
Abstract
This study explored the interaction patterns of family members of individuals with disabilities in a simulated interdisciplinary team problem-solving process. Participants included 15 members of a training cohort within a Leadership Education in Neurodevelopmental and Related Disabilities program. Family trainees and non-family trainees engaged in a simulated team discussion at two points during the training year (Time 1 and Time 2). To understand how family members and other professionals interact in interdisciplinary problem-solving meetings, we applied three coding schemes to the interdisciplinary team discussions to measure language similarity, dominance and domineeringness, problem solving, and balance of power. The results suggested there were trends in the communication dynamics between family trainees and non-family trainees at Time 1 and Time 2. For example, language similarity between groups was high at both Time 1 and Time 2, yet families were less successful at controlling the team conversation at Time 2. The implications of these and other results are discussed.
Keywords
The need for interdisciplinary practice in health care is evidenced by a rich history and vast body of literature. Interdisciplinary practice describes a deep level of collaboration in which services and supports are provided jointly, with professionals of different disciplines making complementary contributions to service delivery (Sorrels-Jones, 1997). There is increasing evidence that interdisciplinary practice may reduce the duplication of or gaps in services (Leipzig et al., 2002), thereby improving health outcomes (Institute of Medicine, 2001), increasing patient satisfaction (Kramer & Schmalenberg, 2003), and reducing financial burden (Leipzig et al., 2002) particularly for individuals with disabilities and special health care needs (SHCN).
Family-Centered Care
Family-centered care, much like interdisciplinary practice, facilitates positive outcomes for individuals with disabilities and SHCN and their families. In contrast with provider-driven models of service delivery, family-centered care recognizes the integral role of the family in supporting individuals with SHCN, and is anchored upon the family’s perceptions of ideal service provision and support (Harbaugh, Tomlinson, & Kirschbaum, 2004; Lotze, Bellin, & Oswald, 2010). Efforts to incorporate principles of family-centered care into service delivery for individuals with disabilities and SHCN have been ongoing since 1987 with the Surgeon General’s call for family-centered, community-based coordinated care for individuals with SHCN and their families (U.S. Department of Health and Human Services, 1987).
Family Members as Part of the Interdisciplinary Team
Family-centered care and interdisciplinary practice are largely conceptualized as two separate constructs. While the literature supports the claim that services and supports for individuals with disabilities and SHCN should be family-centered, and planned and coordinated by an interdisciplinary team, there is not yet a strong evidence base for the consideration of family members as integral, contributing experts of the interdisciplinary team. Family participation in interdisciplinary team meetings has been examined extensively in the special education literature (e.g., Goldstein, Strickland, Turnbull, & Curry, 1980; Valle, 2011). The family-professional relationship in special education is at times strained or not well-defined. Special education professionals report that families do not meet their expectations for involvement in team meetings, yet those same professionals report that parents lack the opportunity to contribute meaningfully to team discussions (Pappas, McLeod, McAllister, & McKinnon, 2008). The most common concern with team meetings reported by families is that their input is not valued in school-based interdisciplinary team meetings for their children with disabilities. Another somewhat less reported concern is that important decisions about their children are made in pre-meetings further excluding families from the decision-making process (Valle, 2011). A third concern is the common use of technical jargon used by professionals in these meetings, which serves as another form of exclusion when families do not understand it. The unequal opportunity to contribute to the decision-making process—whether due to lack of opportunity, lack of input, or lack of understanding of technical jargon—may result in a power differential between the families and professionals.
Ruppar and Gaffney’s (2011) study of the communication trends and perceptions in a school-based interdisciplinary special education meeting suggested that education professionals with the highest professional title (e.g., education administrators) within team meetings held most of the power to structure, facilitate, and make decisions in these team meetings. Although multiple team members, including the families, provided input during the team discussion, the administrators’ comments and decisions had more influence on the final decisions made about the child’s education placement and supports.
In an analysis of the exploratory literature on culturally and linguistically diverse families’ perspectives of school-based interdisciplinary team meetings, the imbalance of power between families and professionals was a theme that emerged across numerous studies (Cobb, 2013). Families reported that this power imbalance resulted in family reluctance to contribute to the team decision-making process during meetings (Kummerer & Lopez-Reyna, 2009).
Although we have more than 25 years of research supporting the fact that families feel excluded and disempowered from the school-based interdisciplinary team process, we know little about the communication patterns in those meetings. The literature in family-professional interaction in team meetings has failed to examine and understand the dynamics of the perceived power imbalance, the microstructures of the interaction patterns in these meetings, the type of language used, or the qualitative nature of change in interaction patterns over time. Using a rigorous process of conversation analysis, the current exploratory study will attempt to measure and understand more about the latter two. Although the field of applied group work has a substantial literature base exploring group member attitudes and perceptions (e.g., Bajnok, Puddester, Macdonald, Archibald, & Kuhl, 2012), less research exists that examines the interaction patterns between families and professionals in interdisciplinary teams and the changes in their interaction patterns over time. This exploratory study aims to address those two gaps in the literature through a case-based simulation (CBS) activity.
To understand how family members contribute to interdisciplinary team problem solving, we examined the microstructures of family-professional interactions in a CBS activity. Specifically, we studied the following constructs in family-professional communication patterns: (a) the similarity or dissimilarity between the languages used by families and professionals, (b) the power difference between families and professionals, and (c) problem-solving language used by families and professionals. Literature suggests that families experience difficulty connecting to the technical jargon used by professionals in meetings (Valle, 2011); likewise, family reports indicate that the imbalance of power in meetings influences their willingness to participate in team discussions (Kummerer & Lopez-Reyna, 2009). As a result, the problem-solving process is influenced by language mismatch and power differential (Valle, 2011). We measured these constructs using two communication coding schemes that are established in the literature (Heatherington & Friedlander, 1990; Niederhoffer & Pennebaker, 2002) and one communication coding scheme that was internally developed by the authors.
Coding Schemes
Coding schemes have been used to explore communication among members of interdisciplinary teams in a range of settings. For example, while coding schemes have been applied to client–professional dyads (e.g., Beyebach & Carranza, 1997; Opel et al., 2013), participants in family therapy groups (e.g., Doba, Pezard, Berna, Vignau, & Nandrino, 2013; Heatherington & Friedlander, 1990), and communication among professionals (e.g., Bennett, Erchul, Young, & Bartel, 2012; Sheehan, Robertson, & Ormond, 2007; Wittenberg-Lyles, Gee, Oliver, & Demiris, 2009), coding schemes have not been commonly applied to teams consisting of interdisciplinary professionals and clients/family members. Moreover, studies considering client or family-inclusive interdisciplinary teams’ communications seldom explore the interdisciplinary professionals’ relationships with clients/families, focusing instead on the team as a whole or on each possible dyad within the team (Erchul et al., 1999).
Selecting the coding schemes to apply in the current study involved an in-depth review of the research on coding schemes and identifying which would be most relevant given the constructs of interest. Coding schemes exist that examine many components of communication, including the level of agreement and disagreement within a group conversation (Galley, McKeown, Hirschberg, & Shriberg, 2004), positivity and engagement within a group (Tausczik & Pennebaker, 2013), language similarity (Niederhoffer & Pennebaker, 2002), control/power (Heatherington & Friedlander, 1990), and problem solving (Bennett et al., 2012; Pazos, Micari, & Light, 2010). The latter three constructs (i.e., similarity, control/power, and problem solving) were measured in the current study using three coding schemes, respectively, Language Style Matching (LSM; Niederhoffer & Pennebaker, 2002), Family Relational Communication Control Coding System (F-RCCCS; Heatherington & Friedlander, 1990), and an internally developed, competency-based problem-solving coding scheme. The method for applying each of the three coding schemes is described below.
Language Style Matching
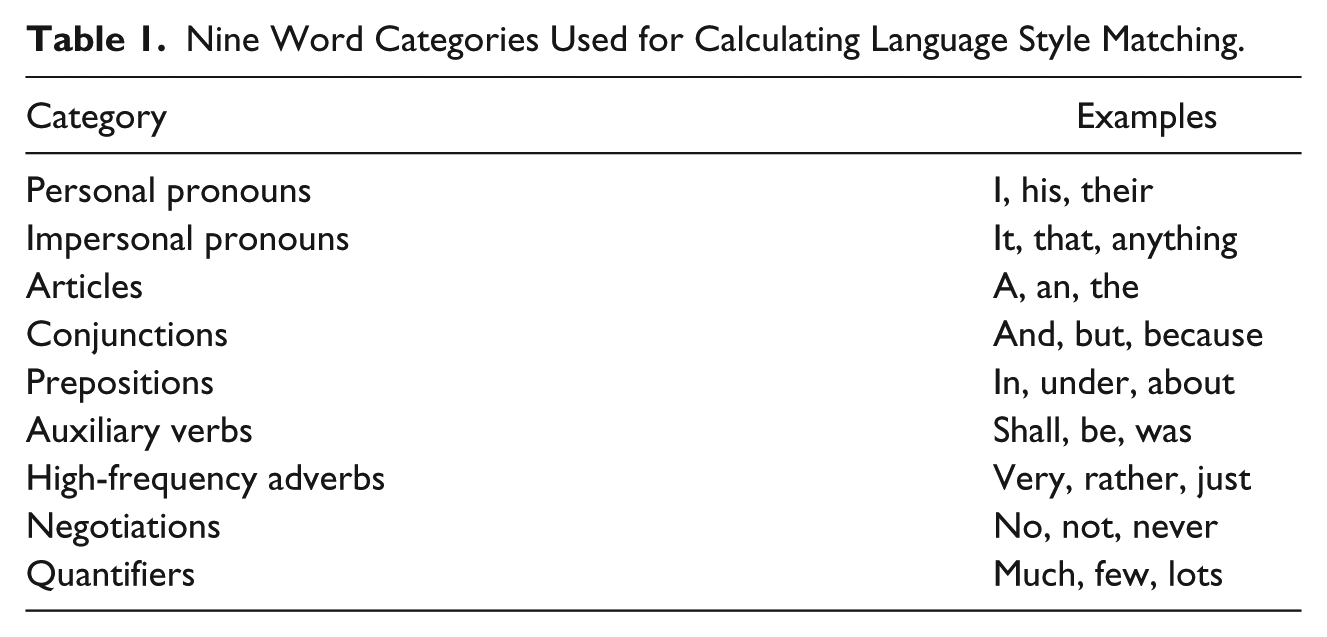
The first coding scheme applied to the interdisciplinary team problem-solving discussions was LSM, which measures similarity in language use and was an important construct to measure in our study given previous research suggesting that incongruencies in language use between professionals and families impedes the problem-solving process. More specifically, the LSM coding scheme measures the relative use of function word categories (i.e., personal pronouns, impersonal pronouns, articles, conjunctions, prepositions, auxiliary verbs, high-frequency adverbs, negations, and quantifiers; see Table 1) between dyads or group members (Niederhoffer & Pennebaker, 2002). LSM provides an estimate of verbal mimicry, which is an indicator of cooperation and being in synch (e.g., Gonzales, Hancock, & Pennebaker, 2010; Pickering & Garrod, 2004). Previously reported internal consistency reliabilities of LSM range from Cronbach’s alphas of .49 to .80 (Pennebaker & Chung, 2012). The present study utilized a computerized text analysis program, Linguistic Inquiry and Word Count (LIWC; Pennebaker, Booth, & Francis, 2007), to assist in the computation of LSM (see Table 1).
Nine Word Categories Used for Calculating Language Style Matching.
Family Relational Communication Control Coding System (F-RCCCS)
The second coding scheme applied to the interdisciplinary team problem-solving discussions was the F-RCCCS (Heatherington & Friedlander, 1990) due to its ability to measure the constructs of power, dominance, and domineeringness, which influence the dynamics in the team problem-solving process (Bennett et al., 2012). The F-RCCCS is a modified version of the relational coding scheme developed by Rogers and Farace (1975). Statements are coded for their purpose: to control conversation (referred to as a one-up), allow/support others to control conversation (one-down), or to accomplish neither (one-across). These codes can be used to determine domineeringness, which relates to attempts to control the conversation, and dominance, which are successful attempts to control the conversation.
Maternal Child Health Leadership Applied Competencies Coding Scheme (MCH-LACCS)
The third and final coding scheme applied to the simulated interdisciplinary team problem-solving discussions was the MCH-LACCS, as the current study was conducted within a Maternal Child Health leadership training program. The MCH-LACCS was developed internally by the authors and identified a team’s use of problem-solving steps while demonstrating leadership competencies. Mouradian and Huebner (2007) identified the MCH Leadership Competencies as core or applied competencies based on MCH leadership discussion at the 2004 MCH Working Conference. Mouradian and Huebner explained how core competencies, such as communication skills, are integral to applied competencies, and moreover, should be present at the time of program entry due to the difficult nature of training such skills. Our research team deliberated the idea of core versus applied competencies as well as Mouradian and Huebner’s assignments of core and applied. After in-depth discussion and analysis of MCH competency survey data, our research team ultimately agreed with the article and determined that 8 of the 12 MCH competencies fit the definition of an applied competency and were coded using MCH-LACCS (see Table 2). In addition, MCH-LACCS analyzed groups’ use of competency-based problem-solving steps, including (a) identifying a problem, (b) devising a plan, (c) carrying out a plan, and (d) evaluating the plan. Table 2 provides definitions of the MCH-LACCS codes.
Definitions of MCH-LACCS Codes.
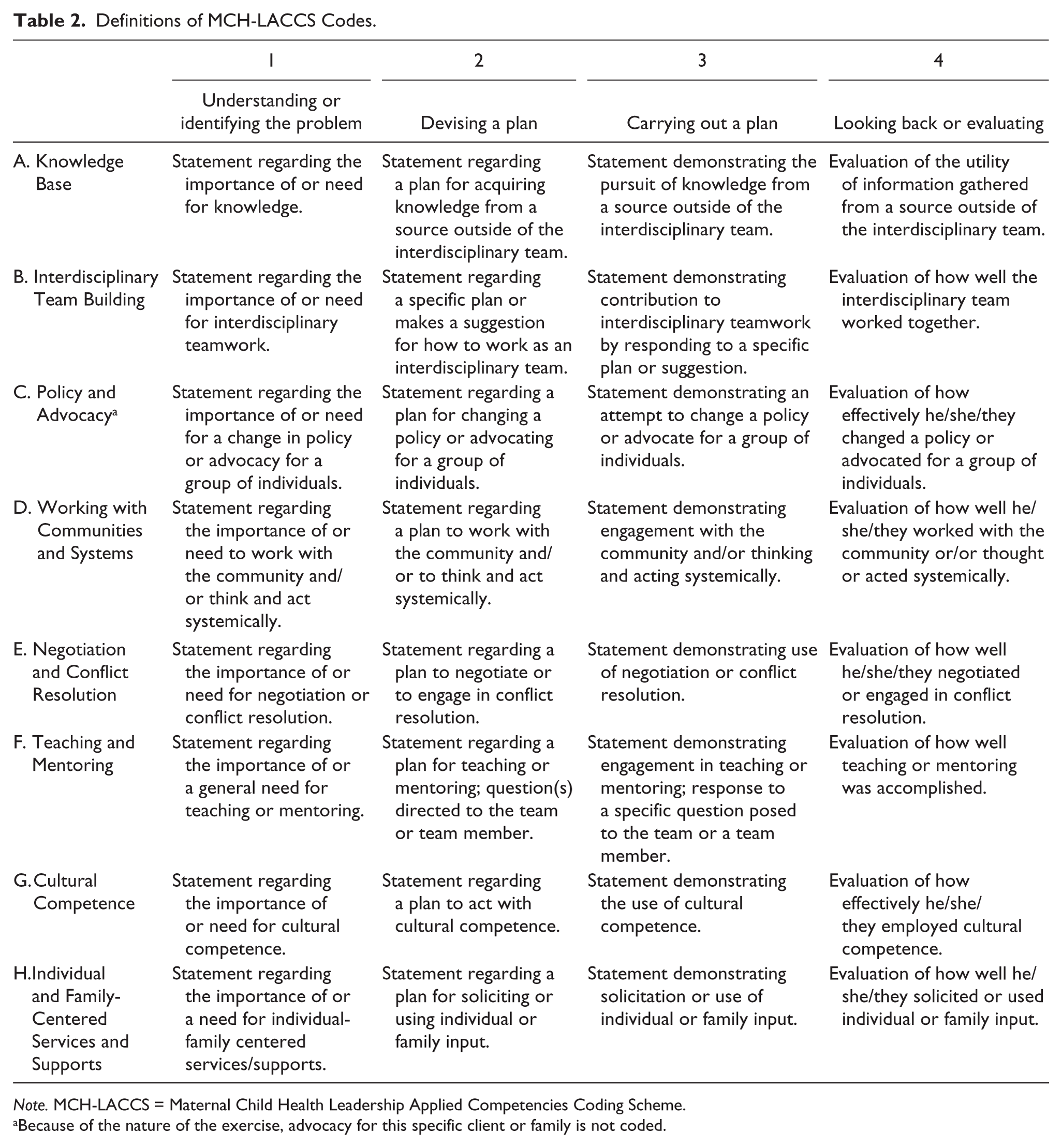
Note. MCH-LACCS = Maternal Child Health Leadership Applied Competencies Coding Scheme.
Because of the nature of the exercise, advocacy for this specific client or family is not coded.
Specifically, we asked the following questions through this study: (a) What do the results of applying the three communication coding schemes suggest about the interaction between family members in simulated interdisciplinary team discussions? and (b) How does the interaction between family members and professionals in simulated interdisciplinary team discussions differ from the Fall semester to the Spring semester along the constructs of language similarity, power/dominance/domineeringness, and competency-based problem solving? This study is largely exploratory, therefore interactions between the constructs will not be examined.
Method
Context
The current exploratory study was conducted within an interdisciplinary training program that emphasizes the importance of family-centered care. The Leadership Education in Neurodevelopmental and Related Disabilities (LEND) interdisciplinary training program, funded by the Maternal and Child Health Bureau (MCHB), is designed to “improve the health of children who have, or are at risk for, neurodevelopmental or related disabilities by preparing trainees from a wide variety of professional disciplines to assume leadership roles” (Health Resources and Services Administration [HRSA], 2010). There are currently 43 LEND programs in the United States that provide graduate level training and opportunities for future leaders. LEND trainees and fellows include students working toward graduate and postgraduate degrees to prepare for careers in clinical care, teaching, research, policy, and advocacy. In addition, LEND trainees also include working professionals, family members, and self-advocates. According to MCHB guidance, LEND trainees can be recruited from a range of 14 core and 6 related disciplines. The core disciplines, include audiology, family advocacy, health administration, developmental pediatrics, nursing, nutrition, occupational and physical therapy, pediatric dentistry, public health, psychology, social work, special education, and speech and language pathology. Related disciplines include child psychiatry, law, genetics, public policy, pediatric rehabilitation, and self-advocacy.
Although participation in LEND varies across programs, each program provides interdisciplinary training, has faculty members and trainees from a range of disciplines, and includes parents or family members as faculty members and trainees. LEND programs also share the following objectives: (a) to advance the knowledge and skills of the full range of child health professionals to improve health and health care for children with developmental disabilities; (b) to provide high-quality interdisciplinary training that emphasizes the integration of services from state and local agencies and organizations, private providers, and communities; (c) to provide health professionals with skills that foster community-based partnerships; and (d) to promote innovative and effective practices to enhance cultural competency, family-centered care, and interdisciplinary partnerships.
CBS Activity Development
Two CBS activities were scheduled during our LEND year, which corresponded to the traditional academic year; one CBS activity took place at Time 1 in the Fall semester (T1) and one took place at Time 2 in the Spring semester (T2). We had a reasonable expectation for change from T1 to T2 due to the nature of the LEND curriculum, which includes several course sessions and field experiences on topics related to family-centered care and interdisciplinary team problem solving during that period. Our aim was to analyze if change in interaction patterns occurred between T1 and T2 as a result of participation in our general LEND curriculum.
The CBS activities consisted of one medical case (T1) and one school-related case (T2), in which a child with a disability and a family seeking services and support is identified. The two activities involved the same family members and background information; however, the medical case focused on one child with a medical diagnosis, whereas the school case centered on another child in the same family experiencing school-related challenges. The trainees received case files intended to mirror an actual case file that a team of interdisciplinary professionals might use as the foundation for service planning and provision. The case files included the target family’s background information, including family history, cultural background, socioeconomic status, summary of concerns about the target child, the target child’s school and medical records, and various community-based supports and resources previously provided to the family.
The case files were developed in collaboration with representatives from a local community-based resource organization and were derived from an existing case. Necessary adjustments were made to protect confidentiality, fill information gaps, achieve consistency across the medical and school-related cases, and incorporate aspects of cultural diversity. The case files described families of color who were immigrants and dual-language speakers. After the cases were developed, they were reviewed by our community representatives again for consistency to reduce the likelihood that the differences between the cases at T1 and T2 would serve as an extraneous variable.
Participants
Our LEND trainees who participated in the CBS identified with the following disciplines: self-advocacy, family advocacy, social work, school psychology, speech language pathology, clinical neuropsychology, and physical therapy. At T1, LEND trainees were divided into two groups. Group 1T1 and Group 2T1 were composed of six and five trainees, respectively, not including the family trainees. At T2, the LEND trainees were divided into three groups. Group 1T2, Group 2T2, and Group 3T2 consisted of five, four, and three trainees respectively, not including the family trainees. One trainee was absent at the T1 CBS but present at the T2 session; however, because we did not analyze individual trainee data, the unit of analysis was the group of trainees, so the difference in sample size from T1 to T2 is inconsequential to our analyses. A limited description of each group is provided to protect the identity of the participants. The individuals playing the role of the family members were former LEND trainees who were trained to act as the family members of the child discussed in the case file.
CBS Administration Procedures
At the time of CBS administration, trainees were divided into their groups. The group facilitator provided instructions regarding the CBS, then gave each trainee a case summary, written instructions for the activity, and a problem-solving facilitation form. Afterward, one case file was provided to the group. Audio recording commenced when the groups began discussing the case. The groups were given 30 min to complete the CBS and to answer the questions outlined on the problem-solving facilitation form, as follows: As a team, (a) discuss “What do we know?” about the child, (b) discuss “What do we need to know?” about the child, (c) develop and write a problem statement in your own words, (d) list possible solutions, and (e) list actions to be taken along with a suggested timeline.
Each group facilitator was available to clarify questions and monitor the group’s progress throughout the case. Group facilitators sat separately from the group and interacted as little as possible during the CBS. The groups debriefed with the group facilitator. During the debriefing, the trainees discussed what went well during the case study, what could have been improved upon or done differently, and their perceptions regarding the family members as part of the interdisciplinary team discussion. Afterward, the groups joined together to participate in a discussion about the experience led by a research team member.
CBS Coding Data Analysis
The purpose of the CBS activity was to observe the interdisciplinary trainees’ interactions and to analyze their specific communication patterns. Data were analyzed using the three selected coding schemes.
Language Style Matching
Gonzales et al. (2010) described a method for calculating LSM between dyads. The dyadic calculation of LSM allowed our study to further analyze the communication patterns between interdisciplinary group members and family members. To perform this analysis, we organized each group’s transcription into two separate documents—Trainee Group, which contained the transcriptions of every trainee in the group, and Family Group, which contained the transcription of the family member(s). Then, each document was run independently through LIWC to determine the percentage of function words each group used. This software calculated Trainee Group’s and Family Group’s percentages for each of the nine word categories listed in Table 1. The percentages yielded by the software were used to calculate the groups’ LSM scores. In dyadic calculations of LSM, the absolute value of the differences between two speakers is divided by the added total for each category. The LSM score always falls between 0 and 1, with 1 indicating the highest degree of LSM. Gonzales et al. provided the following example for calculating personal pronouns (pp) LSM between Person 1 and Person 2 1 :

In this example, Person 1 used 5.7% personal pronouns and Person 2 used 6.4% personal pronouns. Using the above formula, their dyadic personal pronoun LSM score would be as follows:

or

The same calculation is then run for each of the nine function word categories. Then the nine separate mean LSM scores for each category are averaged to yield a dyadic total LSM score Gonzales et al. (2010).
F-RCCCS
Following the F-RCCCS coding scheme, domineeringness was calculated by dividing the number of an individual’s one-up messages by his or her total number of messages. Dominance was calculated by taking the total number of one-up messages from Group Member A that are directly proceeded by a one-down message from Group Member B and dividing it by the overall number of one-up messages spoken by Group Member A (Bennett et al., 2012).
Two members of the research team independently coded CBS transcriptions according to the F-RCCCS coding schemes. Interrater reliability was maintained at or above .90 during the coding process (Bakeman & Gottman, 1987); reliability checks were calculated with 10% of the remaining data to prevent coder drift (Schensul, LeCompte, Nastasi, & Borgatti, 1999).
MCH-LACCS
To apply MCH-LACCS, two members of the research team met regularly to consensus-code the case study transcripts (Hill et al., 2005). The same two coders participated in the consensus coding due to the importance of consistency and reliability of the coding process. Consensus coding involves intense discussion about each code, acknowledgment of the potential influence of researcher bias in the coding process, and engage in equitable discussion before coming to a consensus (Hill et al., 2005). Through the data analysis process, the results are charted. The two coders assigned codes to denote the competency and problem-solving step the interaction best matched (see Table 2 for a description of MCH-LACCS codes). The two coders also noted when a statement was directly related to one from an earlier problem-solving step. The average number of responses that each speaker received from his or her initiating statements can be used to determine his or her influence on the conversation. For example, if a group member explained that team members should introduce themselves (coded as B2), team members’ introductions would be coded (as B3) and a note would be made that they are response statements to that particular initiating statement. Also, comparing the groups’ percentages of statements coded according to each competency provided an estimate of the effort the group put toward each competency in the case study discussions. The two coders also kept track of and reached consensus on statements that were not assigned codes. Full consensus on all statements that were assigned codes and not assigned codes was achieved. Despite being a resource intensive process, consensus coding (Fahy, 2001) was used so that we could ensure 100% agreement during the coding process.
Imbalance of power within interdisciplinary team meetings is a barrier to the shared problem-solving process (Légaré et al., 2010), with individuals with the highest level of formal education often being viewed as having the most power in a team meeting (Légaré et al., 2010). Balance of power refers to the distribution of status (or valuation) among group members (Emerson, 1962) and influence (March, 1955) in a team. Because balance of power is a fundamental characteristic of the team decision-making process (March, 1955; San Martín-Rodríguez, Beaulieu, D’Amour, & Ferrada-Videla, 2005), this construct was measured using the MCH-LACCS coding scheme in the current study. Researchers computed balance of power by first counting the total number of initiating statements made by the each group’s family and trainee subgroups as well as the number of responses, made by any group member, to these initiating statements. For example, the total number of responses made to Group A’s initiating statements was divided by the Group A’s total number of initiating statements to produce balance of power, or the average number of response statements made to group members’ initiating statements.
Results
Language Style Matching
LSM scores are on a scale from 0 to 1, with a score of 1 representing exact function word matching between groups/participants. Results of the dyadic LSM calculations in this study indicate that at T1, Group 1 achieved a dyadic LSM score .806, which suggests a relatively strong LSM between the trainees and the family member.
Results of the dyadic LSM calculations indicate that at T2, Group 1 achieved an LSM score .906, which suggests a strong LSM between the trainees and the family member. Similarly, results of the dyadic LSM calculations indicate that Group 2 achieved an LSM score .842. Group 3 achieved a dyadic LSM score of .758 (see Table 3). This suggests that the language used by trainees was highly similar to the language used by family members.
LSM Scores Between Family and Trainees Measured Through F-RCCCS.
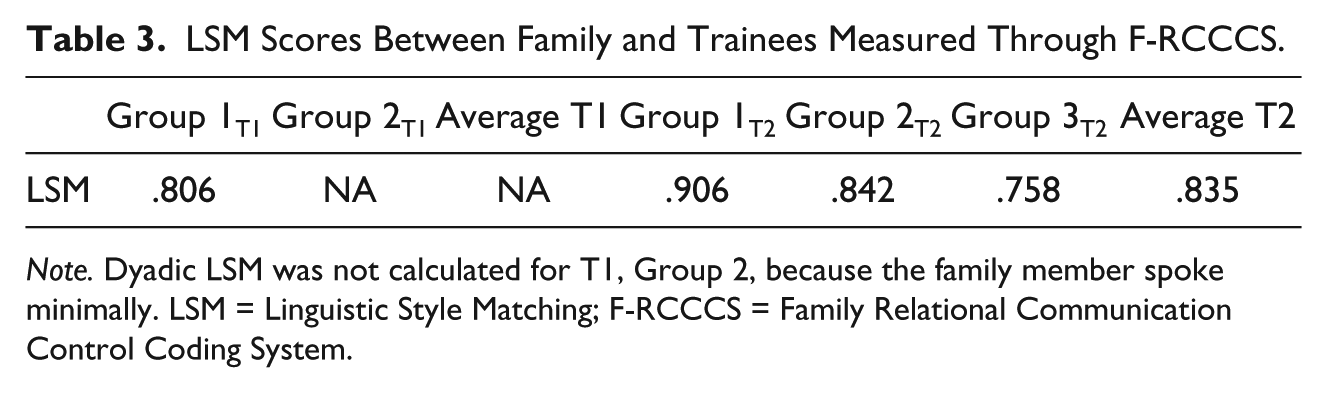
Note. Dyadic LSM was not calculated for T1, Group 2, because the family member spoke minimally. LSM = Linguistic Style Matching; F-RCCCS = Family Relational Communication Control Coding System.
F-RCCCS
Researchers used the F-RCCCS to measure participants’ domineeringness and dominance, with higher scores reflecting greater levels of those two constructs. In addition, group members’ scores were averaged to produce family, trainee, and group scores to allow us to examine the family’s involvement within interdisciplinary team discussions. Results demonstrated that domineeringness remained stable for both family and trainees from T1 to T2, with trainees exhibiting a higher level of domineeringness when compared with family. Specifically, trainees’ domineeringness was 46% at both T1 and T2 while family domineeringness was 26% at T1 and 28% at T2. This suggests that the trainees made more attempts to control the conversation at both T1 and T2. However, dominance shifted from T1 to T2, with trainees demonstrating an increase in dominance as the family’s level of dominance decreased. Specifically, trainee dominance increased from 44% at T1 to 76% at T2 and family dominance decreased from 43% at T1 to 35% at T2. This suggests that the trainees’ attempts to control the conversation were more successful at T2 and the family’s attempts to control the conversation were less successful at T2. Average domineeringness and dominance scores are presented in Tables 4 and 5.
Time 1 (T1) Domineeringness and Dominance Measured Through F-RCCCS.
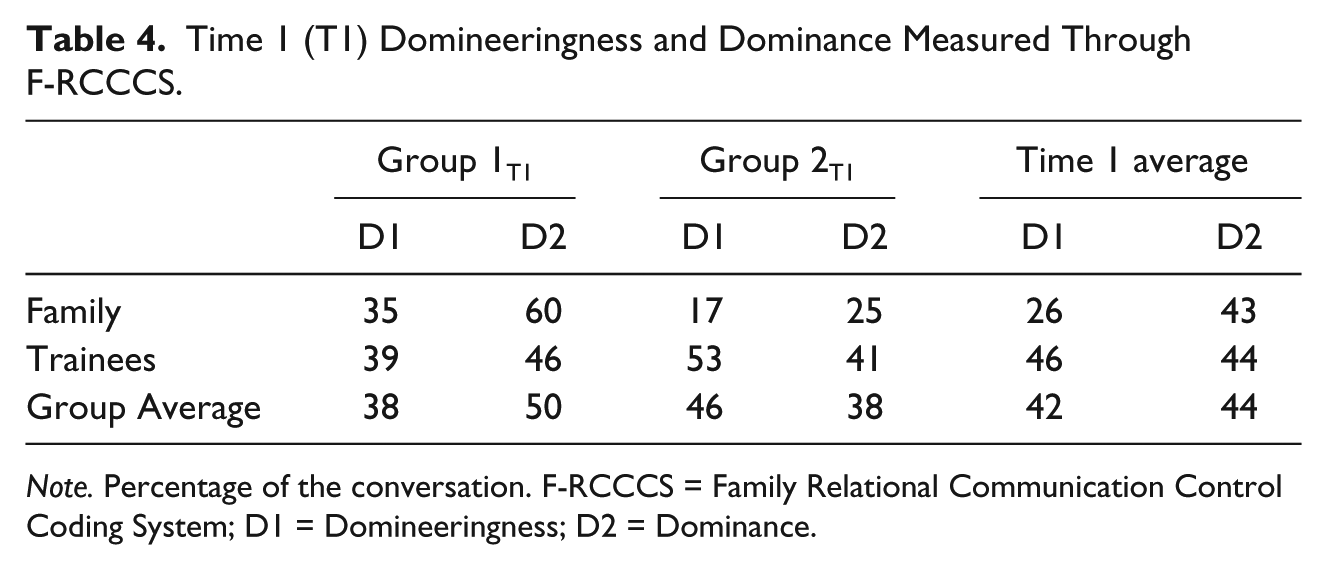
Note. Percentage of the conversation. F-RCCCS = Family Relational Communication Control Coding System; D1 = Domineeringness; D2 = Dominance.
Time 2 (T2) Domineeringness and Dominance Measured Through F-RCCCS.
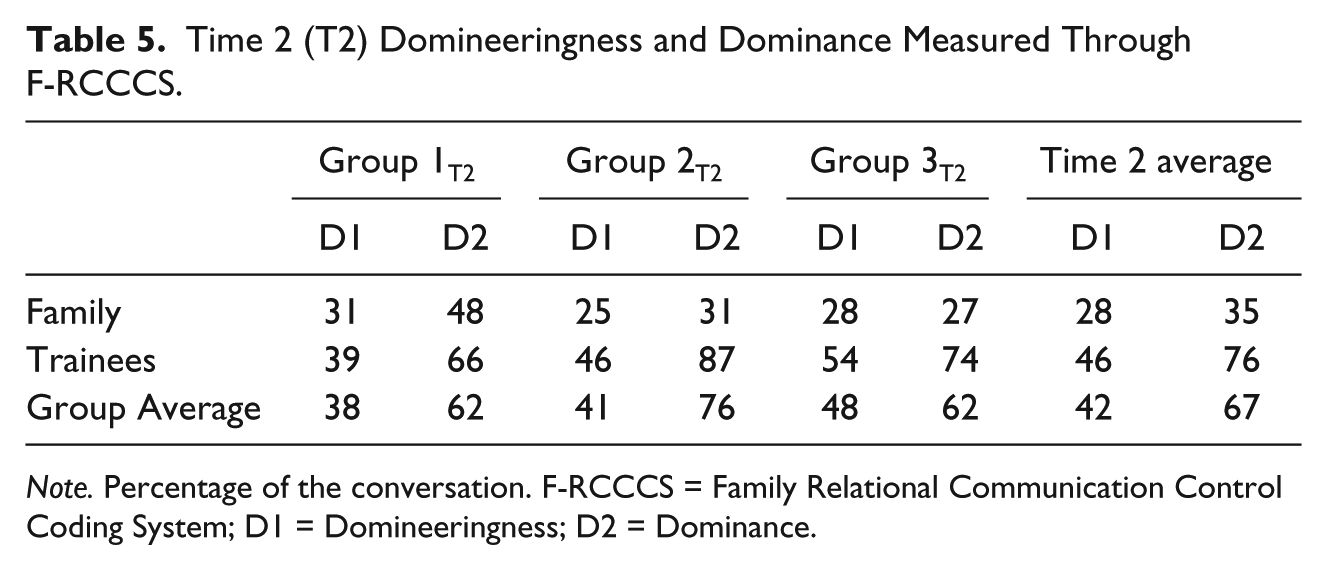
Note. Percentage of the conversation. F-RCCCS = Family Relational Communication Control Coding System; D1 = Domineeringness; D2 = Dominance.
MCH Leadership Competencies Problem-Solving Coding
The researchers applied MCH-LACCS through a qualitative coding process to estimate interdisciplinary practice, family-centered care, and balance of power. In a primary analysis, researchers determined the percentage of coded statements in each competency at T1, T2, and combined across sessions (see Table 6). All the statements were reviewed and discussed in the data analysis phase, but through the consensus coding process at T1, only 52% of the total statements were assigned codes, and at T2, only 50% of the total statements were assigned codes. In qualitative research, it is common not to assign codes to every single statement made in an interview or group discussion. To focus the remaining analyses on the competencies that emerged most often in the analyses, only competencies accounting for more than 25% of coded statements across sessions and demonstrating a 10 or more point change from T1 to T2 were analyzed further. The second phase of analysis involved researchers counting the number of statements made by each group’s family and trainee groups that were coded as (B) Interdisciplinary Team Building, (B2) specific plan or suggestion for how to work as an interdisciplinary team, (H) individual and family-centered services and supports, or (H3) solicitation or use of individual or family input. Problem-solving levels (i.e., B2, H3) were included in the second phase of analysis because researchers were particularly interested in identifying how the rate of initiating interdisciplinary teamwork (B2) changed across sessions and because during transcription and coding it became evident that solicitation of individual or family input (H3) increased dramatically from T1 to T2, accounting for 17% of coded statements at T1 and 50% of coded statements at T2. In a secondary analysis, counts were divided by the total number of statements made by the entire group, resulting in percentages, which are reported in Tables 7 and 8. Most notably, the percentage of all statements that were made by trainees and coded as H3 (solicitation of individual or family input) increased from T1 to T2 (from 10% to 26%), which indicates that trainees asked the family members more questions at T2. The percentage of all statements that were made by trainees and coded as B (Interdisciplinary Team Building) decreased (from 23% to 8%). This suggests that trainees displayed fewer interdisciplinary team building skills at T2 than they displayed at T1.
MCH-LACCS Competencies as Percentages of Total Coded Statements.

Note. MCH-LACCS = Maternal Child Health Leadership Applied Competencies Coding Scheme.
Code analyzed by Time, Group, and Family/Trainee Group Member Designation.
Time 1 (T1) Interdisciplinary Team Building, Individual and Family-Centered Services and Supports, and Power Measured Through MCH-LACCS.
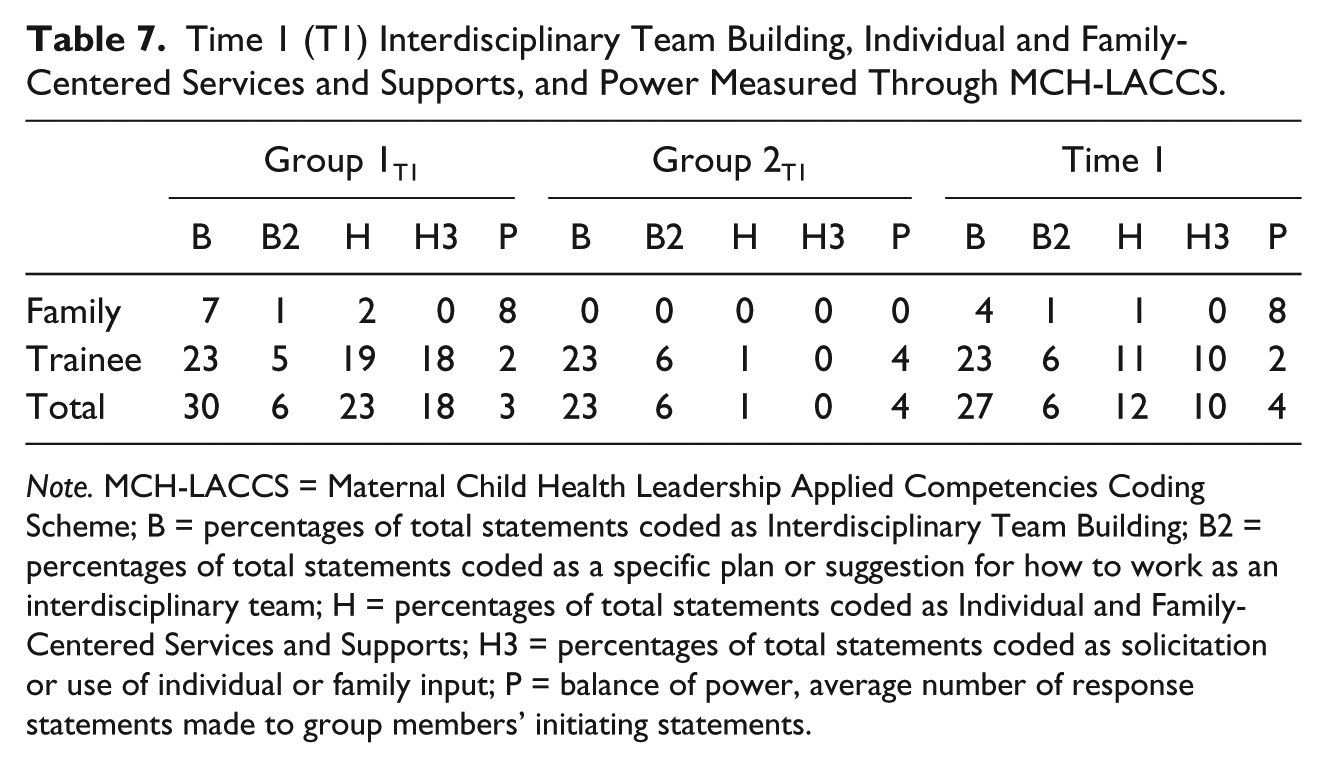
Note. MCH-LACCS = Maternal Child Health Leadership Applied Competencies Coding Scheme; B = percentages of total statements coded as Interdisciplinary Team Building; B2 = percentages of total statements coded as a specific plan or suggestion for how to work as an interdisciplinary team; H = percentages of total statements coded as Individual and Family-Centered Services and Supports; H3 = percentages of total statements coded as solicitation or use of individual or family input; P = balance of power, average number of response statements made to group members’ initiating statements.
Time 2 (T2) Interdisciplinary Team Building, Individual and Family-Centered Services and Supports, and Power Measured Through MCH-LACCS.
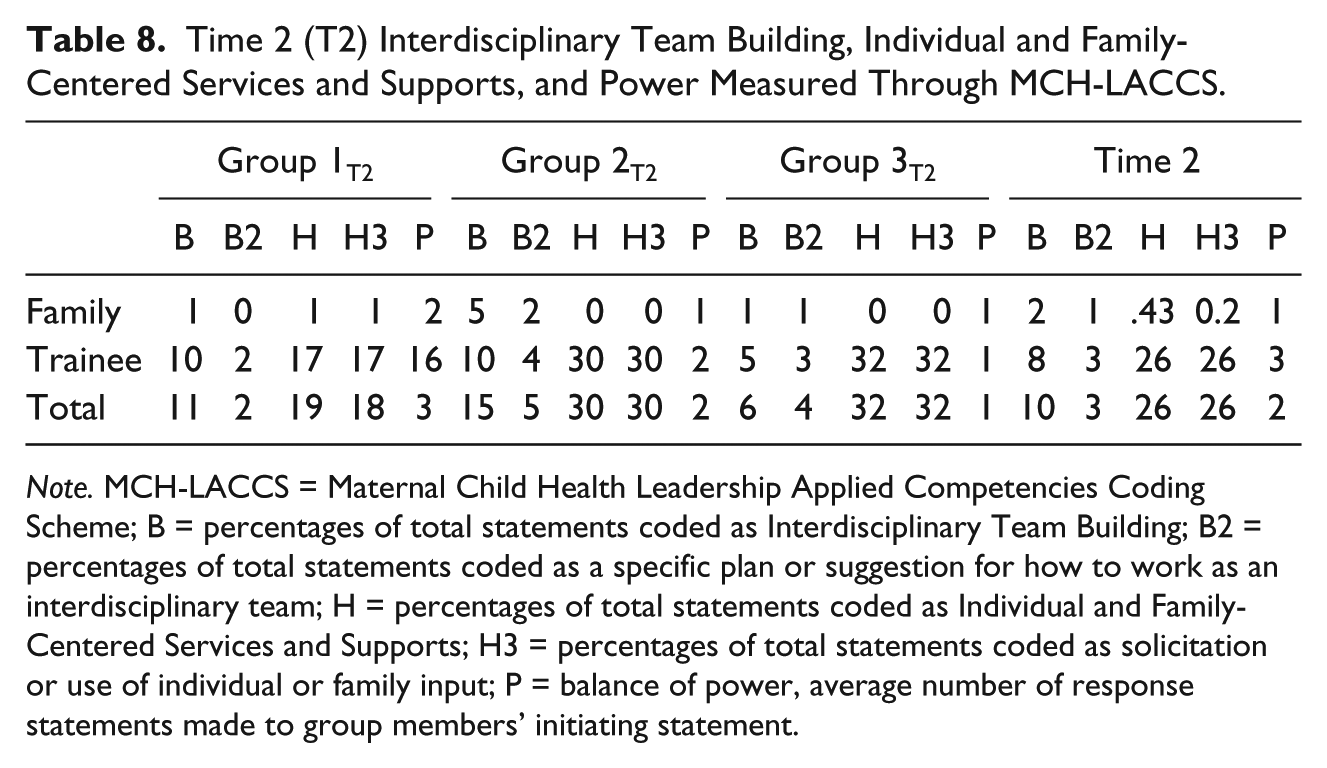
Note. MCH-LACCS = Maternal Child Health Leadership Applied Competencies Coding Scheme; B = percentages of total statements coded as Interdisciplinary Team Building; B2 = percentages of total statements coded as a specific plan or suggestion for how to work as an interdisciplinary team; H = percentages of total statements coded as Individual and Family-Centered Services and Supports; H3 = percentages of total statements coded as solicitation or use of individual or family input; P = balance of power, average number of response statements made to group members’ initiating statement.
Overall, from T1 to T2, balance of power decreased for family (from 8 to 1) while increasing only slightly for trainees (from 2 to 3). These data suggest that family members were responded to less often at T2. Estimates of balance of power are reported in Tables 7 and 8.
Discussion
Through this exploratory study, we sought to learn more about the communication patterns between families and professionals in interdisciplinary team meetings. Specifically, we applied three communication coding schemes to a CBS activity within interdisciplinary teams that included trainees in the role of professionals and trainees in the role of family members to measure language similarity, balance of power, and competency-based problem solving. These constructs were chosen due to the literature suggesting that families feel excluded from team meetings in which jargon is heavily used (Valle, 2011). Also, difficulty understanding the technical language and other team dynamics can lead to an imbalance of power (Kummerer & Lopez-Reyna, 2009) that interferes with the collaborative problem-solving process (Valle, 2011). While effective communication is a critical component of interdisciplinary practice and family-centered care, we do not have enough data examining the dynamics of the communication between families of individuals with disabilities and SHCN and the other team members in problem-solving meetings despite decades of initiatives (Johnson, 2002). The current study was largely exploratory but attempted to fill these gaps by making two unique contributions to the literature. First, to our knowledge, this study is one of the first that used the sophisticated process of applying three different coding schemes to measure language similarity, balance of power, and competency-based problem solving in simulated interdisciplinary team problem-solving conversations that included family members. Second, to our knowledge, this study was among the first to explore changes in these constructs over time.
The results suggested that as a group, trainees had a higher level of domineeringness (attempts to control the conversation) than family participants at both T1 and T2. At T2, trainees increased in dominance (successful attempts at controlling the conversation) and family participants decreased in dominance. In other words, trainees became more effective at controlling the conversation while family participants became less effective at controlling the conversation. Through application of the MCH-LACCS coding scheme, trainees increased their solicitation and use of family participant input at T2; however, interdisciplinary team building and responses to families’ initiating comments decreased. At T2, trainees directed more closed-ended questions to family participants, which may have reduced the back-and-forth conversation between team members and may have reduced the families’ opportunities to guide the conversation. Overall, trainees controlled the interdisciplinary team problem-solving conversation at T1 and T2. Although the dynamics of the conversation changed from T1 and T2, it was not necessarily in the direction of balanced power and communication between the trainees and family participants. Due to the exploratory nature of the study, we are cautious in over extending the implications of the results of the study, yet the results suggest that trends do exist in communication patterns in interdisciplinary team meetings that include family members. These trends relate to the critical constructs of similarity in language, power/dominance/domineeringness, and competency-based problem solving, and are worthy of further research.
Limitations and Future Directions
The current study employed a unique qualitative methodology that included applying three communication coding schemes to CBS activities at two time points. Despite the use of this sophisticated methodology, the current study was exploratory and had several limitations. First, despite knowing more about similarity in language, power/dominance/domineeringness, and competency-based problem-solving components present in the CBS conversations, we have limited knowledge about the quality of the conversations. Future research should examine the quality of the interdisciplinary conversations by measuring participant satisfaction post-activity. A related research question may be, “What level of language similarity and power balance are predictive of high family satisfaction in team meetings with families and professionals?” Additional outcome variables could be assessed against the communication coding scheme data, such as team productivity, which could be assessed by measuring the quality of the treatment plans developed by the interdisciplinary teams. Second, there are limitations that are inherent to a CBS. For example, the individuals playing the family members were former LEND trainees and were familiar with the LEND curriculum and its emphasis on family-centered care. Although the former trainees were trained on their role of family member, it is unknown what effect their role as former trainee may have had on the results. Future research could use community members as family members to control for the potential effect that knowledge of the LEND program may have had on the former trainees’ participation in the team meetings. Third, in the literature, families have reported that the existence of pre-meetings attended by only clinicians/educators may contribute to the family feeling excluded from the decision-making process. The influence of this pre-meeting on family perceptions could be compared with the influence of in-meeting dynamics on family perceptions to further understand construct of imbalance of power between these groups. Fourth, the small sample size limited our ability to test for statistically significant change between T1 and T2. Larger studies, with a comparison group, will strengthen the initial conclusions drawn through this exploratory study. Finally, future research should continue to explore skills important for family-centered, interdisciplinary team meetings so that leadership training programs may have more empirical literature upon which to develop training activities related to interdisciplinary team problem solving and family-centered care.
Footnotes
Authors’ Note
The information or content and conclusions are those of the authors and should not be construed as the official position or policy of, nor should any endorsements be inferred by Health Resources and Services Administration (HRSA), U.S. Department of Health and Human Services (HHS), or the U.S. Government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The development of the LEND evaluation and this article were supported in part by Project T73MC19939 from the Maternal and Child Health Bureau (Public Health Service Act, Section 399BB (e)(1)(A), as amended by the Combating Autism Act of 2006) of the Health Resources and Services Administration (USDHHS) and by Grant 90DD0662 from the Administration on Intellectual and Developmental Disabilities of the Administration on Community Living (USDHHS).