
Abstract
There have been numerous iterations of naming convention specified for myalgic encephalomyelitis (ME) and chronic fatigue syndrome (CFS). As health care turns to “big data” analytics to gain insights, the Google Trends database was mined to ascertain worldwide trends of public interest in several ME- and CFS-related search categories between 2004 and 2019. Time series analysis revealed that though “chronic fatigue syndrome” remains the predominant search category in the ME and CFS field, the interest index declined at a rate of 2.77 per month during the 15-year study period. In the same time period, the interest index in “ME/CFS Hybrid” terms increased at a rate of 3.20 per month. Potential causal mechanisms for these trends and implications for patient sentiment analysis are discussed.
The illness known as myalgic encephalomyelitis (ME) and chronic fatigue syndrome (CFS) has been recognized as a symptomatically complex, debilitating illness that affects up to 24 million people worldwide (Johnston et al., 2013). Myalgic encephalomyelitis and CFS is characterized by impairing levels of fatigue that lasts at least 6 months, and other hallmark symptoms include postexertional malaise, sleep difficulties, and either cognitive impairment or orthostatic intolerance (Institute of Medicine [IOM], 2015). Unfortunately, there still exists disagreement regarding how to define the illness as well as the illness name. For example, in 1934, outbreaks of fatigue-related illnesses called “atypical poliomyelitis” occurred in Los Angeles (Meals et al., 1935). And later, outbreaks in London in 1955 were deemed “encephalomyelitis” (Crowley et al., 1957), and then “chronic mononucleosis-like syndrome” in Nevada in 1984 (Barnes, 1986). National attention in the United States was garnered following the outbreak in Nevada (Wessely, 1994), and in 1988, the Centers for Disease Control and Prevention (CDC) named the unexplained illness CFS (Holmes et al., 1988). Around the same time, clinicians in England were referring to this illness as ME (Ramsay, 1988). In 2003, the Canadian clinical case (CCC) definition was developed for use by clinicians for treatment of the illness, marking the formal introduction of the hybrid illness name, ME/CFS (Carruthers et al., 2003). And most recently in 2015, the IOM (2015) recommended that the illness should be named systemic exertion intolerance disease (SEID).
Following the naming of CFS by the CDC, many patients felt the name trivialized the seriousness of their illness and compounded the stigma they already faced in dealings with skeptical medical professionals (Jason et al., 2004). These decisions have the power to affect the course of treatment of CFS, potentially creating serious consequences for patients (Blease & Geraghty, 2018). For example, when medical trainees were given case descriptions of patients with prototypic symptoms of CFS, 41% of trainees believed patients would recover when referring to the illness as CFS compared with 16% when referring to the illness as ME. The trainees were also more likely to attribute the illness to medical causes when referring to the illness as ME (Jason et al., 2002). These results indicate a stereotyping effect among medical practitioners when the name of an illness is characterized by a single symptom (CFS), rather than a name that uses medical terminology (ME; Jason et al., 2002). Importantly, the manner in which an illness is labeled may have direct impact on the treatment and outcomes of patients (Wojcik et al., 2011). These perceptions may have serious implications; for example, among nondepressed individuals with ME/CFS, suicidal ideation can partly be attributed to patients’ feelings of their illness not being taken seriously by family members and medical professionals (Devendorf et al., 2020). In one study, individuals with ME and CFS who used a more trivialized label for their illness (“chronic fatigue syndrome”) were 2.81 times more likely to have suicide as their cause of death than those who identified with a more nontrivial label (e.g., “myalgic encephalomyelitis,” “ME/CFS”; Johnson et al., 2022).
In 2000, the U.S. Department of Health and Human Services’ CFS Coordinating Committee initiated a subcommittee called the Name Change Workgroup (NCW). The NCW, comprising scientists, clinicians, and patient representatives, was tasked with making ME and CFS name change recommendations to the Secretary of Health and Human Services (Jason, 2007). Based on early NCW meetings, it was clear the scientific community supported the current name of chronic fatigue syndrome, while the patient community was more in favor of the medically sounding name myalgic encephalomyelitis. As discussions continued, constituents were able to reach general consensus on key points of recommendation, specifically, the use of an “umbrella” term to use for the illness name, and the use of subtypes to reflect patient preferences and symptomatic heterogeneity (Jason, 2007). Although the NCW was ultimately dissolved and their recommendations not adopted by the federal government, their key points on naming convention were visible with the inception of the ME/CFS CCC definition (Carruthers et al., 2003). The CCC definition was a landmark in the history of ME and CFS naming convention, representing a compromise between the scientific and patient communities. Hybrid terms such as ME/CFS retain the naming component which describes a common symptom and is also well known in scientific and public spheres (CFS), while also including a name that respects the history of the illness and does not trivialize the medical nature of the patient experience (ME).
Similar to CFS, the IOM (2015) has more recently proposed a name change to SEID focused on a singular, common symptom. Following the SEID name change recommendation, ME and CFS online polls became forums for patients to voice their opinions (Jason & Johnson, 2020). In one survey of 1,004 patients, 62% indicated that the SEID name was “pretty bad or very bad” (Petrison, 2015). In an international sample of 1,045 participants, 65% of the U.S. sample and 68% of the international sample liked or definitely liked the term ME, compared with 16% to 17% who liked or definitely liked SEID (Jason, Nicholson, & Sunnquist, 2016). Other studies have further demonstrated that renaming stigmatized conditions to encompass a wider spectrum of symptoms can decrease negative stereotyping for some patients (Koike et al., 2015).
Of particular interest for this research is how the public has used these different terms to refer to ME and CFS. Infodemiology, described as the monitoring and analysis of internet data aimed to inform public health and policy (Eysenbach, 2009), is one way of investigating usage patterns of ME and CFS naming conventions. On a large scale, Google Trends (GT) uses big data analytics to ascertain public interest over time by aggregating search queries worldwide in a publically accessible, downloadable database (Google, 2020b). Analytic tools such as GT have the advantage of gathering unsolicited, anonymous “subject” data in real time, providing aggregate data visualization, and using trends over time for approximating patient behavior and disease risk surveillance (McCormick et al., 2017). In a review of GT health-related studies by Mavragani et al. (2018), GT has been shown to be valid, valuable, and beneficial for forecasting. In addition, if the searched-for terms are meticulously chosen, GT data can accurately measure public interest (Scharkow & Vogelgesang, 2011).
To this point, GT still represents a relatively novel methodology to measure opinions, behavior, and trends in health care research (Mavragani et al., 2018; Nuti et al., 2014). These types of internet data have the power to complement and extend extant data in health care research (Barrett-Connor et al., 2011). The current exploratory study used mining and analysis of GT data as an evidentiary opportunity to examine trends of ME and CFS naming conventions over time. Using these methodologies, we hypothesized that patient sentiment could potentially facilitate increases in the worldwide use of more clinically sounding (i.e., “myalgic encephalomyelitis”) and inclusive (i.e., “ME/CFS”) naming conventions for ME and CFS. Likewise, we expected to observe decreases in usage of naming conventions for ME and CFS which could trivialize the illness (i.e., “chronic fatigue syndrome” and “systemic exertion intolerance disease”).
Method
Data
Data acquired from GT are an unbiased sample of the trillions of yearly search queries Google maintains, and are anonymous, categorized, and aggregated. Data may be filtered in “non-real time,” providing samples which include time points from 2004 to the most recent 36 hr (Rogers, 2016). Individual queries can include multiple search terms using an “OR” operator (+). Multiple queries may also be compared relative to each other in the GT interface.
Downloadable GT output provides time points (days, months, or years) and a corresponding search volume index (SVI) value. The SVI values are normalized search data such that comparisons between terms are easier. The normalizing process, specified in the query by geography and time period, involves dividing the number of searches for the term(s) of interest by the total number of all queries in that same space-time. The resulting values are then scaled from 0 to 100, such that 100 represents the greatest interest. Google Trends filters out searches made by very few people, duplicate searches (repeated searches from the same user over a short span of time), and various special characters (Google, 2020a).
Procedure
Four main ME and CFS categories of interest and their respective search terms, separated by the “OR” operator, were specified as follows: “ME/CFS Hybrid” category (ME/CFS + ME-CFS + CFS/ME + CFS-ME + MECFS + “ME and CFS” + “CFS and ME”); “chronic fatigue syndrome” category (chronic fatigue syndrome); “myalgic encephalomyelitis” category (myalgic encephalomyelitis + Myalgic Encephalomyelopathy); and “systemic exertion intolerance disease” category (systemic exertion intolerance disease). For the latter three search categories, abbreviated illness naming conventions were strategically not utilized to avoid counting false positives (e.g., CFS was not a search term used in the “chronic fatigue syndrome” category). Similarly, quotation marks were used to ensure specificity in the terms “ME and CFS” and “CFS and ME.” Without the use of quotation marks for these terms, SVI would have inclusively represented searches for the individual terms ME and CFS rather than the desired result of estimating their usage together. Search terms in Google are case insensitive; for example, a search for the term ME/CFS would yield the same SVI values as a search for the term me/cfs. At the time this data mining algorithm was utilized, terms joined by the “OR” operator were limited to seven.
Worldwide data were mined during a 15-year period (August 2004–July 2019), encompassing 180 monthly time points. For the “systemic exertion intolerance disease” category, all analyses were conducted with a starting point of February 2015, corresponding with the release of the IOM report, and the first instance of “systemic exertion intolerance disease” being identified by GT.
Analysis
Temporal trends of ME and CFS naming conventions were ascertained using a four-step process. First, SVI was visually examined during the study period in an uncollated format. Uncollated depictions disaggregated each of the four search categories and were useful in exploring individual category trends.
Second, SVI correlations with time provided additional exploratory information and were calculated for each naming category. Spearman’s rho correlations and Pearson’s correlations were both examined in consideration of nonparametric and parametric distributions, respectively.
Third, autoregressive integrated moving average (ARIMA) models were estimated. Autoregressive integrated moving average models are specified using three terms: p, the autoregressive component which describes the degree to which a current data point is dependent on previous observations (e.g., if p = 0, there is no autocorrelation; if p = 1, the value is affected by the previous value, and so on); d, the integrated component which describes a trend in the data and what type of adjustment is required to achieve a stationary mean (e.g., if d = 0, the mean is stationary; if d = 1, there is a linear trend; if d = 2, there is a quadratic trend, and so on); and q, the moving average component, which describes the persistence of a “random shock” (error) from one data point to the next (e.g., if q = 0, there are no “random shocks” in the data; if q = 1, an observation depends on one preceding “random shock,” and so on). Autoregressive integrated moving average models may also consider seasonality, in which elements of periodicity may be present. Such phenomenon may be observed in the domains of finances or infectious illness research where forecasting is the central priority. In this study, where establishing trend was the focus, seasonality was not considered. All time series analyses were conducted using IBM SPSS Statistics (IBM Corp., 2017) Time Series Modeler (Expert Modeler function), and best-fitting models were those with the lowest Bayesian information criteria (BIC) and highest explained variance (R2).
Finally, based on the trend findings established from the ARIMA models, regression models were fit, and parameter estimates were calculated and interpreted.
Results
When considering disaggregated trends since 2004, the time series plots indicate increases in the searching of the “ME/CFS Hybrid” category (see Figure 1) and decreases in the searching of the “chronic fatigue syndrome” category (see Figure 2). More unstable trends for the “myalgic encephalomyelitis” category (see Figure 3) and the “systemic exertion intolerance disease” category (see Figure 4) were observed, and their comparatively smaller nonparametric and parametric correlation coefficients support these visual findings (see Table 1).
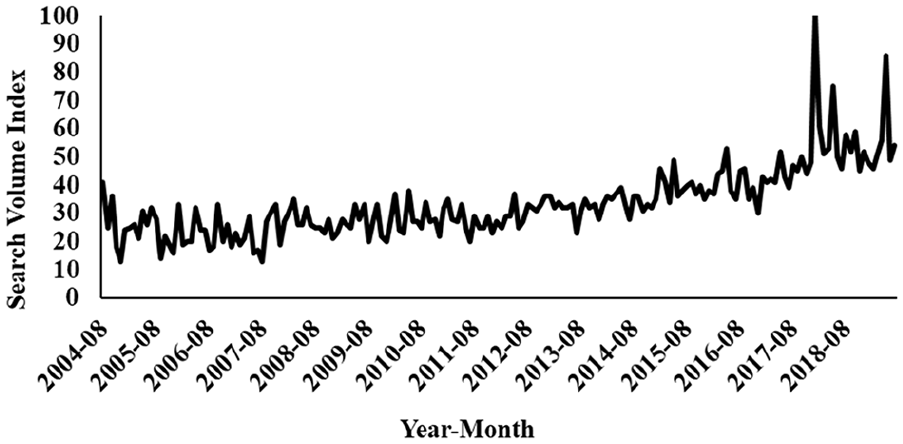
Worldwide Interest in “ME/CFS Hybrids,” 2004 to 2019.
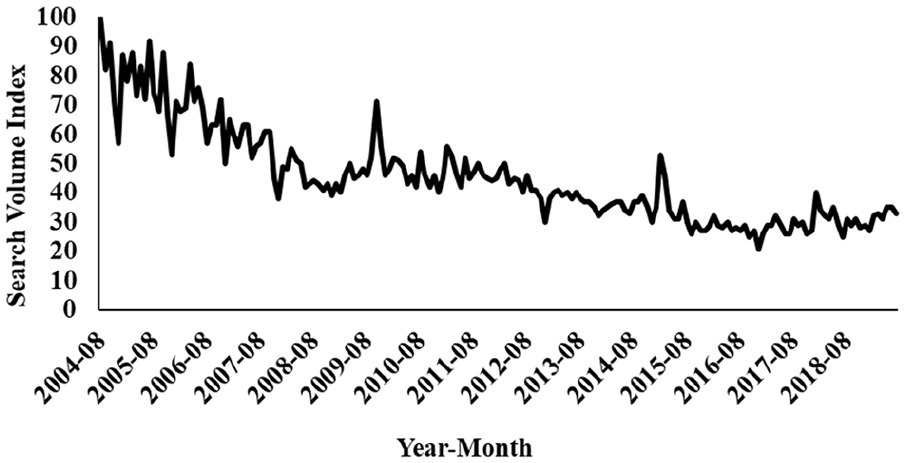
Worldwide Interest in “chronic fatigue syndrome,” 2004 to 2019.
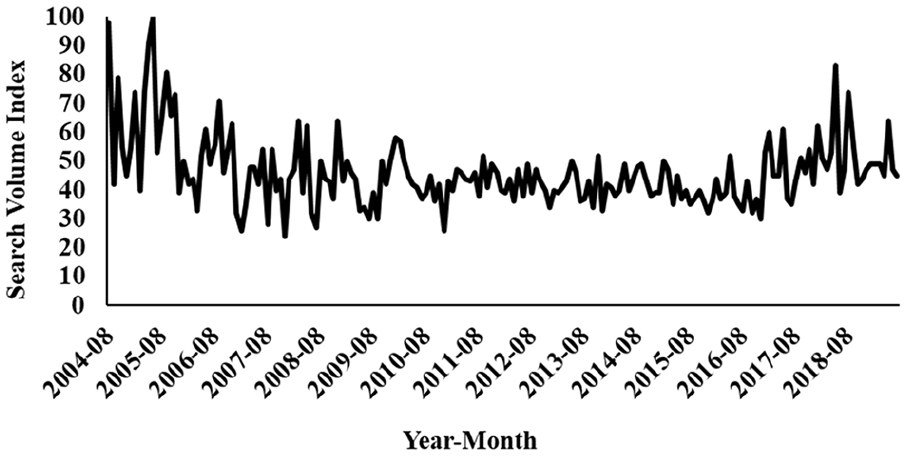
Worldwide Interest in “myalgic encephalomyelitis,” 2004 to 2019.
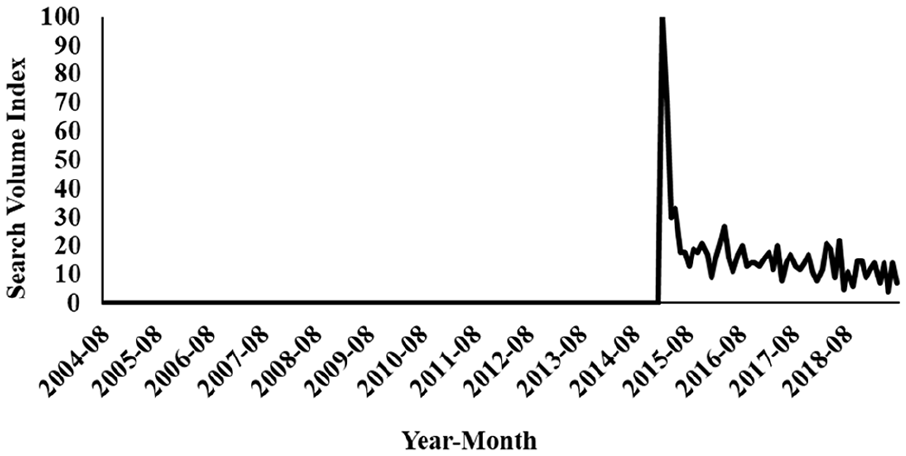
Worldwide Interest in “systemic exertion intolerance disease,” 2004 to 2019.
Summary of Trend Analysis for ME, CFS, and SEID Terms Usage.
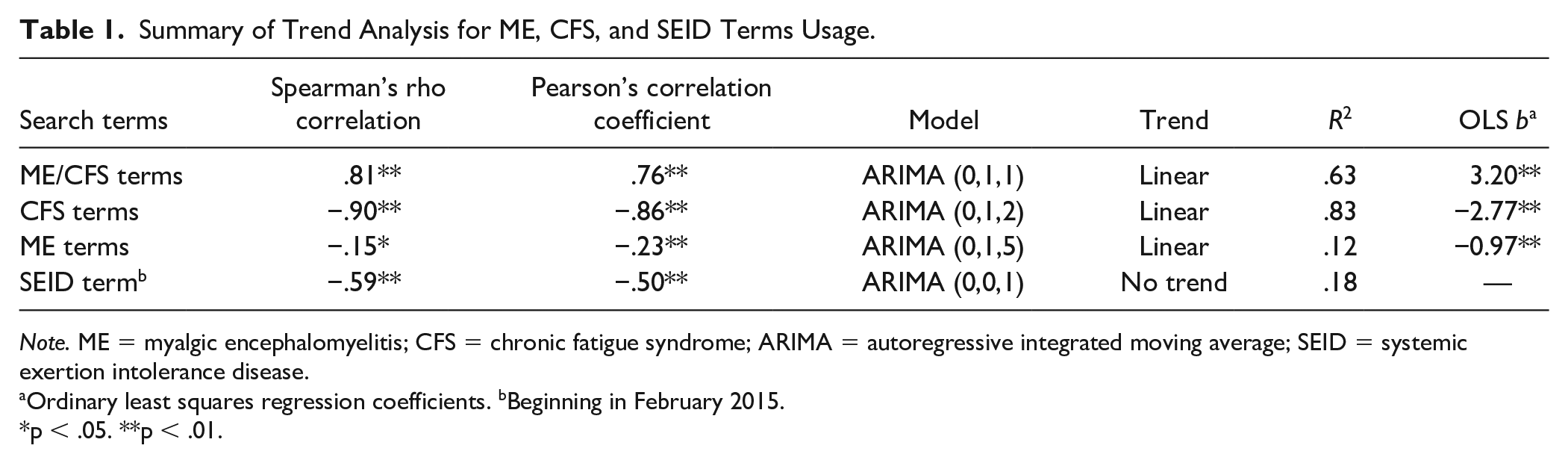
Note. ME = myalgic encephalomyelitis; CFS = chronic fatigue syndrome; ARIMA = autoregressive integrated moving average; SEID = systemic exertion intolerance disease.
Ordinary least squares regression coefficients. bBeginning in February 2015.
p < .05. **p < .01.
Autoregressive integrated moving average model fitting indicated the presence of a positive linear trend for the “ME/CFS Hybrid” category and a negative linear trend for the “chronic fatigue syndrome” category and “myalgic encephalomyelitis” category. Using ordinary least squares regression, these trend slopes were all found to be statistically significant with a Type I error rate of α = .05. No trend was observed for the “systemic exertion intolerance disease” category, perhaps unsurprisingly given the comparatively smaller number of available data points (N = 54). Both the “myalgic encephalomyelitis” category and the “systemic exertion intolerance disease” category exhibited poor model fits, an indication of high unexplained variance. This erratic distribution effect is also apparent in the moving average ARIMA component of “myalgic encephalomyelitis” category (q = 5).
Discussion
Although “chronic fatigue syndrome” remains the predominant nomenclature in the ME and CFS field, the findings of this study suggest the worldwide interest, as measured by SVI, has declined at a rate of 2.77 per month in a 15-year span. In that same stretch of time, the SVI for “ME/CFS Hybrid” terms has exhibited a nearly equal but opposite effect, increasing at a rate of 3.20 per month. The worldwide interest in the “systemic exertion intolerance disease” category was never higher than it was at the time of the IOM report release in 2015. Although no statistically significant linear trend was observed through ARIMA analysis, visual exploration of this category suggests its interest was generally decreasing (see Figure 4). Compared with the other three categories, worldwide interest in the “myalgic encephalomyelitis” category exhibited the most month-to-month variation (see Figure 3), suggesting the potential for instability of the trend estimate that was observed (see Table 1). The reduction of “chronic fatigue syndrome” interest could suggest a simple decrease of interest in the illness over time. However, when considered in conjunction with the increasing interest in “ME/CFS Hybrid” terms, these findings collectively suggest changes in the use of the name.
Social contagion theory guides our interpretation of the present findings. Social contagion has been described as a concept that “applies to human thoughts and ideas, which can be transmitted from person to person via social interaction” (Wang & Wood, 2011, p. 5442). In the internet age, these social interactions are increasingly taking place in forums such as social media websites and message boards, paving the way for novel methodologies. It can be challenging to make inferences concerning the “actor” who is driving contagion trends; in the context of ME and CFS, the patient community, researchers, and governmental entities all play substantial roles in shaping policy concerning the illness. One by-product of competing interests of key stakeholders has been the heterogeneity of the naming conventions visible in the ME and CFS field (Jason, Sunnquist, et al., 2016; Nicholson et al., 2016; Siegel et al., 2018).
We believe that increased usage of the name ME/CFS represents a shift toward the nontrivialization of ME and CFS. For the patient community, trivialization of the illness label has been associated with increased sentiments of stigmatization (Jason et al., 2004), suicidal ideation among nondepressed individuals (Devendorf et al., 2020), and suicide completion (Johnson et al., 2022). In addition, for medical practitioners, trivialization of naming conventions for ME and CFS can have drastic effects on perception of illness seriousness (Jason et al., 2002), which can in turn directly affect the treatment and outcomes of patients (Wojcik et al., 2011).
For medical researchers, consensus on naming convention for ME and CFS could aid in the collection of uniform patient samples, providing more validation in epidemiologic studies and facilitating examination of potential biomarkers (Jason & Johnson, 2020). This is of particular interest and urgency in the ME and CFS field, where patient advocates find themselves in opposition with mental health associations who propose psychiatric etiologies for patients’ somatic experiences (e.g., major depressive disorder, somatic symptom disorder), despite empirical evidence supporting the contrary (Hawk et al., 2007). Scientific discovery in these fundamental areas of disease research could potentially increase funding for ME and CFS research, where the illness has been found to be more underfunded with respect to disease burden than any other disease in the United States (Mirin et al., 2020).
It should be noted that despite increased worldwide popularity in usage, some have been critical of the name ME/CFS, as activists have indicated that it can refer to what are the two separate illnesses. For example, Twisk (2015) maintains that ME and CFS are specified by two distinct case definitions, the Myalgic Encephalomyelitis International Consensus Criteria (ME-ICC; Carruthers et al., 2011) and the Fukuda et al. (1994) CFS criteria, respectively. For Twisk, using the name ME/CFS has an unfortunate consequence of combining two separate illnesses. For example, Jason, Sunnquist, et al. (2016) found that those that met the more broad Fukuda et al. (1994) CFS case definition criteria had less impairment and symptom severity than those that met the ME criteria as operationalized by the ME-ICC case definition (Carruthers et al., 2011). Therefore, some have suggested that the term ME/CFS could ultimately be used to refer to what had been known as CFS, whereas ME could be reserved for those with more severe disability and symptoms (Jason & Johnson, 2020).
What are the implications of this research for policy makers? Following the release of the IOM (2015) report, Jason and Johnson (2020) put forth a series of recommendations which could inform policy and help address controversies surrounding naming conventions for ME and CFS. First and foremost, they suggest that the vetting process concerning naming decisions for ME and CFS involves essential gatekeepers (including patients, researchers, medical professionals, and governmental entities) at all critical decision-making junctures. Next, a series of working papers could be drafted by appointed committee members to address key issues in the field, including naming convention for the illness. With these papers as a foundation, a conference to assemble the various working groups could adopt a consensus name for ME and CFS (Jason & Johnson, 2020). As a possible outcome of these discussions, the label “myalgic encephalomyelitis,” which tends to be supported by most patients (Jason, Nicholson, & Sunnquist, 2016), could be used to represent a homogenous subset of patients who experience higher levels of functional impairment and meet research case definitions. Another subset of patients, those who meet the IOM’s (2015) clinical criteria, could be represented by the name “ME/CFS.” Finally, those who do not meet either of the aforementioned classifications could be categorized as having chronic fatigue. This strategy could provide differentiation between those patients who experience debilitating symptoms (e.g., postexertional malaise) and those who experience fatigue alone (Jason & Johnson, 2020).
Limitations
This study was not without limitations. We believe the search term strategy employed using GT to be comprehensive in representing the major current naming conventions in the ME and CFS field. However, we acknowledge that over the last several decades, there have been numerous iterations for the illness not encompassed in our search methodology (e.g., “atypical poliomyelitis,” “encephalomyelitis,” “chronic mononucleosis-like syndrome”). Although such alternate naming conventions are somewhat dated, we did not examine their prevalence across different geographies, which is an avenue for future inquiry. In addition, because GT uses only a sample of Google searches conducted, smaller countries may be subject to a high degree of sampling variation. However, because the aim of this work was to investigate ME and CFS naming conventions on a worldwide scale, we are confident that this small region sampling error would not have altered the trends reported herein.
Conclusion
Based on GT internet search data, “chronic fatigue syndrome” continues to be the most commonly used term for ME and CFS, though its worldwide usage has decreased over time. Simultaneously, usage of “ME/CFS Hybrid” terms has been on the rise, potentially attributed to the patient community’s stance for the nuances of the illness to be recognized. Regardless of the reasons for increases of interest in “ME/CFS Hybrid” terms, it appears that governmental attempts to steer the name convention issue have not been successful, at least in their most recent attempt. At the current time, the IOM’s “systemic exertion intolerance disease” has yet to gain momentum as a preferred term for ME and CFS, as evidenced by the findings of this study.
The necessary speculation concerning the drivers behind SVI trends may be considered a natural outgrowth of time series analyses. That is, these analyses provide a concise snapshot into what is happening, but alternate tools may be required to gain greater insights into how and why a phenomenon is happening. In recent years, sentiment analysis has gained traction in health care research as a valuable tool in the assessment of patient experiences. As the public becomes increasingly open to engaging with their health care on the internet, patient rating and feedback sites (e.g., RateMDs), micrologs (e.g., Twitter), and social networking sites (e.g., Facebook) are rich sources of patient sentiment which can be “scraped” and analyzed for content (Greaves et al., 2013). In addition, as computing power continues to increase, the information in these data can be processed using subjective text analysis facilitated by machine learning techniques (Khan & Khalid, 2016; Surya Prabha & Sarojini, 2018). To date, sentiment analysis has been used to ascertain patient opinions concerning hospital quality, public health, and illness treatments (Gohil et al., 2018). In the ME and CFS field, patients have demonstrated great willingness to be active participants in the decision-making process by lending their experiences (Holtzman et al., 2019). As such, the patient community represents a critical and obtainable voice as this field moves forward in the “big data” era.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (grant number: HD 072208).