
Abstract
Purpose:
This study examined the construct validity and reliability of a therapeutic alliance measure (Children’s Alliance Questionnaire [CAQ]) for children with psychosocial and/or behavioral problems, receiving therapeutic residential care or day care in the Netherlands.
Methods:
Confirmatory factor analysis of a one-factor model “therapeutic alliance” was conducted on two samples of 115 and 116 children, aged 4–14 years. Reliability analysis and concurrent validity were examined.
Results:
Results showed a good fit to the data, indicating construct validity of the measures. Cronbach’s α reliability coefficients were good for both alliance measures. Concurrent validity was supported by significant relations between the alliance scale and positive group climate (Group Climate Instrument for Children [GCIC]) and treatment motivation (Adolescent Treatment Motivation Questionnaire). No correlations with negative group climate (GCIC) were found.
Discussion:
The CAQ can be used as an assessment tool for therapeutic alliance within both residential treatment and therapeutic day care settings for children.
Introduction
During the 20th century, both researchers and clinicians have defined the concept of therapeutic alliance in a variety of ways (Bordin, 1979; Elvins & Green, 2008; Horvath, 2005; Safran & Muran, 2006). Bordin (1979) distinguished three main components of the alliance: the client–therapist bond or relationship, agreement on goals, and collaboration on tasks. Therapeutic alliance has been extensively researched in the context of adult psychotherapy. Several studies indicate that the quality of therapeutic alliance has a significant impact on treatment outcomes (Ardito & Rabellino, 2011; Flückiger, Del Re, Wampold, Symonds, & Horvath, 2011; Horvath & Bedi, 2002; Martin, Garske, & Davis, 2000; Norcross, 2010).
Various meta-analyses have shown that the effect of therapeutic alliance on treatment outcomes in youth is comparable to its effect on treatment outcomes in adults (Bickman et al., 2012; Karver, Handelsman, Fields, & Bickman, 2006; Shirk & Karver, 2003; Shirk, Karver, & Brown, 2011). However, a recent meta-analytic review, using the largest study sample, found a smaller effect size in youth (McLeod, 2011). Authors suggest that these findings are due to differences in conceptualization and methodology used in research on therapeutic alliance. On a conceptual level, there is no consensus about a general definition of the therapeutic alliance in research on child and youth care (Elvins & Green, 2008; Zack, Castonguay, & Boswell, 2007). It has been argued that the alliance concept in youth may be viewed as a one-dimensional construct due to children’s incapacity to discriminate between different components of the alliance, such as “collaboration on tasks” and “agreement on goals” (DiGiuseppe, Linscott, & Jilton, 1996; Faw, Hogue, Johnson, Diamond, & Liddle, 2005; Hogue, Dauber, Stambaugh, & Cecero, 2006; Shelef & Diamond, 2008).
Children and adolescents often do not seek professional help for their problems voluntarily and are sent to therapy because of perceived behavioral problems (Elvins & Green, 2008; Orsi, Lafortune, & Brochu, 2010; Shirk & Saiz, 1992). Additionally, due to adolescents’ stage of development, they tend to distance themselves from adult influences (Bickman et al., 2004; Fitzpatrick & Irannejad, 2008; Shirk & Karver, 2003). Establishing a therapeutic alliance with children seems even more difficult than forming an alliance with adolescents, because children may not be aware of their problems and often demonstrate resistance to treatment (Elvins & Green, 2008; Shirk & Saiz, 1992).
Studies on therapeutic alliance in children and adolescents have mainly focused on outpatient therapy (Karver et al., 2006; Shirk & Karver, 2003; Shirk et al., 2011). However, many children and youth receive treatment in residential treatment facilities. There are only a few studies that have addressed the role of the therapeutic alliance within a residential treatment setting (Duppong Hurley, Lambert, Van Ryzin, Sullivan, & Stevens, 2013; Handwerk et al., 2008; Orsi et al., 2010). Treatment within such settings brings forth challenges to the assessment of therapeutic alliance because there is not one therapist, but several treatment staff members with whom a client can form an alliance.
Therapeutic Living Group Climate and Treatment Motivation
In treatment of children and adolescents, particularly within residential treatment, an open living group climate is important for treatment success (Van der Helm, 2011; Van der Helm, Klapwijk, Stams, & Van der Laan, 2009; Van der Helm, Stams, & Van der Laan, 2011). An open group climate consists of a supportive environment in which group workers attend to the psychological needs of adolescents and refrain from repressive methods (closed group climate). Such an open living group climate is thought to positively influence the establishment of a therapeutic alliance with children receiving residential treatment. Furthermore, quality of therapeutic alliance has been found to be associated with establishing and/or maintaining treatment motivation in therapy (Constantino, Castonguay, Zack, & DeGeorge, 2010; Karver et al., 2006; Shirk et al., 2011). Studies suggest that failing to engage the child or adolescent in therapeutic activities can negatively affect the bond between the therapist and the child or adolescent (Constantino et al., 2010; Fitzpatrick & Irannejad, 2008).
Development of the Children’s Alliance Questionnaire (CAQ)
In the Dutch-speaking area, only one alliance measure, using Bordin’s conceptualization of the therapeutic alliance, has been validated (Werk Alliantie Vragenlijst, Stinckens, Ulburghs, & Claes, 2009). However, this measure is only suitable for adults. Currently, no validated alliance measure based on Bordin’s conceptualization is available to assess the quality of therapeutic alliance in children and youth. In one Dutch study, a translation of the Therapeutic Alliance Scale for Children (TASC; Shirk & Saiz, 1992) has been used. The TASC measures therapeutic alliance in children aged 12 years and older. Consequently, no validated instruments are available measuring therapeutic alliance in young children (12 years and younger) in The Netherlands. Also, there are no instruments available measuring therapeutic alliance in children with mild intellectual disability, in which case a questionnaire should use simple language.
In this study, various items from the Working Alliance Inventory (WAI-S; Tracey & Kokotovic, 1989) were translated in Dutch and inspected thoroughly by practicing professionals in the field of youth care. The WAI-S is a short questionnaire for adults, derived from the WAI (Horvath & Greenberg, 1989) and was adapted for specific use in a child population and children with mild intellectual disability. In order to create a brief and simplified measure for children (14 years or younger), items that consisted of long or multiple sentences and items containing difficult language were rephrased or dismissed. For the age-group 4–8, the original 7-point scale from the WAI was transformed to a 3-point scale, consisting of “thumbs-up or down” pictures to reduce problems in comprehension of the items for young children and children with mild intellectual disabilities. For the age-group 8–14, a 5-point Likert-type scale was used, without depicting thumbs-up or down.
The aim of this study was to create a measure to assess quality of therapeutic alliance in two distinct age-groups of children receiving residential treatment and therapeutic day care. After constructing the scales, construct and concurrent validity of the measures were assessed by means of confirmatory factor analysis. The relations between therapeutic alliance and living group climate, and therapeutic alliance and treatment motivation, were examined in order to determine concurrent validity. To ensure concurrent validity, the alliance measure should correlate (strongly) with a different instrument that has been previously validated, which is administered at the same time, and assesses a related construct that may be considered a criterion. In this study, concurrent validity is demonstrated when the alliance measure correlates positively with open group climate and treatment motivation. Also, concurrent validity is demonstrated when the alliance measure correlates inversely with closed (i.e., repressive) group climate.
Method
Participants
The sample in the age-group 4–8 consisted of N = 115 children, n = 90 boys (78.3%), and n = 25 girls (21.7%); mean age of respondents was 5.34 (standard deviation [SD] = 1.29). Within this group, 30 children received residential treatment and 85 children received therapeutic day care. The sample in the age-group 8–14 consisted of N = 116 children, n = 78 boys (67.2%), and n = 38 girls (37.8%); mean age of respondents was 10.8 (SD = 1.89). Within this group, 33 children received residential treatment and 83 children received therapeutic day care.
Procedures
This study was conducted in seven institutions for residential treatment and therapeutic day care for children aged 4–8 years and in four institutions for residential treatment and therapeutic day care for children aged 8–14 years. The study was performed between March and July 2012. The parents of the participating children received a letter in which the purpose of the research was disclosed. Parents were asked to give legal permission for their child to participate in the study and signed an informed consent form. Questionnaires were given a number in order to guarantee anonymity of the participants. All measurements were carried out by two researchers who signed a written statement of confidentiality.
Children in the age-group 4–8 were assisted to complete a therapeutic alliance questionnaire and a questionnaire to measure group climate by a assistant researcher who read the questions and answering categories out loud. Children in the age-group 8–14 filled out the therapeutic alliance questionnaire, a group climate questionnaire, and a motivation questionnaire. For the age-group 4–8, questions were written on laminated cards. Three boxes were put out to form answering categories to assist the child in identifying the three answering categories, each depicting a symbol: “thumbs-up,” “thumbs-down,” or “thumb half-way up.” The ‘thumbs-up’ symbol represented the answering category “true,” the “thumbs-down” symbol represented the answering category “not true,” and the “thumb half-way up” symbol represented the answering category “somewhat true.” The (assistant-) researcher read each question to the child and the child was asked to put the question in one of the three boxes. Besides reading the question to the child, the answering categories were also read out loud and explained to the child. Furthermore, in case of apparent misunderstanding or hastily answering by the child, additional questions were asked to ensure the child had understood the question. The (assistant-) researcher was not in any way involved in the treatment of the children. Before administering the questionnaire with the children, the (assistant-) researcher explained to the child that the questions would be applicable to the child’s mentor who had been identified by name. The child was guaranteed that the mentor would not be informed about the answers of the child.
Questionnaires
CAQ
This study used a therapeutic alliance questionnaire, which was partially derived from the WAI (Horvath & Greenberg, 1989) and WAI-S (Tracey & Kokotovic, 1989) measuring therapeutic alliance in an adult population. The WAI-S is a short questionnaire for adults, derived from the WAI and was translated and back translated into Dutch and adapted for specific use in a child population and children with mild intellectual disability. Items in the questionnaire were reformulated into short sentences using simplified language to improve comprehension of the items for very young children. The WAI and WAI-S both measure the “bond,” “task,” and “goal” dimension of the alliance. The measures in this study capture the bond, task, and goal dimension of the alliance construct in a one-dimensional factor “overall alliance.”
Two versions of the questionnaire have been used for two different age-groups. Items were shortened and rephrased in a more simple way, especially for the youngest age-group 4–8 years for whom questions have been formulated instead of statements. Also, some questions were asked from the point of view of the child instead of the use of statements from the point of view of the therapist. For example, “I believe the therapist likes me.” was changed into “Do you like your mentor?”
For the age-group 8–14, either statements from the point of view from the child or the therapist were used. Additionally, the word therapist was replaced with the term “mentor,” because children in psychotherapy are more familiar with this term. For example, “The therapist and I are working towards mutually agreed upon goals.” was changed into “My mentor helps me to achieve my goals.” The questionnaire for the 4–8 age-group contains 10 items that were rated on a 3-point Likert-type scale, ranging from 1 (not true) to 2 (somewhat true) and 3 (true). The questionnaire for the 8–14 age-group contains 9 items that were rated on a 5-point Likert-type scale, ranging from 1 (not at all true) to 3 (in between) and 5 (totally true).
Group Climate Instrument for Children (GCIC)
The GCIC (Strijbosch et al., 2013) was used to assess living group climate. The GCIC questionnaire is derived from the Prison Group Climate Instrument (Van der Helm et al., 2011) that has been extensively researched in groups of adolescents and adults. This instrument consists of four scales: “support,” “growth,” “atmosphere,” and “repression.” The GCIC questionnaire consists of two scales: “open” (positive) group climate and “closed” (negative) group climate. Several items from the “support,” “growth,” and “atmosphere” scales belong to the open climate scale and several items from the “repression” scale belong to the closed group climate scale. An example item of the open group climate scale is “In this group, there are always enough people to help me.” An example item of the closed group climate scale is “The chaos in this group drives me crazy.”
The questionnaire for the age-group 4–8 consists of 20 items rated on a 3-point Likert-type scale ranging from 1 (not true) to 2 (somewhat true) and 3 (true). The instrument measures group climate and differentiates between open (positive) group climate (11 items) and closed (negative) group climate (9 items). Cronbach’s α reliability coefficients were good for both open climate (α = .747) and closed climate (α = .699). The questionnaire for the age-group 8–14 consists of 14 items rated on a 3-point Likert-type scale ranging from 1 (not true) to 2 (somewhat true) and 3 (true). The instrument measures group climate and differentiates between open group climate (9 items) and closed group climate (5 items). In the present sample, Cronbach’s α reliability coefficients were good for open climate (α = .914) and closed climate (α = .718).
Adolescent Treatment Motivation Questionnaire (ATMQ)
To assess treatment motivation, the ATMQ (Van der Helm, Wissink, De Jongh, & Stams, 2013) was used. This instrument was derived from the Motivation for Treatment questionnaire (Van Binsbergen, 2003) and is based on the transtheoretical model of Prochaska and DiClemente (1986). The instrument consists of 11 questions measuring the action phase of treatment motivation as a single construct using a 3-point Likert-type scale ranging from 1 (not true) to 3 (true). An example item is “My treatment helps me.” A higher overall score is to be interpreted as a higher level of motivation for treatment. This questionnaire was only used in the age-group 8–14 because the instrument has not yet been validated for a younger age-group. The internal consistency of the measure was good (α = .753).
Statistical Analyses
Construct validity of the alliance scale was examined by means of confirmatory factor analysis using Amos 18 (Arbuckle, 2007). A one-factor model was specified in which each item loaded on only one factor. Both the model’s χ2 and fit indices, which are nonsensitive to sample size (comparative fit index [CFI], Tucker–Lewis index [TLI], and root mean square error of approximation [RMSEA] 1 ), were used to evaluate model fit (Kline, 2005). The following fit index cutoff values are indicative of good model fit: normed fit index (NFI) > .90; CFI > .90, TLI > .90, and RMSEA < .05 (Kline, 2005). A nonsignificant χ2 indicates exact model fit, a ratio between the χ2 statistic and the degrees of freedom (df) that is lower than 2.5 indicates a close fit to the data (Hu & Bentler, 1999). To account for nonindependence and nonnormality, the robust maximum likelihood estimation procedure was chosen (Muthén & Muthén, 1998). A modification index, giving the expected drop in χ2 if the parameter in question is freely estimated, was used to improve model fit. Thus, parameters that could improve model fit by freeing those parameters were identified. Further improvement of model fit was achieved by removing items that did not load significantly on the factor.
To examine concurrent validity of the alliance measure, we used the two scales of the Group Climate Instrument for Children (GCIC) Questionnaire: open group climate and closed group climate (Strijbosch et al., 2013). For the age-group 8–14, an additional motivation questionnaire was used (ATMQ; Van der Helm et al., 2013). Concurrent validity is demonstrated when alliance correlates positively with open group climate and treatment motivation. Also, concurrent validity is demonstrated when alliance correlates inversely with negative group climate.
Results
Construct Validity and Reliability
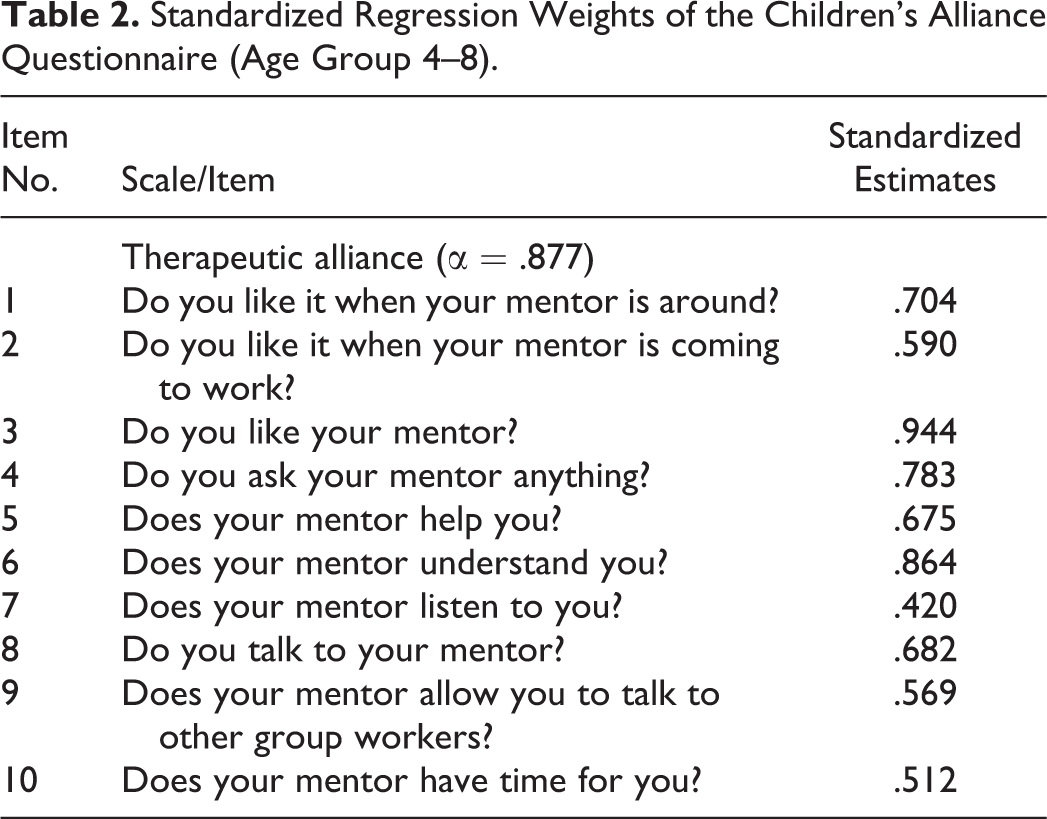
Results for the age-group 4–8 questionnaire (Table 1) indicated a good fit to the data: χ2 = 22.618, df = 22, p = .424; NFI = .940; CFI = .998, TLI = .995, and RMSEA = .017. Results showed factor loadings ranging from .420 to .944 (Table 2). For this age-group, the CAQ was found to be internally consistent (α = .877). Results for the age-group 8–14 questionnaire (Table 1) indicated a good fit to the data: χ2 = 17.804, df = 22, p = .718; NFI = .971; CFI = 1.000, TLI = 1.015, and RMSEA = .000. Results showed factor loadings ranging from .546 to .907 (Table 3). The CAQ for this age-group was also found to be internally consistent (α = .895).
Results of Confirmatory Factor Analysis of the Children’s Alliance Questionnaire (Age Group 4–8).

Note. NFI = normed fit index; CFI = comparative fit index; TLI = Tucker–Lewis index; RMSEA = root mean square error of approximation.
Standardized Regression Weights of the Children’s Alliance Questionnaire (Age Group 4–8).
Standardized Regression Weights of the Children’s Alliance Measure (Age Group 8–14).

Concurrent Validity
To examine concurrent validity of the alliance measure, Pearson’s r test was used to calculate correlations between the alliance scale and the open and closed climate scale of the GCIC questionnaire for both age-groups and the ATMQ for the age-group 8–14. For the 4–8 age-group, we found the alliance scale to have a positive correlation with open group climate (r = .597; p < .01). No significant correlation was found for the alliance scale with closed group climate (Table 4). For the 8–14 age-group, positive correlations were found between the alliance scale and open group climate (r = .525; p < .01) and between alliance and motivation (r = .544; p < .01). No significant correlation was found for the alliance scale with closed group climate (Table 5).
Means, Standard Deviations, Range of the Scores, and Correlations of the Children’s Alliance Questionnaire and GCIC Scales (Age Group 4–8).

Note. GCIC = Group Climate Instrument for Children.
**Correlation is significant at the .01 level (two-tailed).
Means, Standard Deviations, Range of the Scores, and Correlations of the Children’s Alliance Questionnaire, ATMQ, and GCIC Scales (Age Group 8–14).

Note. ATMQ = Adolescent Treatment Motivation Questionnaire; GCIC = Group Climate Instrument for Children.
**Correlation is significant at the .01 level (two-tailed).
Discussion and Applications to Social Work
Few studies have investigated the psychometric properties of therapeutic alliance measures used for psychotherapy in a child population, especially in treatment of young children. The aim of this study was to address this lacuna by examining the factor structure, validity, and reliability of the CAQ, measuring therapeutic alliance in children receiving residential treatment and therapeutic day care in The Netherlands. In doing so, two versions of a therapeutic alliance measure for two age-groups of children—4–8 years and 8–14 years old—were constructed.
Evidence for construct validity of the alliance scales was found in confirmatory factor analyses. Evidence for good internal consistency reliabilities was found in reliability analyses. Results of confirmatory factor analyses indicated that the alliance scales for both age-groups best fit a one-factor solution “overall alliance.” For both the age-group 4–8 years and 8–14 years, evidence for concurrent validity was found in a strong positive correlation between the alliance scale and open group climate. Also, a strong positive correlation was found between the alliance scale and treatment motivation in the age-group 8–14. In both age-groups, no correlations were found between the alliance scale and closed group climate, indicating no support for concurrent validity. This can be possibly explained by the small number of items of which the negative group climate scale consists.
These results are in line with the findings of international studies examining the factor structure of self- and observer-reported therapeutic alliance measures designed for youth psychotherapy (i.e., Adolescent WAI [AWAI], Adolescent Therapeutic Alliance Scale, Vanderbilt Therapeutic Alliance Scale–Revised [VTAS-R]), which also found support for one-factor solutions. Consequently, there is accumulating evidence indicating that children do not seem to discriminate between distinct alliance dimensions of the therapeutic alliance. These findings suggest that the alliance construct in children receiving psychotherapy is best understood as a one-dimensional construct (DiGiuseppe et al., 1996; Faw et al., 2005; Hogue et al., 2006).
Limitations of this study were related to methodological issues as well as the absence of other validated instruments measuring therapeutic alliance in child psychotherapy in The Netherlands facilitating the examination of convergent validity. Currently, there are no validated instruments measuring therapeutic alliance in children and youth in the Netherlands to compare with the CAQ. Items of both alliance scales were derived from a therapeutic alliance measure used in an adult population (WAI-S). A thorough specification of the items had been carried out to fit the developmental level of children, especially young children. The use of items from the original adult measure to assess convergent validity may yield biased results, because the items in the scale may not capture all relevant aspects of the therapeutic alliance in child therapy (Elvins & Green, 2008).
Second, the samples used in this study consist mostly of boys. This could possibly impede generalization of the results of this study to girls. Third, in this study, no data from the point of view of the therapist and no data from ratings by an observer were obtained. Use of therapist and observer ratings in addition to self-report ratings may lead to a better assessment of concurrent (and convergent) validity of the therapeutic alliance in children. Although self-report measures of therapeutic alliance aim to directly assess the perspective of those involved in therapy, thus representing the ideal perspective, developmental factors may limit young children’s ability to comprehend and report on certain aspects of the therapeutic alliance (Shirk & Karver, 2003; Shirk & Saiz, 1992).
An important implication for the field of social work is that the CAQ can be used to assess the quality of therapeutic alliance in children, aged 4–14 years, receiving residential treatment or therapeutic day care. Most importantly, this opens up opportunities for researchers and care providers to routinely monitor the quality of therapeutic alliance between children and staff members throughout the course of treatment. In doing so, clinical practice could benefit greatly from empirical evidence to gain a better understanding of the quality of therapeutic alliance in child psychotherapy. The ability to assess therapeutic alliance in children may lead to improvements in matching the optimal therapeutic alliance fit between children and staff members during treatment.
Future research on the factor structure of therapeutic alliance measures in child psychotherapy may focus on specificity of items of scales measuring relevant aspects of therapeutic alliance in children and youth. More research is needed to thoroughly investigate whether the theoretical framework of therapeutic alliance in adults is applicable to a child population. Also, use of multi-informant ratings of therapeutic alliance might lead to a more complete understanding of the therapeutic alliance in a child population, identifying specific child and therapist behaviors or attitudes toward forming a therapeutic alliance during treatment. In sum, more research is needed to help identify the main factors influencing the therapeutic alliance in child psychotherapy and rating therapeutic alliance from multiple perspectives to identify specific child and therapist behaviors associated with alliance formation in child psychotherapy.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.