
Abstract
A strategic approach to internationalize learning in higher education institutions is to use the curriculum and classroom cultural diversity to create opportunities to broaden students’ intercultural perspectives, appreciate sociocultural variability in professional practice, and improve their intercultural interaction skills. There is no clear consensus, however, on how to “link the global classroom to the global workplace.” The article examines an evidence-based approach to embed intercultural competency development in classroom teaching using an established intercultural resource (EXCELL) in an international human resource management course; a general communication course; a pharmacy course comprising only Saudi Arabian students; and a generic first year pharmacy course. Subsequently, stakeholder analyses with Business, Nursing, and Pharmacy academics and professionals led to the development of intercultural critical incidents for the curriculum. Strengths and limitations of the intercultural resource and recommendations for incorporating intercultural competency development in curriculum design in Business and Health disciplines are discussed.
Keywords
Background
Many universities around the globe now incorporate the development of global perspectives as one of their graduate attributes. Clifford and Joseph (2005) remind us that such development needs to be coupled with cross-cultural capability to participate professionally and socially in a multicultural environment. Cross-cultural capability is related to intercultural competence, which is defined as “a dynamic, ongoing, interactive, self-reflective learning process that transforms attitudes, skills and knowledge for effective communication and interaction across a range of cultures and contexts” (Freeman et al., 2009, p. 13). Given the more affective and transformational nature of this learning, it is less readily incorporated into professional development and curriculum redesign (Leask, 2008; Mak, 2010; Mak & Kennedy, 2012).
Despite the extensive scholarly discourse on internationalization of the curriculum (IoC) to date, the complexity of the pedagogical challenge requires academics and practitioners to continue to explore, document, reflect, and share their practices in a spirit of collegiality as there is no single solution to this contemporary question. Notably, the field has now matured to such an extent that the focus of analysis has shifted from debating the rationale for the internationalized curriculum, to more fine-grained examination of what constitutes good practice in different disciplinary and interdisciplinary contexts.
This article contributes to the discussion of disciplinary perspectives and possibilities by reviewing four case studies where an evidence-based intercultural skills program that focuses on the development of six generic social competencies (EXCELL) has been embedded in diverse courses. Also, we discuss selected processes and outcomes of a 2-year priority project titled “Internationalisation at Home.” Funded by the Australian Government Office for Learning and Teaching (formerly Australian Learning and Teaching Council), the project aimed to enhance the capability of faculty to incorporate intercultural competency development in curriculum design and delivery of Business and Health courses. As part of the project, stakeholder analyses informed the development of intercultural critical incidents for use in the curriculum and in preparation of students for their workplace internships.
The primary questions under investigation here are
What have we learned, from the case studies, about the utility and limitations of incorporating an existing intercultural resource (the EXCELL Program) in intercultural competency development in Business and Health curricula?
Based on analyses of consultations with academics and professionals, what have we found from applying the EXCELL generic competencies framework to the classification of challenging intercultural scenarios in classroom and practice settings?
In the next section, we examine the importance of intercultural competency development in Business and Health disciplines, before outlining the components of EXCELL. Next, we review how EXCELL has been embedded in four Business and Health courses. We will follow this by reporting on challenging intercultural social scenarios generated by stakeholders from Business, Pharmacy, and Nursing. A discussion based on the case studies and stakeholder analyses will provide the foundation for a strategic approach linking generic social skills development to intercultural competency development in diverse disciplines.
Intercultural Competence in Business and Health Disciplines
Far more attention has been given to the development of global perspectives and internationalization of the curriculum (IoC) in Business studies than perhaps any other discipline (Caruana & Ploner, 2012; Lilley, Barker, & Harris, in press). The reasons why Business has led the way include the drivers of the global business environment, and the comparatively higher enrolment of international students in business courses. This has certainly been the case in the United Kingdom, United States, and in Australia, where in 2010, 28% of higher education students were from overseas, and more than half of these were enrolled in Management and Commerce programs (Department of Education, Employment and Workplace Relations, 2011).
While many Business departments may have grappled with what it means to internationalize business education, a lack of consensus remains about how to “link the global classroom to the global workplace” (Ramburuth & Welch, 2005). Barker, Hibbins, and Woods’ (2012) study of Business students (majoring in Tourism and Hospitality management) identified that effective communication training needs to be tailored more closely to professional contexts requiring teamwork, especially with people from culturally and linguistically diverse (CALD) backgrounds.
Similarly, students involved in practicum in diverse health settings need to have well-developed intercultural communication skills to provide safe and effective health provision in a multicultural society (Lester, 1998). Clinical facilitators play an instrumental role in socializing all students into the culture of the clinical environment, as well as modeling culturally competent health care provision (Shaya & Gbarayor, 2006). Previous research has highlighted that pharmacy students can easily adopt negative stereotypes toward the more diverse and vulnerable elements within the client population (Chen, LaLopa, & Dang, 2008), and hence professional education needs to confront stereotyping and other barriers that may interfere with optimal care of clients (Maganlal et al., 2012).
Professional development opportunities are needed by faculty, clinicians, and practicum supervisors to enhance their capacity to create an environment that values learning about each other’s cultures and promotes quality intercultural contact (Sanderson, 2011). Ho, Holmes, and Cooper (2004) and Ward (2006) suggest the use of evidence-based training resources such as the EXCELL Intercultural Skills Program (Mak, Westwood, Barker, & Ishiyama, 1998) to enable international students and migrants to extend their repertoire of social interaction skills in the new culture. More recently, Caruana and Ploner’s (2012) critical review of contemporary practice and educational research in internationalization within the business education subject communities endorsed EXCELL as “a best practice intercultural social effectiveness program designed from established principles of learning” (p. 25).
EXCELL: An Established Intercultural Development Resource
EXCELL is a schematic, skills-based professional development resource centered on the teaching of six generic social competencies: seeking help, making social contact, participation in a group, refusing a request, expressing disagreement, and giving feedback (Mak, Westwood, Ishiyama, & Barker, 1999). In practice, any intercultural social interaction may involve multiple generic social competencies. For example, if a student wants to disagree with his or her tutor about marks deducted from an assignment, the primary competency is “expressing disagreement.” However, if the interaction occurs face-to-face (e.g., during the tutor’s consultation hours), it is likely the student would greet the tutor and make “small talk” before raising their dissatisfaction with the mark. The interaction could also be seen to involve the student “giving feedback” to the tutor. For example, the student may refer to the lack of written comments by the tutor to help explain their marking decisions. In other words, “expressing disagreement” about the mark received requires several generic competencies to be enacted.
As intercultural encounters can pose high levels of social anxiety and sometimes involve high stakes, it is important for students to understand what behaviors are considered appropriate in the interaction. While these competencies are challenging for many students from CALD backgrounds and shy students regardless of their background, they are fundamental to effective intercultural interactions in culturally diverse classrooms and workplaces.
The complete EXCELL process teaches each generic social competency in five stages: Alliance Building to engage participants and show respect for their cultural background and life experience; Cultural Mapping to build understanding of behaviors appropriate for a specified social scenario within a cultural context; and the practice and applied stages called Cultural Coaching, Contracting, and Transfer beyond the classroom (Westwood, Mak, Barker, & Ishiyama, 2000). The complete EXCELL process (comprising six sessions of 2-3 hr each) is recommended where systematic training of behavioral competence is required.
Case Studies in Discipline-Based Intercultural Competency Development
This section discusses four instances or case studies where EXCELL was embedded in different disciplines in two Australian universities: a third year business course, a general communication course, a pharmacy course for Saudi Arabian students, and a first year pharmacy course. Table 1 summarizes the sample, outcome measures, results, and limitations of each trial.
Summary of Cases Incorporating EXCELL in the Curriculum.
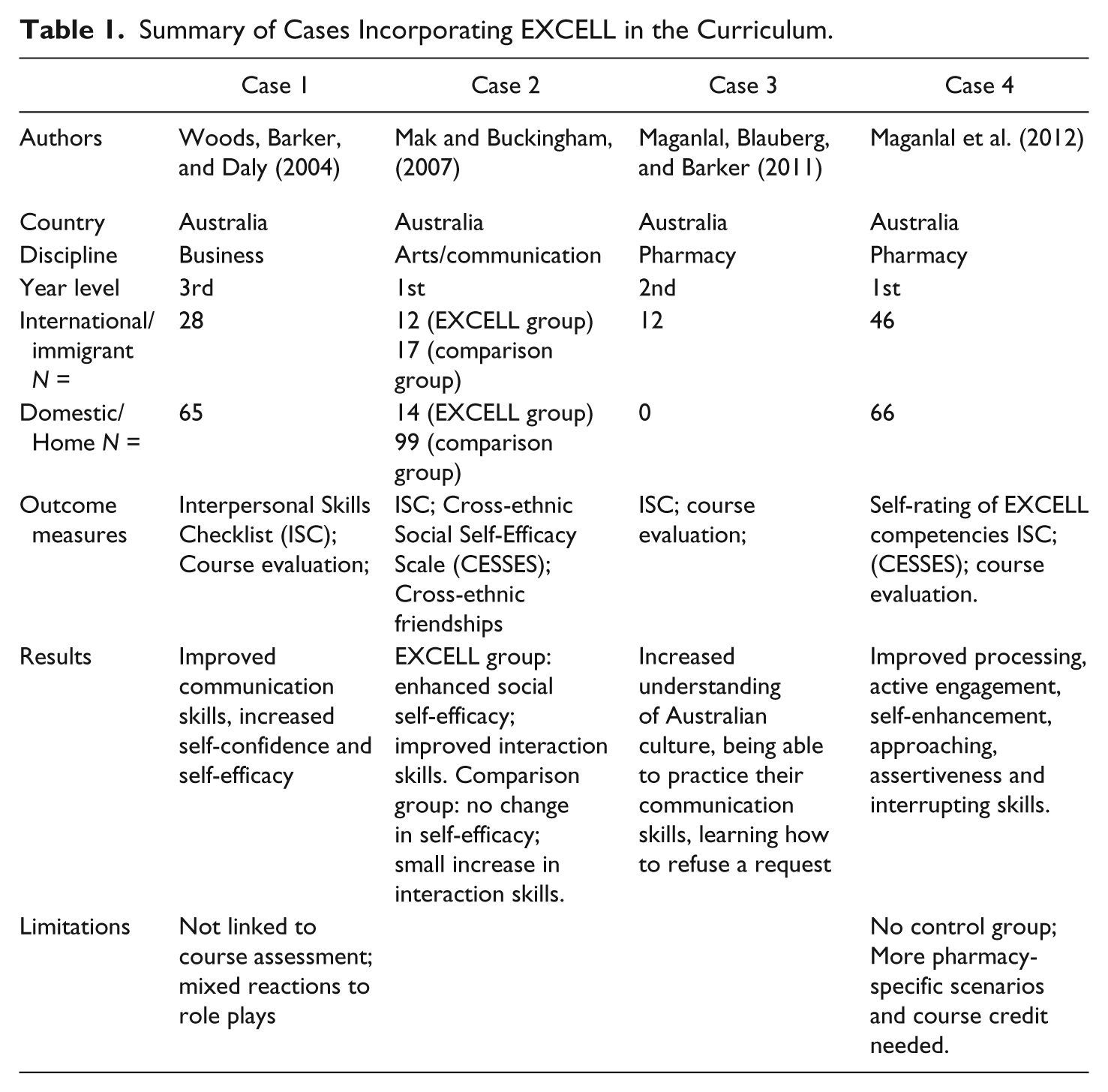
Case 1: International human resource management
Many international business courses, especially management and human resource management courses, focus on the development of analytical skills and understanding the application of theoretical concepts (Woods, Barker, & Daly, 2004; see also Lane, Maznevksi, Di Stefano, & Dietz, 2009). In contrast, EXCELL focuses on developing practical skills in intercultural communication. The objective of the teaching innovation was to assess whether integrating intercultural skills development in the analysis of international human resource management case studies would (a) improve students’ skills in identifying cross-cultural interaction problems in business situations, (b) improve students’ skills in identifying appropriate strategies to overcome problems in cross-cultural business interactions, and (c) increase students’ self-confidence and self-efficacy in cross-cultural situations.
EXCELL skills development was embedded in four, 2-hr workshops. Traditionally, students examined case studies such as one involving an expatriate manager working in an Asia-Pacific subsidiary who needs to give feedback to Head Office in New York about an employment contract. In the teaching redesign described here, instead of only a case discussion students enacted the case, taking on the role of the manager giving feedback. A pretest posttest design found that students were able to demonstrate improvements in some of the specific intercultural competences required in business as well as reporting increased self-confidence and self-efficacy in cross-cultural situations. Additionally, participants demonstrated improved identification and articulation of cross-cultural business problems and formulation of appropriate intervention strategies. Learning journals enabled students to reflect on their learning and develop action plans for how to further develop their competencies in intercultural management. Integration of the case study method with elements of EXCELL was supported, however, because students are more accustomed to courses that emphasize theories and conceptual analysis, the rationale for including a skills component within the course must be explained from the outset. Also, participation needs to be linked to course assessment, and facilitators need to be appropriately trained in the method.
Case 2: Communication course
This study used a quasi-experimental design to investigate whether adding a skills-based sociocultural training module (EXCELL) to a university course on communication would improve students’ (a) social interaction skills, (b) cross-ethnic social self-efficacy, and (c) amounts of cross-ethnic friendships (see Mak & Buckingham, 2007). A subsample (N = 26) of enrolled students (total N = 142) volunteered to complete 2-hr EXCELL workshops over a period of 6 weeks, as an additional module in their curriculum. The remaining students who studied only the knowledge-based general communication course served as a comparison group.
The study found that incorporating the EXCELL program in a group of local and international students represents an effective approach to fostering positive intergroup contact and developing self-efficacy in interacting with others. In line with Harrison’s (1992) research, combining both behavior modeling and cultural knowledge learning in cross-cultural management was more effective in facilitating changes in attitudes and behaviors, than was either method individually. The research could be enhanced through a follow-up design to explore whether improved intercultural social skills and confidence and cross-ethnic friendships are maintained over time.
Case 3: Pharmacy course for Saudi Arabian students
EXCELL was embedded in the “Introduction to Pharmacy and Practice” bridging course within the second year of the Bachelor of Clinical Pharmacy for a cohort of 12 newly arrived Saudi Arabian students (Maganlal, Blauberg, & Barker, 2011). Students examined how each of the six generic competencies was performed in their culture, compared with in Australia, and the cultural values underpinning the behaviors. Scenarios drawn from Pharmacy practice (e.g., giving feedback to a hospital pharmacist) were role-played by students.
Evidence suggests the EXCELL program helped the Saudi students improve their social interactions skills in their new cultural context. Students commented that the most useful parts of the EXCELL program were an increase in understanding of the Australian culture, being able to practice their communication skills, and learning about the competency of how to refuse a request. To achieve wider applicability for Health students across the higher education sector, vignettes of practice scenarios involving multiple health practitioners need to be developed and filmed for use in the classroom.
Case 4: First year Pharmacy course
Further to the intervention described in Case 3, EXCELL was integrated into the first seven weeks of a first-year pharmacy course to enhance intercultural competence and improve pharmacy students’ confidence and self-efficacy in the university and wider social setting (see Maganlal et al., 2012). The program aimed to teach social competencies relevant to the Australian context for all pharmacy students, both domestic and international. Pre- and postsurveys were conducted to evaluate the impact of the EXCELL course on students’ intercultural and interpersonal skills as well as students’ perceptions about the course. The course was also evaluated by the faculty who facilitated the workshops.
Postprogram tests showed that students improved in each of the six generic competencies. While international students rated the course as significantly more valuable than domestic students, the faculty found the course very useful for enhancing interactions between domestic and international students. Embedding the EXCELL in a first year Pharmacy course appears to be a promising strategy to improve students’ intercultural competence and social interaction skills. Students were reluctant to engage in homework related to skills practice because of the “not-for-credit” status of the course. Future development needs to consider more pharmacy-specific and more interpersonally challenging scenarios to fully engage domestic students.
Reflections on the Case Studies
The four case studies presented here provide a context for analyzing the strengths and limitations of embedding skills development in different disciplines. Each case demonstrated particular ways of integrating a behavioral component in courses that had traditionally focused more on development of cognitive and analytical skills. Each application resulted in enhanced self-reported intercultural communication skills and improved self-efficacy of students. There were no major differences between different disciplinary contexts in what is involved in the integration of skills development. Each application required real commitment on the part of faculty, including the capability development of workshop facilitators. The challenges experienced in each of the four cases studies included (a) ensuring that discipline-specific critical incident scenarios were used, (b) assessing students’ baseline skills levels, and (c) evaluating outcomes separately for international and domestic students. Also, it would be useful to consistently assess any change in intercultural attitudes and cross-ethnic friendships and the use of comparison groups, as in the Mak and Buckingham (2007) study.
Taken together, the curricular innovations suggest there is merit in embedding the EXCELL framework to develop students’ generic social competencies. It is argued that intercultural competencies (e.g., expressing disagreement to a peer who is from a culturally and linguistically different background) require more refined skills, than does the execution of generic social competencies (e.g., expressing disagreement to a peer from the same culture), because of the complexity of cultural differences. If intercultural competencies constitute a graduate attribute, then faculty need to help students to achieve mastery of generic social competencies as a foundation to building intercultural competencies.
To date, much of the emphasis in IoC has been on the inclusion of international and global dimensions in course content and assessment (Rizvi & Lingard, 2010; Shiel, 2007). IoC must also address behavioral and affective development of students as emerging global graduates. The need to ground intercultural competency development in the substrata of specific disciplines is the primary pathway to engage faculty, clinical preceptors, industry practitioners, and most importantly, students of the discipline.
Critical Incident Scenarios Generated From Faculty and Industry Professionals
Each of the above case studies highlights the need to turn to disciplinary experts to gather discipline-specific critical incident scenarios that can be used in the classroom. These consultations comprised the foundational study within the “Internationalisation at Home” project funded by the Australian Government Office for Learning and Teaching. Stakeholder groups (Business, Nursing, and Pharmacy faculty members and industry professionals) were consulted to assess the need for sociocultural competence development in discipline-specific classes and workplaces. Each stakeholder group was asked to identify challenging intercultural social scenarios (or critical incident scenarios) for use in the design of curriculum resources for professional development workshops for Business and Health faculty at two Australian universities. The data reported here draw on six discipline-specific focus groups held with Business, Nursing, and Pharmacy academics and industry professionals/clinical facilitators in Brisbane and the Gold Coast, Queensland. Faculty members included 10 from Business, 7 from Nursing, and 6 from Pharmacy. Industry consultations included 10 Business people, 19 registered nurses, four nurse clinicians, and six community pharmacists. An audio recording device was used by facilitators to capture the focus group discussion, which was subsequently professionally transcribed.
Analysis of stakeholders’ responses has shown recurrent critical incident scenarios in intercultural social interactions in (a) the classroom and (b) the workplace, which can be addressed by improved cultural knowledge and generic social competencies that underpin effective intercultural communication.
Common Critical Incident Social Scenarios in Business, Nursing, and Pharmacy Classrooms
Table 2 lists some of the most common critical incident social scenarios in the classroom identified by stakeholders. Each scenario has been linked to one of the six EXCELL key competencies. As discussed earlier, more than one competency may be involved in any interpersonal interaction. Interestingly, most of the scenarios reported by stakeholders were not discipline-specific, nor were they necessarily highly intercultural in nature. For example, take the example given by Business and Health faculty about students’ difficulties in seeking help or information. From time to time, domestic (home) and international students need to seek an extension from a faculty member to complete an assessment piece (e.g., a delay due to ill health). The interaction may prove more challenging for shy students, those unfamiliar with the norms of interacting with university faculty, and particularly some international students who are not experienced communicators in the new cultural context.
Common Critical Incident Social Scenarios in Business, Nursing, and Pharmacy Classrooms.
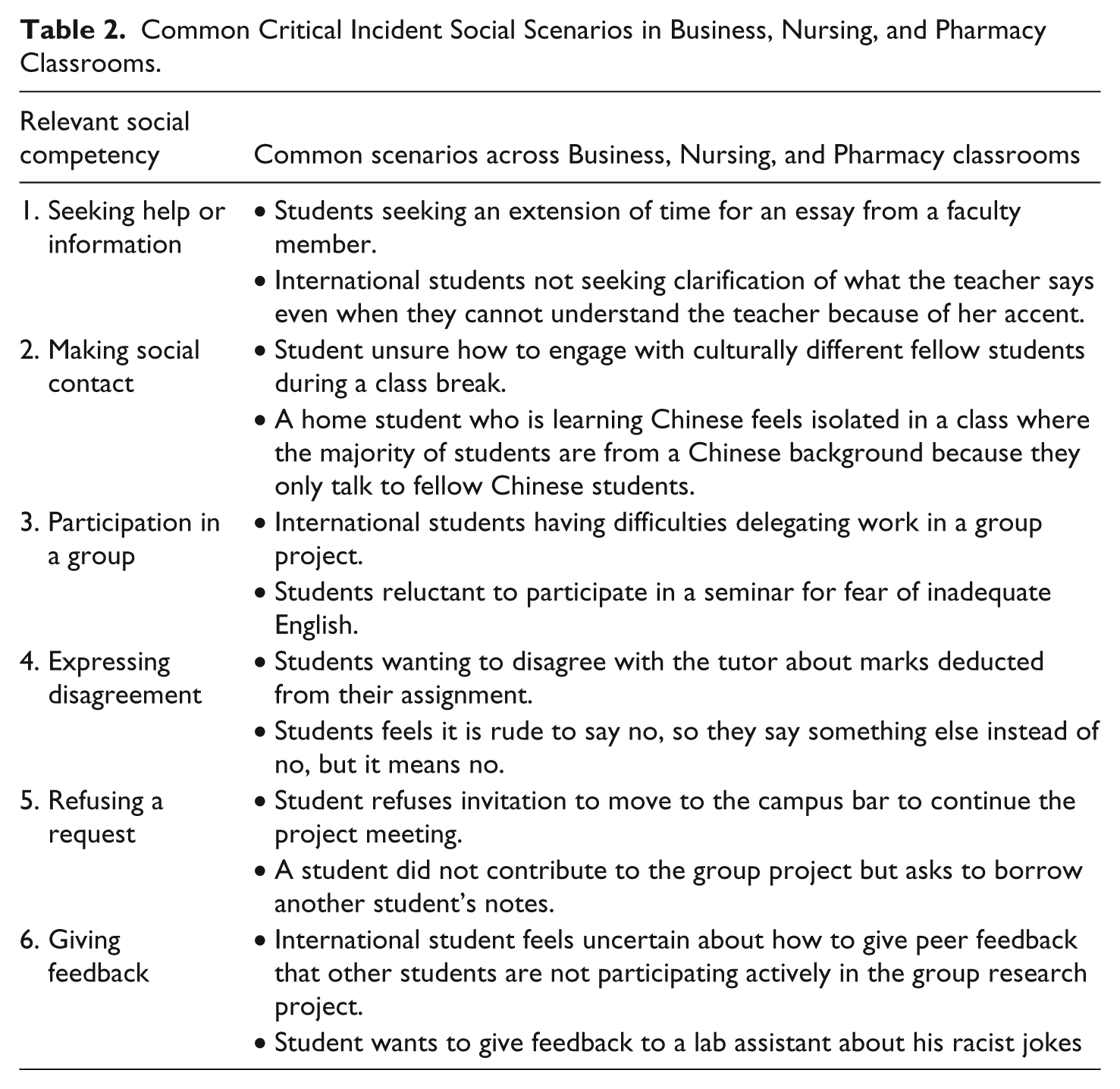
The intercultural scenarios offered by faculty stakeholders highlight several generic issues in the classroom. Interestingly, irrespective of discipline, there was a high level of similarity in the types of challenging classroom scenarios identified. Multicultural group work, in particular, was a frequently occurring situation where intercultural communication competencies were tested in the classroom. Productive group work not only requires what EXCELL defines as access competencies (i.e., active participation, making social contact, and seeking help or information) but group projects also provide a context in which students frequently need to express disagreement, refuse a request, and give feedback to other group members (i.e., negotiation competencies). In particular, faculty noted issues around students not being able to delegate work in a group project; not being able to chat with other group members; and refusing a request by a group member to borrow another student’s notes.
Faculty from the three disciplines also noted three scenarios in relation to “giving feedback” and “refusing a request” that they found challenging. These included refusing “thank you” gifts from students so as to uphold their institution’s policy in this area as well as their uneasiness about the motivation behind the gift-giving. Interestingly, faculty from each discipline also identified the challenges in giving feedback to students who insisted their marks be increased or to students about to become more actively engaged in class activities.
Common Critical Incident Social Scenarios in Business, Nursing, and Pharmacy practice
Table 3 presents examples of common critical incident reported by practitioners from diverse disciplines. The scenarios refer to practice in business organizations, hospitals, health care settings, and pharmacies mapped against the six competencies.
Common Critical Incident Social Scenarios in Business, Nursing, and Pharamcy Practice.

The highly multicultural nature of Australian society is a theme that underpins the scenarios identified by industry stakeholders. Similar to the scenarios described in the classroom, discipline representatives commented that cultural diversity refers not just to international students but also to students, staff, patients, clients, and community members from CALD backgrounds. Related to multiculturalism, several scenarios focused particularly on religious practices. The competency of giving feedback was required when an intern had to inform her supervisor about not being able to attend a workgroup lunch owing to her religious practices (i.e., fasting during Ramadan). A related scenario involved a student who did not drink alcohol or eat pork for religious reasons and who had been advised that alcohol and pork dishes would be served at a staff social function.
Many of the other scenarios common across the disciplines involved lack of confidence and lack of assertiveness in workplace interactions. Sometimes these situations were exacerbated by cultural differences, but gender and power differences between student interns and senior staff members/supervisors/clinical preceptors were evident. Clearly, the interplay between adjusting to the culture of the workplace, societal cultural factors, and power differentials were intertwined in many scenarios, depending on the characteristics of the interactants. For example, stakeholders reported numerous incidents of interns being reluctant to seek help from supervisors about difficulties encountered on a project or task, or challenging the supervisor about an issue (e.g., providing feedback to a clinical preceptor that her expectations about the time frame for completing an assigned task is unrealistic). These types of scenarios were explained by stakeholders as the problem of “losing face.” Other examples included expressing disagreement with a supervisor about a course of action and refusing a request to work overtime because saying “no” may indicate uncooperativeness on the part of the intern or staff member. Analysis of the common scenarios across stakeholders indicated the robustness of the six generic social competencies underpinning them. In the next section, we examine whether the framework continues to hold when discipline-specific critical incidents are examined.
Discipline-Specific Critical Incident Social Scenarios in Professional Practice
Compared with classroom scenarios, which did not seem to differ significantly between disciplines, many discipline-specific critical incident scenarios were discussed by stakeholders. Table 4 presents six scenarios from stakeholder practice, mapped against the six general social competencies.
Discipline-Specific Critical Incident Social Scenarios in Professional Practice.

Analysis of the critical incident social scenarios underlined the importance of skilled communication in health care settings, particularly where cultural differences were present. As discussed earlier, in a multicultural society intercultural communication challenges occur frequently between health professionals and patients/clients, between supervisors and students, and between workgroup peers. While the Business practice examples underlined important issues (such as the need to provide worksite privacy to allow a Muslim employee to pray in private without disrupting the workgroup), asking for help or giving feedback seemed to be particularly crucial in Health settings where patients’ health and safety were at stake. Take, for example, the situation of the Vietnamese intern who did not speak to patients unless requested, or the pharmacist who had to speak indirectly about a female patient’s health needs through her husband acting as interpreter. Scenarios such as these highlight the importance of generic social competencies that underpin intercultural communication. Furthermore, the scenarios point to the crucial role played by industry supervisors and clinical preceptors in providing on-the-job skills development and constructive feedback to interns. Industry stakeholders shared many challenges they experience as they try to manage their own heavy workloads, while trying to provide the appropriate level of guidance to “professionals-in-training.” Their need for professional development resources and support was evident as they discussed how intercultural factors made practice more complex, regardless of whether this stemmed from the needs of clients/patients, colleagues, students, or the interplay between them. The workplace is indeed where “the rubber meets the road.” A test of an effective internationalized curriculum, therefore, is whether graduates can demonstrate the capacities to interact effectively with clients, peers, and supervisors from CALD backgrounds.
Each critical incident provided by stakeholders constitutes rich case material for students preparing for internships. It gives them a preview of the types of incidents they may encounter in pharmacies, hospital wards, and business organizations. Similarly, the cases can be used in professional development workshops for faculty and practitioners who supervise students on their internships as well as provide resources for course assessment. If IoC is to be grounded in practice, then it is most instructive to use stakeholder-generated intercultural critical incidents as curricula resources. In particular, the scenarios illustrate how and why intercultural knowledge, awareness, and skills are needed by professionals. Taken a step further, the scenarios can provide the basis for employing EXCELL techniques such as mapping the stages of interactions and the values underpinning each stage. For example, Pharmacy students could practice refusing a client’s request to purchase a banned substance. If needed, the student can be coached to ensure their behavior would be perceived as culturally and professionally appropriate by colleagues and supervisors.
Overview
The conundrum articulated by Ramburuth and Welch (2005) among other scholars in IoC is the lack of clear consensus on how to “link the global classroom to the global workplace” (p. 6). Practitioners, disciplinary scholars, and educators wrestle this conundrum in their efforts to determine how to embed global perspectives in the curriculum as well as how best to prepare and support students to be interculturally skilled in their group work assignments in class (Woods, Barker, & Hibbins, 2011) and their industry internships in multicultural settings (Dunne, 2011).
This article has examined several published studies in Business and Health disciplines that have used aspects of the EXCELL Intercultural Skills Program—a behavioral competence development approach grounded in a participatory strategy that builds intercultural inclusion and awareness of self and others. These studies have addressed the challenge of operationalizing and embedding intercultural awareness and skills development. While limitations are identified, the review suggests some merit in adapting the active participation aspects of the program to facilitate students’ cognitive, affective, and behavioral development. Comparative analyses of the application of EXCELL in disciplines as diverse as Business and Pharmacy indicate that its relevance is not confined to particular disciplinary or cultural contexts.
In sum, the case studies and stakeholder-generated scenarios provide a rich resource that contributes to the development of “new and effective approaches and interventions to ensure campus and classroom culture motivates and rewards interaction across cultures for all students” (Leask & Carroll, 2011, p. 657). We argue this resource can also be adapted to ensure disciplinary relevance not only in the campus and classroom but also in industry and professional settings. The challenge for educators is to pitch the intercultural learning activities appropriately to enable all students (whether home or international) to be actively engaged and stimulated.
Preliminary analyses of the stakeholder study indicate the value of seeking the perspectives of practitioners and faculty about the need for intercultural competencies. Stakeholders identified multiple practice-based examples where intercultural awareness and skills were needed in six generic social competencies. It seems that there are recurrent critical incident scenarios in intercultural social interactions that can largely be addressed by improved cultural knowledge and generic social competencies that underpin effective intercultural communication. As part of the “Internationalisation at Home” project funded by the Office of Learning and Teaching, the same process will be repeated by consulting groups of students from different disciplines. All stakeholder examples will be translated into curriculum resources that can be adapted for Business, Health, and other disciplines (see https://sites.google.com/site/internationalisationathome). Promoting the development of intercultural competence of Business and Health students will enable them to move with confidence from the classroom to the boardroom and ward.
Footnotes
Acknowledgements
Support for this publication has been provided by the Australian Government Office for Learning and Teaching (ALTC PP10-1810). The views expressed in this publication do not necessarily reflect the views of the Australian Government Office for Learning and Teaching. The authors would like to acknowledge the contributions from the Internationalisation at Home Project Managers Sylvia Alston (Canberra) and Ruth Hills and Agata Mouasher (Griffith University), other team members and project associates—Peter Woods, Saras Henderson, Nick Buys, Jasmina Fezjic, and Satish Maganlal at Griffith University, and Anne Daly, James Neil, and Laurie Grealish at the University of Canberra.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research reported was funded by the Australian Government Office for Learning and Teaching.