
Abstract
Compared to its peers, India has always spent far less on health. This is slowly changing as are the drivers that are forcing some of these changes. Demographical and epidemiological changes have moved the disease burden away from communicable and maternal and childhood diseases to non-communicable diseases. More people are city dwellers and achieving UHC is one of Sustainable Development Goals. To tackle these commitments and shifting demands, in 2017, there was a committed move towards improving primary health care by introducing comprehensive PHC through health and wellness centres. These centres are close to the community and by improving the quality of care given and increasing the range of services that they provide, there should be an increase in access to health. However, much needs to be done to ensure that these centres will provide high quality care to the local populations. Training the healthcare workers needed to staff these HWCs will take time. Keeping the required funding to expand the programme will be challenging in the current fiscal space. There is a need to integrate care and flow of funds between primary and secondary care and empowering local populations to engage in governance of the HWCs will take time.
Keywords
Introduction and Major Challenges to Achieving Universal Health Care
By adopting the National Health Policy 2017, the Government of India agreed to increase access and availability of healthcare services to its population and continued the journey by achieving Universal Health Coverage (UHC), one of the Sustainable Development Goals (SDGs) by 2030. Between 2010 and 2018, the UHC service coverage index improved from 47% to 61% and with the current projections, it is estimated that this would reach to 75% by 2030.
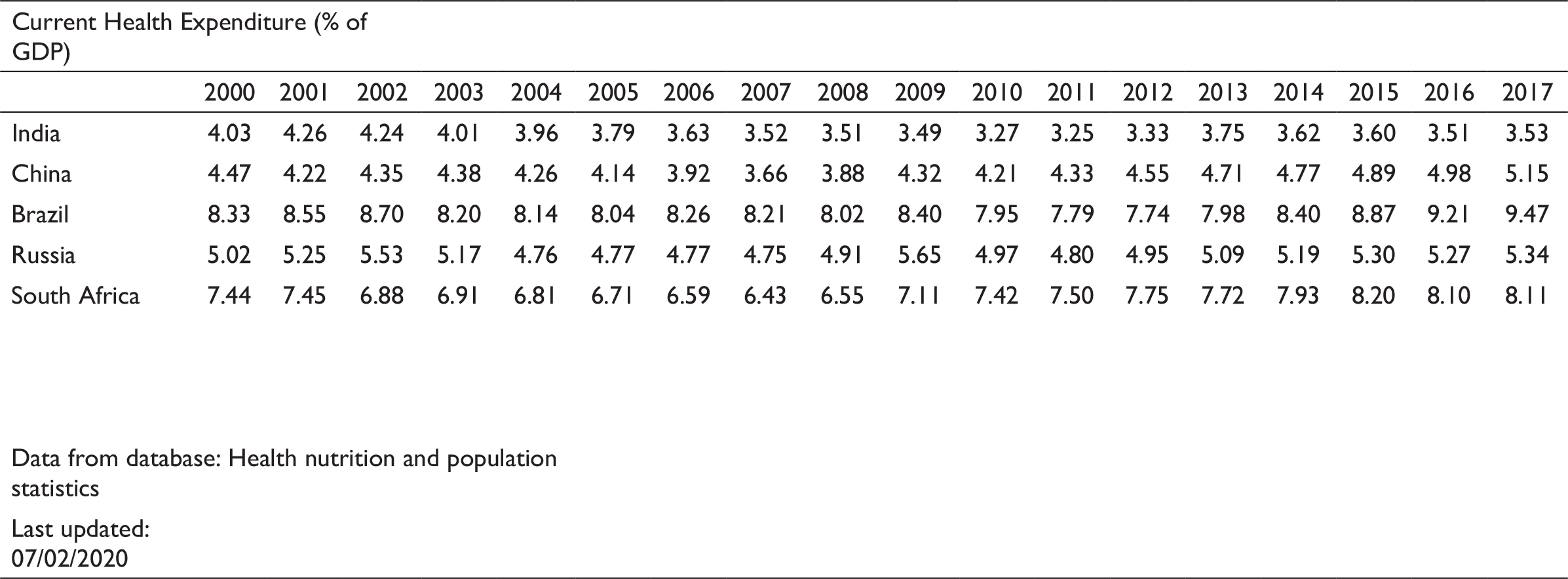
This is within the context that India historically spent a lower amount of its gross domestic product (GDP) on health compared to its peers or what has been recommended by international development partners such as the World Health Organization (WHO) and World Bank (WB). Figures 1a and 1b attest to this statement.
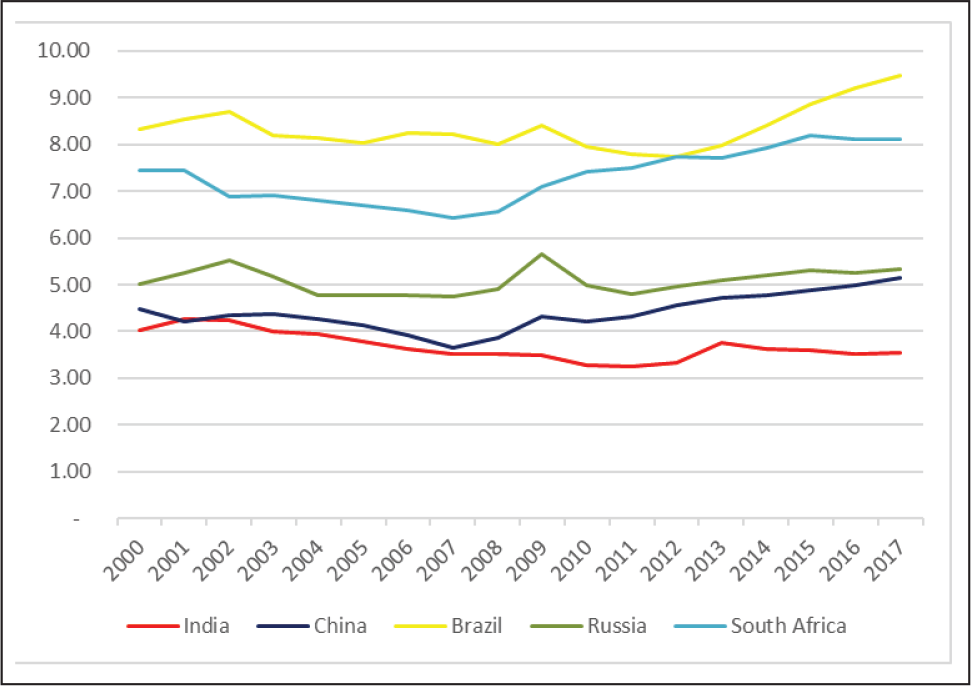
Source: World Bank data bank
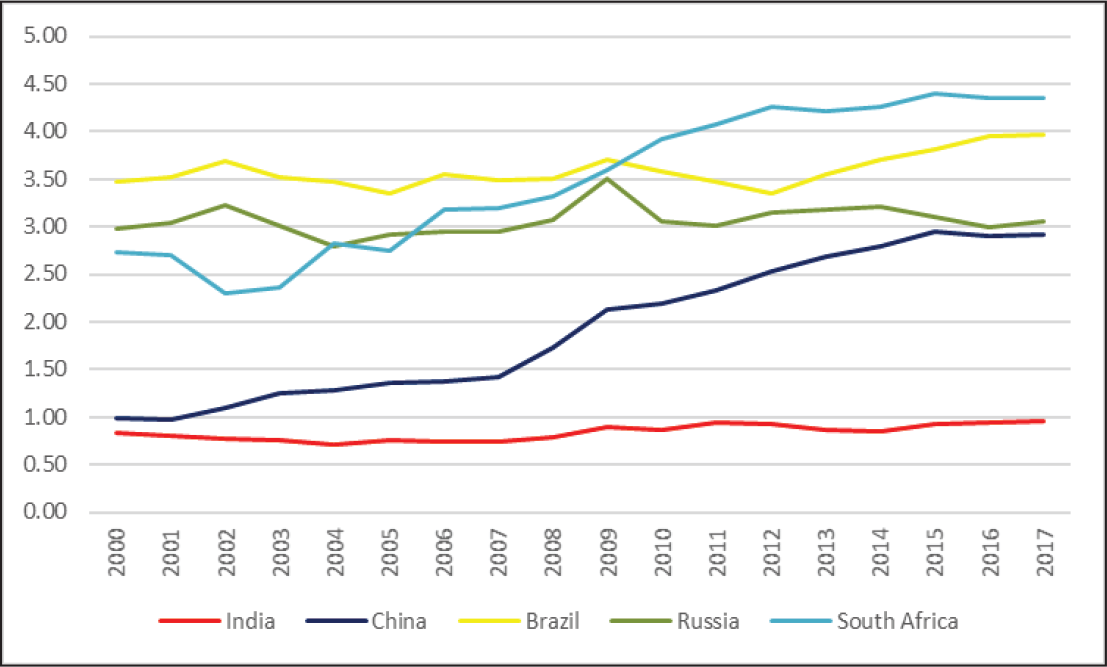
Source: World Bank data bank
Added to the low health expenditure, there are additional epidemiological, structural and political challenges that hamper achieving UHC goal. India is a transitional country epidemiologically and hence suffers from double burden of both communicable and non-communicable diseases (NCDs), although there is a definite shift towards NCDs (Figure 2). Changing disease patterns have major implications on the health system delivery as unlike majority of communicable diseases where the interaction with care providers is discrete and episodic, most NCDs are chronic, requiring long-term interaction with health care providers where emphasis is as much on maintenance and secondary prevention as on cure.
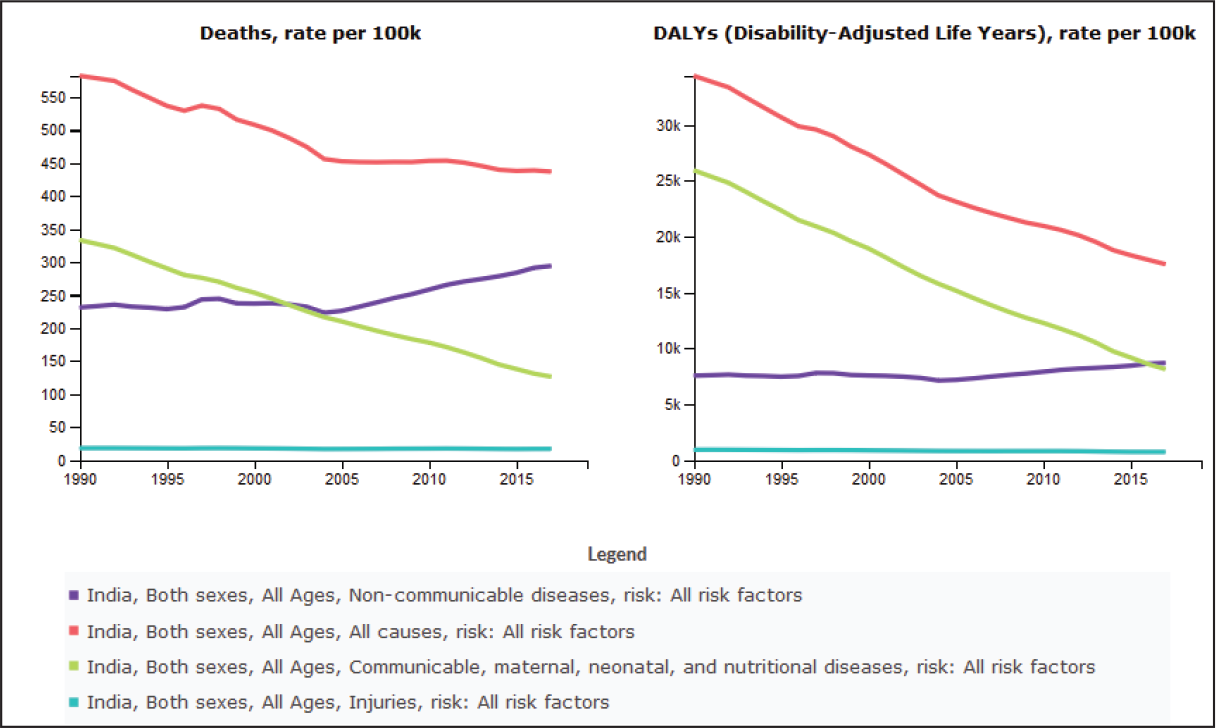
Source: IHME: India disease burden 2000–2017
Having the right kind and right number of health care workers at the right place at the right time is a corner stone of providing good-quality, accessible health care. Like many other countries in Asia, India suffers from both shortages and maldistribution of health care workers. The density of doctors, nurses and midwives in India was 25.8 per 10,000 population in 2018 , which is below the 44.5 per 10,000 threshold set up in the 2016 WHO Global Strategy on Human Resources for Health to achieve the health SDGs. Also, there is a maldistribution of health workers at the subnational level, in urban–rural areas and in public–private sector. The shortage of health workers is more acute in central and eastern states while higher in Delhi, Punjab and southern states. Whereas 68% of the Indian population lives in rural areas (as per last Census), there are only 34% of doctors and 33% of nurses work in rural areas. More than 80% of doctors and 70% of nurses work in the private sector (Karan et al., 2019). Other health workforce challenges include uneven quality of nursing and medical education and uneven performance of health workers while providing health services.
Added to this is the influence that certain cadres of health care workers exercise to block or slow down legislative procedures for expansion of the functions of other health care staff in what they traditionally see as their areas of practice. This in effect decreases the flexibility that policymakers seek in order to fill the gap in service provision by shifting some of the functions of one cadre of health care workers to another.
Finally, as public health and hospitals is a state subject in India, varied fiscal and governance capacities cause wide variations in health care services and outcomes. The complexity of funding sources and roles and responsibilities across national and state level leads to complex negotiations between national and state programmes. It also means that there are regional variations on how services are resourced, who they cater to and how they function.
Achieving Universal Health Care Through PHC: The Evolution of Services in India
A core feature of achieving UHC is strengthening of primary health care (PHC) ( Palagyi et al., 2019; Reddy et al., 2011; Stigler et al., 2016), especially a PHC sector that can prevent and manage chronic diseases close to patients, relieving the pressure on secondary care level to deal with more acute exacerbations of the disease. This will require a PHC sector that is structured and geared differently than what was envisioned in 2005 when the National Rural Health Mission (NRHM) was established.
The National Rural Health Mission, which evolved to become the National Health Mission (NHM) in 2013 now covers both rural and urban care and has the primary responsibility of being the engine for achieving UHC, with a focus on community, PHC and sub-tertiary care providers (Ministry of Health and Family Welfare & Government of India, 2014). However, even in the recent 12th Five Year Plan (2012–2017), NHM’s outcomes were focused primarily on maternal child health and communicable diseases with minor emphasis on NCD control (Palagyi et al., 2019; Planning Commission, Government of India, 2013).
In 2017, India adopted the National Health Policy which promises to increase public expenditure on health to 2.5% of GDP by 2025 (Ministry of Health and Family Welfare & Government of India, 2017). Appropriately, a new programme called Ayushman Bharat (AB) was launched in 2018 to streamline how services will be delivered. AB aims to achieve UHC and meet SDGs by moving away from sectoral and segmented approach to care delivery to a more comprehensive health care service approach. The scheme is divided into two interrelated components, Pradhan Mantri Jan Arogya Yojana (PMJAY) and Comprehensive Primary Health Care through the Health and Wellness Centres (HWCs).
Pradhan Mantri Jan Arogya Yojana is a government-funded health insurance scheme for the most disadvantaged 500 million people in the country. It aims to mitigate catastrophic health expenditures for its beneficiaries. Consequently, it mainly covers cost of in-patient care in pre-approved private and government secondary and tertiary hospitals up to a predefined ceiling.
Health and Wellness Centres are envisaged to be revamped primary health care facilities that will deliver comprehensive PHC (CPHC) in 150,000 sites across the country by 2022–2023. They focus on promotive, preventative and curative health services across 12 disease sets which include communicable, reproductive, maternal and child health services, as well as screening and management of NCDs (Ved et al., 2019). In addition, basic dental, mental, ophthalmic, care of the elderly and ear, nose and throat (ENT) services will be covered. To provide such a breadth of services at PHC level involves a paradigm shift and a need to move away from a model which focuses on episodic care in select diseases to service delivery that has to cater to chronic and episodic care across a much wider range of conditions.
This upgrading in both breadth and depth of services is being rolled out in a stepwise manner as there is a need to train staff. The initial phase will focus on more established reproductive and maternal child health services with additional added services like diabetes and hypertension. Other services will be introduced as training and supplies become available. In this article, we will only focus on HWCs as they are the backbone of the new revamped PHC strategy in India.
Challenges in Delivering CPHC Through HWCs
Funding of Services
Although the national health plan envisions health budget to be 2.5% of GDP by 2025, the reality so far is far lower, and the trends do not appear to support the increase in budget. As table 1 shows, budgetary estimates, combining central and state budgets for health for 2018–2019 and 2019–2020 tax years remained static at 1.25% and 1.26 % of GDP, respectively . More worryingly, based on the current projections, and even if we do not take into account government revenue constriction in 2020 and 2021 due to COVID-19 outbreak, the gap between funds needed and funds provided will increase . Great care must also be taken to ensure that the required budget for HWCs and primary health care are ringfenced and are not diverted to other parts of the health sector.
Health Care Expenditure Made by Union and State Governments (in ₹10 million).
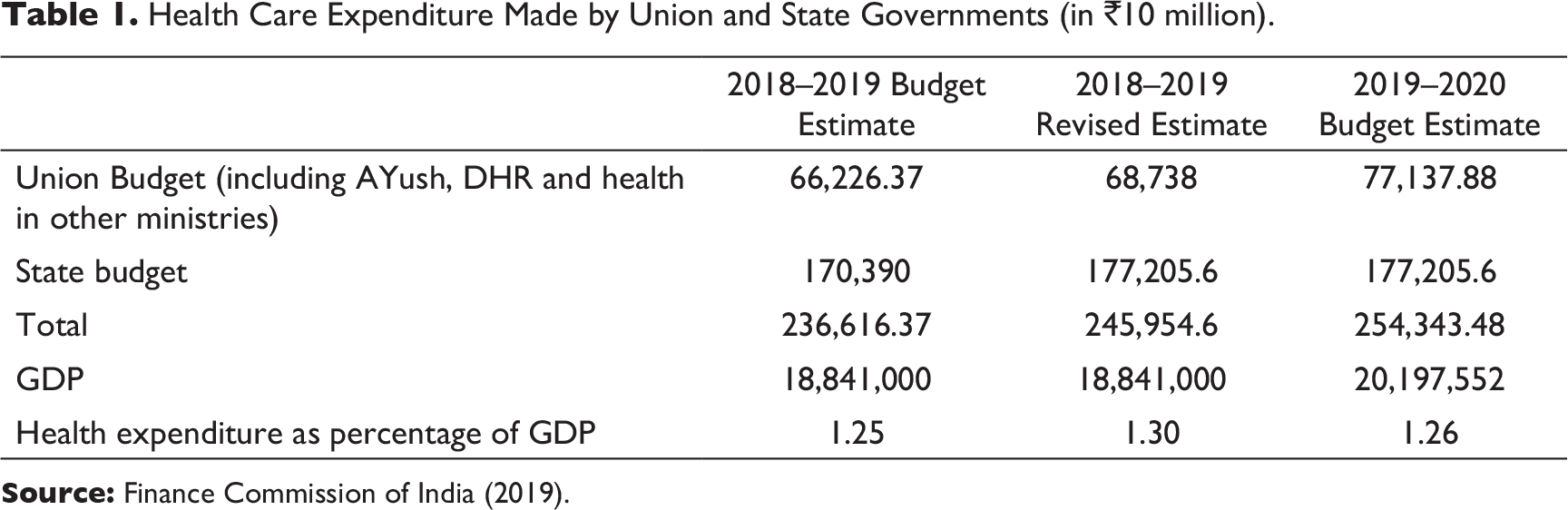
Source: Finance Commission of India (2019).
The Challenge of Staffing Health and Wellness Centres
The sub-centre-level HWCs are to be led by mid-level health care providers that are to come primarily from nurses (Bachelor nurses and general nurse midwives) and Ayurveda doctors, trained additionally for 6 months in public health and primary care to become community health officers. So far, this training has been provided primarily by the Indira Gandhi National Open University in district hospitals across the country. The Nursing Council has decided to revise the syllabus of BSc Nursing to incorporate additional elements of public health and primary care so that nurses can work as community health officers. This will help generate a large pool of mid-level providers capable of providing primary care at the sub-centre level HWCs from the BSc pass-outs.
Challenges remain in deploying the community health officers in the sub-centre-level HWCs., By June 2020, only about 25,000 Community Health Officers (CHOs) had been trained and deployed in HWCs as against the requirement of training and deploying nearly 125,000 CHOs needed for all the sub-centre-level HWCs. Moreover, the quality of the training and their motivation to serve at the sub-centre level, located mostly in small villages, will continue to be a challenge.
Service Provision
The chronic care management requires improved access to comprehensive person-centred care where health workers follow up patients over time and smooth integration between primary care and higher-level facilities. This requires that the 12 disease sets not be provided in silos but in a comprehensive and integrated way responding to patient needs. It also requires well-defined referral pathways that are well understood and adhered to and ideally facilitated by an information technology (IT) system to allow for effective two-way communication between PHC facilities and higher-level facilities of care. This also requires better integration between the twin components of AB, that is, HWCs and PMJAY insurance mechanism.
Another challenge in the provision of services in HWCs is the limitation of community health officers on prescribing medicines. They can dispense medicines previously prescribed by a medical doctor, but not initiate the prescription. This represents a challenge since a large number of basic disease conditions that can be effectively managed at the primary care level by CHOs have to be referred to a PHC or a CHC for a medical doctor to initiate the treatment. This hampers the credibility of the SC-HWCs and adds one more layer and extra cost for patients to get the treatment they need. The National Medical Commission bill represents an opportunity to regulate nurse- and mid-level provider prescription in India.
The other challenge is regularly enhancing the capacity and quality of PHC-level service providers to deliver wider set of services, since currently operationalised HWCs do not usually provide services for more than 7 or 8 of the 12 disease sets.
PHC in the Urban Settings
Prior to establishment of National Urban Health Mission (NUHM) in 2013 and even for many years afterwards, there was a potpourri of pilots, programmes committees and plans that tried to streamline PHC services in urban setting, most of which were focusing on curative outpatient services for the urban poor (Kumar et al., 2016). This is understandable as historically, the focus of the public health sector has been on rural health. However, urbanisation over the last few decades has meant that substantial numbers of urban poor have little access to health services. NUHM provides directions for comprehensive planning of urban health care structure but often, states do not allocate or spend the allocated budget (Kumar et al., 2018)
Especially in urban settings, the depth and breadth of the variation in health outcomes and service delivery indicators can only be seen if the data are disaggregated by location, since citywide data will be an average of poor and rich urban dwellers and often, the mobile urban poor are not even enumerated. This is particularly an issue in the urban setting as poor and rich neighbourhoods can coexist in same district or sub-district level, making data disaggregation more difficult.
As already mentioned, AB aims to develop a network of HWCs which provide treatment and follow-up, free medication and referral to higher levels. HWCs, once staffed and supplied with dispensable commodities as planned, can act as a major node for PHC services, improving access to services for the urban poor. Up to July 2020, a total of 3,336 Urban PHC sites were upgraded to HWCs (Ministry of Health and Family Welfare & Government of India, n.d.). However, unlike their rural counterparts, the urban HWCs are dealing with clients that are more affluent and expect to be seen by a Medical Officer rather than a CHO as is currently practised. In addition, the corner stone of service provision at HWCs is doing a robust enumeration of the catchment population. HWCs in urban areas are supposed to offer services to 50,000. They may be able to identify at-risk individuals at the slums fringing the big urban conurbations, but often residents in urban settings will not give the staff permission to enumerate them.
Role of the Private Sector
As of 2017, 72% of current health expenditure (CHE) in India was utilised in the domestic private sector (The World Bank, n.d.), and over 60% of CHE is met through the out-of-pocket expenditure, a significant proportion of which is spent on medicines and ambulatory services which will fall under HWCs remit. Introducing 150,000 HWCs that have better trained staff compared to private sector health centres with free diagnostic and medicines will pose a major challenge to the status quo and the dominant role of the private providers, especially in the ambulatory care, diagnostic labs and pharmacy sectors.
Unlike PMJAY which empanels and incorporates private providers in its hospital provider network, there is no clarity on the relationship between HWCs and their private counterparts. Competition with the private sector is more prominent in the urban setting than in rural, and anecdotal evidence shows that there is increased footfall in the rural HCWs compared to before. In the absence of any clear demarcation of roles and responsibilities, one can assume that private providers will do their best to keep their dominant share of the market
Ensuring Quality of Care
Health and wellness centres are tackling challenges of care quality in two different ways. Incremental rollout of training material for staff as they increase areas that they provide services and pay for performance incentivisation. At the national level, there are pre-agreed indicators with targets which form the basis of team-based, performance-based bonuses. Currently, a CHO can earn an additional 60% of their base salary from such bonuses. Most of the indicators are linked to maternal and child health activities and diabetes and hypertension screening. However, as the range of services increases, the number of indicators will also increase, and there will be a need to review performance-based incentives. Quality is also improved by putting in place systems that remind staff to do outreach activities for individual patients. As outreach for screening and follow-up of people with chronic diseases is an important pillar of HWCs, putting systems in place to facilitate this is an important quality step.
Interacting with the Local Community
One of the functions of HWCs is to focus on wellness and act as the primary focus in the community for health promotion and prevention campaigns. In addition, they will act as a hub for local accredited social health activists (ASHAs) who are the lynchpin between the formal health centre and the community. Consequently, there is much scope for interacting with the local community through everyday activities of HWCs, and in later years, there are aspirations to involve local communities in the social audit of the HWCs.
This process is a unidirectional flow from experts to the local lay people. It is not clear from documentations around establishing of HWCs whether there is a role or a mandate for local communities to be directly involved in influencing how local HWCs can deliver their services. Such empowering practices will improve acceptability of the centres by the local community and increase their effectiveness as has been shown in similar instances in other countries (Haque et al., 2020). Nonetheless, historically, there are other avenues, especially in rural settings, that allow for an element of oversight: The village health sanitation and nutrition committees that include men and women are well established and allow oversight of PHC services locally. In urban settings, the equivalent only involves women and focuses on maternal and child health services only and hence is not as well placed to review urban HWCs functions.
Innovations in Service Delivery
Multiple innovations are incorporated into how HWCs will deliver their services. At the system level, for the first time, ASHAs are becoming part of the PHC programmes and there is a move from care given by individuals to a team-based care delivery. Routine practices from other areas are being used innovatively to enhance the impact of activities in other fields; long-held practices such as microplanning to run immunisation and deworming campaigns are now used to plan outreach activities to screen diabetic and hypertensive patients.
Integral to the concept of HWCs is use of innovative technologies to support patients and help with referrals. In almost all states where HWCs are being rolled out, teleconsultations for specialist services are being provided via video conferencing, while in certain sites, patient details are sent electronically to hospitals prior to appointment (Ministry of Health and Family Welfare & Government of India, 2020).
On the wellness front, there is a big push to provide yoga sessions and a campaign to look at healthy eating is proposed to be rolled out through these HWCs.
Conclusion and Summary
To establish HWCs and make them the corner stone of PHC services many challenges had to be overcome. By August 2020, over 41,000 PHC centres, sub-health centres and urban primary health care centres have been converted to HWCs across all states with the exception of Delhi and Lakshadweep. This is in line with the rollout plan which envisaged 40,000 HWCs by April 2020. This is a major achievement considering the complexities involved in different health system delivery, regulatory and oversight mechanisms in various states that had to be negotiated.
Certain actions such as changing prescription refills from weekly to monthly, has been popular with patients and this has translated into increase usage, especially in the rural areas. However, as, it is becoming clear that the complex social milieu of patients and their aspirations in urban settings will mean that the current model of service delivery will not be as successful in urban areas compared to rural ones. Tweaking number and quality of staff in HWCs or redefining catchment areas may be needed to ensure their success. Other challenges that need to be addressed are allowing CHOs prescribing essential medicines in HWCs and improving the coordination between PHCs and secondary and tertiary public and private hospitals.
Health and wellness centres generate enormous amounts of data from routine information on service utilisation and performance indicators to surveillance data. However, any data collected must be reviewed and acted on rather than simply collated and archived. The importance of such follow-on actions was shown during the 2020 COVID-19 response where although fever cases were collected and reported up on a weekly basis, apart from a very few exceptions, no action was taken to link them with ongoing COVID-19 outbreaks. Similarly, there is a need to move beyond indicators that focus on input and processes and link performance payments to outcomes and outputs and to focus on response.
Finally, one must acknowledge that the concept of HWCs is a true paradigm shift to put PHC in front and centre of UHC and move away from individual, one-to-one care delivery system to team-based care. In the 2 years since roll out of HWCs started, much has been achieved while much more is planned. With the current downturn in GDP growth and decreased government finances in the short term, the big challenge to effectiveness of HWCs is ensuring that the promised funds for HWCs are provided, not only to roll out the numbers to 150,000 but also to make sure they go beyond maternal and child health and diabetes and hypertension screening, and provide full range of services across the 12 areas that have been envisioned.
Footnotes
Declaration of Conflicting Interests
Funding
The authors received no financial support for the research, authorship and/or publication of this article.