A systematic and sustained approach with attention on all functions of health systems would be pertinent for pandemic preparedness. This requires high levels of political commitment, effective stewardship providing policy direction, strategic investments in health systems, especially in health infrastructure for safe service delivery, adequate number and distribution of trained and motivated health workforce, robust health information infrastructure for national digital health mission to be effective, local research and development, production and reliable supply chains of essential medicines, vaccines and medical products. The key lesson from the COVID-19 pandemic is that India needs to immediately start with the much-delayed investment in comprehensive health sector reforms, beginning with a substantial boost in public health financing. Only then the impact of future epidemics can be minimised, and patient safety can be ensured.
Footnotes
Declaration of Conflicting Interests
Funding
The author received no financial support for the research, authorship and/or publication of this article.