
Abstract
Background.
Commercial
Methods.
Pre-test/post-test research design and qualitative questions were used to measure the impact of an
Results.
Data from the analysis of the pre and post observations of
Conclusion.
This pilot study sets the foundation for future use and exploration of
Background
Nurses are responsible for providing safe, high-quality care within increasingly complex and challenging health care settings. Today, health care calls for healthcare providers who are equipped with strong leadership, teamwork, and communication skills. Nurses have a vital role to play in improving healthcare and mitigating adverse events. However, to be part of the solution of making health care safer, nurses need the appropriate skill set. Medical errors are estimated to account for more than 440,000 deaths in the United States (U.S.) yearly (Makary, 2016). While controversy over the exact incidence rate of medical errors continues, poor communication among health care providers and ineffective leadership have been identified as significant contributing factors in the commission of errors (Agency for Healthcare Research And Quality [AHRQ], 2019a; Nether, 2017). Teamwork and collaboration are core competencies identified by the Quality and Safety Education for Nurses (QSEN) initiative considered essential in the provision of safe high-quality care for pre-licensure and graduate nursing students (QSEN, 2003). To actively prepare future nurses to work in safe, quality-driven practice environment, there is a need for curricula designed to increase confidence and competences to work in teams, utilize effective communication, and display leadership skills. Learning opportunities that encompass communication, teamwork, and leadership skills should be incorporated into nursing pre-and post licensure programs (The American Association of Colleges of Nursing, 2008; Cronenwett et al., 2007).
The use of a variety of non-traditional teaching strategies are found in nursing education literature, including gaming, problem-based learning, flipped classroom, and simulation. Nursing education has employed the use of simulated learning environments to actively engage students in the transference of knowledge (Robinson & Dearmon, 2013; Freeman et al., 2014). Escape room experiences incorporate simulation and gaming principles that actively engage participants in collaborative efforts to find and analyze data in order to solve a puzzle or dilemma. The aim of this pilot study was to evaluate the use of an escape room as an innovative educational method to promote leadership, teamwork, communication, and delegation skills in RN-BSN nursing students.
Introduction to the Scenarios
Participants completed a baseline and post escape room clinical-based simulation activity and an escape room activity. The participants were evaluated using the University of Miami Crisis Resource Management (UM-CRM) tool for each of the three encounters. The UM-CRM tool is an adaptation of the Ottawa CRM tool, which measures observed behaviors in the areas of teamwork, communication, leadership, situational awareness, resource management, and delegation (Kim, et al, 2009). Before and after the escape room activity, participants were asked to anonymously complete a demographic questionnaire, as well as the TeamSTEPPS® [Team Strategies and Tools to Enhance Performance and Patient Safety] Teamwork Attitudes Questionnaire [T-TAQ], and four self-reflective qualitative questions.
The objectives of all scenarios were: (1) discuss the principles of team communication, shared mental model, and closed-loop communication, (2) verbalize a list of differential diagnoses and differences in clinical management, (3) identify the resources available for emergencies, and (4) demonstrate positive team dynamics to accomplish the goal of patient care. Prior to the baseline clinical simulation, students were pre-briefed, including explanation of the purpose of simulation, discussion of safe environment, and introduction to the high-fidelity manikin and simulation setting. In regards to the clinical-based simulated activity, establishment of realism was discussed. The students were divided into groups of five for the pre- and post-clinical simulation encounters but participated in the escape room experience as a single group of 10. Participants were instructed that they would have 60 minutes to complete the escape room activity.
The Flow of the Escape Room
A non-clinical commercial establishment was contracted to run the escape room activity. Even though the escape room activity theme was based on Sherlock Holmes, students were observed using the UM-CRM Tool. While students had 60 minutes to solve six activities involving puzzles, riddles, cues, locked boxes, and finding the escape key, they were scored in regard to teamwork, communication, leadership, situational awareness, resource management, and delegation. The puzzle pieces were randomly hidden throughout the escape room, which required students to scavenge for attainment of all pieces prior to solving the puzzle. Some riddles involved the use of pictures to solve a number scramble puzzle, which decoded a locked box.
Equipment
The clinical-based simulation room was set up as a two-patient room in a hospital ward with standard equipment, including, hospital beds, curtains, oxygen access, intravenous pumps, patient-controlled analgesia pumps, cardiac monitors, emergency cart, and emergency call button. The room had additional props, such as stethoscopes, patient charts, incentive spirometer, and dressing supplies. A high-fidelity manikin and standardized patient (SP) were employed for the previously validated clinical-based simulated activities. Each team simulation activity lasted eight minutes, and debriefing of the simulation activity was based on identified objectives.
The escape room activity involved the use of holographic puzzles, which had missing pieces hidden in furniture (roll-top desk, bookshelves, curio cabinet, and ottoman) and books, behind picture frames, and under area rugs and wooden candlesticks. These puzzle pieces unlocked a box that contained a magnifying glass, which was intended to be used to read a coordinate in small print on a map. Participants were required to use pictorial riddles to successfully solve a common phrase, which had letters highlighted to correspond with the numbers needed to open the second and final locked box. The last locked box contained a black light, which detected fluoresces from the ink depicted on a wall illustrating the escape room exit key.
Five constructs: communication, team structure, mutual support, situational monitoring and leadership were collected utilizing the TeamSTEPPS® T-TAQ survey (Marguet & Ogaz, 2019; AHRQ, 2017; AHRQ, 2019b). The 30-item TeamSTEPPS ® T-TAQ questionnaire rates participant agreement using a 5-point Likert-scale summation instrument with scores ranging from 0 to 150 and has a reported Cronbach’s alpha ranging from 0.70 to 0.83 with respondents of the healthcare population (AHRQ, 2019b). Participants’ perception of effective communication, team structure, mutual support, situational monitoring and leadership are seen with higher scores. Appendix A provides the TeamSTEPPS ® T-TAQ.
The 13-item UM-CRM tool uses a 3-point Likert-scale summation instrument with scores ranging from 0 to 26 with a reported Cronbach’s alpha of .88 with a population of 190 healthcare students (Sanko et al., 2015). Higher scores indicate team proficiency with problem solving, situational awareness, resource utilization, communication, and leadership skills. Appendix B provides the UM-CRM tool.
Eight questions were administered to participants regarding self-reported levels of confidence and competence in the areas of teamwork, communication, leadership, delegation, and resource management. The questions used a 10-point Likert scale with scores ranging from 0 (not at all confident/competent) to 10 (completely confident/competent). There is no reported reliability with these questions, as this tool is a new adaptation of a medication administration confidence and competence tool (Sanko & Mckay, 2017). The original tool was evaluated in an undergraduate nursing population and found to have good demonstration of reliability with (α = .90, all item-total correlations >0.30) Appendix C provides the Self-Reported Levels of Confidence and Competence tool.
Four open-ended qualitative self-reflective questions were asked following the escape room. Every question started with the prefix, “Following the escape room experience, what did you learn in terms of…” The stems of each of the four questions were, respectively: “communicating within a team, leadership/delegation, situational awareness, and availability of resources.”
Outcomes
A total of 10 RN-BSN students who were full-time employed, female, and Hispanic, with reported ages ranging from 25 to 64 participated. Participants reported from 3 to 25 years of practice as registered nurses. Only three participants answered both the pre-post confidence/competence and T-TAQ surveys. Data were analyzed using SPSS version 25 (International Business Machines Corporation, 2017). Paired t-tests were used to analyze pre-post data from the T-TAQ, the confidence and competence measure, and the observational data collected using the UM-CRM tool.
Analysis of the data examining teamwork attitudes collected using the T-TAQ (n = 3) demonstrated time dependent improvements in the following sub-scales of the T-TAQ: Leadership (0.33 mean change), communication (0.34 mean change), and situation monitoring (1.0 mean change). Team structure was identical both pre and post intervention. Mutual support mean values decreased from pre to post intervention (4.0 mean change). No results reached the level of statistical significance.
Data from the analysis of the pre and post observations of simulation encounters demonstrated no differences in the group scores pre or post encounter (p = 0.926). Time-dependent differences demonstrated marked statistically significant improvements in observed teamwork and leadership, p <.001, pre-mean 18.5, post-mean 35.0 when comparing the pre escape room observations with the post escape room observations. Inter-rater reliability had 100% agreement among the three raters.
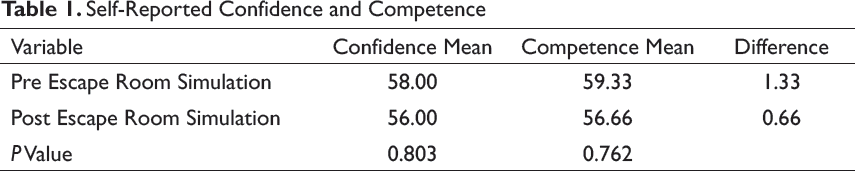
Analysis of data examining changes in feelings of teamwork confidence and competence (n = 3) demonstrated decreases in feelings of teamwork confidence and competence, but were not found to be statistically significant (Table 1). Decreases in feelings of confidence and competences mimic other studies looking at confidence and competence as an outcome measure and simulation as an intervention/tool for observation (Sanko & McKay, 2017)
Self-Reported Confidence and Competence
The qualitative data demonstrated that participants enjoyed the experience and found the escape room to be a fun and rewarding way to learn and hone leadership and teamwork skills. Participants noted the value of delegation and leadership: “It is important to know what we are doing, so we can delegate and choose a leader… there almost always needs to be a team leader who delegates in order to complete a task more efficiently” (Participant 3). In terms of the importance of situational awareness, participants recognized the importance of seeing the big picture and having situational awareness to solve problems most effectively: “…to be able to look at every aspect of the room from a distance to be able to understand the bigger picture” (Participant 5). Finally, the escape room succeeded in teaching participants the benefits of utilizing resources:
… resources are of most importance; many times in life we struggle through life and don’t tap on [sic] available resources that will facilitate our work. In the escape room experience, we could have made use of available resources to solve the puzzles faster…to better utilize [sic] the resources available, better distribution of people and better use of time could have been established if we communicated at the beginning of the activity (Participant 1).
Even though 10 students were enrolled in this pilot study, only three completed all measures; therefore, a limitation of the study is the small convenience sample and the lack of a control group, which hinders the ability to generalize the findings (Salkind, 2013). Traditionally, nursing students were accustomed to participating in simulation activities in groups of two to three people; however, the escape room activity involved participants to be in a group of 10. Due to different sized groups with potential for less interaction and a tendency to align with colleagues’ average performance, the results from the escape room activity may have been affected. Another limitation of the study is not having collected data on prior commercial escape room experiences, which would have identified those participants with increasing expertise in similar environments. The self-reported level of confidence and competence research instrument is another potential limitation of the study as this instrument was developed for use in this study and has not been previously used within this population. Lastly, although participation in this study was voluntary and the students’ course grades were not affected, perceived pressure to answer questions and the videotaping of the clinical-based scenarios (even though this is usual practice for all simulation encounters) may have contributed to another potential limitation of the study.
Future Applications
This pilot study sets the foundation for future use and exploration of escape room experiences to teach teamwork, communication, leadership and situational awareness. Study findings suggest that the use of an escape room is an effective way to impart the critical skills needed to work as a collaborative member of a team. Moreover, the use of an escape room and subsequent clinically based simulation allowed for an educational system where students could experience making mistakes, followed by the opportunity to put learned skills into practice in a new scenario.
Although this pilot study did not yield large enough sample sizes to sufficiently power the study, it informs the educational community about how escape rooms can be used and evaluated in education. The findings do give insight into the potential effectiveness of such an educational approach. In the current landscape of educating the digital native learners that are accustomed to fast-paced information and interactive modalities of learning, tactics like escape rooms, simulation, and gaming may be the wave of the future. This study also provided the authors with a way to pilot an escape room in a simulation framework that can be used for different purposes, such as training inter-professional teams, and developing critical thinking and problem-solving skills.
Further, the study allowed us to explore of the use of an escape room for assessing teamwork, leadership, and communication skills on a small scale, the aim being to test concept feasibility prior to launching a full-scale production of the concept. For this study, we employed the use of a commercial escape room space, rather than incurring the expense of creating our own. Given the program’s relative success and the study’s promising findings, we are now exploring the potential for creating an escape room of our own for educational purposes.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material for The Impact of an Escape Room Simulation to Improve Nursing Teamwork, Leadership and Communication Skills: A Pilot Project by Beatriz Valdes, Mary Mckay, Jill S. Sanko, in Simulation & Gaming
Footnotes
Declaration of Conflicting Interests
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Authors’ Biographies
Contact:
Contact:
Contact:
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.