
Abstract
Objectives:
To identify early markers of acute treatment response among youth with anxiety disorders receiving cognitive behavioral therapy (CBT), selective serotonin reuptake inhibitor (SSRI) monotherapy, or their combination.
Background:
Although many youth with anxiety disorders benefit from CBT or SSRIs, response trajectories vary. Identifying early indicators of nonresponse may guide sequencing strategies and improve timely treatment delivery.
Methods:
Using data from the Child/Adolescent Anxiety Multimodal Study, improvement trajectories were modeled for youth (age 7–17) randomized to sertraline monotherapy (N = 133), CBT monotherapy (N = 139), their combination (N = 140), and placebo (N = 76). Patients were stratified by percent change in Pediatric Anxiety Rating Scale (PARS) scores at multiple time points, and logarithmic and logistic time-trend regression models were used to estimate the probability of response. Receiver operating characteristic (ROC) analyses were used to identify thresholds of improvement for predicting response.
Results:
In the sertraline group, ≥25% improvement in PARS score at week 4 had a higher probability of response by week 12 (60.8%) than <25% improvement (31.7%, p = 0.001). In CBT-treated youth, week 4 PARS improvement was less predictive of response, with ≥25% improvement predicting a 47.9% chance of response compared with 28.6% for <25% improvement (p = 0.025). In the combined treatment, ≥25% improvement predicted a73.3% probability of response, whereas <25% improvement yielded a 51.3% likelihood of response (p < 0.001). ROC analyses similarly suggested that week 4 improvement in PARS scores in the CBT group had near equivocal predictive value, though this improved by week 6 to levels comparable to those of the other treatment groups. At week 6, roughly 25% improvement in PARS score in the combined treatment had the best sensitivity and specificity for predicting response.
Conclusions:
Early improvement can predict treatment response in youth with anxiety disorders receiving sertraline monotherapy or combination treatment (sertraline and CBT). Conversely, the absence of early improvement in CBT-treated youth does not reliably predict treatment nonresponse. Treatment-specific thresholds may inform clinical decision making, and support earlier SSRI optimization while allowing more time to observe CBT-related gains.
Keywords
Introduction
Characterizing treatment response trajectories in youth with anxiety and related disorders is critical for guiding clinical decision-making. Identifying response signatures: distinct, early-emerging patterns of change suggest when it is warranted to switch or augment, and predict whether a given treatment will likely succeed or veer toward futility, all of which may influence the acceptability of treatments (McNeil et al., 2025). These signatures, akin to a treatment’s fingerprint in a specific patient, may reduce uncertainty for patients, families, and clinicians, shortening the time youth spend on ineffective treatments, and potentially optimizing the path to remission.
Anxiety disorders commonly emerge in childhood or adolescence (Beesdo et al., 2010; Warner et al., 2023) and are associated with substantial morbidity (Asselmann et al., 2018; Ramsawh et al., 2010; Ramsawh and Chavira, 2016). Youth with untreated anxiety disorders experience academic underachievement and difficulties in peer and family relationships (Copeland et al., 2015; Pollard et al., 2023). Over the longer term, untreated youth are at increased risk of developing depressive (Beesdo et al., 2007; Bittner et al., 2004), substance use disorders (Asselmann et al., 2014), and including suicide attempts (Husky et al., 2012).
Importantly, many children and adolescents with anxiety disorders benefit from first-line treatments such as cognitive behavioral therapy (CBT) (Locher et al., 2017; Walkup et al., 2008) and selective serotonin reuptake inhibitors (SSRIs) (Dobson et al., 2019; Locher et al., 2017; Strawn et al., 2018). However, despite the efficacy of CBT and SSRIs, treatment response trajectories—the pattern and timing of symptom change over the course of treatment—vary considerably (Bai et al., 2023; Strawn et al., 2022; Suresh et al., 2020).
Expert consensus suggests that for SSRIs, 8–12 weeks are needed to assess response (Baldwin et al., 2005), assuming adequate dosing (Ramsey et al., 2021; Strawn et al., 2019) and adherence (Strawn et al., 2021, 2025). In contrast, improvement with CBT may trail what is seen with SSRIs. Its core components, including psychoeducation, relaxation training, cognitive restructuring, and exposure exercises, are typically introduced sequentially (Ale et al., 2015; Mendez et al., 2023). Although exposures exercises are empirically supported as the most active ingredient of CBT (Peris et al., 2017; Whiteside et al., 2020), they may be delivered later in treatment and delay response trajectory (Mendez et al., 2023; Peris et al., 2015).
Trajectories of improvement have been directly examined in the Child/Adolescent Anxiety Multimodal Study (CAMS), in which youth aged 7–17 years (N = 488) were randomized to CBT, sertraline, their combination, or placebo (Peris et al., 2015; Walkup et al., 2008). The probability of sertraline response plateaued by week 8 (Strawn et al., 2017, 2018). In contrast, CBT response probability increased over the 12-weeks of treatment (Strawn et al., 2017). Among CBT-treated youth, longitudinal discontinuity analyses revealed that the introduction of cognitive restructuring (e.g., modifying maladaptive self-talk) and exposure tasks dramatically increased the trajectory of CBT response, whereas relaxation training had minimal impact (Peris et al., 2015).
Data on trajectories of response will be critical to empirically determine the best starting treatment and sequences in care to achieve remission. New methodologies, such as sequential multiple assignment randomized trials (SMART), will require evidence-based guidance about time frames for achieving a response that signals a later good outcome. In a SMART trial of interpersonal psychotherapy for depressed adolescents (IPT-A), patients were randomized to a decision point at either week 4 or week 8, at which insufficient responders were re-randomized to either more frequent IPT-A sessions or fluoxetine augmentation. Earlier intervention (at week 4) resulted in greater reductions in depressive symptoms and improved functioning compared with intervention at week 8 (Gunlicks-Stoessel et al., 2019). These findings highlight the utility of tracking symptoms early in psychotherapy and suggest that adjustment earlier in treatment could improve outcomes.
Given these considerations, a key question is whether reductions in anxiety symptoms at specific time points during treatment, whether CBT, pharmacotherapy, or their combination, can reliably predict eventual treatment response or remission. Understanding these early markers would represent a shift from a “wait-and-see” approach to a more proactive, data-driven model of care, in which treatments are adjusted not after failure but in anticipation of it.
To address this question, we examined whether early symptom changes at specific time points could predict subsequent treatment response in youth with anxiety disorders. We hypothesized that treatment response trajectories differ by treatment modality and that thresholds of early symptom improvement can predict eventual treatment response. Using data from the CAMS (Walkup et al., 2008), we estimated the likelihood of treatment response based on varying degrees of improvement (or lack thereof) at clinically relevant time points in youth receiving CBT, SSRI monotherapy, or their combined treatment.
Methods
Participants
Data were obtained from the CAMS—a 12-week, multicenter, randomized controlled trial that examined the efficacy of CBT (N = 139), sertraline (N = 133), their combination (N = 140), and placebo (N = 76) in youth with pediatric anxiety disorders. The sample was predominantly White (79%) and non-Hispanic, with a mean age of 10.7 ± 2.8 years. Anxiety disorder diagnoses within the sample included separation anxiety disorder (54%), generalized anxiety disorder (79%), and social anxiety disorder (46%), with many participants meeting criteria for more than one anxiety disorder. Baseline anxiety severity was moderate-to-severe, as measured by the Pediatric Anxiety Rating Scale (PARS) (The Research Units on Pediatric P, 2002). Dimensional and categorical measures of anxiety severity and global severity were obtained at weeks 4, 8, and 12. CAMS was conducted at six academic medical centers (University of California, Los Angeles; Johns Hopkins University; Columbia University; Duke University; Temple University; and the University of Pittsburgh) across the United States. Institutional review boards at each study center approved the study protocol, and subjects and one or more guardians provided written informed consent before study procedures.
Statistical analysis
Treatment effects were modeled using a Bayesian inferential approach, with posterior distributions estimated using Hamiltonian Monte Carlo simulations, as previously described (Mills and Strawn, 2020; Stimpfl et al., 2023; Suresh et al., 2020). Uninformative priors were used in all models.
Patients were stratified into quintiles based on the observed percentage change from baseline in PARS scores at week 4,
The following models were estimated for each quintile-grouped datasets. A logarithmic trend model was specified as:
Finally, to identify PARS improvement thresholds that best predict response, receiver operating characteristic (ROC) analyses were conducted at weeks 4 and 6. As there were no observed data at week 6, PARS values were imputed using the fitted trajectory model. Sensitivity and specificity were calculated at the optimal threshold determined by Youden’s J statistic. Patients were subsequently classified as predicted responders or nonresponders based on this threshold, and baseline demographic and clinical characteristics were summarized descriptively within predicted response groups for each treatment arm (Table 2).
Analyses were conducted in Julia (version 1.11) (Bezanson et al., 2017) and R (version 4.5.0) (R Core Team, 2024). Models were estimated using 5000 iterations of the No-U-Turn Hamiltonian Monte Carlo sampler in Turing.jl (Ge et al., 2018). For all analyses, Bayesian posterior tail-area equivalents of a frequentist p value for evidence against the null hypothesis (H0) were determined and considered statistically significant at p < 0.05 level. Means are represented as mean ± standard deviation, and precision is expressed as 95% credible intervals (Bezanson et al., 2017; Ge et al., 2018; R Core Team, 2024).
Results
Symptom trajectories based on week 4 improvement
For the week 4 PARS improvement modeling, trajectory coefficients were negative, decreased as the PARS improvement threshold increased, and were statistically significant at p < 0.001 for all quintile models (Fig. 1). The probability of reaching a response at week 12 (CGI-I score of ≤2), as estimated by the fitted Bayesian models, is presented in Table 1. In sertraline-treated patients, a ≥25% improvement in PARS score at week 4 predicted a 60.8% probability of response (CGI-I ≤ 2) by week 12, compared with 31.7% for those with <25% improvement (p = 0.001). For patients receiving CBT, a ≥25% improvement at week 4 predicted a 47.9% chance of response, compared with 28.6% for patients with <25% improvement (p = 0.025). In the combined treatment, a ≥25% improvement at week 4 predicted a 73.3% probability of response, whereas improvement of <25% was associated with a 51.3% likelihood of improvement (p < 0.001).
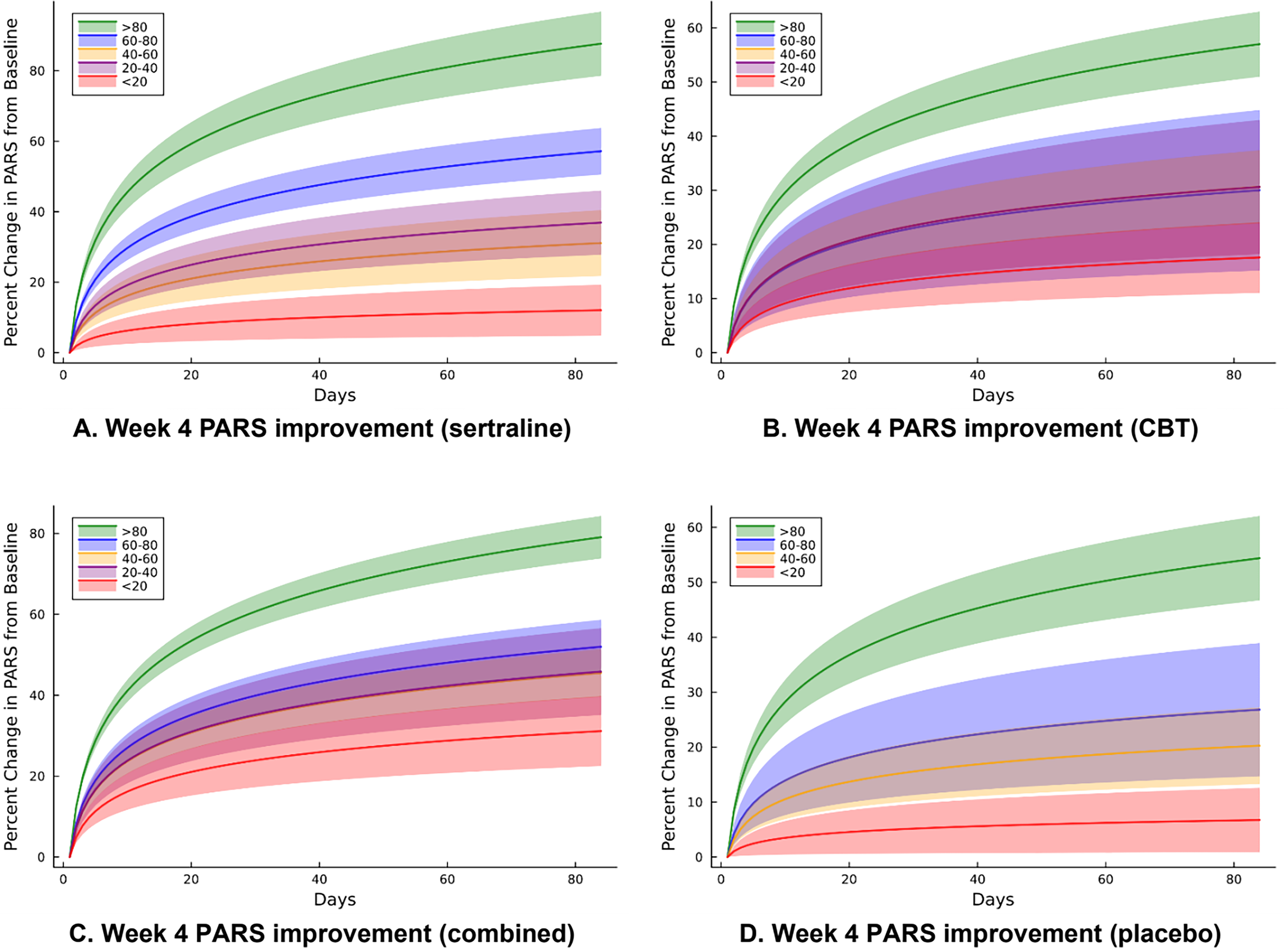
Trajectory of improvement (weeks 0–12) based on week 4 improvement (percentage change in PARS). Model-estimated improvement trajectories by quintile of percent reduction in PARS score from baseline to week 4 in anxious youth randomized to
Predicted Probability of Response Based on Percent Pediatric Anxiety Rating Scale Reduction
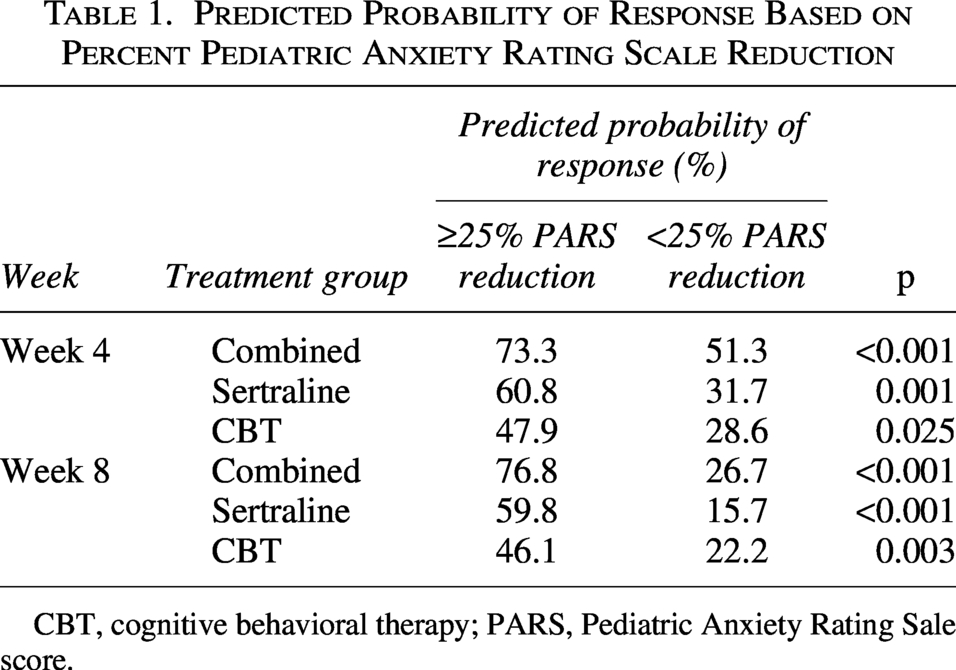
CBT, cognitive behavioral therapy; PARS, Pediatric Anxiety Rating Sale score.
Symptom trajectories based on week 8 improvement
Similarly, for the week 8 PARS improvement modeling, trajectory coefficients were negative, decreased as the PARS improvement threshold increased, and were statistically significant at p < 0.001 for all quintile models except the <20% improvement by week 8 group (p = 0.16) (Fig. 2). In sertraline-treated patients, a ≥25% improvement in PARS score at week 8 predicted a 59.8% probability of response (CGI-I ≤ 2) by week 12, compared with 15.7% for those with <25% improvement (p < 0.001) (Table 1). For patients receiving CBT, a ≥25% improvement at week 8 predicted a 46.1% chance of response, compared with 22.2% for patients with <25% improvement (p = 0.003). In the combined treatment, a ≥25% improvement at week 8 predicted a 76.8% probability of response, whereas improvement of <25% was associated with a 26.7% likelihood of improvement (p < 0.001).
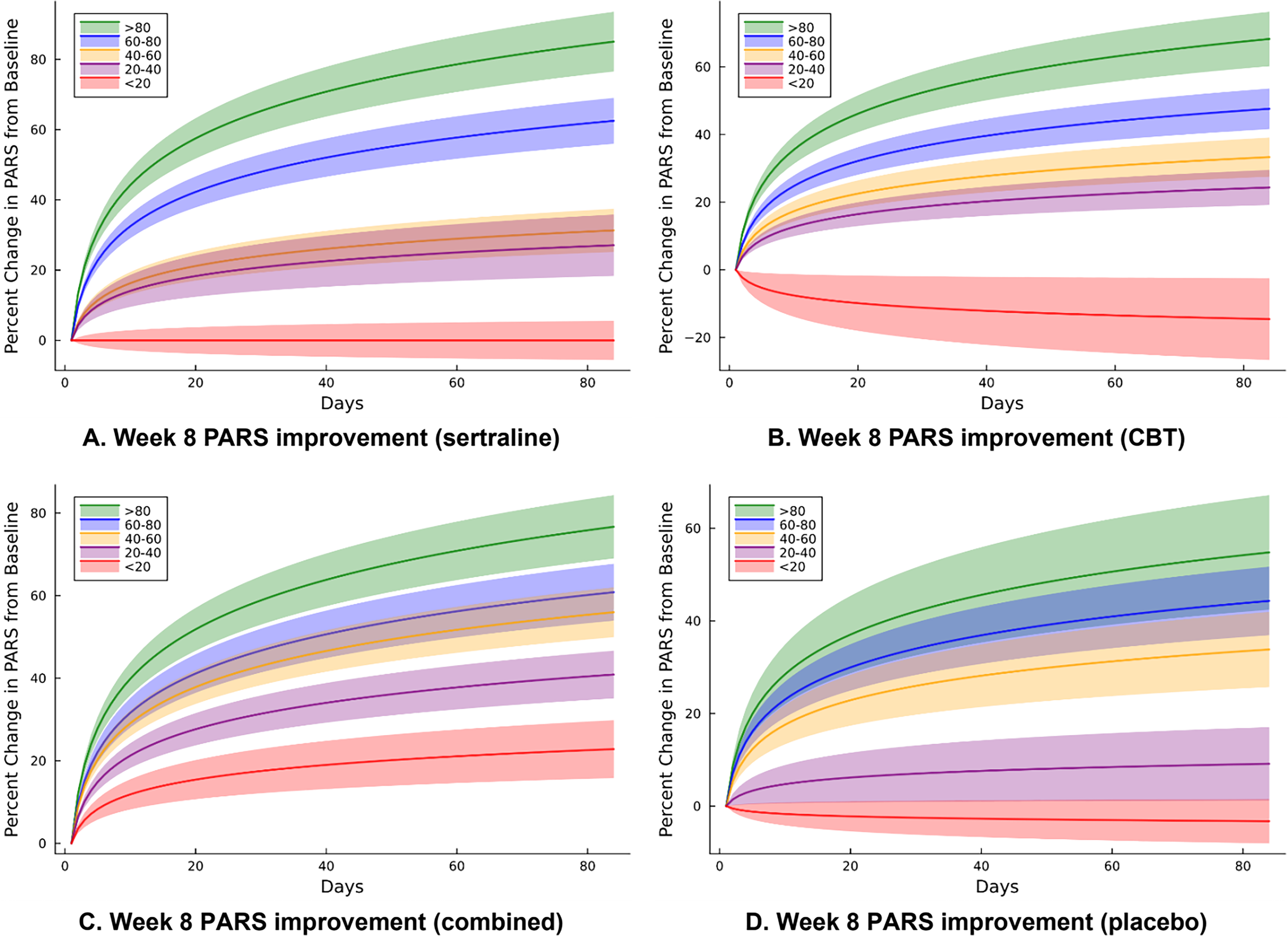
Trajectory of improvement (weeks 0–12) based on week 8 improvement (percentage change in PARS). Model-estimated improvement trajectories by quintile of percent reduction in PARS score from baseline to week 8 in anxious youth randomized to
Receiver operating characteristic analyses
In a ROC analyses, the predictive utility of early symptom improvement differed by treatment (Fig. 3). The percentage improvement (threshold) in PARS score at weeks 4 and week 6 that yielded the best combination of sensitivity and specificity for predicting response at week 12 is shown in Table 2. For CBT-treated youth, week 4 improvement was a poor predictor of week 12 response (area under the curve [AUC] 0.52; sensitivity 0.43), whereas at week 6 improvement substantially better discriminated between responders and nonresponders at week 12 (AUC 0.78; sensitivity 0.78). In contrast, for sertraline-treated patients, predictive accuracy was similar at both weeks 4 and 6. Week 4 improvement yielded moderate discrimination (AUC, 0.73; sensitivity, 0.68), and week 6 metrics improved only modestly (AUC, 0.86; sensitivity, 0.85). Combined treatment showed the highest Youden’s Index at J = 0.82 (indicating strongest overall performance), with week 6 improvement providing excellent classification accuracy (AUC, 0.94; sensitivity, 0.86), whereas week 4 predictions were already robust (AUC, 0.76; sensitivity, 0.75). Placebo trajectories showed moderate predictive performance at both time points. Demographic characteristics were summarized according to predicted likelihood of response at week 6 (Table 3).
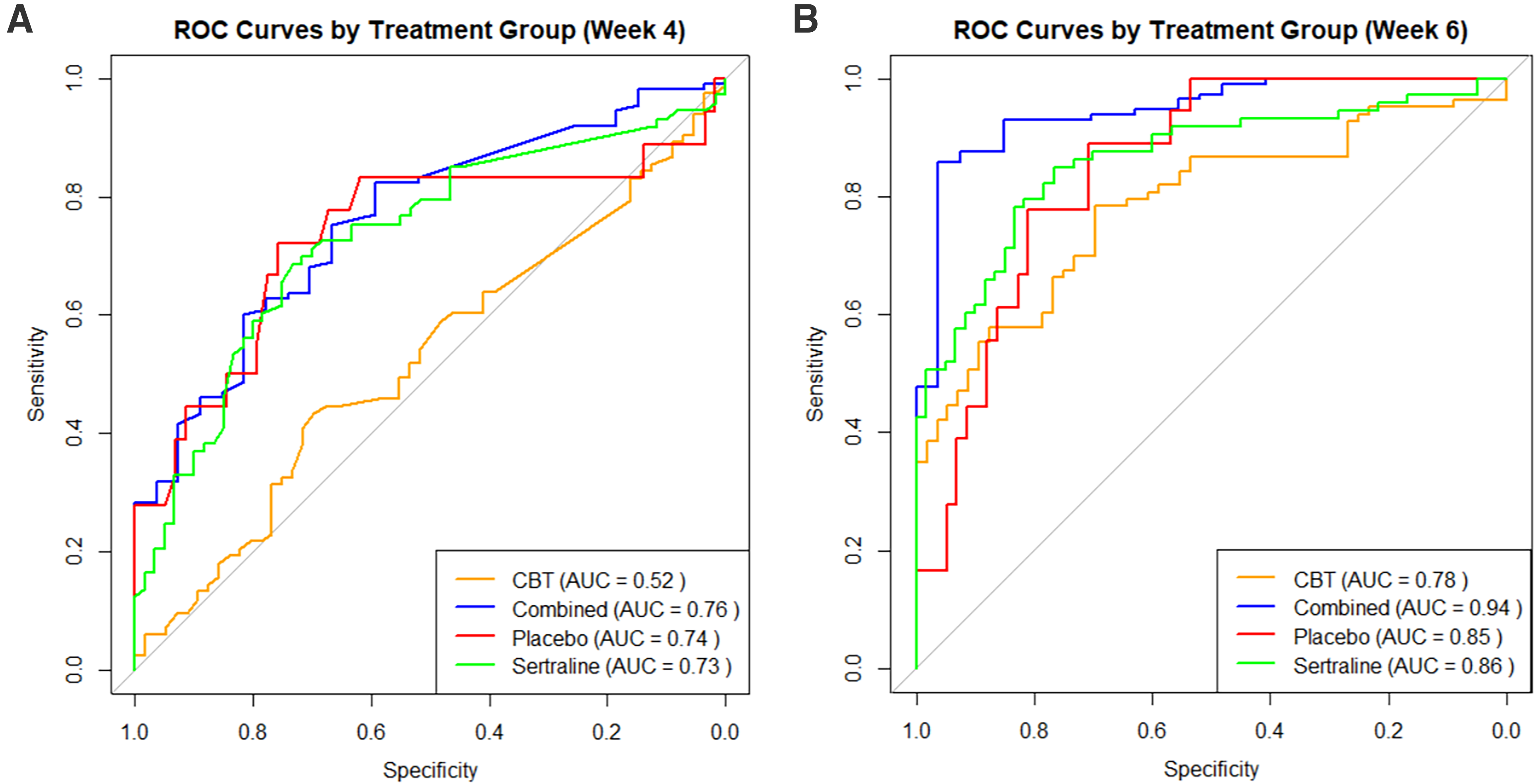
Receiver operating characteristic (ROC) curves by treatment group. Receiver operating characteristic analyses by treatment group based on the optimal percent reduction in PARS score for predicting endpoint treatment response (CGI-I
Receiver Operating Characteristic Analysis: Sensitivity and Specificity
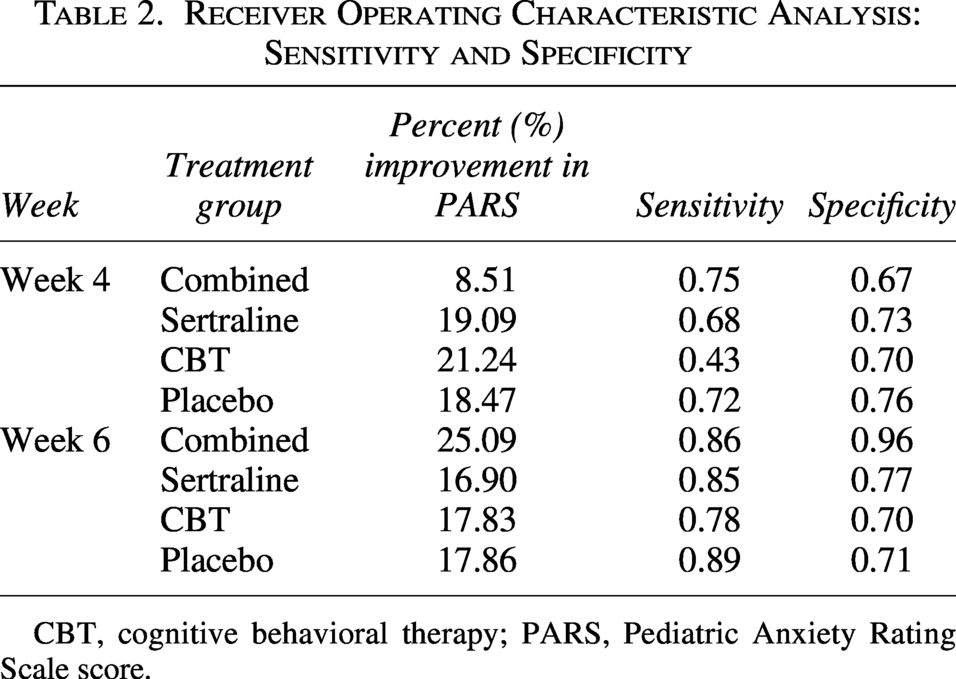
CBT, cognitive behavioral therapy; PARS, Pediatric Anxiety Rating Scale score.
Demographics by Predicted Response at Week 6
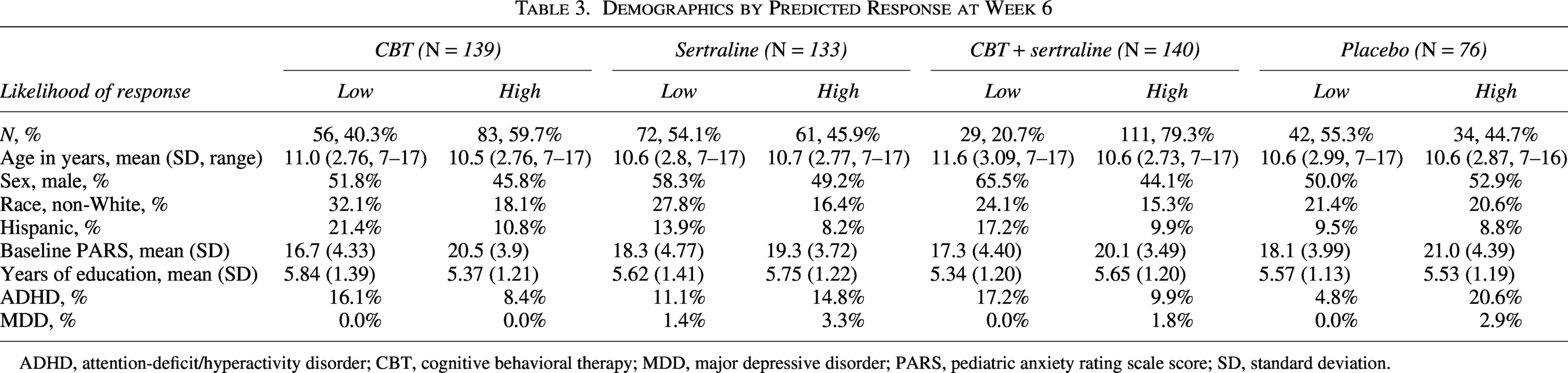
ADHD, attention-deficit/hyperactivity disorder; CBT, cognitive behavioral therapy; MDD, major depressive disorder; PARS, pediatric anxiety rating scale score; SD, standard deviation.
Discussion
Treatment response trajectories vary among youth and by intervention type. Characterizing patient-specific treatment-response trajectories may help clinicians move beyond general, “one-size-fits-all” timelines and better tailor care for youth with anxiety disorders. Furthermore, improvement thresholds and associated probability of response may prove valuable for measurement-based care by providing useful targets for clinicians during shared decision-making conversations with patients and families. While “starting low and going slow” has guided clinicians for decades, with an increasing focus on quality of care and optimizing outcomes there may be increased urgency to identify effective and efficient treatment pathways to ensure the best chance for remission and improve long-term outcomes. Improving the pace of care to ensure optimal outcomes has the potential for not only improving short- and long-term outcomes but may also facilitate better patient/family engagement and adherence, allow for accurate attribution of treatment engagement to benefit and potential for patients and families to invest more deeply in treatment via efficient optimized and personalized treatment trajectories.
The current study examined how the magnitude of early symptom improvement predicts eventual treatment response in youth with anxiety disorders receiving CBT, SSRI monotherapy, or their combination. Consistent with prior literature documenting distinct timelines to response, we found differences in response trajectories among the three active treatments. It was possible to predict acute-treatment response for SSRI monotherapy early in the course of treatment: Using our fitted trajectory model, we found that positive treatment response could be meaningfully estimated as early as week 4.
This study extends prior work by introducing response probabilities and treatment-specific improvement thresholds that may be used to guide tailored, shared clinical decision-making, thereby providing an avenue to advance measurement-based care. Our ROC analysis identified the week 4 and week 6 PARS percent-improvement thresholds that maximized the combined sensitivity and specificity for predicting treatment response. Results were variable at week 4, with particularly poor sensitivity (43%) of the CBT improvement threshold (21% improvement in PARS score) in identifying likely responders, resulting in poorer overall discriminative performance (i.e., AUC) compared with the other treatment groups. Week 6 thresholds demonstrated fair (70%–79%) to excellent (≥90%) sensitivity and specificity across all groups. Combined treatment at week 6 demonstrated the strongest early prediction, reflecting its more rapid treatment trajectory. Given the sequential, multicomponent structure of CBT used in CAMS, with exposure exercises concentrated in the second half of treatment, longer time frames were needed to reliably gauge CBT response.
Early improvement did not meaningfully predict treatment response in CBT-monotherapy youth, and those with slower response trajectories still had the possibility of favorable response. This is expected given that exposures—the most active ingredient in CBT—did not begin until week 6 in CAMS and were linked to the steepest rate of change thereafter (Peris et al., 2015). Caregivers and providers should keep this in mind when tracking clinical response. Whereas week 4 symptom improvement may be sufficient to guide decisions about staying the course/augmenting for SSRI monotherapy, a longer time frame is needed to evaluate whether to augment CBT monotherapy with medication or intensified CBT. This is particularly true given research showing that CBT effects tend to “grow” over time as skills consolidate with additional practice both in and out of therapy (Kendall et al., 2004; Kodal et al., 2018). Further research is needed to determine whether exposure tasks can be introduced earlier without reducing efficacy. For example, a recent randomized controlled trial in anxious youth compared CBT introducing exposure early (sessions 2–3) versus delaying exposure until session 7. The early-exposure group showed greater anxiety reduction at mid treatment and post treatment, as well as faster response and remission and more rapid reductions in avoidance and functional impairment (Gloe et al., 2026; Whiteside et al., 2024).
A common clinical assumption is that SSRIs require at least 4–6 weeks before treatment effects can be assessed; however, this view does not acknowledge early, clinically meaningful symptom change, which has been demonstrated meta-analytically in SSRI-treated youth with anxiety disorders (Strawn et al., 2018). The neurobiological basis of this notion—i.e., the apparent delayed action of SSRIs in many disorders—has been attributed to desensitization and subsequent downregulation of 5-HT1A somatodendritic autoreceptors, resulting in increased serotonin release at the synapse (Albert et al., 1996; Hervás et al., 2001); however, this single mechanism is unlikely to account for the full extent of clinical improvement observed with SSRI treatment. Our results suggest that SSRI response in anxiety disorders may be meaningfully assessed earlier than 8 weeks. This is consistent with recent studies, including a meta-analysis of antidepressant response in pediatric anxiety disorders (Strawn et al., 2018) and a placebo-controlled trial of escitalopram in youth with generalized anxiety disorder that demonstrated significant improvement by week 2 (Strawn et al., 2023). Mechanistically, increased amygdala–ventrolateral prefrontal cortex connectivity has been observed in escitalopram-treated youth within the first 2 weeks of treatment (Lu et al., 2021).
Furthermore, it is also important to consider that the neurobiology and timing of treatment response may differ across psychiatric disorders. For example, SSRI response in obsessive-compulsive disorder has conventionally been considered delayed relative to depressive and anxiety disorders (Pittenger and Bloch, 2014), potentially reflecting slower circuit-level changes or the influence of family factors (Jacoby et al., 2021; Lebowitz et al., 2016; Peris et al., 2008); however, some patients improve faster, even within the first several weeks (Issari et al., 2016). Other important factors in determining an adequate treatment trial include adherence and appropriate dosing. Optimal dosing may require consideration of individual pharmacokinetic factors (e.g., CYP metabolizer phenotype), as significant variability in medication exposure has been observed for some SSRIs (e.g., escitalopram) across metabolizer phenotypes (Strawn et al., 2021).
Beyond treatment and disorder, demographic, clinical, and psychological factors may influence treatment-response trajectories. Faster response trajectories to SSRI + CBT combination treatment have been observed in younger patients and in those with milder baseline symptom severity and depressive disorders. In contrast, slower response trajectories have been observed among males, adolescents, and minoritized children, and those with greater baseline symptom severity and externalizing disorders such as attention-deficit/hyperactivity disorder (Strawn et al., 2022; Taylor et al., 2018). Furthermore, an analysis of CAMS participants at 3-month follow-up suggested that gains in coping efficacy mediated residual improvement in the CBT, sertraline, and combined-treatment groups (Kendall et al., 2016).
Future directions include out-of-sample validation as well as examining response trajectories in different disorders, pharmacotherapies and psychotherapies, and understanding the impact of individual patient factors, such as comorbidity and pharmacokinetic variability. Response trajectories should also be examined in naturalistic settings given that treatment sequences, combinations, and titration schedules may differ significantly as compared to that of rigorous clinical trials.
Limitations
Although this is the first trajectory-based examination of the likelihood of treatment response based on early symptom improvement in children and adolescents with anxiety disorders, there are several important limitations. First, our analyses were restricted to CBT and sertraline monotherapies, their combination and placebo (i.e., those conditions used in CAMS); therefore, these findings may not generalize to other psychotherapies or pharmacotherapies, including other SSRIs. In this regard, response trajectories may differ with more rapid SSRI titration schedules, as prior work has demonstrated clinically meaningful improvement as early as week 2 under more aggressive dosing strategies (Strawn et al., 2018). Similarly, for some SSRIs in youth, dosing may be informed individual differences in medication metabolism, which may produce faster improvement (Strawn et al., 2021) Second, although CAMS was conducted within a rigorously implemented, double-blind, placebo-controlled framework, there are inherent concerns related to generalizability. Participants with common real-world comorbidities (e.g., substance use disorders, significant depressive symptoms, or complex medical conditions) were excluded. As a result, early-response thresholds that we have observed herein may not fully translate to more heterogeneous clinical populations. Third, residual confounding cannot be entirely ruled out. Treatment adherence, family functioning, school stressors, or therapist variability (in the CBT condition) may influence early improvement but were not explicitly modeled.
Conclusion
Early clinical improvement may meaningfully predict eventual treatment response among youth with anxiety disorders receiving CBT, SSRIs, or their combination, although response trajectories differ by treatment modality. Treatment-specific symptom-improvement thresholds may inform clinical decision-making by supporting earlier evaluation of SSRI monotherapy while allowing additional time for CBT-related improvement to emerge.
Clinical Significance
In treating pediatric anxiety disorders, clinicians must allow for an adequate treatment trial while avoiding delays in effective treatment. For some patients, early improvement can signal an increased probability of response. Trajectories of improvement among CBT-treated patients may be delayed, potentially reflecting the later introduction of effective exposures within the sequence of treatment. In cases of insufficient treatment response, clinicians may consider earlier optimization of SSRI monotherapy—such as dose escalation, augmentation with psychotherapy or additional pharmacotherapy, or switching medications—while allowing more time to evaluate the efficacy of CBT. Target thresholds of symptom improvement may meaningfully predict response and help guide shared decision-making conversations with patients and their families.
Footnotes
Disclosures
J.R.S. has received research support from the National Institutes of Health and PCORI and has also received material support from Myriad Genetics. Additionally, he receives royalties from Springer Publishing and Cambridge University Press, honoraria from the Neuroscience Education Institute, and serves as an author for UpToDate. J.R.S. has served as a consultant for MindMed, AbbVie, Alkermes, Collegium, Otsuka, Vistagen, and Genomind. He also serves on the speaker’s bureau for Abbvie, Collegium, and Myriad Genetics. J.A.M. has received research support from the National Institutes of Health and the Yung Family Foundation. T.S.P. has received research support from the National Institutes of Health, the National Science Foundation, and PCORI and has also received royalties from Elsevier and Oxford University Press. J.C.P. has received research support from the National Institutes of Health and royalties from Elsevier, Guilford Press, and Oxford University Press. In addition, he is a part-owner of VirtuallyBetter Health, LLC, a digital mental health company. J.T.W. receives royalties from Oxford Press and Wolters Kluwer. The other authors declare no potential conflicts of interest.