
Abstract
With the upcoming release of the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-V) there has been a necessary critique of the DSM-IV including questions regarding how to best improve the next iteration of the DSM classification system. The aim of this article is to provide commentary on the probable direction the DSM-V is headed with regard to panic attacks, panic disorder (PD), and agoraphobia (AG). The DSM-V Work Group’s recommendations for panic attacks, PD, and AG are reviewed, and important diagnostic questions and concerns are raised. Future research directions are discussed that will hopefully help improve our understanding of anxiety and our ability to accurately diagnose and classify these conditions.
The Diagnostic and Statistical Manual of Mental Disorders (DSM) provides the standardized classification system of psychiatric disorders used in the United States. Produced by the American Psychiatric Association, the DSM nosology allows researchers and mental health professionals to communicate quickly and effectively about the nature of an individual’s psychopathology. Scheduled for release in May of 2013, the next iteration of the DSM, the DSM-V, has been highly anticipated due to potentially significant changes to the classification structure and specific diagnostic criteria of certain mental disorders. The focus of this article is to discuss potential changes for panic disorder (PD) and agoraphobia (AG) in the DSM-V. At the time of this writing the revisions for PD and AG have not been finalized, however, there are clear indications as to where the DSM-V is headed. Specifically, summary documents have been published detailing the proposed changes made by the DSM-V Work Groups on PD (Craske et al., 2010) and AG (Wittchen, Gloster, Beesdo-Baum, Fava, & Craske, 2010). Although no field trials have been published on the proposed criteria, these reports will allow us to comment on the recommendations and likely changes for DSM-V PD and AG. Moreover, the issues raised by the Work Groups highlight some of the major contemporary controversies with regard to these diagnoses.
Background
Anxiety can be an adaptive mechanism, as it prepares humans for action and readies them to protect themselves from anticipated threat. However, this “alarm system” can be detrimental when it is triggered for no apparent reason, when it is triggered in situations that are known to be safe, and when it is activated for extended periods of time. One result of a malfunctioning “alarm system” is panic, or an intense emotional arousal. In some cases, this fight or flight response can result in an overwhelming emotional experience called a panic attack. According to the Diagnostic and Statistical Manual of Mental Disorders, fourth edition, text revision (DSM-IV-TR; American Psychiatric Association [APA], 2000), a panic attack is defined as a discrete period of intense fear or discomfort during which an individual experiences four or more somatic and/or cognitive symptoms (e.g., racing heart, fear of losing control). Although individuals across many psychiatric disorders experience panic attacks, panic is only diagnostically tied to PD and AG.
Affecting approximately 2–3% of the adult population at any given time, PD is an anxiety condition that has been intensively investigated (Grant et al., 2006; Kessler et al., 2006). According to the DSM-IV-TR (APA, 2000), the essential feature of PD is recurrent, unexpected panic attacks accompanied by significant panic-related worry and/or behavioral avoidance. Panic-related worry can be focused on fears of having additional panic attacks (e.g., “Will I panic at work today?” “If I go to the supermarket will I panic?”) or consequences of the panic per se (e.g., “If I panic I will have a heart attack” “If I panic I will lose control”). Behavioral change resulting from fears of panic can manifest in avoidance of places or activities that the individual feels will result in panic (e.g., supermarkets, movie theaters, vigorous exercise). Importantly, the experience of panic attacks cannot be the direct physiological result of a substance (e.g., caffeine, medication) or a general medical condition (e.g., hyperthyroidism). For many individuals, PD is an incapacitating condition that results in significant social, occupational, and functional impairment (Barlow, 2002; Bystritsky et al., 2010; Klerman, Weissman, Ouellette, Johnson, & Greenwald, 1991).
Closely linked to PD is the diagnosis of AG. AG is defined as the experience of marked distress in or avoidance of situations in which an individual fears they may experience a panic attack or panic-like symptoms (e.g., dizziness, diarrhea; APA, 2000). Currently, AG is not classified as a separate codable disorder, but rather is used as a specifier in the context of PD (e.g., PD with or without AG). However, a diagnosis of “agoraphobia without history of panic disorder” can be given in the event of a patient who experiences significant impairment related to AG, but has never met the full criteria for a PD diagnosis. PD with AG is the less common manifestation of PD. Epidemiological studies have found 12-month prevalence rates for PD without AG and PD with AG to be around 1.6% and 0.6%, respectively (Grant et al., 2006; Kessler et al., 2006). Individuals diagnosed with PD with AG have greater impairment as compared to those with PD without AG or AG without history of PD. Specifically, these individuals have higher levels of issues with role functioning, work productivity, disability, and disability days taken off from work (Andrews & Slade, 2002; Wittchen et al., 2008).
DSM-V—Likely Revisions and Diagnostic Considerations
Panic Attacks
Based on the information coming from the DSM-V Work Group, it appears there will be minimal suggested revisions to the DSM-IV-TR criteria for panic attacks. Between the Diagnostic and Statistical Manual of Mental Disorders, third edition (DSM-III-R; APA, 1987) and the DSM-IV, there were two major changes in how we classify panic attacks. The first change was that panic attacks were moved to the beginning of the anxiety disorders section rather than being diagnosed within the context of PD. This was done to, correctly, indicate that panic attacks are seen in patients across all anxiety disorder diagnoses, not just in PD patients. The addition of panic attack specifiers (spontaneous, situationally disposed, or situationally bound) to identify the predictability of the panic attacks constituted the second major diagnostic change. The spontaneous specifier is given when the occurrence of panic attacks is completely unpredictable. Panic attacks that are more predictable are designated as situationally bound or situationally predisposed depending if they are occurring automatically or regularly in the context of certain cues. The work group notes, however, that since the publication of the DSM-IV there has been relatively little research examining these two major changes. This unfortunately means that the most substantive changes to the panic attack criteria since the Diagnostic and Statistical Manual of Mental Disorders, third edition, revised (DSM-III-R) have unclear empirical support.
With regard to the isolation of panic attacks at the beginning of the anxiety disorders section, the work group raises the question of whether the presence of panic attacks should be included as a specifier across all anxiety disorders. We feel that this is very reasonable as the DSM-IV does not make it clear what the diagnostic role of panic attacks should be. It appears the isolation of panic attacks in the DSM-IV is simply serving as a reminder to clinicians that panic occurs in a wide array of patients, but there is no indication that certain conditions should be diagnosed with a panic attack specifier (e.g., obsessive-compulsive disorder [OCD] with or without panic attacks). Therefore, the DSM-IV presentation of panic attacks is contradictory. On one hand, clinicians are supposed to keep in mind that panic attacks could occur within the context of any anxiety disorder, however, they are not required to include a diagnosis of panic outside of PD and AG. It seems that clinicians should either be required to specify the presence of panic attacks for other anxiety diagnoses, or the diagnosis of panic attacks should be returned to the PD and AG sections.
The Work Group suggests that the specification of panic may be useful in conveying important information about the nature, severity, or response to treatment of anxiety disorders. Despite the utility of such a heuristic, the research available to the Work Group was too limited in scope to allow it to reach solid conclusions. The chief concern is that the majority of research related to panic has focused on PD. This is not surprising given that, as mentioned above, the diagnosis of panic is only formally recognized within the context of PD. Still, there are several studies which have shown panic attacks to be predictive of a range of anxiety disorders apart from PD, as well as nonanxiety conditions such as mood and substance use disorders (Bernstein, Zvolensky, Sachs-Ericsson, Schmidt, & Bonn-Miller, 2006; Goodwin & Gotlib, 2004). Unfortunately, this information is not particularly relevant to the issue of whether panic should be used as a diagnostic specifier. To make that determination, we would need to examine a range of anxiety disorder patients with and without panic attacks, and these data do not appear to be available. Regardless of these potential issues, the Work Group feels that panic attacks can provide useful information so it is not proposing any changes.
Separate from the issue of the overall utility of diagnosing panic attacks, the Work Group also considered three issues involving: (1) the temporal requirement for the “peaking” of panic attack symptoms within 10 min, (2) the viability of the 13 current endorsable panic symptoms, (3) the cutoff for a full panic attack being the experience of at least four of these symptoms (Boulenger, Uhde, Wolff, & Post, 1984). The temporal criterion, that the panic symptoms must peak within 10 min, was the final panic attack issue examined in depth by the Work Group. The purpose for the inclusion of this criterion in the DSM is to discriminate between anxiety, which is often quite high in patients with these conditions and can be enduring, and panic, which is typically viewed as a discrete event. The literature in this area shows a clear disagreement between studies that monitor physiological measures of arousal and those that rely on self-report data. Studies that directly assess physiology show clear and distinct physiological peaks during panic attacks that are distinct from anxiety (Cohen, Barlow, & Blanchard, 1985). There is less clarity in studies using self-report symptoms, with some reports suggesting that only a minority of panic attacks are experienced with a clear surge of symptoms (Essau, Conradt, & Petermann, 1999). However, it is reasonable to assume that these differences are due to problems associated with retrospective self-reports as well as difficulties associated with pulling apart individual levels of subjective distress. For example, many patients with PD experience a comparably high level of baseline anxiety that can build further until the onset of full panic. Therefore, the Work Group has recommended that the DSM-V include graphical depictions of subjective intensity, demonstrating how panic can result from either calm or anxious states. These graphical depictions will consist of four graphs demonstrating the level of distress before, during, and after the panic attack. The four graphs will display: (1) a panic attack beginning and ending in a calm state, (2) a panic attack beginning in a calm state and ending in an anxious state, (3) a panic attack starting in an anxious state and ending in a calm state, and (4) a series of panic attacks where the first attack starts in a calm state and ends in an anxious state, and a second attack that starts in an anxious state and ends in a calm state. Such graphical depictions will presumably lead to more valid and reliable reports of panic attacks as opposed to intense feelings of anxiety.
Although the recommendation to include graphic depictions of panic seems reasonable and may lead to increased diagnostic reliability, the untested nature of this methodology makes it unclear how it may affect diagnoses. Furthermore, this recommendation does not directly address the issue of whether the endorsement of “discrete panic” is an important contributor to the diagnosis of panic attacks. Researchers that investigated this question reported that there were no overall differences between patients who do or do not endorse clear, discrete panic peaks (Scupi, Benson, Brown, & Uhde, 1997). It could be stated that the difference between these patient groups is that one has a clear fear of panic while the other presumably has a fear of anxiety. Determining whether these two groups are in fact indistinct is an important endeavor, as it would suggest that the fear of panic per se should be replaced with a more all-encompassing fear of anxiety or panic that would lack the characteristic discreteness seen in previous versions of the DSM.
The 13 panic attack symptoms listed in the DSM are highly weighted toward symptoms that are cardiorespiratory in nature, such as shortness of breath and rapid heart rate. Furthermore, dizziness, derealization, and tingling might also be considered respiratory symptoms, as they result from hyperventilation. Additionally, there are two “cognitive” symptoms of panic listed in the DSM: fear of losing control or going crazy and fear of dying. The literature review has shown that all these symptoms of panic occur in both community and patient samples with enough consistency to justify their inclusion in the DSM. However, the literature review also highlights the lack of research addressing the questions of whether certain symptoms are more powerful in predicting the diagnosis of panic. In one study, utilizing item response theory (IRT), researchers found that certain panic symptoms were useful in predicting the severity of panic, which suggests that this may be an area that future research should address (Ietsugu, Sukigara, & Furukawa, 2007). Since there is a clear distinction between the cognitive appraisal symptoms and the physiological symptoms of panic, it is curious that the Work Group did not consider further evaluating the value of these two types of symptoms with regard to their role in the diagnosis of panic attacks. It appears that the cognitive appraisal symptoms are more closely linked with PD, where patients often fear both physical and cognitive catastrophe will result from panic. As the diagnosis of panic attacks was removed from the PD section in the DSM-IV, it seems possible that the two cognitive symptoms are simply left over, as they may have been more useful in diagnosis PD rather than making a diagnosis of panic per se.
According to the DSM-IV, panic attacks can only be diagnosed when 4 or more of the 13 panic symptoms cooccur within a single episode. When patients report panic attacks with fewer than four symptoms, they are commonly referred to as limited symptom attacks. Consistent with the other issues discussed in this section, the Work Group found a dearth of studies that sought to ascertain whether the four symptom cutoff was optimal in the diagnosis of panic attacks. The literature suggests that in the assessment of panic attack symptoms (typically the worst panic attack experienced) only approximately half the panic attacks met the four symptom cutoff (Craske et al., 2010). This information seems to suggest that full symptom panic attacks are not the norm and may in fact be atypical, though their identification may still provide utility as research suggests that the overall severity of panic symptoms predicts important outcomes. For example, increased likelihood of inpatient admission and increased risk for suicide attempts have been associated with the number of panic attack symptoms experienced (Horwath, Wolk, Leon, & al., 1998).
Currently, the four symptom threshold appears to be both an arbitrary and underresearched criterion. The plausibility of a four symptom cutoff is supported by at least one receiver operator curve analysis that found a three symptom cutoff to be optimal, with a four symptom cutoff achieving comparable sensitivity and specificity (Craske et al., 2010). A necessary area of future work is to determine whether the current panic symptoms are adequately weighted. There is a heavy emphasis given to cardiorespiratory symptoms, as 6 of the 11 current physical panic symptoms are either cardiovascular or respiratory in nature. Given this emphasis on the cardiorespiratory arousal in panic, it seems empirical work is needed to determine whether it is reasonable to have multiple criteria/symptoms tapping into this singular domain. For example, these six symptoms could be collapsed into one criterion entitled “cardiopulmonary arousal” symptoms. On the other hand, it is also plausible that the DSM does not go far enough in weighting the importance of certain panic symptoms. For example, some etiological models suggest certain symptoms would be expected to be more critical than others, such as dyspnea (Schmidt, Telch, & Jaimez, 1996). A variety of methodological and statistical approaches could be used to determine whether this criterion, a different categorical threshold, or a dimensional approach would be the most suitable in the long run.
On the surface, it may seem that a lack of recommended changes for DSM-V would signify that we have achieved considerable clarity about the diagnostic issues surrounding panic. However, it seems that a deeper understanding reveals that the research findings reviewed by the Work Group are somewhat disappointing. The inertia with respect to panic attacks in the DSM appears to be rooted in the fact that panic per se has received relatively little attention in the empirical literature, as compared to PD. In all fairness, there are probably a number of contributing factors to this lack of data. One key issue that appears to be limiting the research on panic attacks is that panic attacks, as a clinical phenomenon, are not an independent, diagnosable condition. Moreover, panic is not required to be considered (or for that matter at all involved) in the diagnosis of most clinical conditions, with the sole exceptions being PD and AG.
In terms of empirical support for considering panic outside of any specific anxiety diagnosis, we know very little about how panic presents differentially across the numerous clinical conditions where it may be present. The assumption appears to be that panic will be expressed uniformly regardless of the anxiety disorder with which it is associated. On the other hand, the heterogeneity of panic attacks suggests that panic in the context of PD may differ substantially from panic in Social Phobia, GAD, and other conditions. Additionally, the impact panic attacks have on the course, severity and treatment of anxiety disorders has not been fully elucidated. Until we know more about panic attacks across the different disorders, we must conclude that little significant progress has been made on establishing the substantive diagnostic changes in the criteria for panic attacks. In summary, the lack of novel panic research is reflected in the lack of recommended changes by the Work Group.
Panic Disorder
Compared to considering issues related to panic attacks and AG, the Work Group spent considerably less time evaluating issues pertaining to PD. There were two primary requirements for a diagnosis of PD that the Work Group considered including the necessity of: (1) two or more unexpected panic attacks and (2) 1 month of panic-related worry. These are reasonable issues to evaluate as both criteria were altered between the DSM-III-R and the DSM-IV. The decision to change the threshold from four or more panic attacks (DSM-III-R) to the DSM-IV “recurrent” (two or more) panic attacks requirement was based on data suggesting that patients can experience clinically significant impairment, including hospitalization, after as few as one or two panic attacks (Horwath et al., 1998). However, as noted by the Work Group, there has been minimal research since the release of the DSM-IV on this issue. Therefore, it is quite possible that the recurrence threshold is either too high or too low, but there is simply not sufficient empirical evidence to make a recommended change to this criterion.
In addition to recurrent panic attacks, a diagnosis of PD is only warranted when the panic attacks are unexpected. The notion of unexpected, or “spontaneous” panic attacks was added to the DSM-IV as a method to differentiate PD from other anxiety conditions in which patients experience panic attacks that are “bound” to certain situations or cues. Unfortunately, the notion of unexpected or spontaneous panic is problematic. Primarily, it seems unrealistic that someone who has never experienced panic could truly anticipate such an experience. Therefore, even if an individual is anticipating significant anxiety or stress in a given situation, a full-blown panic attack would be very likely unanticipated. In other words, with regard to a first panic attack, how could it be anything other than unexpected?
A second issue is that after the first experience of panic, an individual should seemingly have an increased ability to anticipate additional panic attacks, particularly when placed in a similar situation to when they had previously experienced panic. The ability to effectively anticipate panic would appear to be based on a number of factors, but one seemingly important issue is that person’s ability to correctly identify cues related to the initial panic attack. For example, someone may experience their first panic attack at: (a) a social gathering, (b) when they were feeling sick, and (c) drinking alcohol after (d) a particularly stressful day at work. Imagine that this same individual experiences a panic attack after a couple of weeks at another social gathering. Some people would have attributed the initial panic attack to feeling sick and drinking alcohol, and therefore would not have anticipated experiencing another panic attack when there were not sick. However, other people might attribute the initial panic attack to the social function, and therefore would be more likely to indicate the second panic attack was more expected. Thus, we have the somewhat arbitrary association of panic with certain initial cues (social situation vs. illness) resulting in a second panic experience being diagnosed as cued or spontaneous.
Another factor that may contribute to the diagnosis of spontaneous versus cued panic has to do with interoceptive accuracy. Some researchers have suggested that panic attacks result from conditioning of internal bodily sensations (Bouton, Mineka, & Barlow, 2001). In line with interoceptively conditioned panic, we would suggest that individuals who are more sensitive to and aware of their internal bodily states would be more likely to associate the initial panic attack with the experience of a particular physiological symptom. As a result, we would argue that significant individual differences are likely to contribute to an individual’s ability to correctly identify panic attacks as anticipated or not. Obviously, our assertions are somewhat speculative but they highlight significant limitations in the diagnostic requirements for ascertaining the so-called spontaneous nature of panic attacks.
In addition to the experience of spontaneous panic attacks, patients with PD can experience situationally disposed or cued panic attacks (Kessler et al., 2006). Furthermore, the vast majority of patients with PD and AG report experiencing cued panic attacks (Kessler et al., 2006). As one of the core features of PD is the development of a fear of panic attacks, it begs the question of whether experiencing recurrent spontaneous panic attacks is necessary to develop such a fear. Certainly uncued panic attacks are more characteristic of PD patients than other anxiety disorder patients; however, it seems that intense physiological arousal is sufficient for the development and maintenance of panic-related worry, making the specific type of panic (cued vs. uncued) irrelevant. Based on the lack of empirical literature, we are left without satisfactory answers regarding the type of panic needed (spontaneous) and minimum frequency of panic attacks required to suggest appropriate changes to the diagnostic structure for PD.
According to cognitive models of panic, the single most defining issue in the diagnosis of PD is the DSM-IV criterion of panic-related worry (Clark, 1986). In the DSM, worry can be conceptualized in two ways. The individual can clearly endorse panic-related worry or that person could display a significant behavioral change due to the panic (presumably due to panic-related worry). Technically, panic-related worry in the DSM-IV can be indicated by either of the two subcriteria: (1) worry about having additional panic or (2) worry about the consequences of having a panic attack. In regard to panic-related worry, the DSM-V Work Group focused on the apparent redundancy of Subcriteria 1 and 2. Citing unpublished data, the Work Group discussed that worry about additional panic and worry about panic-related consequences are highly correlated (Craske et al., 2010). We agree that it would be difficult to imagine a scenario in which fear of additional panic and fear of panic-related consequences (e.g., panic resulting in a heart attack) would not be related. However, there are plenty of patients with PD who fail to identify a specific panic-related consequence during an intake interview. Often, this happens in patients who have experienced panic for an extended period of time. It is not necessarily true that these individuals do not have any fears of panic-related consequences; it is simply that over time, the panic itself has become the focus of their concerns and is more salient than the panic-related consequences. Therefore, we believe that the Work Group correctly suggested, in an effort to reduce redundancy, the consolidation of these two subcriteria, such that fears of having additional panic attacks and fears of panic-related consequences would be combined into a singular cognitive criterion of panic-related worry.
In the absence of panic-related worry, PD can still be diagnosed if the development of panic-related avoidance behaviors is significant. It is true that patients with PD demonstrate avoidance behaviors in an effort to reduce the risk of future panic attacks. However, as the Work Group points out, this criterion and the diagnostic criteria for the AG specifier are essentially isomorphic. In an effort to address this issue, the Work Group recommends that this subcriterion be changed to: “significant maladaptive change in behavior because of the attacks (e.g., behaviors designed to avoid having PAs), which may include agoraphobic avoidance.” While we appreciate the attention of the Work Group to this issue, we believe that their recommendation does not sufficiently disentangle the redundancy, and therefore does not remedy the issue of redundancy in the diagnostic process. In other words, even with this change, clinicians will consider avoidance behaviors in the diagnosis of PD, and then consider the same behaviors with regard to the AG specifier.
Agoraphobia
AG has had a complex historical relationship with PD and panic. One of the more controversial diagnostic issues in this area has been the existence of AG as separate diagnostic entity outside of PD. Contemporary classification systems highlight this controversy. In the DSM-IV-TR, AG is viewed as subordinate to PD, while in the International Classification of Diseases 10th edition (ICD-10) AG is viewed as an independent condition. This diagnostic discrepancy appears to have evolved out of differences in how European (ICD-10) and American (DSM) researchers have conceptualized the nature of AG and, interestingly, is one of the few instances where the ICD-10 and DSM-IV classification systems differ.
The first modern conceptualization of AG suggested that this was a phobic disorder resulting from a fear of public places in patients who may or may not experience panic attacks (Marks & Bebbington, 1976). Thus, the diagnosis of AG predated PD, and was originally coded in the ICD as a condition marked by avoidance due to multiple fears and phobias, with no necessary diagnostic connection to panic. Similarly, AG first appeared as a diagnosis in the DSM-III (APA, 1980) and was coded to allow for the specification of the presence or absence of panic attacks. After the publication of the DSM-III, the popular opinion in America shifted and patients with AG were viewed to be avoiding situations due to a fear of the onset of panic. This change in conceptualization was reflected in the DSM-III-R, where AG was diagnosed within the context of PD (PD with or without AG).
The classification of AG as a subordinate diagnosis continued in the DSM-IV. Currently, a diagnosis of AG can be given, but only in the context of panic and PD. Severe avoidance in the absence of a clear history of PD can be diagnosed as AG without history of PD. However, this diagnosis is complicated by the fact that the presence of AG must be “related to fear of developing panic-like symptoms” (p. 443), which could be limited symptom panic attacks not qualifying as full panic attacks (necessary for a PD diagnosis). A prototypical example of individuals diagnosed with AG without a history of PD are those who avoid situations due to a fear of medical catastrophe resulting from a medical condition, such as individuals with irritable bowel syndrome (IBS) who are concerned about a sudden onset of diarrhea in a location where access to a bathroom is restricted. Thus, panic attacks and PD have been integrally linked with AG in every iteration of the DSM since the inclusion of AG in the DSM-III.
The main focus of the DSM-V Work Group centered on discussions about the classification of PD and AG as separate entities. Specifically, the evidence was reviewed to address the question of whether to maintain the structure from the DSM-IV and keep AG as a secondary diagnosis to PD.
Research has shown an interesting pattern of divergence between AG and PD. In many epidemiological studies, researchers have found a high percentage of individuals diagnosed with AG that have no history of PD (Faravelli, Furukawa, & Truglia, 2009). On the other hand, studies examining clinical samples have failed to corroborate these findings such that AG with no history of PD is rarely encountered (Kessler et al., 2006). To explain this discrepancy, some researchers have suggested that the rates of AG without history of PD are inflated in large epidemiological studies due to deficiencies on the part of the interviewers, who are typically not trained mental health professionals, to accurately assess for panic (Barlow, 2002).
Regardless of these notable discrepancies, recent research out of Europe has provided compelling evidence that AG can exist independent of panic or panic-like symptoms in a significant number of individuals (Faravelli, Cosci, Rotella, Faravelli, & Catena Dell’Osso, 2008; Fava & Morton, 2009; Wittchen, Reed, & Kessler, 1998). Furthermore, one review of prospective reports and incidence patterns suggests that despite the common comorbidity of AG and PD, there are a substantial number of individuals who meet criteria for AG without any history of panic or panic-like symptoms (Wittchen et al., 2008).
The Work Group failed to reach a consensus decision on the issue of the independence of AG. The principle issue appears to be that despite the empirical evidence supporting the existence of individuals with AG without a history of panic, these individuals rarely present for treatment (and therefore have little effect on real-world clinical settings), and that the current diagnostic system functions well. However, the Work Group decided to recommend that AG and PD become separate diagnostic entities that can be diagnosed independently in an effort to simplify the system, removing the need for AG without history of PD. Thus, patients can be diagnosed with PD, with AG, or with both.
Our belief about this discussion is that the recommendation by the Work Group is not only reasonable but could also serve to alleviate some problematic issues in diagnosing AG related to the DSM-IV-TR classification. In the DSM-IV-TR, we are categorizing two very different clinical phenomena with the same nomenclature since we currently allow AG to serve as both a subordinate specifier (in the context of PD) and a diagnosable disorder (AG without history of PD). With the typical PD with AG case, we see individuals who are exhibiting extreme behavioral avoidance due to a fear of panic or panic-like symptoms. On the other hand, individuals who meet for AG without history of PD are presumably different enough from PD with AG patients as to not warrant a PD diagnoses. Indeed, an IBS patient who avoids public places out of a fear of experiencing diarrhea in the absence of a restroom would require a different treatment approach than a patient who avoids public places due to a fear of panic. Therefore, we support the Work Group’s recommendation in the hopes that it will reduce the potential confusion resulting from the use of AG as both a specifier and a diagnostic entity in the current classification system.
Following the DSM-IV (APA, 1994) classification, AG essentially serves as an index of phobic avoidance when diagnosed in the context of PD. By assigning the AG specifier, the clinician is acknowledging that the phobic avoidance behavior is clinically significant. This creates an arbitrary categorical description of avoidance severity. It is quite possible that two patients with PD who fall slightly on either side of “clinically significant” avoidance are more similar than two other patients receiving the AG specifier (one with moderate avoidance and one with extreme avoidance). In the spirit of addressing such an issue, the architects of the DSM and DSM critics have long debated the merits of dimensional assessments, and in our opinion this is an area where a dimensional assessment of phobic avoidance would provide a more useful depiction of a patient’s condition (Schmidt & Cromer, 2008).
Another issue exists in relation to considering AG in the diagnosis of PD. When AG is given in the context of PD, it is essentially an indication of phobic avoidance. This raises the question of why is this specifier is considered in a PD diagnosis but not in the diagnosis of any other anxiety disorders? Knowledge of the level of phobic avoidance, and a diagnosis of AG in the context of PD, can provide clinical utility (e.g., predicting treatment response for PD patients). However, it appears as though the Work Group did not dedicate significant discussion to why a diagnosis of AG, or some other avoidance specifier must be considered in the context of PD, but not for other phobic anxiety conditions (e.g., social phobia, specific phobia).
With most of the Work Group’s discussion surrounding AG dedicated to the potential independence of AG from panic and PD, it seems that the Work Group has not adequately addressed the appropriateness of the current diagnostic criteria for AG. On top of the issues raised in this article, there are other critical issues concerning the diagnostic criteria of AG per se.
There have been minimal changes to the diagnostic criteria of AG in the recent editions of the DSM. According to the DSM-III-R, a diagnosis of AG is warranted when and individual restricts travel (avoidance), needs someone to travel with them (use of companions), or endures these situations with extreme anxiety (marked distress) due to fears of experiencing panic or panic-like symptoms. It is important to note that the DSM-III-R definition of AG does not require the individual to exhibit phobic avoidance. In fact, individuals with no avoidance behavior can receive an AG diagnosis as long as they endure agoraphobic situations with extreme distress or if they require a companion in such situations. For example, an individual may travel extensively but need their spouse to do so, or they might be able to travel alone while experiencing extreme distress, yet an AG diagnosis is still indicated. Some researchers have criticized the broad nature of this criterion as being overinclusive (Cox, Endler, & Swinson, 1995; Schmidt & Cromer, 2008). Nonetheless, in the DSM-III-R the central role of avoidance behaviors was highlighted in the classification of the severity of AG (none, mild, moderate, severe). The current version of the DSM (DSM-IV-TR; APA, 2000) does not include such a classification, giving equal weight to avoidance, distress, and use of companions in the determination of a dichotomous diagnosis (absent, present).
The unspecified mixture of actual avoidance, distress in situations, and use of companions required for an AG diagnosis in DSM-IV illustrates the potential problems with this current criterion. Currently, the criterion suggests that when considering AG, equal weight should be given to these three issues. Yet, we know that clinicians are more apt to make a diagnosis in patients who present with more centrally casual (e.g., avoidance behaviors) versus peripheral symptoms (Kim & Ahn, 2002). Following this logic, with regard to AG, clinicians should give stronger consideration to avoidance behaviors as compared to the experience of distress or the use of companions. Furthermore, clinicians should be less reliable in making AG diagnoses when these secondary features are present in the absence of phobic avoidance. Unfortunately, empirical work supports the occurrence of both these fallacies when considering an AG diagnosis (Schmidt, Salas, Bernert, & Schatschneider, 2005). As can clearly be seen, there are still a number of important diagnostic issues that need to be addressed pertaining to the diagnosis of AG, both independent from and in the context of PD.
Discussion and Applications to Social Work
There are several notable recommendations that arose from the Work Group discussions (Table 1). Primarily, we fully support the Work Group’s recommendation to remove AG as a specifier in the context of PD, and have it be classified as a separate diagnosable condition. This will serve to not only help account for the individuals who experience AG without panic, but will hopefully clear up some of the confusion that can result from having AG as both a specifier (PD with AG) and a separate diagnostic entity (AG without history of PD) in our current system. Another notable recommendation from the work group is to consolidate worry about having additional panic and worry about the consequences of panic into a single panic-related worry criterion for the diagnosis of PD. Due to the research supporting the highly correlated nature of these phenomena, it seems intuitive to combine them to reduce redundancy.
Nonetheless, the main issue highlighted by the Work Group’s discussions is the dearth of research addressing the diagnostic criteria for panic attacks, PD, and AG. Since the publication of the DSM-IV, there has been minimal literature to support or refute the current criteria, leaving us with an inability to thoughtfully reconstruct the criteria to more accurately reflect the nature of these conditions. To further complicate this issue, when this article was written the final window had closed for the public to comment on the proposed changes for DSM-V, yet the data from the field trials for panic and AG had not yet been published, leaving no publically available data regarding the reliability and validity of these new criteria. It is unclear how experts in the field are supposed to provide valuable analysis as to the reliability and validity of the proposed changes in the absence of the data which most directly address this issue. It is not our opinion that the DSM-V committee is being intentionally opaque, but rather that given the lack of studies over the past two decades that have addressed the diagnostic issues surrounding panic and AG, the data from the field trials would have been of particular benefit to this public discussion.
Pros and Cons of DSM-V Proposed Changes.
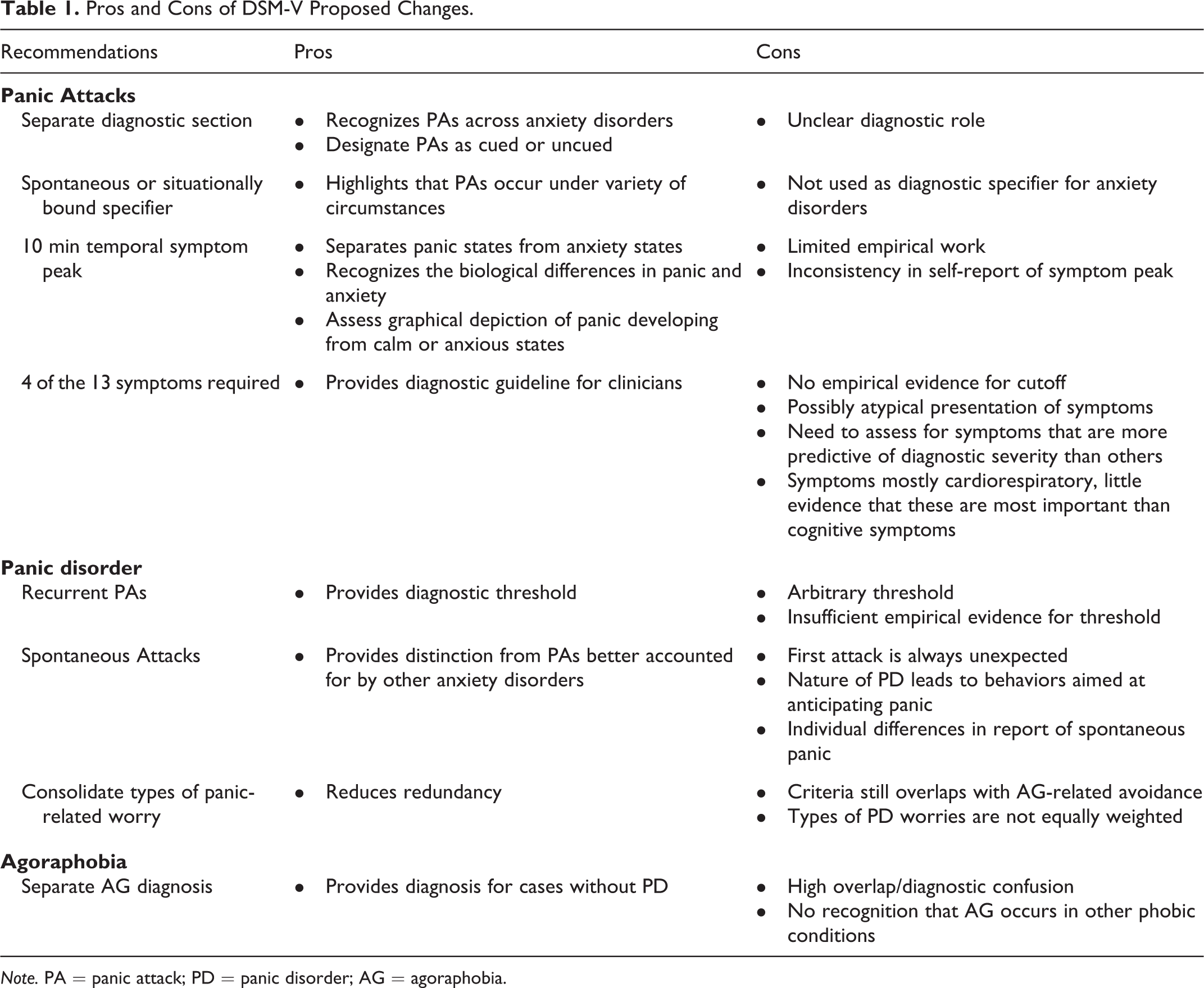
Note. PA = panic attack; PD = panic disorder; AG = agoraphobia.
It is our opinion that there are specific areas of research that would greatly help both our understanding of the nature of panic and AG as well as our ability to define these conditions in future iterations of the DSM. With regard to panic per se, studies should investigate the nature of panic attacks across anxiety diagnoses, and how they impact the course, severity, and treatment of different anxiety conditions. This information would shed light on whether panic attacks would be a useful specifier across anxiety diagnoses that could help clinicians to determine the most appropriate treatment for their clients. Furthermore, research should attempt to illuminate whether individuals who fear panic are a distinct group from individuals who fear anxiety. The Work Group’s suggestion to have graphical depictions of panic episodes could help in improving the diagnostic reliability of “discrete panic,” but empirically establishing a clear difference between these groups will be an important step in determining whether endorsing “discrete panic” is an integral part of diagnosing the presence of panic attacks.
Two more research agendas that would help clarify our understanding of panic attacks for future iterations of the DSM would be to establish the validity of the four panic symptoms cutoff for a full panic attack and an investigation of the usefulness and the weighting of both cardiopulmonary and cognitive symptoms of panic. Given the Work Group’s review of the literature which suggests about half of the individuals do not meet the four symptom threshold, and are therefore diagnosed with “limited symptom panic attacks,” it would be wise to establish a data-driven cutoff that will identify the occurrence of panic attacks with the greatest balance of sensitivity and specificity. With regard to the weighting of the cardiopulmonary and cognitive symptoms, research should investigate the effects of having the symptoms weighted so heavily toward cardiopulmonary experiences. It is possible that a more balanced system would be more appropriate. On the other hand, it is also possible that the cognitive symptoms of panic do not belong in the diagnosis of panic attacks. As discussed previously, it may be that cognitive symptoms of panic are really more relevant when considering a PD diagnosis, rather than the presence of panic per se.
With regard to PD, it seems that researchers should investigate the suitability of the criterion requiring the experience of “recurrent” and “unexpected” panic attacks. At face value, this may appear to be an appropriate necessity for someone to be diagnosed with PD, however, there does not appear to be sufficient evidence to claim that an individual who experiences a single panic attack cannot be impaired by panic-related worry and avoidance behaviors. Furthermore, as discussed earlier, the unexpected nature of panic is largely dependent on individual differences in how adept one is at identifying potential environmental or interoceptive cues. Therefore, we should empirically examine whether there is truly a difference between individuals who claim to have unexpected versus cued panic attacks and whether those differences are essential when considering a PD diagnosis. It is possible that research will show that a broader criterion stating that an individual must have experienced at least one panic attack may provide more diagnostic utility than “recurrent” and “unexpected” panic attacks, and place the focus more centrally on panic-related worry and avoidance behaviors.
On the subject of avoidance behaviors, an important endeavor will be to attempt to differentiate panic-related avoidance from agoraphobic avoidance. The proposal by the Work Group to include the phrase “which may include agoraphobic avoidance” in the PD panic-related avoidance subcriterion highlights the complexity of this diagnostic issue. At what point does panic-related avoidance turn into AG? In order to improve this classification system we must determine the empirical difference between panic-related avoidance behavior that qualifies an individual for a PD diagnosis but is not sufficient for an AG diagnosis. Furthermore, researchers should investigate the effect of giving equal weight to avoidance behaviors, enduring with extreme distress, and requiring companionship when considering AG with regard to both the validity and reliability of AG diagnoses.
The DSM-V panic and AG Work Group carefully reviewed the extant literature and made recommended changes to the diagnostic criteria for panic attacks, PD, and AG, with the hopes of improving our current diagnostic classification system. However, it has become evident, the Work Group was severely handicapped by the shear lack of research over the last two decades addressing these complex diagnostic questions. Hopefully, researchers will respond to this dearth of information and attempt to empirically address these important diagnostic issues. Our hope is that in future iterations of the DSM we will feel more confident in our ability to revise the panic and AG criteria to more accurately classify these clinical presentations.
The proposed changes to the DSM-V will have numerous clinical applications. These applications will likely impact clinicians the most when they are performing diagnostic evaluations and determining the most efficacious treatment for the presenting problems. Perhaps one of the most important clinical applications in using the DSM-V criteria will be observed in determining whether panic attacks are associated with PD or another disorder. To illustrate, while the DSM’s separation of the diagnostic criteria for panic attacks and PD increases the recognition that panic attacks occur outside of PD, the unclear diagnostic role of this separation is problematic in that it fails to provide the necessary specification for determining whether panic is associated with PD or another disorder. With this in mind, it is especially important for clinicians to differentiate between panic attacks that are due to panic-related fears (i.e., fear that something is wrong with them, worry about having another panic attack) and panic attacks occurring in the context of other anxiety disorders (i.e., fear of negative evaluation, fear of contamination) to determine whether PD is present or if the panic attacks are better accounted for by another anxiety disorder diagnosis.
Another important clinical application will be the use of the graphical depictions of panic. Although most panic attacks have a temporal peak around 10 min after the onset of symptoms, it is important to remember that some patients experiencing panic attacks will report their symptoms as lasting much longer than the typical presentation. Clinicians must also be cognizant of individual differences in the ability to provide accurate retrospective reports of panic symptoms. It is possible that some patients experiencing panic attacks during a period of increasing anxiety may report their panic attacks as lasting hours when the actual panic attack may have lasted a few minutes. Using the DSM-V graphical depictions will be useful in determining whether the patient experienced a distinct panic attack during that time or if they are describing a period of prolonged anxiety.
These examples highlight a few of the ways in which the changes to the DSM-V may impact clinicians working with patients experiencing panic attacks, PD, and AG. While it is difficult to predict the extent to which changes in the DSM will impact clinicians, it is important for clinicians to appreciate the reasons, as well as the many limitations that are related to the proposed changes.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.