
Abstract
Objective:
This randomized controlled trial examined the effect of an intensive experiential workshop based on the Satir growth model (SGM) that aims at cultivating self-transformation.
Method:
Ninety-six adult participants were randomly assigned to the intervention group (52 participants) or the wait-list control group. The role of self-transformation, measured by the Perceived Self-Transformation Scale, in the relationship between affects and mental health problems was examined using mediation analyses.
Results:
After the workshop, the intervention group demonstrated higher levels of self-transformation (η2 = .308, p < .001), as well as significant improvement (p < .001) in positive (η2 = .557) and negative (η2 = .293) affects, self-esteem (η2 = .538), spirituality (η2 = .473), and mental health problems (η2 = .386). Importantly, increased self-transformation after the workshop partially mediated the relationship between reduced negative affect and mental health problems in the intervention group (indirect effect: β = 0.163, 95% confidence interval [0.035, 0.343]).
Conclusion:
Findings of this study suggest that the SGM-based intervention can be effective in ameliorating mental health problems.
Integrity of the self, or personal integrity, is of vital importance to the mental well-being of a person and harmony of interpersonal relationships. According to Satir, family is often the most affected social unit that bears the brunt of low personal integrity, which includes low self-worth and self-esteem (Rasheed, Rasheed, & Marley, 2011). Satir viewed that dysfunction in a family member may cause dysfunction in other family members. Depression and anxiety, which are the most common intrapsychic problems resulting from diminished levels of self-esteem, self-confidence, and self-control (MacKinnon, Michels, & Buckley, 2016), could hinder family members from functioning effectively and hence damage family health (Lima Rodriguez, Lima Serrano, Jimenez Picon, & Dominguez Sanchez, 2012). Previous studies on childbearing families showed that parental depression imposed direct and negative main effects on family functioning and youth well-being (Pakenham & Cox, 2012). It also mediated the association between family material hardship and adolescents’ problem behaviors (Sun, Li, Zhang, Bao, & Wang, 2015) and negatively influenced partner relationships and further destroyed harmony in a family (Ramchandani et al., 2011). Importantly, intrapsychic problems could also worsen interpersonal relationship between couples. For instance, the two depression-related behaviors, reassurance seeking and negative feedback seeking, might increase hostility and stress between couples (Timmons & Joiner, 2008). Also, partners of individuals with depression might tend to display more hostility and submissiveness toward the depressed person than partners of nondepressed individuals (Knobloch-Fedders, Knobloch, Durbin, Rosen, & Critchfield, 2013).
Given that lowering in self-worth, self-esteem, self-confidence, and self-control may be the underlying causes of intrapsychic and interpersonal conflicts in family, the Satir growth model (SGM) can be an appropriate family therapy to tackle these potential precursors of family dysfunction. The SGM emphasizes on “transformation” of the self (Simon, 2002), which helps individuals achieve a more coherent and healthier sense of self that has intrapsychic and interpersonal implications (Lee, 2002). For instance, Satir’s therapy challenges and transforms different internal values, perceptions, and beliefs that may affect the implicit family rules we held and expectations we impose on ourselves and our family members (Satir, Banmen, Gerber, & Gomori, 1991). It is believed that by understanding and reconnecting to oneself, one would be able to interact with his or her family members in a more positive way. Therefore, this self-transformation process is regarded as having primary importance compared to relieving the symptoms presented by a dysfunctional family (Rasheed et al., 2011). Also, Satir’s therapy highlights the importance of individual’s feelings on family communication. A previous study showing that positive affect positively correlated with the levels of family satisfaction (Carruth, Tate, Moffett, & Hill, 1997) corroborates this viewpoint. On the other hand, negative affect is a well-known distress factor that is highly associated with mental health problems (Goldberg, Krueger, Andrews, & Hobbs, 2009), while low positive affect is a significant predictor of depression (Watson, Clark, & Carey, 1988). It remains unclear whether self-transformation plays a role in the relationship between affects and mental health problems.
Despite the potential of the SGM in improving personal integrity and family health, thus far only few empirical studies have been conducted to verify the effectiveness of the SGM (Wretman, 2016). The effect of the SGM-based intervention on family relationships was explored in a group of Taiwanese college students (Der Pan, 2000), which is the only and most vigorous empirical study that has been conducted for testing the SGM. It was found that the participants’ relationships with their family members, measured by the Family Relationship Scale and Family-Self Scale, were significantly improved after the SGM-based intervention compared to the passive control condition. At the follow-up assessment, this improvement was maintained 8 weeks after the intervention. Although this study gives an initial evidence on the effectiveness of SGM-based intervention on improving family relationships, more empirical studies are needed to investigate the effectiveness of SGM on improving family processes (Wretman, 2016). In addition, it is still unclear whether and how changes in the self may dynamically facilitate this improvement. In Der Pan’s (2000) study, the fundamental change induced by the intervention, which likely involved self-transformation processes, was not investigated. The understanding of this could help to better translate the theory of SGM into useful application in individual and family therapy. One possible reason for the lack of empirical investigation on this topic is that there is only one validated scale, the Congruence Scale that could specifically capture therapeutic changes induced by SGM (Lee, 2002). Nonetheless, the Congruence Scale was validated in a Caucasian sample, whose individualistic culture is quite different from the relatively collectivist values predominant in Hong Kong.
For the sake of cultural sensitivity, the Perceived Self-Transformation Scale (PSTS-17) has recently been developed and validated to specifically assess SGM induced self-transformation in a Hong Kong Chinese sample (Leung, Lau, & Chung, 2019). The PSTS-17 has four dimensions, which are self-awareness, self-doubt, others-oriented, and openness to share. It has been shown that the PSTS-17 is a reliable and valid construct for measuring the core values specifically directed at Satir’s model and SGM in the Chinese population in Hong Kong. The aim of the current study was to test the effectiveness of an intensive Satir workshop for personal and professional development (which is referred to as the Satir workshop hereafter) that aims at bringing self-transformation to the participants. Findings of this study could provide preliminary evidence on the effectiveness of Satir workshop in ameliorating mental health problems through self-transformation.
Hypotheses
In this study, the following hypotheses were made.
Method
Participants
Participants in this study were 96 adults, Meanage(SD) = 37.41 (8.95) years, age range = 21–60 years, who enrolled in the Satir workshop offered by the Hong Kong Satir Center for Human Development from August 2014 to September 2015. Inclusion criteria were adults age ranged from 20 to 60 years, with no previous experience in the Satir model. The experimental group (who attended the Satir workshop first) consisted of 52 subjects (8 males); the wait-list control group (who attended the Satir workshop after the completion of study) consisted of 44 subjects (8 males). The demographic data are presented in Table 1.
Demographic Data.
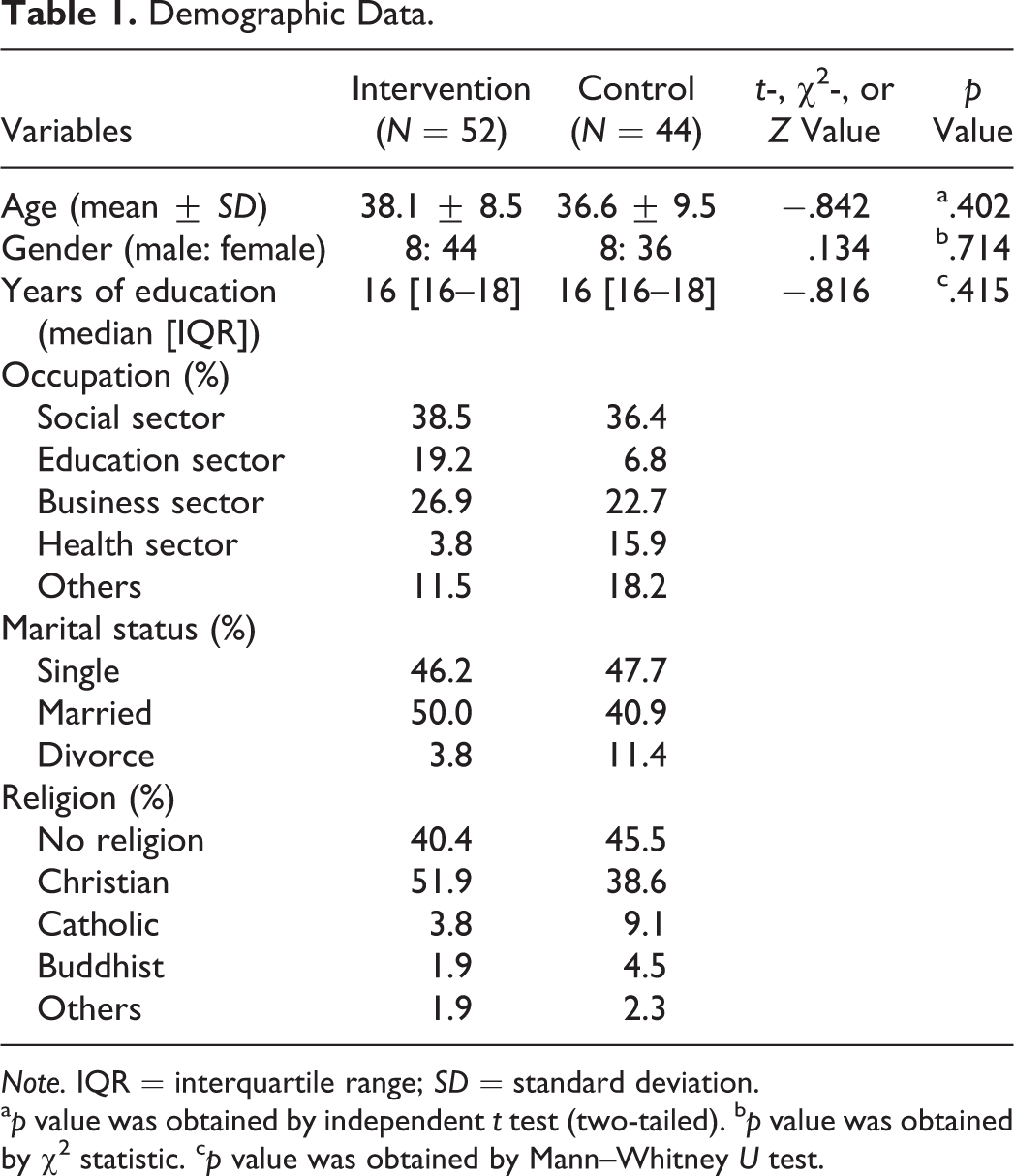
Note. IQR = interquartile range; SD = standard deviation.
a p value was obtained by independent t test (two-tailed). b p value was obtained by χ2 statistic. c p value was obtained by Mann–Whitney U test.
Design and Procedure
Recruitment
This project was not preregistered in a clinical trials registry. Recruitment was conducted following the approval of the Human Research Ethics Committee for Non-Clinical Faculties of The University of Hong Kong (EA570114). There were four Satir workshops held during the study period. The class size of each of the workshop was around 27–30 participants. Participants received the description of the study design and the procedures of the study and then completed a written informed consent form on the day of enrollment. Their participation was purely voluntary; no incentives were given to the participants. They were then randomly assigned to either the intervention group or the wait-list control group. Self-reported assessments were conducted right before (T1) and right after (T2) the intervention or waiting period and 1 month after the completion of intervention or waiting period (T3).
Randomization
Random assignment was performed by an administrative staff in the team. A block randomization approach was adopted with a block size of 27–30 (the size of a class of the Satir workshop). The four classes were randomly assigned to either the intervention group or the wait-list control group in 1:1 ratio using a lucky draw method. For example, if the first two classes are randomly assigned to the intervention groups, then the remaining two classes would be the wait-list control groups. Under such an arrangement, 52 subjects were assigned to the experimental group and 44 subjects were assigned to the wait-list control group. None of the participants dropped out due to the result of random assignment.
Participant flow
Figure 1 illustrates the participant flow from pretest, posttest to follow-up assessments. An initial sample of 114 subjects were invited to join this study. After receiving a detailed description of the study, 96 of them (84.2%) agreed to participate. For the intervention group, pretest assessment was conducted right before the start of the class on the first day of the workshop, using self-reported questionnaires. Posttest assessment was conducted right after the end of the class on the last day of the workshop, using the same set of questionnaires. Follow-up assessment was conducted 1 month after the completion of the workshop. The same set of questionnaires were mailed to each subject, and they were required to complete and send back the questionnaires to the research team by mail. For the wait-list control group, the assessment schedule was the same as that for the experimental group. They were required to complete the pretest and posttest assessments at home and then mailed back the questionnaires to the center. Specifically, the posttest assessment should be completed 3 days after the pretest. They filled in the same set of questionnaires for the follow-up assessment 1 month after the posttest in the center right before the start of the class, on the first day they attended the Satir workshop.

The Consolidated Standards of Reporting Trials (CONSORT) diagram for the flow of the study.
The number of dropout (n = 1 for each group) and lost to follow-up (n = 2 for each group) were the same across the groups. In addition, one subject in the wait-list control group missed the posttest assessment.
Intervention
The intervention is in the form of an experiential workshop comprises of three and a half consecutive days of 21 hr, which includes some meditation sections on the last 2 days. It is based on the Satir model with the emphasis on strengthening self-awareness and self-esteem as well as facilitating congruent communication. By learning to be more aware of own inner experience, one could obtain a better understanding of themselves and others, which could help develop and maintain a more satisfying relationship with the self and others. All the workshops were conducted by the same trainer with more than 30 years of experience in Satir model and helpers who have received substantial training in the Satir model. The content of the workshop is described as follows.
Day 1 (Lecture: 7–10 p.m.): Warm up and team building. Subjects were instructed to walk around the treatment room, get familiar with the environment, and introduce themselves to each other. A sharing exercise was followed, participants were asked to share something interesting about their names, a happy event in their childhood, and three strengths of themselves. The first day workshop was ended with a debriefing section and participants shared their expectations toward joining the workshop before they left.
Day 2 (Lecture:10 a.m.–5:30 p.m.; Group discussion: 5:30–9:30 p.m.): Coping stances and primary triad. Normal patterns that are usually presented by people under stress were introduced to the participants. Explanation on the four coping stances: placating, blaming, being superreasonable, and being irrelevant was provided to the participants. A role-play game was followed, each participant played a role in a family to plan for a coming family trip, while each of them was instructed to use different coping stances. The concept of primary triad that explains how people were made in a family was introduced to the participants. A sharing section was followed; participants were asked to share their own experiences in primary triad as being the child in a family. The second day workshop was ended with a debriefing section summarizing what had been learnt from the day.
Day 3 (Lecture:10 a.m.–5:30 p.m.; Group discussion: 5:30–9:30 p.m.): Iceberg and congruence. Participants were guided to meditate and think about their own journey from birth to present and recall the abilities that they had developed. The iceberg–metaphor of personal internal world was then introduced to the participants. A demonstration on how different parts of iceberg could be achieved was delivered. In the second half of the section, the idea of congruence was introduced. A small group activity was followed; participants were asked to practice congruent communication in groups of three (the learning trio). Participants were guided to draw family map; the idea of family rules and the transformation of family rules were introduced. The concept of family reconstruction was introduced; participants were instructed to prepare for the family reconstruction activity on Day 4.
Day 4 (Lecture: 10 a.m.–5:30 p.m.): Family reconstruction. Participants were guided to meditate about the growth of parents. A role-play exercise was followed, one participant was chosen as the “Star” to experience family reconstruction. The “Star” invited the other participants as the role-players as the “Star” family members. The rest of the participants observed the role-play exercise and learnt the family reconstruction process demonstrated by the “Star” family. Small group discussion and reflection were followed, which was facilitated by helpers. Temperature reading—a communication tool that consists of appreciation, puzzle or concern, complains with recommendations, new information, hopes, and wishes—was introduced to the participants. A sharing section on learning experience in the workshop and a debriefing section were carried out to end the workshop.
Control Condition
We adopted a passive control condition, in which the participants were on the waiting list for a period of 1–2 months. No intervention was provided at that period of time, but the participants would join the workshop after this waiting period.
Measures
PSTS-17
The PSTS-17 in Chinese is a reliable and valid measure for the core values in the SGM for the Chinese population in Hong Kong (Leung et al., 2019). The PSTS-17 assesses four dimensions related to Satir’s therapeutic approaches, namely, self-awareness, self-doubt, others-oriented, and openness to share. It is rated with a 6-point Likert-type scale, ranging from 6 (strongly agree) to 1 (strongly disagree). High scores indicate great extent of the characteristics in the total and subscales of the PSTS-17, except that high scores indicate less extent of self-doubt. Sample questions are: “I am aware of my emotional responses when facing stress,” “When I have some negative feelings (e.g., anger, anxiety, fear), I don’t like myself,” “I try to avoid facing conflicts,” and “I tell others my worries and puzzle.” The Cronbach’s α of the PSTS-17 in this studied cohort was .678, indicating an acceptable reliability. The Cronbach’s αs of self-awareness, self-doubt, others-oriented, and openness to share subscales were .74, .85, .78, and .82, suggesting a good reliability. The test–retest reliability was examined by Pearson’s correlation analysis on T1 and T3 data. Significant correlations were observed in PSTS-17 (r = .681, p < .001), self-awareness (r = .618, p < .001), self-doubt (r = .751, p < .001), others-oriented (r = .549, p < .001), and openness to share (r = .624, p < .001).
Rosenberg Self-Esteem Scale
We measured self-esteem using Rosenberg Self-Esteem Scale (Rosenberg, 1965). The validated Chinese version of this scale was used in the current study (Tsang, 1997). It consists of 10 items using a 4-point Likert-type scale ranging from 1 (strongly agree) to 4 (strongly disagree). The higher the score, the higher the self-esteem. Sample questions are: “I feel like a person who has a number of good qualities,” “I certainly feel useless at times.” The Cronbach’s α of the Rosenberg Self-esteem Scale in this studied cohort was .86, indicating a good reliability. There was evidence on the test–retest reliability of Rosenberg Self-Esteem Scale (r = .790, p < .001; T1 vs. T3).
General Health Questionnaire (GHQ-12)
We measured metal health status using a short form of GHQ-12 in Chinese (Pan & Goldberg, 1990). It is the most commonly used assessment tool for common mental disorders, in addition to being a general measure of psychiatric well-being. It consists of 12 items using a 4-point Likert-type scale. The higher the score, the higher the level of psychiatric impairment. Sample questions are: “Have you recently lost much sleep over worry,” “Have you recently been able to face up to your problems,” and “Have you recently been feeling unhappy and depressed.” The Cronbach’s α of the GHQ-12 in this studied cohort was .93, indicating an excellent reliability. There was evidence on the test–retest reliability of GHQ-12 (r = .593, p < .001; T1 vs. T3).
The spirituality subscale of the Body-Mind Spirit Well-Being Inventory (S-BMS-13)
We measured spirituality using the spirituality subscale of the Chinese version of S-BMS-13 (Ng, Yau, Chan, Chan, & Ho, 2005). It consists of 13 items with three distinct components: tranquillity, disorientation, and resilience, using a 11-point Likert-type scale ranging from 0 (totally disagree) to 10 (totally agree). It evaluates the subject’s core values, philosophy, and the extent to which life is being meaningful. High scores indicate high levels of spirituality. Sample questions are: “I have lost direction in life,” “I lack the vitality of life,” and “I can take something up, or let go of it.” The Cronbach’s α of the S-BMS-13 Scale in this studied cohort was .86, indicating a good reliability. There was evidence on the test–retest reliability of S-BMS-13 (r = .715, p < .001; T1 vs. T3).
The Chinese Affect Scale (CAS)
We measured the positive and negative affects using the CAS (Hamid & Cheung, 1996). It consists of 10 items for positive affect (e.g., excited, energetic) and 10 items for negative affect (e.g., sad, nervous) using a 5-point Likert-type scale, which rates the frequency of occurrence of positive and negative affects from 0 (not at all) to 4 (all the time). The Cronbach’s α of the positive and negative affects in this studied cohort were .87 and .87, respectively, indicating a good reliability. There was evidence on the test–retest reliability of CAS (PA: r = .462, p < .001; NA: r = .483, p < .001; T1 vs. T3).
Statistical analysis
An intention-to-treat analysis approach was adopted in this study. Missing data were completely at random and were handled by last observation carried forward method. Average scores were reported for each measure. The normality of data distribution from each group at each time point was confirmed by Shapiro–Wilk test. Data that were not normally distributed, including positive affect, negative affect, self-esteem, GHQ-12, and S-BMS-13, were transformed using a two-step transformation approach (Templeton, 2011). Normality of the transformed data was tested once again before doing any parametric analysis. Enhanced normality using the two-step transformation method was reported to improve the normality of residuals (Templeton, 2011) that is required to fulfill one of the assumptions for carrying out two-way analysis of covariance (ANCOVA) with repeated measures (will be mentioned again below). Therefore, transformed data were used.
Demographic data were examined using independent t test (two-tailed), χ2 statistic or Mann–Whitney U test, where appropriate. Pretreatment differences of all the behavioral measures were examined by independent t test (two-tailed). The Group × Time interaction effect was determined using two-way ANCOVA with repeated measures, controlling for the effect of age. For data that violated the sphericity assumption, Greenhouse-Geisser correction was applied. For any significant Group × Time interaction, post hoc analysis was performed in the intervention group using paired t test. The effect size was calculated using partial eta-squared (
To further examine the role of self-transformation in the relationship between positive affect/negative affect and mental health problems, mediation analyses were performed in the experimental group (n = 52) using Model 4 in the PROCESS macro v3.0 for SPSS (Hayes, 2013). Changes in the score (T2 − T1) of positive affect or negative affect (predictors) and changes in the score of PSTS-17 (mediators) after the intervention were entered in the linear regression models to predict changes in the score of GHQ-12 (outcome measures). The effect of age was adjusted by including it as a covariate in the regression models. The PROCESS macro is based on ordinary least squares regression and adopts a nonparametric bootstrapping procedure (5,000 bootstrapped samples in this study), which gives rise to a bias-corrected confidence interval (CI) for effect size inference (Shrout & Bolger, 2002). The presence of a significant effect is denoted if zero is not included by the upper and lower bound of 95% CI (Preacher & Hayes, 2008).
All statistical analyses were performed using IBM SPSS Statistics 23. Statistically significance is indicated by p < .05. In particular, Bonferroni correction was applied to correct for multiple comparison for ANCOVA (p < .005 was defined as significant for a total of 10 comparisons including the four subscales of PSTS-17).
Results
Treatment Outcomes
Hypothesis 1: Improvement in self-transformation–the primary outcome
There were no significant between-group differences in the total score of self-transformation and its subscales at pretreatment time point (T1). There were significant Group × Time interaction effects on the total score of self-transformation (
Group-by-Time Training Effect.
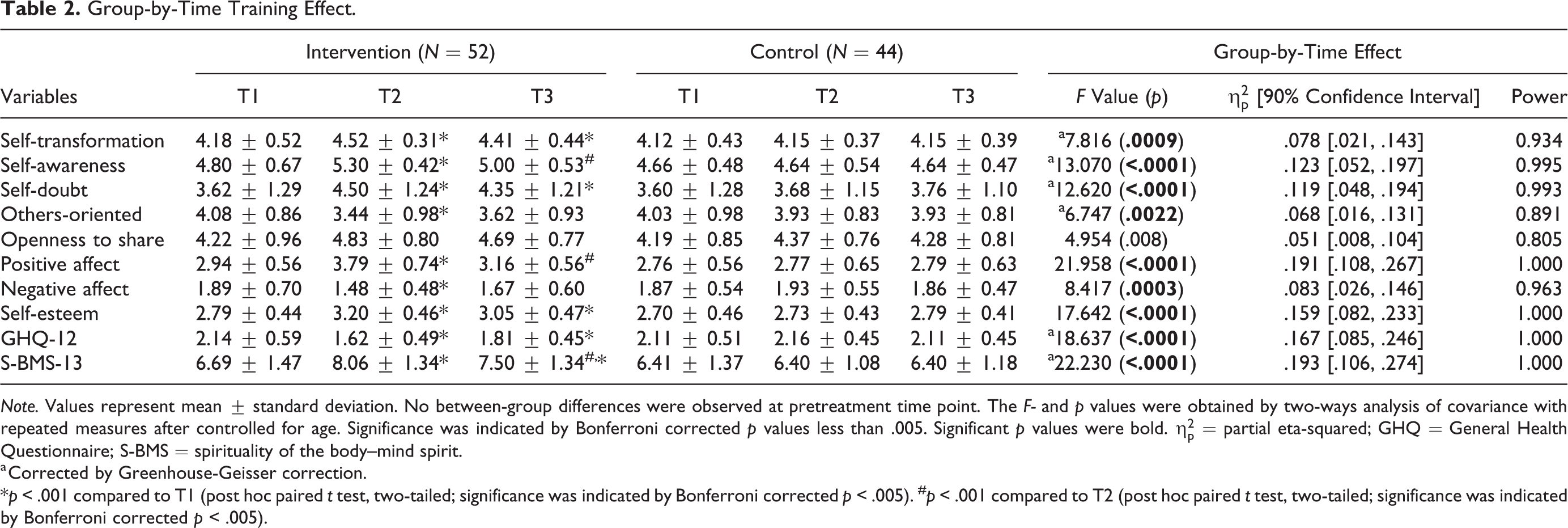
Note. Values represent mean ± standard deviation. No between-group differences were observed at pretreatment time point. The F- and p values were obtained by two-ways analysis of covariance with repeated measures after controlled for age. Significance was indicated by Bonferroni corrected p values less than .005. Significant p values were bold.
a Corrected by Greenhouse-Geisser correction.
*p < .001 compared to T1 (post hoc paired t test, two-tailed; significance was indicated by Bonferroni corrected p < .005). # p < .001 compared to T2 (post hoc paired t test, two-tailed; significance was indicated by Bonferroni corrected p < .005).
Post hoc analyses were conducted on the intervention group for outcome measures with significant interaction effects. Results indicated that increased levels of self-transformation (η2 = .308), self-awareness (η2 = .401), and decreased levels of self-doubt (η2 = .366) that is indicated by increased scores for this subscale and others-oriented (η2 = .220) after intervention were all significant (p < .001). There were no significant changes in self-transformation, self-doubt, and others-oriented from posttest (T2) to follow-up (T3), whereas the decreases in self-awareness were significant (p < .001) from T2 to T3. Although a general diminution of the training effect on self-transformation and its subscales was observed in the intervention group after 1 month, the total scores of self-transformation at the follow-up time point were still significantly higher than that at pretreatment time point. In particular, there was a significant improvement in self-doubt at the follow-up time point compared to that at the pretreatment time point (Table 2).
No significant changes in the total score of self-transformation and its subscales across the studied time points were observed in the control group (Table 2).
Hypothesis 2: Changes in affects, self-esteem, spirituality, and mental health problems—the secondary outcomes
There were no significant between-group differences in positive affect, negative affect, self-esteem, spirituality score, and mental health problems at the pretreatment time point (T1). Significant Group × Time interaction effects on positive affect (
Post hoc analyses on the intervention group indicated that increases in positive affect (η2 = .557), self-esteem (η2 = .538), and spirituality (η2 = .473) score and decreases in negative affect (η2 = .293) and mental health problems (η2 = .386) after the Satir workshop were all significant (p < .001). The reduction of positive affect and spirituality from T2 toT3 was significant, in which the score of positive affect at follow-up became comparable to that at pretreatment time point, whereas the spirituality score at the follow-up time point remained higher than that at the pretreatment time point. On the other hand, the training effects on self-esteem and mental health problems were maintained at the follow-up time point, which were significantly improved compared to that at the pretreatment time point. Nonetheless, the diminution effects observed for these measures at follow-up were apparently partial (Table 2).
No significant changes in the secondary measures across the studied time points were observed in the control group (Table 2).
Hypothesis 3: Mediating role of self-transformation in the relationship between changes in affects and mental health problems
The regression model that included changes in the score of negative affect, self-transformation, and age in predicting mental health problems (GHQ-12) was significant (F = 8.433, R 2 = .345, p = .0001, n = 52). Both changes in negative affect (β = .278, p = .032) and self-transformation (β = −.128, p = .006) had a main effect on changes in mental health problems, after controlling for the effect of age in a linear regression model. The direct effect of changes in negative affect on changes in mental health problems was significant (β = .278, p = .032); the indirect effect of changes in negative affect on changes in mental health problems through changes in self-transformation was also significant (β = .163, 95% CI [.040, .343]). These findings suggest that self-transformation is a significant mediator for the relationship between negative affect and mental health problems, in which the influence of negative affect on mental health problems is partially mediated via the effect of self-transformation (Figure 2; Table 3).
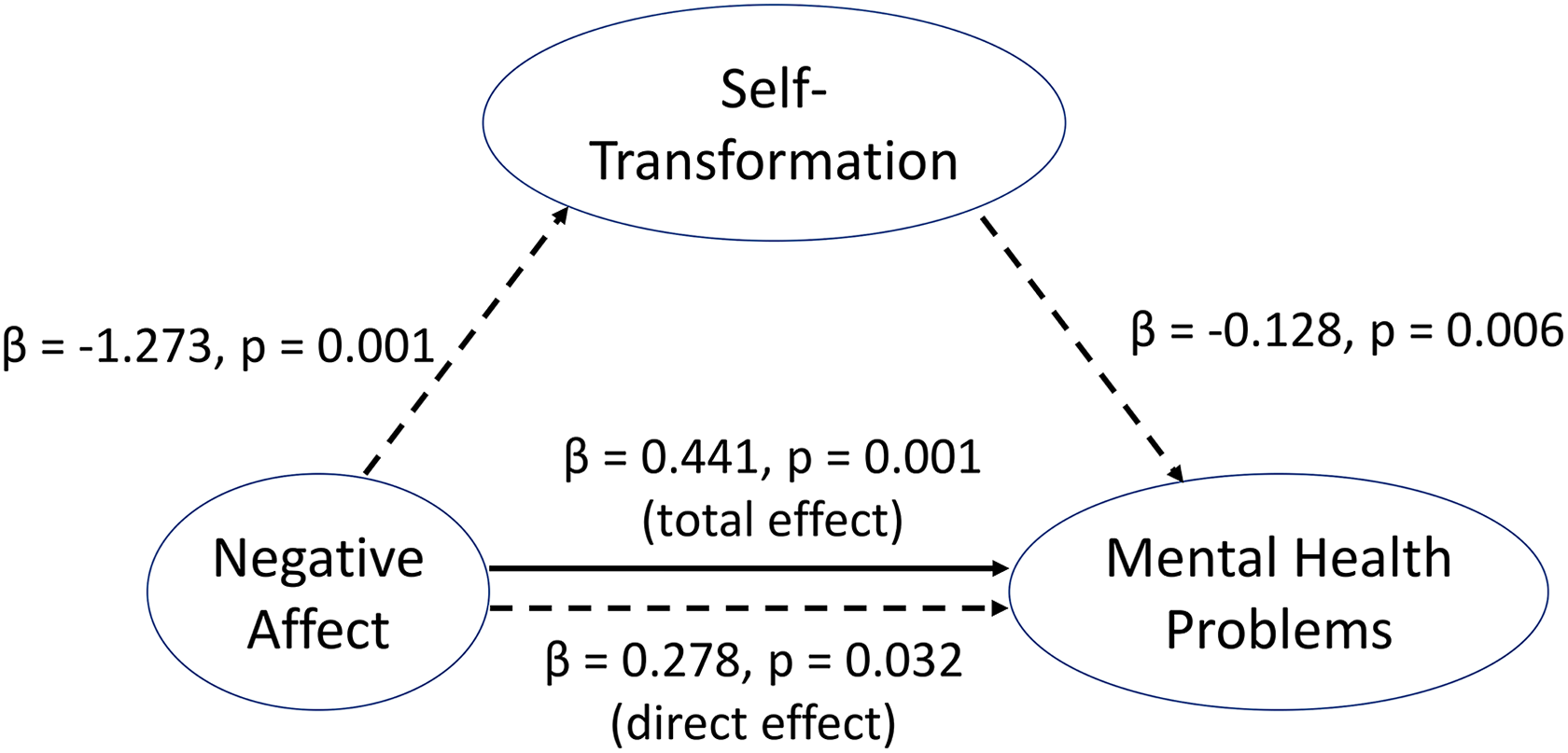
The mediation pathway for the relationship among changes in negative affect (predictor), self-transformation (mediator), and mental health problems (outcome). The indirect effect of changes in negative affect on changes in mental health problems through changes in self-transformation was significant (β = .163, bootstrapped 95% confidence interval [.035, .343]), adjusted for the effect of age.
Mediation Role of Changes in Self-Transformation on the Relationship Between Changes in Negative Affect and Mental Health Problems.

Note. NA = not available; SE = standard error; GHQ = General Health Questionnaire; PSTS = Perceived Self-Transformation Scale.
a Values were obtained from 5,000 bootstrap samples.
On the other hand, the association between changes in positive affect and changes in self-transformation was nonsignificant (r = .268, p = .055, n = 52); therefore, mediation effect of changes in self-transformation on the relationship between changes in positive affect and mental health problems was not tested.
Discussion and Applications to Practice
Our findings demonstrate that the participants in the intervention group, who underwent a total of 21 hr of SGM-based workshop, experienced substantial degrees of self-transformation. The subdomains of self-transformation improved after intervention, including increased levels of self-awareness, as well as decreased levels of self-doubt and others-oriented, although the Group × Time interaction effect on openness to share was only marginal. All these improvements in the intervention group were maintained for 1 month after the Satir workshop, except that there was a reduction in the levels of self-awareness at follow-up. Nonetheless, their levels of self-awareness at follow-up were still higher than that at pretreatment time point. The results provide some evidence to support our first hypothesis that the Satir workshop could facilitate the cultivation of self-transformation. In addition, for the intervention group, improvements extended to the secondary outcomes, which include increased positive affect, self-esteem, and spirituality and reduced negative affect and mental health problems, immediately after the Satir workshop. Although these beneficial training effects significantly diminished as time passed after intervention, these measures at follow-up were still significantly better than that at pretreatment time point except for positive affect. This suggests that the diminution effects were only partial except for positive affect. As expected, there were no changes in the control group at any time point. These findings support our second hypothesis that the Satir workshop could improve affects, self-esteem, spirituality, and mental health problems. Findings from the mediation analysis demonstrate that improved self-transformation after Satir workshop is a significant mediator of the relationship between reduced negative affect and mental health problems in the intervention group, suggesting that self-transformation could be a modifiable factor for tackling mental health problems, which supports our third hypothesis. Findings of this study provide preliminary evidence on the effectiveness of the SGM-based intervention on improving mental well-being.
The positive effects of SGM-based intervention observed on the primary and secondary outcomes in this study corroborate the only published study that also demonstrated improvements following a SGM-based group counseling (Der Pan, 2000). In particular, they focused on family relationships while we focused on personal growth and mental well-being. We both found that the improvements after intervention were maintained at follow-up. Specifically, in our study, only the positive effects on primary outcomes could be maintained despite some reductions in self-awareness. In addition, the sample size for each group in our study was at least double compared to that in Der Pan’s (2000) study. Therefore, we had a stronger power to detect significant changes after intervention, which may be particularly important for capturing intangible intrapsychic changes induced by the SGM-based workshop. Overall, both Der Pan’s (2000) and our studies provide supportive evidence toward the effectiveness of SGM in bringing positive changes to individuals.
The positive changes we observed in the intervention group may be explained by the fact that our SGM-based workshop provided a series of opportunities for the participants to connect with their own inner experience, which built an important foundation to support transformation in the self and changes in relationship with others. Also, the supportive and positive atmosphere that was established at the beginning of the workshop facilitated the members to engage in the process of change (Satir et al., 1991). Enhanced self-awareness allows ones to attend to their own feelings and become aware of their inner experiences. By connecting to the deeper underlying dimensions of one’s behaviors, such as feelings, perceptions, expectations, and yearnings, a person could gain a better understanding of the intrapsychic forces that helps one make better choices for oneself. This may also affect his or her communication patterns with others (Satir et al., 1991). Furthermore, changes detected by the self-doubt subscale, such as becoming more willing to acknowledge one’s negative feelings, indicate that the transformation process had taken place (Leung et al., 2019). It is because acknowledging and accepting one’s negative feelings or emotions is the key emphasis of the Chaos stage in the transformation process of the Satir model (Satir & Baldwin, 1983). In fact, it is typical to reexperience this Chaos stage when the participants tried to practice what they had just learnt from the workshop in their daily lives. This may explain for the general reductions in self-transformation scores at follow-up, of which the diminution effect was relatively more obvious to the self-awareness than the other three subscores. Nonetheless, the total self-transformation score and the subscores for self-doubt, others-oriented, and openness to share at follow-up remained similar to that right after the workshop. These observations support the viewpoint that changes associated with self-transformation are enduring (Brubacher, 2006; Satir et al., 1991).
Although the Group × Time interaction effect on openness to share was at trend level based on the statistical significance defined in this study, it is possible that this factor may require much more time and effort to be substantially changed, especially in the Chinese society. A previous review written by family counselors in Hong Kong highlighted the extreme difficulty for participants in Hong Kong to share private intimate thoughts with other participants during therapy session because of the hidden cultural rule to keep feelings inside oneself and not to express to others (Cheung & Chan, 2002). Nonetheless, there was a clear trend that participants in the intervention group showed higher levels of openness to share after the intervention. Future studies should employ a longer term of SGM-based intervention in order to verify our results.
The positive changes in the secondary outcomes right after the Satir workshop in the intervention group were also in line with our expectations. It has long been believed especially by practitioners who follow the SGM method that the SGM method works for many individuals (Wretman, 2016). Our quantitative study provides evidence to further support this long-standing faith. Higher self-esteem, which is an important goal and a core element of SGM therapy (Wretman, 2016), has been shown to impose unique contributions on influencing affects and mental health problems such as depression (Orth, Robins, & Widaman, 2012). Furthermore, it was previously shown that positive affect positively correlated with family satisfaction (Carruth et al., 1997), while parental depression negatively correlated with partner relationships (Ramchandani et al., 2011), family functioning, and youth well-being (Pakenham & Cox, 2012). Therefore, the enhanced self-esteem, improved affect, and reduced mental health problems after the SGM-based workshop may have potential implications on up-regulating family health and relationships, in which future studies should verify this speculation. However, these positive effects significantly diminished after the completion of the workshop. The degree of diminution in the secondary measures was greater than that in most of the primary measures. This is in line with the prediction based on the Satir model that reduction of dysfunctional symptoms is not as enduring as changes associated with self-transformation (Brubacher, 2006; Satir et al., 1991). In particular, the level of positive affect even returned to the pretreatment time point level at follow-up. It remains unclear whether a modified Satir workshop with a stronger intensity or longer treatment duration could improve the sustainability of these positive changes. This requires future studies to confirm. Nonetheless, our findings suggest that the intensive Satir workshop that was conducted in 31/2 days could induce a large effect (
Negative affect was broadly and generally associated with symptoms and diagnosis of mental disorders such as depression and anxiety, which made it a general predictor of mental health problems and psychiatric disorder. On the other hand, positive affect was consistently and more specifically in predicting symptoms and diagnoses of depression (Watson et al., 1988). We found that both negative and positive affect and mental health problems assessed by CAS and GHQ-12, respectively, were improved after the intensive workshop. In addition, the association between reduced negative affect and mental health problems was partially mediated through the increase in self-transformation after the intervention, indicating that self-transformation could be a good modifiable factor for tackling negative affect-induced mental health problems.
To conclude, our preliminary findings suggest that the SGM-based workshop could bring about positive influences toward participants’ mental well-being and self-transformation. Self-transformation may be a good modifiable factor that can be cultivated via SGM-based intervention to ameliorate negative affect-induced mental health problems. Our findings support the effectiveness of the SGM-based intervention.
There are several limitations in the current study. First, the inclusive bias for sampling is unavoidable in the current study, which limits the interpretation of our findings. Our studied subjects were highly educated, predominantly women, and had a high motivation in the Satir workshop. Although a randomized approach was adopted to minimize such a bias, future studies are warranted to confirm our findings in a more generalized population. Second, all data collections relied on self-reported questionnaires in the current study, in which objective measures on the desired outcomes were absent. Given subjective measures may be more relevant to reflect self-perceived changes favorable to oneself, subjective biases might occur, for example, social desirability effects. Future studies should consider incorporating both subjective and objective measures on self-transformation and well-being, as well as including social desirability bias assessments, for example, Marlowe–Crowne Social Desirability Scale and Balanced Inventory of Desirable Responding (Leite & Beretvas, 2005) to control for the effect. Last, due to the limited resources, an active control group was missing in the current setting. The effect of social interaction during the workshop on outcome measures and the placebo effect due to the subject’s expectations on the workshop cannot, therefore, be ignored. Future studies may include an active control group to minimize the effect of these confounding factors.
Supplemental Material
Supplementary_Table_1 - Effects of the Satir Model on Mental Health: A Randomized Controlled Trial
Supplementary_Table_1 for Effects of the Satir Model on Mental Health: A Randomized Controlled Trial by Way Kwok-Wai Lau, Pamela Pui-Yu Leung and Catherine Lai-Ping Chung in Research on Social Work Practice
Footnotes
Authors’ Note
This project was not preregistered in a clinical trials registry. The pretreatment data have been used in a previous publication (Leung, Lau, & Chung, 2019).
Acknowledgments
The authors wish to thank Dr. John Banmen and Dr. Marie Lam for their valuable advice and the staff of the Hong Kong Satir Center for Human Development and others who have helped in the various phases of the study for their contributions to the project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Hong Kong Satir Center for Human Development.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.