
Abstract
Purpose:
There is scant child welfare research on parenting interventions for parents with intellectual and developmental disabilities (I/DD). This mixed-methods research examined client participation in an in-home parenting intervention, including client characteristics, which clients benefit most from participation, and key aspects of program participation.
Method:
The sample included participant program records, client satisfaction surveys, stakeholder interviews, and a staff focus group. The quantitative data were analyzed using growth curves and binary logistic regression. The qualitative data were analyzed using thematic analysis.
Results:
Time spent in Project Improving Parenting Achievements Together was predictive of improvement in parenting skills and the home environment and reduction in the odds of out-of-home placement for children of parents with I/DD. The intensity of services, tailored education, community engagement, and client–worker relationship were the key aspects of program participation.
Discussion:
With proper supports, parents with I/DD can learn parenting skills, improve the home environment, and keep their family intact.
Keywords
An estimated 2.3% of parents in the United States have an intellectual and developmental disability (I/DD; Kaye, 2012). Research shows that children of parents with disabilities are at high risk for allegations of child maltreatment, foster care placement, and termination of parental rights, the first step in freeing children for adoption (Booth & Booth, 2004; DeZelar & Lightfoot, 2018; McConnell et al., 2020; White, 2015). Additionally, children of parents with I/DD are disproportionately represented in foster care compared to children of parents with other disabilities.
Foster care, while sometimes necessary to ensure children’s safety, has been associated with long-term negative outcomes. Compared to the general population, foster youth experience higher rates of substance abuse, criminal behavior, mental health disorders, and physical health conditions including increased morbidity and mortality, among many others (Okpych & Courtney, 2014; Rebbe et al., 2018). Foster youth also experience higher rates of suspension from school, expulsion, and dropout, which can contribute to ongoing socioeconomic disadvantage into adulthood (Ferguson & Wolkow, 2012; Okpych & Courtney, 2014).
In recent years, there have been efforts to bring awareness to the unique service needs of parents with I/DD involved in child welfare; however, there are “few formal programs supporting parents with disabilities and little funding sources to pay for formal or informal parental supports” (Lightfoot & LaLiberte, 2011, p. 5). Researchers in the UK conducted a systematic review of research on interventions to promote social supports and parenting skills in parents with I/DD (Wilson et al., 2014). They found a limited number of outcome studies (n = 7) in their review; however, there was some evidence that intensive behaviorally based interventions may be effective in developing positive parenting skills (Wilson et al., 2014).
This study contributes to the literature focused on specialized parenting interventions for parents with I/DD by examining the experiences and outcomes of parents with I/DD who participated in Project Improving Parenting Achievements Together (IMPACT),, an intensive in-home parenting program for parents with I/DDs at risk for child removal and placement in foster care. Specifically, it examines the characteristics of clients who participate, the clients who benefit most from participation, and stakeholders’ views of the key components of the program.
Literature Review
According to the U.S. Department of Health and Human Services, approximately 674,000 children, aged <1 to 18 years in the United States experienced child maltreatment in 2017, and 442,995 children were placed in foster care (U.S. Department of Health & Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau, 2019). Child maltreatment is associated with increased risk for negative health outcomes across the life span including those related to emotional and behavioral health, cognitive development and achievement, and educational attainment (Merrick & Latzman, 2014). In addition, foster care placement is associated with negative outcomes into adulthood, such as higher rates of substance abuse, criminal behavior, mental health disorders, and poor physical health, as compared to the general population (Okpych & Courtney, 2014; Rebbe et al., 2018).
Research shows that children of parents with I/DD are at high risk for child welfare involvement. Studies estimate that 10%–15% of child welfare cases include at least one parent with I/DD (Booth & Booth, 2004; McConnell et al., 2011), and The California Evidence-Based Clearinghouse for Child Welfare (2019) reports parents with I/DD as a high-risk group, as up to 22% of parents with cognitive disabilities have child welfare involvement at some point. The National Council on Disability (2012) estimates that between 40% and 80% of parents with I/DD will lose custody of their child at some point. Using data from the 2010 American Community Study, Kaye (2012) reported that 1.5 million parents of children in the United States have an I/DD; however, researchers caution that due to poor identification, assessment, and reporting of I/DD, it is difficult to determine exactly how many children of parents with I/DD are involved in child welfare cases, and the known proportion of cases is likely underreported (LaLiberte & Lightfoot, 2013).
Risk Factors for Child Welfare Involvement Among Parents With I/DD
Research on parents with I/DDs demonstrates that this population is more likely to become involved with the child welfare system if they are female, African American, Native American/Alaska, and/or living in poverty (LaLiberte et al., 2017). Indeed, there is evidence of disproportionality and disparity by race/ethnicity in the child welfare system more generally, with an overrepresentation of Native American/Alaska Native and African American children at all decision-making points in child welfare cases (U.S. Department of Health & Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau, 2016).
LaLiberte et al. (2017) found that when race, gender, and poverty were controlled for, parents with I/DD were still more likely to be involved with Child Protective Services (CPS) and to experience termination of parental rights compared to parents without intellectual disabilities. In addition to demographic characteristics, others have investigated the ecological and social factors contributing to child welfare involvement among this population. These factors include high rates of poverty, housing instability or homelessness, substance use, mental health issues, domestic violence, and low levels of social support among parents with I/DD (Monsen et al., 2011; Slayter & Jensen, 2019).
In order to account for disparities in child welfare involvement for parents with I/DD, studies have examined maltreatment rates and trends among this population. Findings largely indicate parents with I/DD are more likely to become involved with child welfare agencies due to neglect rather than other forms of maltreatment (Azar et al., 2012; Slayter & Jensen, 2019; Tymchuk & Andron, 1990). Furthermore, while neglect is more likely to occur in cases when parents have I/DD, both physical and sexual abuse are less likely to occur in this population compared to their peers (Slayter & Jensen, 2019).
Other research suggests that parents with I/DD may be discriminated against based on their disability status, which violate their rights under Section 504 of the Rehabilitation Act and the American Disabilities Act requiring programs and services to be modified to accommodate the needs of individuals with disabilities (National Council on Disability, 2012).
In addition, several states still include disability as a ground for termination of parental rights in child dependency proceedings (National Council on Disability, 2012). This may place parents with I/DD at a disadvantage, as it posits that individuals with I/DD are incapable of parenting children safely (HHS Press Office, 2019; National Council on Disability, 2012).
Services to Promote Positive Parenting Among Parents With I/DD
There is a scant literature on evidence-based practices for parents with I/DD, and programs tailored to the unique needs of parents with I/DD are limited (Lightfoot et al., 2018; Slayter & Jensen, 2019). As a result, child welfare professionals often lack an understanding of the unique service needs of this population, particularly in the absence of specialized training for working with this population (Lightfoot et al., 2018; Slayter & Jensen, 2019). Despite limited research, a systematic review that included seven studies of interventions designed to assist parents with I/DD found that intensive behavioral programs may be effective at developing positive parenting skills (Wilson et al., 2014).
Existing programs for parents with I/DD include parent education kits, parent support groups, navigation services, and home visiting programs such as Step-by-Step and Positive Parenting (The California Evidence-Based Clearinghouse for Child Welfare, 2019). Parent education kits often include lesson plans, modules, and parent workbooks with topics such as recognizing when a child is sick, calling the doctor, using medicines safely, and identifying dangerous objects in the home. In contrast, parent navigation services include more services in addition to parenting materials. As an example, the Disabled Parenting Project (https://disabledparenting.com) includes a resource directory for parents with disabilities, blogs, opportunities to connect to the community, and adaptive parenting products.
Another intervention used to support parents with I/DD is home visiting programs. Typically, home visiting programs include components fostering parent–child interactions, childcare, child development, home safety and management, and problem-solving (The California Evidence-Based Clearinghouse for Child Welfare, 2019). One such program listed on the California Evidence-Based Clearinghouse for Child Welfare is Project IMPACT, an intensive in-home behaviorally based parent training program designed for parents with I/DD who are at-risk for foster care placement and who have open child welfare cases. In a preliminary study, individuals who completed Project IMPACT saw statistically significant improvements in several domains including childcare skills, managing a household, and parent–child interactions (Rao, 2013). Additionally, 1 year after program completion, 97% of families for whom data were available remained intact (Rao, 2013).
Study Rationale
There is limited research focused on the experiences and outcomes of interventions designed for parents with I/DD involved in child welfare. This study expands upon Rao’s (2013) study of Project IMPACT utilizing a larger sample size, looking at different outcomes, and assessing the acquisition of parenting skills over time. Using a mixed-methods design, it answers the research questions (RQs): (1) What are the characteristics of clients referred to the program? (2) Which clients benefit most from participation? and (3) What do stakeholders report as the key aspects of program participation? The first two RQs were answered using quantitative methods, while the third employed qualitative methods. Taken together, this study provides a more robust examination of Project IMPACT than previously published.
Method
The study was an academic–community partnership consisting of researchers from Boston University’s School of Social Work, Montclair State University Department of Social Work and Child Advocacy, and child welfare practitioners from the Westchester Institute for Human Development (WIHD). The study protocol was approved by the institutional review boards of all three institutions. The authors report no known conflicts of interest. The study received pilot funding from Boston University’s Center for Innovation in Social Work and Health 2018 Innovation Pilot Funding Grant, which funds a 1-year, cross-disciplinary project focused on social work and health, led by a Boston University faculty member.
Study Site
Project IMPACT was developed at WIHD in conjunction with the Westchester County Department of Social Services (DSS) in New York State. Project IMPACT is administered by WIHD, and clients are referred from DSS. Project IMPACT aims to (1) identify risk and protective factors for each client served, (2) provide specialized parenting education and training to promote healthy child development, and (3) prevent children from entering or reentering foster care.
Clients participating in the program receive specialized services in their homes from a master’s level social worker under the supervision of a clinical psychologist three times per week for 4–6 months. Services are tailored to the individual needs and strengths of the client, their family situation, and their children’s developmental needs. Topics covered include parent–child interaction skills, basic childcare, child development, home/health safety, home management, parent advocacy, and problem-solving/planning skills. The intervention uses a combination of verbal instruction, visual aids, modeling, and hands-on practice to develop parenting skills and knowledge. Parenting assessments are collected at intake, when skills are taught at discharge and 3 months postintervention.
Sampling
All clients (N = 133) enrolled in the program between 2006 and 2017 and who attended at least one session were included in the quantitative sample. Clients (n = 99) who completed the program completed a client satisfaction survey at discharge. Their DSS workers (n = 59) also completed a program satisfaction survey. In addition, semistructured interviews were held with 6 DSS workers, and a focus group was held with 3 Project IMPACT social workers, herein referred to as PI clinicians.
Data Collection
Quantitative phase—measures
Clinical data mining, a form of research that uses existing agency records to integrate practice and program evaluations (Epstein, 2010), was used to extract data from the files of all 133 clients who participated in Project IMPACT between 2006 and 2017. In the process of preparing data for analysis, data were validated by Project IMPACT staff if any measures were found to contain extreme values. In those cases, and this was done approximately 20 times, clinicians went back into client files to verify the information provided to the research team, and any corrections were made. Approximately three errors in some measure were found randomly. All other data were correct as originally reported. Additional child welfare outcome data were obtained for these clients from the County’s DSS.
Demographic and programmatic information
Parent and child demographic information was collected at intake. These included parental age, preferred language, race/ethnicity, whether there were previous CPS reports aside from the current one, whether children were ever placed in out-of-home care, whether the parent had involvement with the State’s Office for People with Developmental Disabilities, whether the client had previously taken parenting classes, the parent’s IQ, whether the client had a history of mental health problems, whether the client had a history of domestic violence, how many other services the client was receiving, the ages of each child in the client’s family, how many children were in the client’s family, and how many of the children had a history of developmental disabilities or special needs. Programmatic data included who the worker was providing services, the length of time enrolled in Project IMPACT, and, if the client ended the program prematurely, the reasons for doing so. Each client’s index child was selected based on how difficult the child was for the client to parent. The index child was each client’s most difficult child.
Parenting
The Skills Assessment for Parents with Intellectual Disability assessed clients’ parenting skills at the four time points described earlier. This instrument was recently validated in a study of parents with I/DD (Zeitlin et al., forthcoming). Parenting skills were measured by the clients’ social worker primarily through observing whether parents were able to demonstrate up to 113 behaviors associated with skills needed for safe parenting (e.g., knowing when and how to contact a doctor, recognizing and knowing how to decrease a child’s negative behavior) across three subscales: Parent–Child Interactions, Daily Life Skills, and Overall Safety. At baseline, coefficient α for the Parent–Child Interactions subscale was .81; for Daily Life Skills, it was .68; and for Overall Safety, it was .66. For each behavior, a score of 0 was given if the behavior did not apply or the parent was unable to demonstrate it correctly, and a score of 1 was given if the parent was able to demonstrate the skill. Additionally, a total parenting score for each client was obtained by taking a sum of each of the subscales.
Home environment
The Home Observation for Measurement of the Environment (HOME) Inventory (Caldwell & Bradley, 1984) was used to measure the quality of the home environment at baseline, discharge, and 3-month follow-up. This instrument has been used in previous research with parents with I/DD. In this study, the HOME inventory measured parental acceptance of child behavior, opportunities for stimulation, and the physical environment of the home by the client’s social worker. Four versions of the HOME inventory exist and are based on child age. Scores were standardized across versions based upon the percentage of the total possible score achieved at each time point.
Child behavior
This research used the Child Behavior Checklist (CBCL; Achenbach & Ruffle, 2000) to assess both internalizing and externalizing behavior problems in clients’ children. This validated measure has two versions, one for preschoolers and one for school-aged children. The version most appropriate for each client’s index child was selected. In both versions, scores are standardized and compared to expected behaviors based on child age and gender. Standardized mean scores are set at 50 with a standard deviation (SD) of 10. Similar to the HOME inventory, child behavior was assessed at three time points.
Out-of-home care
One year after terminating from Project IMPACT, data were obtained for each client. If any of the clients’ children were placed in out-of-home care within that year, the client was flagged for foster care services with 0 = family remained intact and 1 = family had child(ren) placed in out-of-home care.
Data collection—qualitative phase
Qualitative data were collected to examine stakeholder perspectives on the key aspects of participation in Project IMPACT. Data included client and worker satisfaction surveys, interviews with DSS workers, a focus group with Project IMPACT staff, and informational interviews with the PI Director.
Between 2006 and 2017, client satisfaction surveys were administered to clients (n = 99) and DSS workers (n = 59) at the end of the program and included both quantitative and open-ended items. The client satisfaction survey was developed by the Director of Project IMPACT and used by the program to capture the perspectives of clients and workers. Domains included program participation, services received, satisfaction with services, relationship with the worker, and performance in the program.
To supplement the survey data, interviews were conducted between May 2019 and August 2019 with 6 DSS workers who referred clients to the program. The questions were developed by the first and second authors in consultation with Project IMPACT staff and the extant literature. Domains included how workers identify parents with I/DD; risk factors for children of parents with I/DD; decisions to refer to Project IMPACT; strengths and limitations of Project IMPACT services; knowledge, training, and support of DSS workers; and additional support services needed for clients. The Director of Project IMPACT emailed DSS staff who referred clients to the program describing the study and contact information for the first author. The interviews, held on the phone, were conducted by the first author and a trained PhD student. Prior to the start of the interview, participants were read a verbal consent form outlining the study purpose, risks, benefits, and voluntary participation. All participants voluntarily agreed to participate. The interviews lasted between 30 and 45 min, were audio-recorded, and transcribed verbatim. Interview participants were compensated with a US$25 Starbucks gift cards.
To gain the perspective of Project IMPACT clinicians, a focus group was held with all social work staff (N = 3) employed by Project IMPACT. The Director of Project IMPACT assisted in the recruitment and scheduling of the focus group but did not participate. The instrument was developed by the first and second authors in consultation with the Director of Project IMPACT and the extant literature. Questions covered a variety of topics including risk and protective factors for the client population, the role of the clinician, services provided, strengths and limitations of the program, and areas of improvement. The first and second author co-facilitated the focus group, held in person in a private room at the WIHD. Prior to the start of the focus group, participants were read a verbal consent form outlining the study purpose, risks, benefits, and voluntary participation. All participants voluntarily agreed to participate. The focus group lasted 1 hr, was audio-recorded, and transcribed verbatim.
Data analysis—quantitative phase
The first RQ was answered using univariate statistics to describe the characteristics of the sample. The second RQ was answered using growth curves and binary logistic regression. Growth curves were used to examine the degree to which two dependent variables changed over time: parenting skills and the quality of the home environment. Growth curves are a type of longitudinal analysis that can be used to study between-subject differences in within-subject change (Caldwell & Bradley, 1984). Fixed effects in these analyses were the mean trajectory of both parenting and home environment scores, while the random effects represent the variance of the individual trajectories around the mean. Competing models were assessed by comparing residuals, Bayesian information criteria, and Akaike information criteria (Curran et al., 2010).
Binary logistic regression, a form of statistical modeling based on the generalized linear model, is appropriate in predicting dichotomous outcomes at a single time point (Auerbach & Zeitlin, 2015). In this case, the outcome assessed was the absence or presence of out-of-home placement of children 1 year after concluding Project IMPACT.
Data analysis—qualitative phase
Data analysis was guided by the stages of thematic analysis (Braun & Clarke, 2012). The first author, with over a decade of child welfare practice experience and extensive experience conducting qualitative thematic analysis, and a trained doctoral student conducted the analysis. The first step consisted of reading through 10 open-ended survey responses, two interviews, and one focus group transcript and identifying initial codes related to the RQ3. The first author and the trained doctoral student coded each of these data sources independently. This initial coding process was inductive in nature, meaning that all codes were identified directly from the data sources without a priori determination. The research team then convened to discuss the initial codes emerging from the transcripts and resolve discrepancies in the researchers’ interpretation of the transcripts.
These initial codes were further consolidated into focused codes, which were then applied to the remainder of the open-ended survey responses and interviews, noting any new codes that were not accounted for. The research team then met again to discuss the focused codes and any new codes emerging from the remainder of the interview transcripts. During this process, the research team discussed diverging interpretations in the coding process and rereviewed all relevant transcript excerpts until the team arrived at a consensus. To account for researcher reflexivity, the doctoral student completed memos reflecting on the coding process, any differences in data interpretation among the research team, the consensus process, and outcomes generated by the team. The memos were used as an intermediary step between data analysis and developing the findings.
The final step included meeting together to discuss the focused codes across all data sources and to develop, define, and describe the salient themes. This included revisiting the data to identify illustrative examples and quotes. The iterative coding process identified four salient themes: intensive support services, tailored parenting curriculum, community engagement, and positive worker–client relationship. These themes were reviewed by all authors and agreed upon as distinct themes corresponding to distinct codes. To enhance credibility of the findings, the researchers met weekly throughout the coding process for peer review and debriefing sessions. The PhD student wrote memos that were then reviewed by the first author. They triangulated multiple data sources (interviews, surveys, and focus groups) and compared and contrasted their findings to the literature.
Results
Quantitative Results: RQ1
The participants in the sample were racially and ethnically diverse. The largest group (n = 62; 47.33%) identified as Black, non-Hispanic, and the next largest group identified as Hispanic (n = 52; 39.69%), with the remainder of the sample being White. The mean age of participants was 34.55 years (SD = 8.95).
The participants typically had previous child welfare involvement with nearly nine in 10 (n = 117) having a previous history with CPS and slightly over one quarter (n = 35; 26.72%) having a history of child removal. Nearly half the sample had previous parent training (n = 60; 49.59%). Slightly over one in 10 participants had involvement with the State’s Office for People with Developmental Disabilities (n = 14; 10.69%); however, the mean full-scale IQ of the sample was 65.15 (SD = 10.54). Over half the sample had a history of mental health treatment (n = 79; 60.31%), and 50 individuals had a history of domestic violence (38.76%). It should be noted that the majority of the sample had at least one child with a history of developmental needs (n = 85; 65.38%). The mean household size was 2.5 children (SD = 1.55).
Most of the sample completed Project IMPACT (n = 92; 69.7%), and the mean length of time in the program for all participants was 4.64 months (SD = 1.98). Upon entering the program, clients had relatively low parenting skills and a problematic home environment. At baseline, mean parenting skills were 49.76 (SD = 14.48) of a possible total score of 113. The mean score of the home environment was 51.11 (SD = 16.56) of a possible total score of 100. The characteristics of clients participating in Project IMPACT are shown in Table 1.
Description of the Sample.
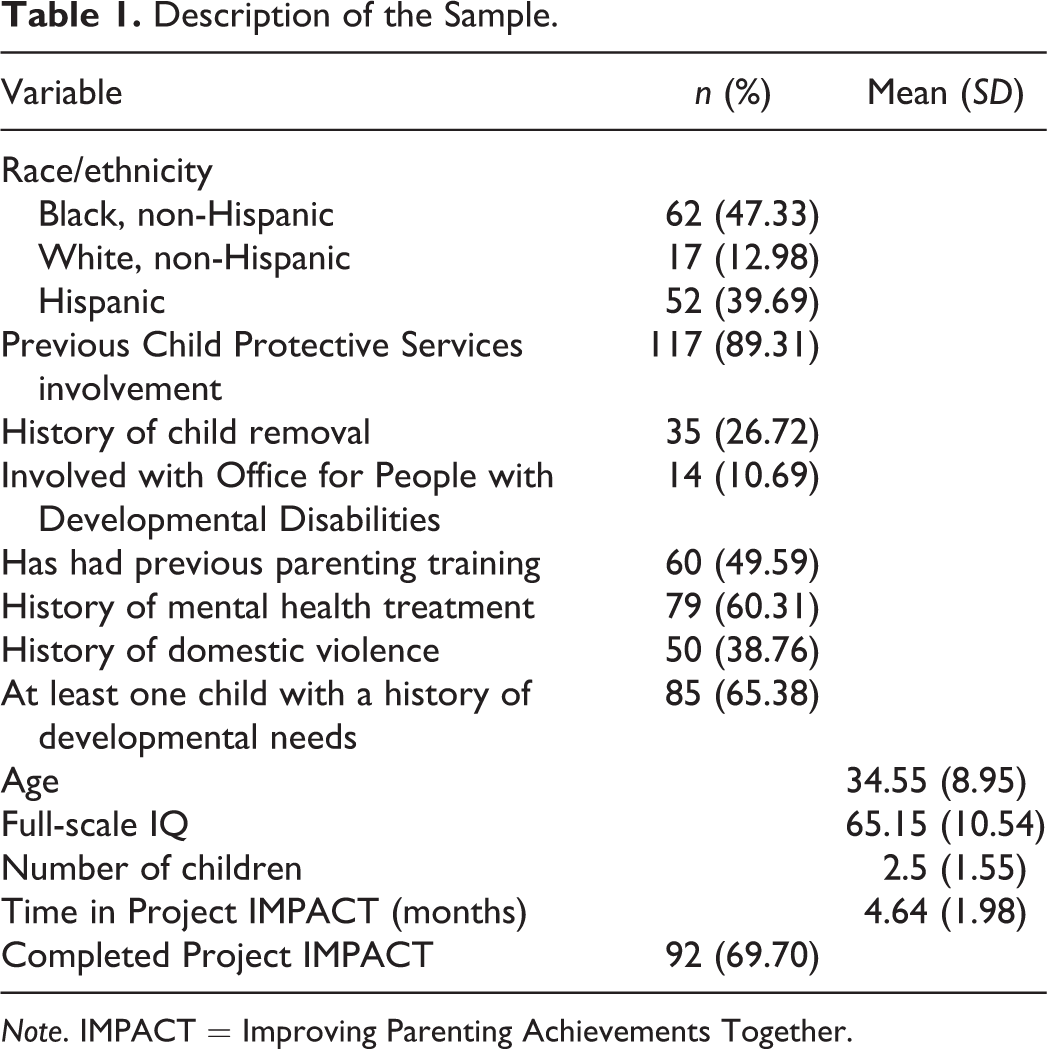
Note. IMPACT = Improving Parenting Achievements Together.
Quantitative Results: RQ2
Our modeling found that parenting skills improved significantly over time with the best fitting growth curve model being conditional on three-time invariant predictors: number of children, participation in previous parenting classes, and time in treatment. The predicted fixed effects of this model are displayed in Table 2 and illustrated in Figure 1.
Participants who had participated in a previous parenting program had predicted higher parenting scores than those who did not by 4.75 points (p = .02), and each additional child that a client had reduced predicted parenting scores by 1.16 points (p = .05). Both total time in the program as measured in months and time period were predictive of significant increases in parenting scores (p = .01 and p < .01, respectively). there was an interaction between these reducing the overall prediction of parenting skills by 1.86 points (p < .01).
Fixed Effects Prediction Of Parenting Skills.
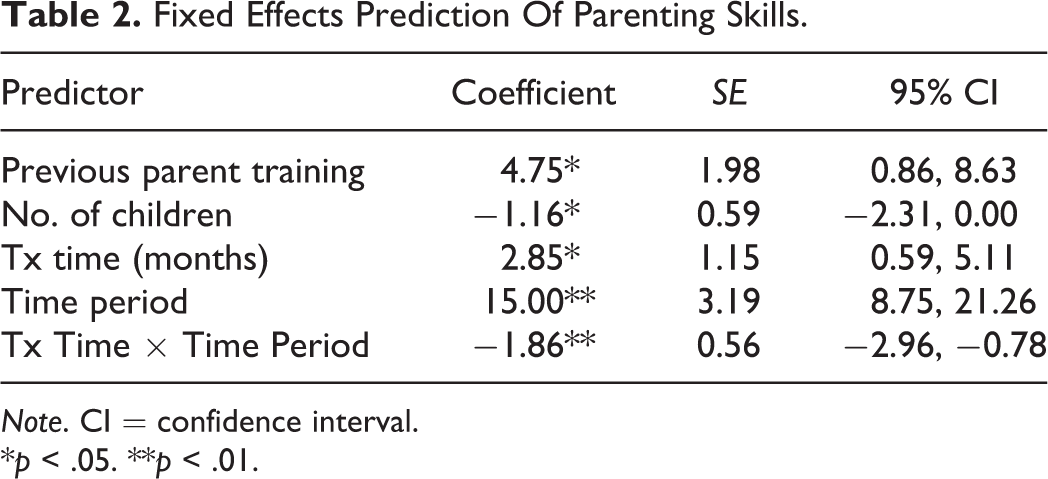
Note. CI = confidence interval.
*p < .05. **p < .01.

Predicted scores on Westchester Institute for Human Development Parenting Scale.
The home environment also improved significantly over time with the best fitting growth curve model being conditional on two-time invariant predictors, number of children and time in treatment, and one-time variant predictor, child behavior. The predicted fixed effects of this model are displayed in Table 3 and illustrated in Figure 2.
Fixed Effects Prediction of Home Environment.
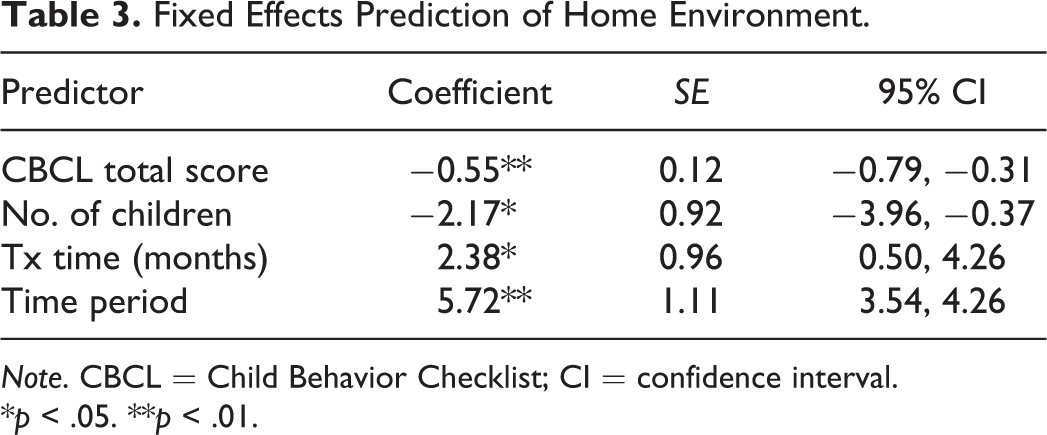
Note. CBCL = Child Behavior Checklist; CI = confidence interval.
*p < .05. **p < .01.
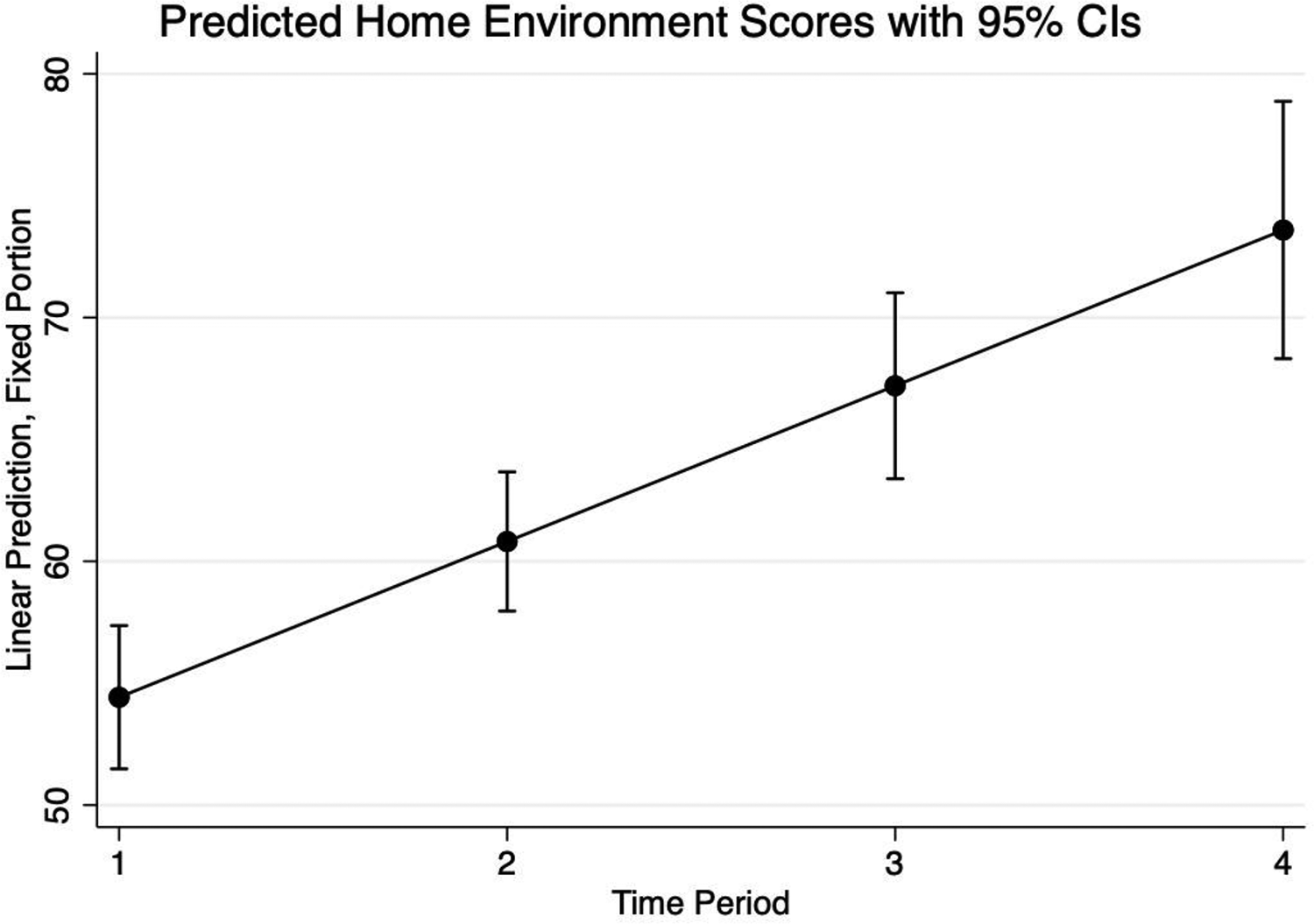
Predicted Home Observation for Measurement of the Environment inventory scores.
Each additional child in the family reduced home environment scores by 2.17 points (p = .02), and each additional point on the total CBCL reduced home environment scores by 0.55 points (p < .00). Time in treatment significantly improved home environment scores with each additional month involved in Project IMPACT increasing home environment scores by 2.38 months (p = .01). Finally, each additional time period predicted a 5.72 point improvement in the home environment (p < .00).
Finally, the odds of out-of-home placement were identified based on two logistic regression models. Time in treatment significantly predicted out-of-home placement (odds ratio [OR] = .63; p < .00) as did program completion (OR = .09; p < .00). These results are displayed in Table 4. For each additional month spent in Project IMPACT, there was an associated 37% reduction in the odds of a child being placed in out-of-home care 1-year post-discharge. Similarly, parents who completed Project IMPACT saw a 91% reduction in the odds of a child being placed in out-of-home care 1 year after concluding the program.
Logistic Regression Results Predicting Out-of-Home Placement.
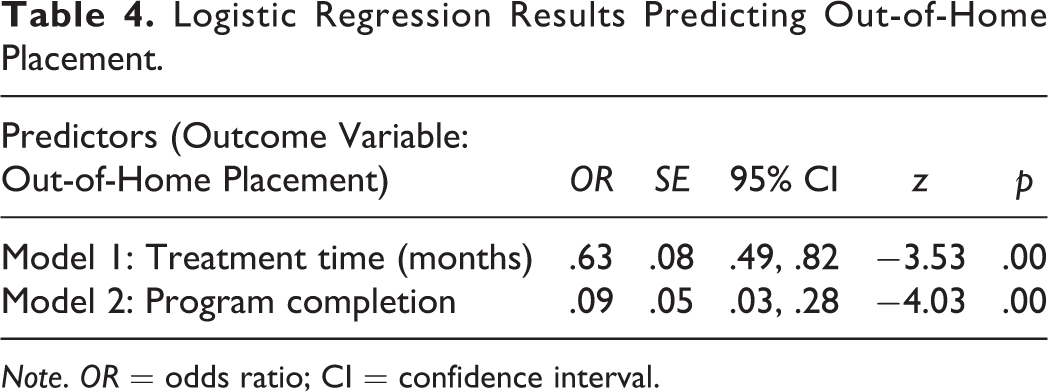
Note. OR = odds ratio; CI = confidence interval.
Qualitative Results: RQ3
Participants reported intensive support services, tailored parenting curriculum, community engagement, and positive worker–client relationship as key components of program participation. These themes are discussed in depth below.
Intensive support services
Participants reported the intensity of services provided by Project IMPACT as a critical aspect of keeping families safely together. Intensity referred to the frequency of visits (3 days a week), time spent on home instruction (1.5–2 hr), and the duration of the program (4–6 months). Compared to frontline child welfare workers, Project IMPACT clinicians spend more intensive time with their clients. A DSS worker reported, “A caseworker can only be there for half an hour or an hour, but a Project IMPACT worker goes to them at least three days a week so they do have that extended time with them.” The time spent with families allows for a more comprehensive assessment of client needs, which can result in more holistic service delivery and more opportunities for skills building.
In the focus group, Project IMPACT clinicians discussed visiting their clients in their homes and communities multiple times a week to guide parents with everyday tasks such as childcare, home management, problem-solving, and advocacy. One clinician described her role as integrating with the family. She reported, “because we get to know the family, we become part of their family. We meet them in the mornings, lunchtime, dinnertime, so we know what they’re doing.”
While participants uniformly agreed with the benefit of providing intensive services for 4–6 months, some stakeholders wished Project IMPACT could last for a longer time period and/or have a step-down program. As reported by a DSS worker, “I would love for Project IMPACT to be more than 6 months.” Similarly, a client reported “I would like to work with Project IMPACT for 1 year.” Project IMPACT social workers agreed that parents may need ongoing support, especially as children go through different developmental stages, which may require different parenting skills. While clients who complete Project IMPACT are provided with a transition plan, there is a need for ongoing support. As discussed by a Project IMPACT clinician, We do what we can for the six months, but before we’re done with the family, we’re like, “Okay, these are the supports you’re going to still need, so practice these skills.” So, you’re still going to need in-home parenting support from this agency. It might not be as intense as us, it’ll be a step down, but they’ll need ongoing support.
Tailored parenting curriculum
Project IMPACT services are strengths based and tailored to the unique learning styles of parents with I/DD. The intervention is focused on assisting parents in parenting their children and preventing placement or re-entry of children into foster care. It consists of skills training using a combination of hands-on practice and visual aids. Assessments of parents conducted at the start of the program and throughout the duration of the program act as a guide to tailor services to individual client and family needs.
In the focus group, the clinicians reported supporting their clients in day-to-day tasks based on their unique needs. Examples of daily tasks included bathing, feeding and toilet training their child, budgeting, developing to-do lists, grocery shopping, and cooking. To teach these skills, the instructions had to be repeated frequently and broken down into smaller components. Visual aids were used to reinforce skills, and parents received small incentives (e.g., gift cards) and childcare supplies for their participation. A Project IMPACT clinician reported, We follow curricula, and we have different skills. When we meet with the client at the first initial meeting, we know what the main need is. We have clients that are having problems with budgeting, so we start first with a budgeting sheet. We get their budget, and then we help them develop a budget where they can manage their food stamps and make their money last for the whole month. So that’s where we start, but we touch base in everything that has to do with, you know, it’s like managing our own life. You know, we help them arrange doctors’ appointments, we help them with food shopping. When we had Project IMPACT come in, they were working on kind of the same concrete things, you know, let’s go over the schedule. How are you going to manage caring for this child as opposed to the other child? Informing her and using repetition a lot, you know, what are we doing today?
Interagency collaboration and advocacy
Another critical component of Project IMPACT is the communication and collaboration between the Project IMPACT clinician, the DSS caseworkers, and community-based agencies. The first home visit is conducted in collaboration with Project IMPACT clinician and the DSS caseworker. Then, the Project IMPACT clinician provides regular updates to the DSS caseworker throughout each client’s participation. They communicate and collaborate on a regular basis to ensure that clients are referred to appropriate services and the DSS worker acts as an ongoing resource.
As needed, Project IMPACT clinicians attend community meetings with parents to provide support and educate other professionals about their clients’ needs. Examples include attending medical appointments, school appointments, and social security meetings. One Project IMPACT client said, “the PI worker provided help to apply for Section 8 and other medical appointments.” Project IMPACT clinicians also attend Family Network Meetings, which are facilitated by the Department of Community Mental Health. These meetings bring together multiple service providers on a monthly basis to discuss the families’ strengths and needs and identify priority areas that need attention. Each member of the meeting is then tasked with one or more responsibilities that they agree to follow up on with the client. Particularly for parents with I/DD, these network meetings help ensure that parents are receiving targeted support and that there is accountability from all members of the family’s service team, even after Project IMPACT services end.
Project IMPACT clinicians also act as advocates for parents. Advocacy can take on many forms across the areas of educational, medical, and daily living support. Examples of advocacy provided include helping clients understand and navigate the special education system, doctor’s appointments, and housing/benefits procedures. The clinicians support clients by helping them complete applications, preparing questions for upcoming meetings, and accompanying parents to meetings and appointments. Additionally, a common focus of advocacy is educating those working with the client about optimal ways to communicate with them. As reported by one DSS worker, They’re (Project IMPACT clinicians) strong advocates for the parents, and I know that the parents have really liked that because, because we’ve had several recent cases where the worker was really advocating strongly for the parent, and I know that they really appreciate it.
Worker–client relationship
Overwhelmingly, participants discussed the importance of the quality of the relationship between Project IMPACT clinicians and their clients. Themes that emerged included building trust and rapport, providing social–emotional support, and treating clients with respect and dignity. As an example, a DSS worker said of the Project IMPACT clinician, she “provided excellent level of support while being able to gain mother’s trust, respect, & cooperation.” Similarly, a Project IMPACT client said of her social worker, “She treated me like a human being, not a client.”
Project IMPACT staff shared the importance of joining with the family in everyday activities, which helped create a positive and lasting relationship between the social worker and the family. As reported by a DSS worker, Um, the ladies, they’re excellent at what they do, and they know how to engage a family. And they remember the family when they see the family in the community. Or when they come here, they’ll ask you, “Well have you seen so and so? And how is so and so doing?”
Discussion and Applications to Practice
This study examined an intensive parenting skills program for parents with I/DDs at risk for child removal due to allegations of child maltreatment. Findings show that parents who participate in Project IMPACT demonstrate improvement in parenting skills and the home environment that can help families remain intact even after terminating from the program. Parents with fewer children had more improvement in both outcomes; parents whose children exhibited fewer behavioral problems demonstrated more improvement in the home environment. This perhaps is because HOME inventory scores can be negatively affected by challenges in the areas of positive parent/child interactions and forms of discipline. Additionally, a main component of the HOME is a child’s access to a variety of stimulating activities, both in and outside of the home. For participants with children with fewer behavioral problems, the focus of services can be on promoting age-appropriate child activities, as opposed to more attention on managing problematic behaviors.
Findings also show that the length of time spent in the program, regardless of whether parents complete the program, is related to keeping families together. Specifically, those parents who fully complete Project IMPACT saw a 91% reduction in the odds of out-of-home placement for their children. From the start of services, each additional month participating in the program reduced the odds of out-of-home placement by 37%. Some stakeholders desired that Project IMPACT last longer than 6 months or there was a step-down program option. The duration of interventions for parents with I/DD has been discussed previously by researchers, noting that The more opportunities parents with I/DD have to learn and practice skills would likely have positive implications for mastery of the targeted adult and child behaviors, but this likelihood must be carefully weighed against logistical concerns of parent education programs such as financial cost. (Knowles et al., 2015)
The intensive nature of services affords clinicians the opportunity to conduct a comprehensive assessment of client and family needs and tailor services to the needs of parents with I/DD and the developmental stage of their child/ren. The clinicians provide different modalities of parenting skills training including the use of modeling, visual aids, and repetition. Clinicians also have regular communication with community stakeholders, including and recommending, requesting, and attending Family Network Meetings, which are facilitated by the Department of Community Mental Health. Project IMPACT clinicians advocate for clients in the realms of public benefits, health, mental health, housing, and education. Project IMPACT’s utilization of various modalities to improve parenting skills is in accordance with prior research recommendations regarding the importance of adapting behavioral interventions to diverse learning styles and capacities (Azar et al., 2012).
Another qualitative finding is the quality of the relationship between the client and the clinician. Stakeholders described key characteristics such as developing trust and rapport, providing social–emotional support, and demonstrating an investment in the current and long-term success of their families. Project IMPACT clinicians integrate into the family, assisting with daily living, and “become like part of the family.”
Findings from this study underscore the importance of providing services tailored to the unique needs of parents with I/DD, confirming prior research recommendations to move toward tailored service models rather than a one size fits all approach (Azar et al., 2012; Slayter & Jensen, 2019; Wilson et al., 2014). Providing these services can help improve parenting skills, the home environment, and help keep children at home safely. It may also be more cost-effective than placing children in foster care. While it is unclear what the long-term outcomes are for these children, the fact that parents who had longer involvement with Project IMPACT saw significant decreases in the odds of having their children removed suggests that parents who participated in the program benefited even if they were unable to complete the program; however, those that completed the program had the greatest benefit. These findings also point to the need to assess program efficacy by determining both the most effective interventions and the optimal duration of participation needed to achieve best results (Knowles et al., 2015).
The Family First Prevention Services Act of 2018 (Family First) has prioritized Title IV-E funding for prevention services specifically for in-home parenting skill-based training for children at imminent risk for foster care placement. To date, there are few documented evidence-based parenting programs for parents with I/DD involved in child welfare (Knowles et al., 2015; Lightfoot et al., 2018). There is a need for additional funding and programmatic support for interventions targeted specifically to parents with I/DD involved in the child welfare system particularly since this group appears to be a sizable proportion of the child welfare population.
Future research would benefit from an experimental or quasi-experimental design with a control group to determine whether PI is more effective than other programs in teaching positive parenting skills and keeping families safe and intact. For example, Westchester County has a robust service array with which Project IMPACT clinicians connect clients. It is unclear whether a similar program with less robust community services would be able to sustain similar outcomes, particularly that of keeping families intact after program discharge. While the qualitative data captured multiple stakeholder perspectives, including parent voices in the client satisfaction surveys, additional research should use a prospective study design that employs multiple methods (e.g., observation, interviews) to capture the perceptions and experiences of parents with I/DD. For these reasons, we recommend replicating this study in other settings and with additional evidence-based program satisfaction feedback.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Boston University’s Center for Innovation in Social Work and Health’s 2018 Innovation Pilot Funding Grant.