
Abstract
Background:
Since independence, life expectancy has increased substantially in India, but the goal of health-for-all has not been achieved yet. Hence, National Rural Health Mission was launched in 2005, and several strategies were implemented to strengthen the health system. Impact evaluation of the mission was done to learn lessons for future health planning.
Materials and Methods:
Logical evaluation framework was used to examine input, output and impact indicators systematically using time series data from Health Management Information System, National Family Health Surveys, National Sample Surveys and Sample Registration Scheme.
Findings:
After launch of the mission, fund allocation has increased nearly five times. The number of auxiliary nurse midwives has doubled, and the number of nurses has trebled. The number of accredited social health activists has increased to about one million. Institutional deliveries have increased from 38.7% in 2005–2006 to 78.9% in 2015–2016. Full immunisation coverage has increased from 43.5% to 62%. Oral rehydration solution (ORS) use in childhood diarrhoea has increased from 26% to 51%. Infant mortality rate has declined from 58 in 2005 to 33 per 1,000 live births in 2017 and maternal mortality ratio has also registered a decline from 254 in 2004–2006 to 122/100000 live births in 2015–2017. However, out-of-pocket health expenditure continues to be fairly high (69.3% of the total expenditure on health).
Conclusions:
Though National Health Mission has made a significant impact, the goal of universal care coverage is not yet fully achieved. Hence, capacity of health system needs to be trebled by a substantial increase in fund allocation.
Keywords
Introduction
In India, fertility and mortality indicators have improved since independence (Ministry of Home Affairs, 1971–2003); however, the goal of universal health coverage is yet to be achieved (World Health Organization, 2017). The government health system has become a predominant provider of preventive health services, but curative services have so far remained largely in the private sector. As a result, out-of-pocket (OOP) health expenditures have increased, affecting poverty eradication programmes (Selvaraj et al., 2018). Health expenditures are likely to increase further due to the rising trend of non-communicable diseases (NCDs) as revealed by the verbal autopsy-based causes of death reports (Causes of Death Statistics, 2010–2013). Communicable diseases such as TB, HIV, malaria, dengue etc. are still endemic. Moreover, government health system continues to be weak; only two doctors are supposed to look after about a population of 30,000 in rural areas (Rural Health Statistics, 2018).
Since independence, several efforts have been made for expansion of the government health system, but National Health Mission (NHM) is one of the large-scale programmes implemented in recent times (National Health Mission, 2013). The achievements and challenges of NHM need to be examined keeping in view the historical health system context and the current aspirations to achieve universal health coverage (Ayushman Bharat, 2018).
Health System Context
The health survey and development committee, set up before the independence, had recommended integration of preventive and curative services (Government of India, 1946). This report formed the foundations of health system development in independent India. At present, Chief Medical Officer (CMO) heads the health organisation in the district covering all promotive, preventive, curative and rehabilitative services, and a District Health Officer (DHO) and few Senior Medical Officers (SMOs) assist CMO for managing vertical health programmes such as TB, Malaria, reproductive & child health (RCH), and NCD, etc. The Director of Health Services (DHS) in each state and a Director General of Health Services (DGHS) at the country level are the top health administrators.
At the bottom of the health system pyramid are two health workers (1 male and 1 female) posted at a sub-health centre (SHC) to serve a population of 5000 in 4–5 villages. They are supposed to provide first-contact primary care. The primary health care team is led by a medical officer (MO) from the Primary Health Centre (PHC), where one male and one female health assistant support MO in supervising the health workers of five sub-health centres. PHCs provide outpatient care to a population of 30,000. A Senior Medical Officer (SMO) is head of the health organisation in a community development block, who looks after four–five PHCs.
Community Health Centre (CHC) is the first referral unit which serves about 100,000 population. Specialist doctors are supposed to be posted at CHC which also has about 30 beds and provides 24x7 emergency services. Each district has about 5–10 CHCs depending on its population size. And there are 2–3 government hospitals with 50–300 beds at sub-district and district levels. Beside the government health system, many informal medical practitioners also practice. Qualified medical practitioners are also available in the cities. Thus, health system in India is mix of government and private sector functioning side by side.
In the initial 25 years after independence, the main focus of government health system was on family planning and communicable disease control. Auxiliary nurse midwives and male health workers played a significant role in the development of primary health care in the rural areas. After Alma-Ata Declaration in 1978 (WHO, 1978), community health volunteers (CHVs) were trained to provide primary health care in every village (Maru, 1983), and traditional birth attendants were also trained for conducting domiciliary childbirths in hygienic and safe manner (Kakkar, 1980). Under the Integrated Child Development Services Scheme (ICDS, 1975), Anganwadi Workers (AWWs), were positioned in Anganwadi Centres (AWCs) to cater to about 200 households for delivering non-formal preschool education, supplementary nutrition and health check-up services to under-five-children and their mothers. These changes were articulated in the first National Health Policy (NHP) announced in 1983 (National Health Policy, 1983).
Despite these developments, the access to government health system has been limited, especially for the curative services; hence, people continue to utilise informal medical practitioners in the villages and urban slums (Chandra, 2017). As a consequence, the private health system has grown rapidly in the last few decades. Most of the people now utilise private health system for outpatient care and also for a substantial proportion of inpatient care (National Sample Survey Organisation, 2006, 2014). Health care utilisation by poor people is low compared to the rich. After a careful review of the emerging situation, NHP was revised in 2002, as Millennium Development Goals had renewed the emphasis on health development (National Health Policy, 2002). In this scenario, the Government of India planned the National Rural Health Mission (NRHM) in 2005 to move towards the universal health coverage (National Rural Health Mission, 2005–2012).
National Health Mission of India
Initially, NRHM was launched in selected states of India in 2005. However, later on, it was extended to all states, and a National Urban Health Mission (NUHM) was also launched in 2013. Now, NRHM and NUHM are the two parts of a unified NHM (National Health Mission, 2013). The aim of the mission is to have accessible, affordable, accountable, and effective primary health care for all. A major commitment of the government is to increase health budget from 0.9% to 2–3% of the gross domestic product (GDP). The major goals to be achieved by year 2018 were infant mortality rate (IMR) of 28/1,000 livebirths, maternal mortality ratio (MMR) of 100/100000 livebirths and total fertility rate (TFR) of 2.1.
Though most of the goals of NHM continue to be centred around mother and child health and family planning, major changes were made in the strategies (National Rural Health Mission, 2005–2012). The focus is not only on health but also on universal access to public services for food, nutrition, sanitation and hygiene with a more holistic approach. The emphasis is on comprehensive primary care with prevention of both communicable and NCDs in pluralistic health system where modern as well as traditional medical systems are utilised as per the needs.
Several approaches have been implemented to strengthen the government health system. There is a special focus on community involvement. Village health, sanitation and nutrition committees were set up in every village, and patient welfare societies (Rogi Kalian Samitis) were constituted in every government health institution. These committees have representatives of the local councils elected by the people and civil society organisations who are supposed to monitor health institutions as part of the community monitoring strategy. The community dimension was also strengthened by having one accredited social health activist (ASHA) in every village (1 for a population of 1,000)—a middle-age married/widowed/divorced women with elementary education who has communication and leadership skills (ASHA, 2005). The village council chooses ASHA from among the residents of the village. She is a volunteer who activates and links the community with the health service. She is paid a modest honorarium linked to her performance.
One of the major initiatives was to improve health management system. At state and district levels, health societies were set up which were backed-up by programme management units (PMU) to handle planning, health information, finances, etc. Innovations such as outsourcing or contracting of human resources or services, setting up of 24x7 emergency services and maternity care in selected PHCs, and, above all, monitoring systems using information technology (IT) were encouraged. Indian public health standards were declared for each type of health institution as a benchmark (Indian Public Health Standards, 2012).
Flexible funding was a new initiative. Demand side financing (Janani Suraksha Yojna, 2005) and risk pooling were also included in the strategy. Though Government of India had started Social Health Insurance Schemes (Central Government Health Scheme, 1954; Employee’s State Insurance Scheme, 1952) for organised sector employees soon after attaining independence, their coverage was limited. In 2008, the Government of India started Rashtriya Swasthya Bima Yojana (RSBY) (Rashtriya Swasthya Bima Yojna, 2008) as a social insurance scheme for unorganised sector workers. Many state governments have also started their own RSBY-like schemes for families living below the poverty line. In 2018, the Government of India has also launched Pradhan Mantri Jan Swasthya Yojana (PMJAY) to extend social insurance coverage to 40% of the households considered to be vulnerable (Ayushman Bharat, 2018).
The implementation of NHM is backed by a robust monitoring and evaluation methodology. Beside the routine administrative data, common review missions by stakeholders—independent monitoring committee with academics and development partners—also conduct inspections every year using qualitative methods (Common Review Mission, 2007). It is the right time to conduct independent evaluation of NHM to learn the lessons for future health planning and programming.
Materials and Methods
Logical framework approach was used for conducting the evaluation of NHM. The inputs, processes, outputs, outcomes and impacts were compared during the NHM implementation time period. Analysis of Government of India budget and rural health statistics was done to compute input indicators. Independently conducted household sample surveys such as National Family Health Surveys and National Sample Surveys conducted periodically by independent agencies were used to assess coverages. Sample Registration System data were used to assess the impact on infant and maternal mortality.
Findings
Since the launch of NHM, the fund allocation has increased about five times (Figure 1) (Janakiraman & Kapur, 2016). Health infrastructure has also registered a significant growth. The number of health institutions has increased, and the number of human resources has also almost doubled in NHM period (Table 1) (Rural Health Statistics, 2018).
Funds Allocation to National Health Mission by Governement of India (Indian Rupees in Crores).

The number of a new type of volunteer, that is, ASHA, who were inducted in every village, stands at about one million now. Most of them were placed in the initial 5 years of NRHM. They have linked the communities with the health services (Table 1).
Health Institutions and Health Workforce.

Coverage of Maternal and Child Health Indicators.

The proportion of fully immunised children in 12–23-month age group has increased from 43.5% to 62% in 2015–2016. Treatment of fever or acute respiratory infections (ARI) among under-five-children has increased from 69.6% to 73.2% and oral rehydration solution use in diarrhoea has increased from 26% to 51%. There is a decline in childhood undernutrition also.
Out-of-pocket Health Expenditures Per Hospitalisation (in ₹).

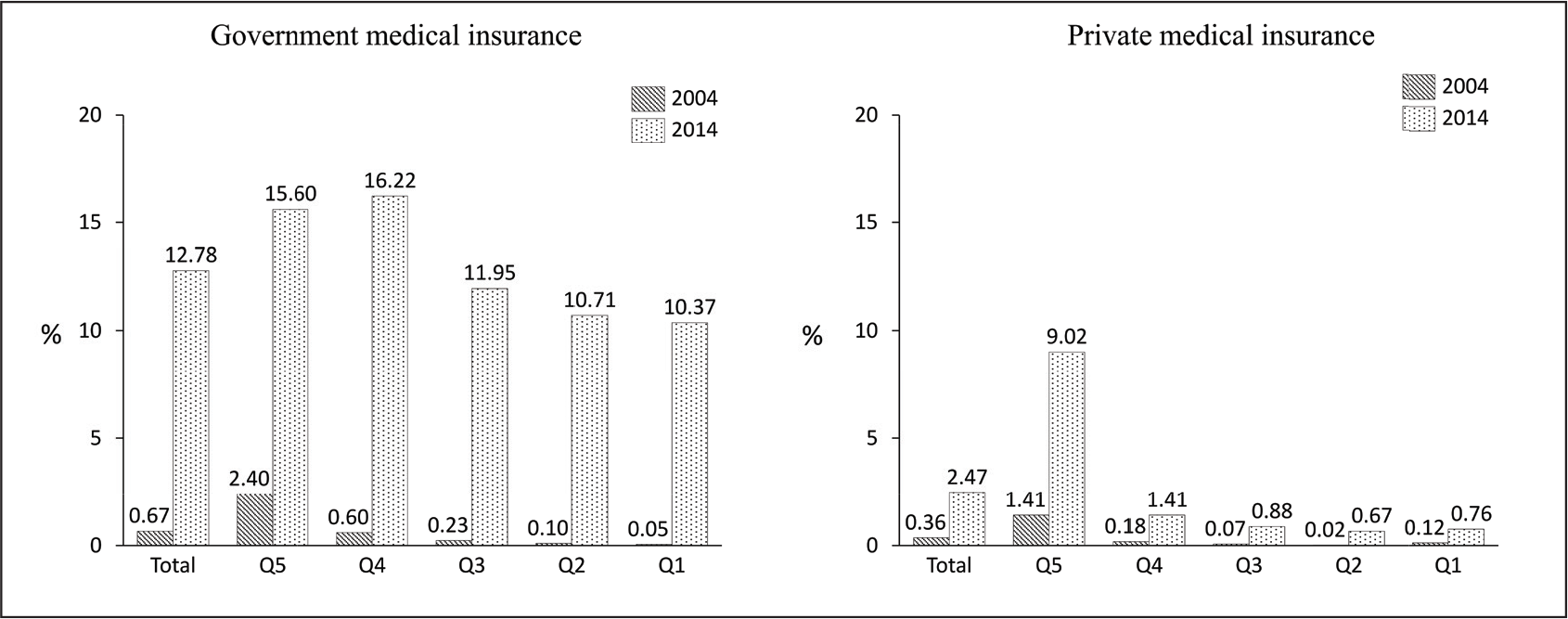
National Sample Survey Organisation (NSSO) data show that OOP on hospitalisation in government health services has declined (Table 3) (National Sample Survey Organisation, 2006, 2014; National Statistical Office, 2019). The coverage of government-funded social insurance schemes has also improved from 1% to 14%. Coverage is higher among the rich as compared to the poor (Figure 2). Rich people buy private medical insurance whereas poor people are covered mostly by social insurance.
Insurance Coverage (%) by Consumer Expenditure Quintile.
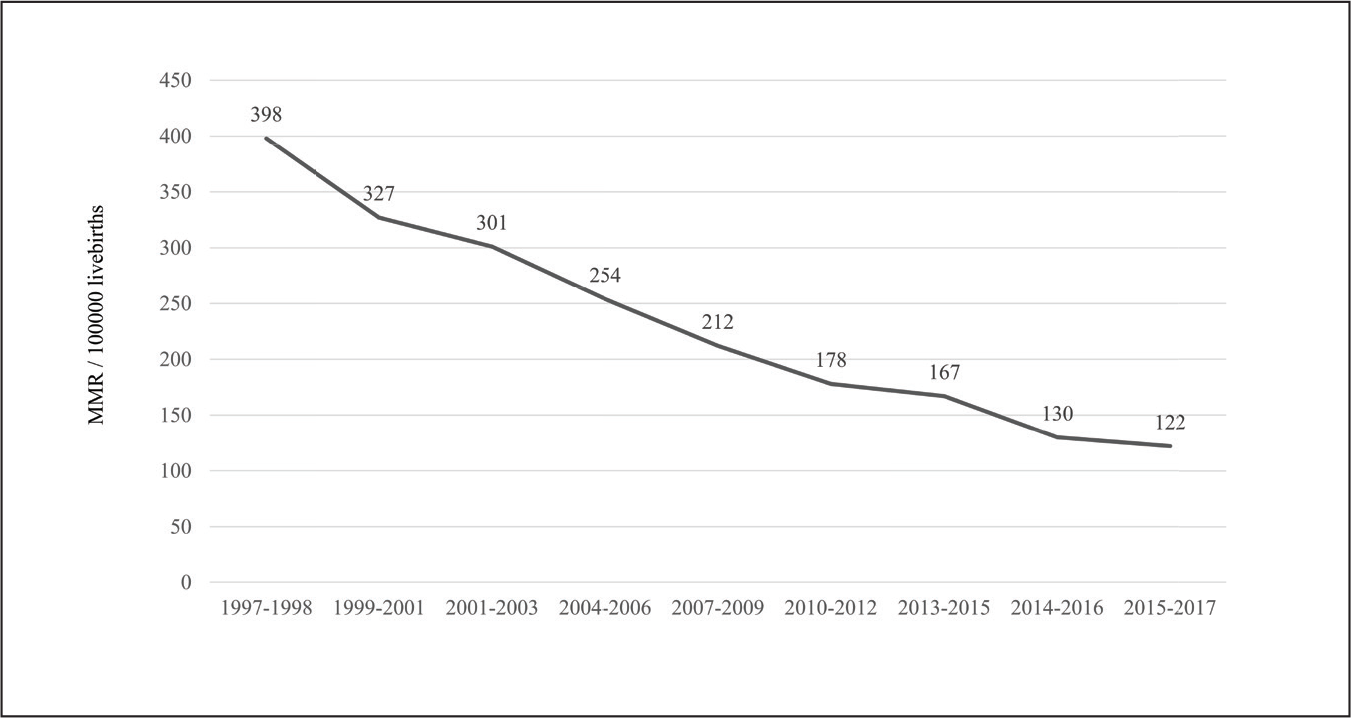
As shown in Figures 3 and 4, Sample Registration System (SRS) revealed that infant mortality rate has declined from 58 in 2005 to 33 per 1,000 livebirths in 2017, and maternal mortality ratio has also declined from 254 in 2004–2006 to 122/100,000 livebirths in 2015–2017 (Office of Registrar General of India & Census Commissioner, 2015–2017).
Infant Mortality Rate/1,000 Livebirths.

Maternal Mortality Ratio/100,000 Livebirths.
Discussion
National Health Mission has led to improvements in health status of Indian population as indicated by a faster decline in infant mortality—a sensitive indicator of population health—after the launch of the mission in 2005 (3.6% per year) compared to earlier 10-year period (2.2% per year). Logical Framework Approach (Levine, 2007) used for evaluating NHM indicates that huge changes have occurred in inputs (Table 1 and Figure 1), outcomes (Tables 2 and 3, Figure 2) and impacts (Figures 3 and 4) which have a logical temporal link. In one of the states of India, in multivariable analysis, the effect of NHM was found to be significant in reducing socio-economic, geographic and gender inequalities (Gupta et al., 2016).
Considerable progress has been made under NHM; however, many challenges remain. The goal of universal health coverage is yet to be fully achieved. The proportion of people experiencing impoverishment due to OOP health expenses is fairly high (Universal Health Coverage in India, 2017). Malnutrition is still a major problem. Almost 35% of the under-five-children are stunted in India (UNICEF, 2019). Health infrastructure is not yet adequate and there is huge shortage of human resources for health (Rural Health Statistics, 2018 –2019). Funding is still very low (Universal Health Coverage in India, 2017). Government spends merely about 1.2% of GDP on health. Most of the people who approach health services have to buy healthcare out of their pocket leading to exacerbation of poverty.
National Health Accounts data show that the OOP health expenditure is still quite high (National Health Accounts Estimates for India, 2018). Most of the OOP payment in government health institutions is for buying the drugs (Selvaraj et al., 2018) and diagnostics. Due to OOP health expenditures, every year about 69 million people in India fall below poverty line (Levinson, 2016). The coverage of social insurance scheme is still very low (National Statistical Office, 2019). The National Health Protection Scheme launched in 2018 is expected to raise it further in future (Ayushman Bharat, 2018).
After a careful look at the current situation, the Government of India had revised NHP in 2017 (National Health Policy, 2017). Key thrust continues to be on Comprehensive Primary Health Care. The Government of India has declared that all SHCs and PHCs will have one HWC by the year 2022 (Health and Wellness Centres, 2018). However, several supply- and demand-side issues need to be addressed. In the supply side, HWCs need to be well resourced. The capacity of government hospitals would also require substantial augmentation, especially in remote rural areas as private hospitals are not available in these areas.
Demand-side financing for comprehensive primary health care with gate keeping function can create incentives for people to practise prevention and seek care in primary health care facilities. As sufficient capacity is not yet available in government health system particularly for super speciality care; strategic purchasing from the private sector may be done in the short term. In the long term, expansion of government health system should be planned to keep the healthcare costs low along with the planning for adequate human resources (doctors, nurses, and technicians etc.). IT can also be leveraged to educate people, for sending reminders for follow-up and for building the databases for monitoring and accountability.
Conclusion
The National Health Mission has made a significant progress in strengthening the government health system which has resulted in acceleration of the decline in infant and maternal mortality, but OOP expenditures still continue to be high. Hence, public spending on health should be increased to about 5% of GDP so that NHM can be augmented further to deliver UHC at an affordable cost.
Footnotes
Acknowledgements
I would like to thank my colleagues Dr Shankar Prinja, Additional Professor, Dr DS Faujdar, PhD Scholar, Dr Jyoti Dikshit, Junior Research Fellow and Dr Sumit Kataria, MPH Scholar from the Department of Community Medicine and School of Public Health, Post-Graduate Institute of Medical Education and Research, Chandigarh for their assistance.
Declaration of Conflicting Interests
Funding Statement
The author disclosed receipt of the following financial support for the research, authorship and/or publication of this article: We did not receive any funds for this study.