
Abstract
Ayushman Bharat is a flagship programme of Government of India and has been much publicised; however, the extent of its translation to the ground level has not been documented. A study was conducted to assess the implementation and satisfaction of the AB-PMJAY scheme in the inpatient department of AIIMS, New Delhi. Data were collected from January 2019 to June 2019. The sample size was a universal sample, and therefore, all the beneficiaries who availed the services at AIIMS, New Delhi were enrolled. A total of 120 patients were enrolled in the study. The mean age of the participant was 36.37 years, about 45.83% of the participants were illiterate and 69.17% resided in the rural area. A total of 88% of patients did not face any problem in availing the scheme, while 18% of the patients were asked to purchase medications from outside. Patients were highly satisfied with the ease and benefits of availing the scheme. The government should examine the reasons why some medications are being purchased from outside, and a contingency fund may be given to the hospital to prevent people from purchasing the medications from outside.
Introduction
India’s gross domestic product (GDP) was estimated to have increased to 6.6% in 2017–2018 and was expected to grow to 7.3% in 2018–2019. With approximately 1.33 billion population, India has a huge rural–urban population divide, and almost 70% of the Indian population live in the rural area. With such a large proportion of population still residing in rural India, the country faces a dual health care problem of communicable and non-communicable diseases. Some of the reasons for increased morbidity in India are lack of access and poor quality of medical treatment and huge out-of-pocket (OOP) expenditure ranging from thousand rupees to crores of rupees (The Wire, 2016).
The divide can be seen in the data provided by the Indian Consumer 360 survey, which reports that an Indian spends ₹9,373 annually on medical expenses. Consumers living in the rural area spend ₹6,371 annually, while those living in the urban area spend ₹11,387 annually on medical expenses. In India, around 6% do not seek health care due to financial reasons (National Sample Survey Organisation, Ministry of Statistics and Programme Implementation, Government of India, 2006), and about 30% of the rural population do not avail any medical services because of financial constraint. The WHO report also highlighted that because of high OOP expenditure, 3.2% of Indians fall below poverty line (BPL) (Ministry of Finance, 2022).
Several steps have been taken by Government of India in accordance with the National Health Policy 2017 to ensure universal health coverage mainly through health insurance and increasing government health expenditure as percentage of GDP from current 1.15% to 2.5% by 2025 (Ministry of Health & Family Welfare GoI, 2017). Insurance Regulatory and Development Authority (IRDA) documented that in the year 2017, about 76% of Indians did not have a health insurance. The Government of India announced an Ayushman Bharat Yojana-National Health Protection Scheme (AB-NHPM) in the year 2018 that was rolled out across all states/UTs in all districts of the country. The aim of this programme is to provide a service to create a healthy, capable and content new India, and it has two goals: (1) To create a network of health and wellness infrastructure across the nation to deliver comprehensive primary healthcare services and (2) To provide health insurance cover to at least 40% of India’s population which is deprived of secondary and tertiary care services. Under this scheme, all types of medical treatments, except organ transplantation, are provided for eligible families (Government of India, n.d.a, n.d.b; Lahariya, 2008).
This scheme will cover poor BPL families, deprived rural families and urban families whose occupational category has been identified as per 2011 Socio-Economic Caste Census (SECC) data. The AB-NHPM scheme will cover about 10 crore poor and vulnerable families (approximately 50 crore beneficiaries) by providing coverage of up to 5 lakh rupees per family per year for secondary and tertiary care hospitalisation. The benefit cover will also include pre- and post-hospitalisation expenses, and there will be no restriction on the size and age of the covered beneficiary family. The payment for medical treatment will be made on the basis of the approved package rate (as defined by the government). The package rates include all costs associated with treatment, and transaction of money to the beneficiary is paperless and cashless. The beneficiaries can avail benefits in both public and empanelled private hospitals. The estimated cost for the scheme is about ₹250 billion over 2018–2019 and 2019–2020 years for both centre and states. This scheme covers poor BPL families, deprived rural families and urban families for whom occupational category has been identified as per 2011 SECC data. This scheme covers over 10 crore families (approximately 50 crore citizens) across the country with a health insurance coverage of up to 5 lakh rupees per family per year for secondary and tertiary care hospitalisation (Government of India, n.d.a, n.d.b, Lahariya, 2008).
Since long, the Government of India is thriving to provide health coverage to the poor and vulnerable population; with this objective, a similar scheme by the name of RSBY (Rashtriya Swasthya Bima Yojana) was launched in 2008 by the Ministry of Labour and Employment (MoLE) in India (MoLE, 2008). Similar in nature, it had a comprehensive design to provide health care from public and private stakeholders, but due to intensive paperwork, the scheme did not take off as expected in the public sector (MoLE, 2014).
Since both the schemes are following the PPP model, it is requires institutional features, which include capacity of governments to manage contracts, regulate private providers, help raise capital and ensure a transparent procurement and oversight process that minimises cronyism and favouritism (Batley & Scott, 2010; Gentry & Fernandez, 1998; Kula & Fryatt, 2014). It is also documented that robust design and incentives to care providers are imperative for implementation of the scheme at a larger scale (Osborne & Gaebler, 1992).
The success of any government-implemented social scheme relies on the communication and the consequent level of awareness. Thus, it is important to assess the same in the case of the newly launched AB-PMJAY to explore any necessary course corrections, if required, in terms of communication. A study was planned to assess the level of awareness and satisfaction about the AB-PMJAY scheme among beneficiaries of this scheme in the indoor patient department of All India Institute of Medical Sciences (AIIMS), New Delhi.
Methodology
This study was a cross-sectional study conducted in the inpatient department (IPD) of AIIMS, a tertiary care hospital. AIIMS is one of the first institute which implemented the scheme. The study was conducted in the main hospital which consists of 1132 hospital beds spread across various specialties. Data were collected from January 2019 to June 2019 after due approval from the institute’s ethics committee. The study population were patients who availed the benefits of Ayushman Bharat and were admitted to the IPD of AIIMS. Patients who were admitted in the wards and availed the scheme were included in the study, while those who refused to provide the consent for the study were excluded. The sample size was a universal sample, and therefore, all the beneficiaries who availed the services at AIIMS, New Delhi, were enrolled. A questionnaire was designed and validated. It was then administered to the patients who had availed the benefit under the AB-PMJAY scheme in AIIMS, New Delhi, at the time of discharge.
Data were entered in EpiInfo 7.0.8.3. Data analysis was performed using Statistical Package for Social Sciences (Release 2011, SPSS Statistics for Windows, Version 20.0., Armonk, NY: IBM Corp). Variables were described as proportions or mean (SD), as applicable. A p-value of <0.05 was considered statistically significant.
Results
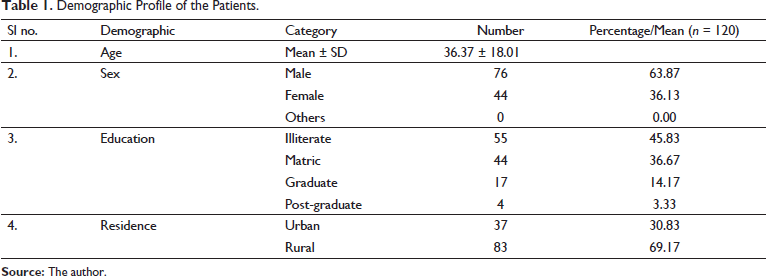
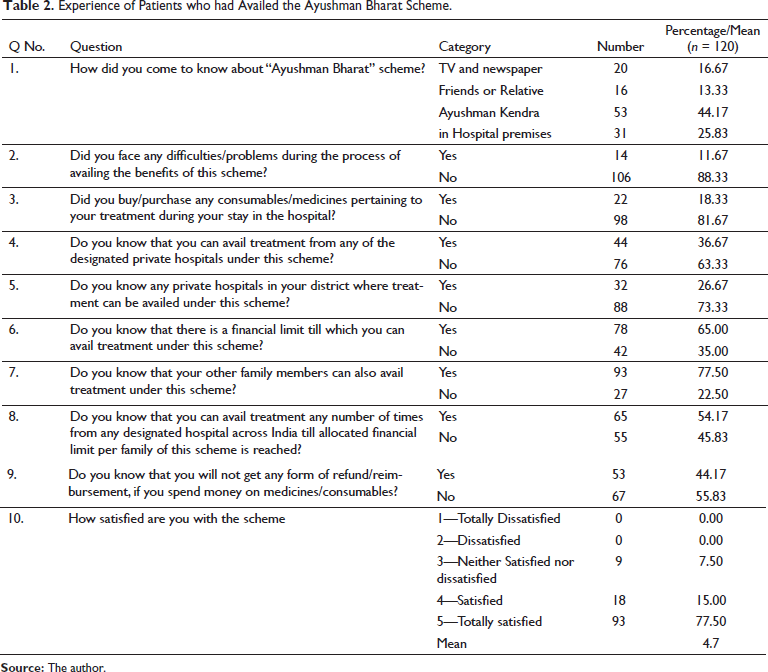
A total of 120 patients were enrolled in the study. The mean age of the participant was 36.37 years, the maximum number of participants (63.87%) were males. About 45.83% of the participants were illiterate, and 69.17% patients resided in the rural area (Table 1). About 44% of the patients knew about the scheme from the Ayushman Kendra set up in the hospital. A total of 88% of patients did not face any problem in availing the scheme, while 18% of the patients were asked to get medications from outside. About 44% patients did not know that they can avail the scheme from private hospitals near their residing area. Almost 92% of the patients were satisfied with the scheme and delivery of the scheme (Table 2).
Demographic Profile of the Patients.
Experience of Patients who had Availed the Ayushman Bharat Scheme.
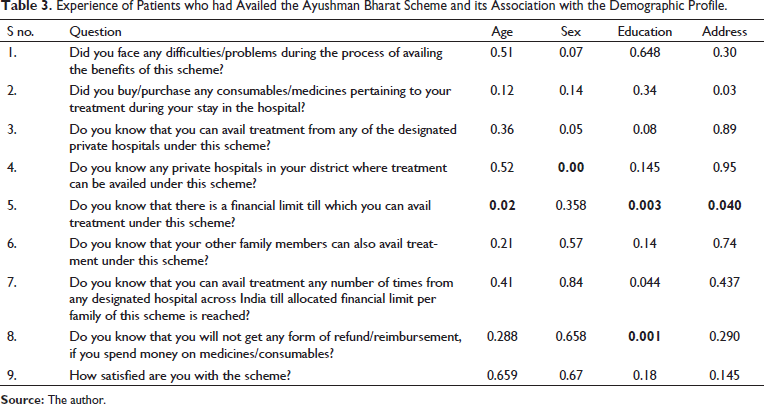
The result showed that the urban population purchased more medicines from outside during the hospital stay. Male participants were not aware about other hospitals in the district which provided the Ayushman Bharat scheme. Age and education were the determining factors in understanding the financial details of the scheme. Education also played a role in making the participants aware of the reimbursement policies of the scheme (Table 3).
Experience of Patients who had Availed the Ayushman Bharat Scheme and its Association with the Demographic Profile.
Discussion
The Ayushman Bharat scheme combines two initiatives announced in a single programme. These two initiatives will meet the range of health care needs across primary, secondary and tertiary care; they appear synergistic and may help in increasing accessibility, availability, appropriate care and affordability. The financial coverage in the AB-NHPM scheme is around 17 times more generous than the RSBY scheme and two to four times more generous when compared with the other state government-funded health insurance schemes in India. There appears a political will and commitment for the Ayushman Bharat programme (ABP) in India. The community and civil society play a crucial role in ensuring that political promises and commitments are sustained in changing political environment (Hughes & Leethongdee, 2007; Webster, 2002).
A study conducted by Quynh and Dhar (2014) on the Vietnam health insurance scheme showed that people were not satisfied with the scheme provided for health insurance as the poor are issued a free health insurance card, enjoy 95% reduction/concession in hospital fees and should be taken care of in the same way as all other individuals who possess the health insurance card. This also means that poor people receive the same quality of health care services as other better-off individuals who still need to pay from their pocket. They were also not satisfied with the preauthorisation process to avail the scheme. But in our study, the awareness and satisfaction level was high due to the fact that the processes were well thought off and all the procedures were free of cost, wherein patients were not spending a single penny from their pocket.
A study by Pattnaik et al. (2019) showed that commercial insurance companies achieved a satisfaction of 46%, while government-sponsored schemes like Central Government Health Scheme (CGHS) and Employees’ State Insurance Corporation (ESIC) have a satisfaction score of 83%, which is almost double than that of the commercial insurance schemes. A study conducted by Sarker et al. (2018) showed that people were satisfied with the health insurance scheme of the government in Bangladesh. These results are comparable to our study where government sponsored schemes have higher satisfaction rate.
Once the beneficiary is identified and gets into the system, the overall experience is reportedly good. The systems built into the functioning of the scheme have been very efficient and effective. About 82% beneficiaries reported that they did not have to purchase anything, and 88% reported that they did not face any kind of difficulties/problems while availing the benefits of the scheme. For a new scheme, these are very encouraging findings. About 78% of the beneficiaries who availed the scheme reported to be extremely satisfied with the scheme. None of the beneficiaries interviewed reported any form of dissatisfaction about the scheme. These results again reflect the excellent systems and policies adopted for operationalising the scheme.
The result showed that the urban population purchased more medicines from outside during the hospital stay. Age and education were the determining factors in understanding the financial details of the scheme. Education also played a role in making the participants aware of the reimbursement policies of the scheme. Randolph and Viswanath (2004) in their review have noted that the mass media campaigns of the government will have to compete with media messages from a myriad of sources for public attention. They have noted factors that can lead to success of the mass media campaigns, which include (Bang et al., 2019):
Influencing the information environment and maximising exposure Creative marketing and messages Creating supportive environment Developing campaigns with a careful understanding of the determinants Process analysis and especially assessing exposure to campaign messages could serve as useful intermediate markers both in making midcourse correction and in explaining final campaign outcomes.
A study conducted in India on social marketing by Archana Singh et al. explored the possibilities of leveraging social marketing for social entrepreneurial ventures (SEVs). Implicit or explicit applications of marketing principles for social good is called ‘social marketing’. Social marketing is finding increasing applications in various domains ranging from poverty alleviation and education to health care (Singh et al., 2015). Its principles can also be factored in while designing mass media campaigns.
considering contextual factors, partnering and networking, community focus and innovative strategies, major role for technology and customise promotion techniques for local needs
Conclusion
The scheme was well received by general population visiting a tertiary care hospital. The AB-PMJAY is a very ambitious scheme that has taken off well. The overall beneficiary experience is found to be very good, which points towards a robust system/mechanism that the scheme has adopted. However, significant work needs to be done on the communication front wherein the fine lines have been clearly missed. The overall success of the scheme hinges around an effective communication strategy. An innovative approach by making the whole awareness drive market driven with a major role for technology can be a game changer.
Recommendations
The Ayushman Kendra had a huge impact in utilisation of the scheme in government hospitals where the people received all the information and were facilitated. These kendras should be opened in private hospitals for better awareness and utilisation of the scheme in private hospitals. The study also gives an insight that regardless of the packages made, one fifth of the patients required medications from outside which were not reimbursed; hence, proper funds for contingencies may be earmarked for patient convenience. Satisfaction survey should be conducted across hospitals for further improvement of the scheme.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.