
Abstract
Purpose:
To systematically review and meta-analyze all published studies, written in Chinese and published in China, focusing on mindfulness-based interventions for Chinese breast cancer patients’ mental health and quality of life outcomes.
Methods:
Following the Cochrane guideline, this study searched across five electronic debases, two professional websites, two major Chinese oncology journals, and reference lists of existing reviews and included studies. Meta-analysis was conducted using meta-regression with robust variance estimation. Publication bias and risk of bias were assessed and evaluated in the final analysis.
Results:
A final of 35 clinical trials included 126 effect sizes and 3,100 participants. Studies reported an overall large and statistically significant treatment effect, g = 0.963, p < .001.
Conclusions:
Mindfulness-based interventions were significantly effective for Chinese breast cancer patients and are recommended for oncology social workers. Moderator analyses identified group-based mindfulness interventions as significantly more effective than individual-based interventions, and mindfulness-based interventions delivered as therapeutic
Female breast cancer is highly prevalent internationally with over 2 million newly diagnosed breast cancer patients worldwide in 2018 (Bray et al., 2018). In that year, over 620,000 breast cancer patients died (6.6%), resulting in breast cancer having the second highest mortality rate among all cancer diseases and the highest for female cancer patients (Bray et al., 2018; Ferlay et al., 2019). It is worth noting that there exist salient cancer disparities between developed and developing countries, with developing countries, like China for example, reporting sharp increases in breast cancer incidences and deaths over the past decade (DeSantis et al., 2015). Despite the aforementioned statistics, advances in breast cancer care have significantly improved the life expectancy of breast cancer patients worldwide. The average 5-year survival rate for women with nonmetastatic invasive breast cancer is 91% (Ghoncheh et al., 2016). While the survival rate of breast cancer patients has, fortunately, increased over the years, psychosocial care for breast cancer patients and survivors remains an area of concern, especially for ethnic/racial minority patients in the United States and patients from developing countries (Izci et al., 2016; Weis, 2015).
A systematic review of depression and anxiety among breast cancer patients revealed a prevalence rate of 40% and 27% for these disorders, respectively (Maass et al., 2015). Moreover, studies have found over 30% of breast cancer patients experience psychological distress, further compromising their cancer care and posttreatment survivorship experience (Fradelos et al., 2017). In addition, late entry and side effects of cancer treatment as well as other risk factors, for example, stigma, major life interruptions, pose significant impacts on breast cancer survivors’ quality of life (Fu et al., 2015), with studies reporting poor quality of life among breast cancer patients and survivors years post cancer treatment completion (Hamood et al., 2018). Considering these major psychosocial challenges among breast cancer patients (i.e., mental health and quality of life decline), it is critical for psychosocial oncology providers, particularly oncology social workers, to deliver evidence-supported treatments to improve breast cancer patients’ mental health and quality of life challenges.
To our knowledge, there exist nine meta-analytic reviews focusing on psychosocial interventions for breast cancer patients’ mental health and/or quality of life outcomes, including three reviews focused on psychosocial interventions (Chen et al., 2018; Matthews et al., 2017; Tatrow & Montgomery, 2006) and six reviews focused on mindfulness-based interventions (Cramer et al., 2012; Haller et al., 2017; Huang et al., 2016; Zainal et al., 2013; J. Zhang et al., 2016; Zhang, Zhao, & Zheng, 2019). In general, studies have favored the treatment effect of psychosocial interventions for depression, anxiety, psychological distress, and quality of life, with the strongest evidence supporting mindfulness-based interventions. However, existing reviews have overwhelmingly focused on Western literature written in English, with fewer than 5% of the clinical trials included in published reviews examining breast cancer patients and survivors of racial minority backgrounds. This has created a critical gap in the research synthesis literature of psychosocial interventions for breast cancer patients and practitioners, especially for oncology social workers serving minority breast cancer patients, particularly Chinese breast cancer patients.
Chinese Americans are one of the largest immigrant groups in the United States, and furthermore, Chinese is the most prevalent of Asian Americans with breast cancer diagnoses (Jenny et al., 2011; Telli et al., 2011). Notably, Chinese American breast cancer patients report higher levels of distress and poorer quality of life when compared with their White counterparts (Lu et al., 2017). Moreover, Chinese American breast cancer patients are less likely to seek out psychosocial services, due to the increased stigma associated with cancer diagnoses in Asian culture (Tsai & Lu, 2019), further widening the disparity for Chinese Americans with breast cancer. Finally, cancer patients of various ages and racial backgrounds respond differently to mindfulness-based interventions (Maskarinec et al., 2000; A. Zhang et al., 2020). Consequently, findings from existing reviews supporting mindfulness-based interventions for White breast cancer patients cannot be assumed to be effective for Chinese (American) breast cancer patients. The purpose of the present study, therefore, is to systematically review and meta-analyze the effectiveness of mindfulness-based interventions for breast cancer patients’ mental health and quality of life outcomes published in the Chinese literature. We anticipate these findings will not only be relevant to Chinese breast cancer patients in China but also provide direct social work practice implications for oncology social workers in the United States when working with breast cancer patients of Chinese descent.
Method
Following the Cochrane Collaboration Guidelines (Higgins & Green, 2011), this study searched across five electronic databases including (1) China Academic Journals Full-Text Database, (2) China Academic Journal Network Publishing Database, (3) China Academic Journals Electronic Publishing House, (4) China Science and Technology Journal Databases (including medical journals), and (5) WanFang Data Knowledge Service Platform which integrates over 15 additional academic databases. Combined together, our search strategy was inclusive of over 20 electronic databases, and these databases included publications from Mainland China, Taiwan, Hong Kong, and Macau. For each database, we searched studies using “zheng nian” (mindfulness), “chan xiu” (Zen), “ming xiang” (meditation), or “nei guan” (inner reflection) to capture studies using mindfulness-based interventions; and “ru xian ai” (breast cancer), “ru xian liu” (breast oncology), or “ru xian zhong liu” (breast malignancy) to capture studies involving breast cancer patients.
In addition to the electronic data search, we conducted manual and gray literature searches including (1) Screening of reference lists of eligible studies; (2) Searching relevant professional websites: China Anti-Cancer Association (http://www.caca.org.cn/english/); Chinese Society of Clinical Oncology (http://www.csco.ac.cn/); and (3) Major Chinese oncology journals, that is, Chinese Journal of Cancer Research and the Chinese Journal of Cancer.
Study Eligibility and Screening
The search included all Chinese language studies from inception date through August 1, 2020 (the date the initial search of electronic databases was completed). Studies were eligible if they met the following criteria: (1) evaluated a mindfulness-based intervention, (2) targeted breast cancer patients and/or survivors, (3) focused on patients’ mental health and/or quality of life outcomes, and (4) used a controlled trial design with or without randomly assigning study participants. A study was excluded if (1) there was not a comparison group; (2) it only focused on outcomes other than mental health and quality of life; and (3) it did not provide enough statistical information to calculate an effect size. Two research assistants independently screened each study by first reviewing the title and abstract, and for those considered for inclusion subsequently reading the complete article. Interscreener reliability reached satisfactory levels of 84% and 96% for title/abstract and full-text screening, respectively. Disagreements were resolved by discussion between the two reviewers. The two reviewers spent two 1.5-hr meetings discussing all disagreements. If unsuccessful in obtaining consensus, the disagreement was resolved by a third reviewer who is a full professor with a background in psychology and social work from a Tier 1 university in China. Only one article was brought to a third reviewer for a decision.
Data Extraction, Publication Bias, and Risk of Bias
Data were extracted systematically using a predefined coding sheet centering on (1) study characteristics (e.g., bibliographic information, type of publication); (2) participants’ demographics (e.g., age, socioeconomic background); (3) study design (e.g., type of comparison group, use of random assignment or not); (4) intervention characteristics, (e.g., treatment modality, including individual vs. group intervention), provider background; and (5) Statistical information necessary to calculate an effect size for mental health and/or quality of life outcomes. Publication bias was assessed employing funnel plot as well as Vevea and Woods (2005) sensitivity analysis with a priori weight function. Funnel plot is a commonly used visual tool for inspecting publication bias, and a symmetric funnel plot, i.e., effect size estimates are evenly distributed, is a sign of low concern for publication bias. The Vevea and Woods sensitivity analysis is a statistical/visual procedure to evaluate publication bias. The model calculates an observed overall treatment effect size and a theoretical treatment effect size which assumes the funnel plot is perfectly symmetric (Zhang, Franklin, et al., 2019). If the difference between the two overall effect size estimates is statistically nonsignificant, it indicates low concern for publication bias. Finally, risk of bias of randomized controlled trial studies was evaluated using the Cochrane risk of bias for randomized trials second version (RoB 2; Higgins et al., 2019). For controlled trial studies without randomization, the Risk of Bias in Non-Randomized Studies of Interventions (ROBINS-I; Sterne et al., 2016) was applied.
Statistical Analysis
All eligible studies reported continuous outcomes, thus standardized mean difference (SMD) was calculated using small sample size corrected Hedges’s g (Cooper et al., 2019), noted as g in this study. We first descriptively analyzed study characteristics (e.g., year of publication, types of mindfulness-based intervention) and intervention length. For meta-analysis, we used meta-regression with robust variance estimation (RVE; Hedges et al., 2010). Meta-regression with RVE is the optimal method to analyze effect sizes in this study because it permits the inclusion of multiple effect sizes from the same study, which is not allowable in classic meta-analysis methods. Furthermore, meta-regression with RVE provides a flexible analytical framework to conduct subgroup and moderator analyses which has the potential to offer important clinical implications for evidence-based social work practice. Finally, meta-regression with RVE uses a powerful variance modeling strategy, producing robust statistical inference across fixed- versus random-effects models of meta-analysis (Hedges et al., 2010; Tanner-Smith & Tipton, 2014).
Results
Search Results
Figure 1 demonstrates the literature search process. Initial search of electronic databases and manual searches identified a total of 378 studies for title and abstract screening once duplicates were removed. First excluded were 266 studies that simply did not meet inclusion criteria. A detailed full-text review was then completed for 112 studies, which further excluded 77 studies for various reasons recorded in Figure 1. The final analytical sample totaled 35 clinical trials focusing on mindfulness-based intervention for Chinese breast cancer patients.
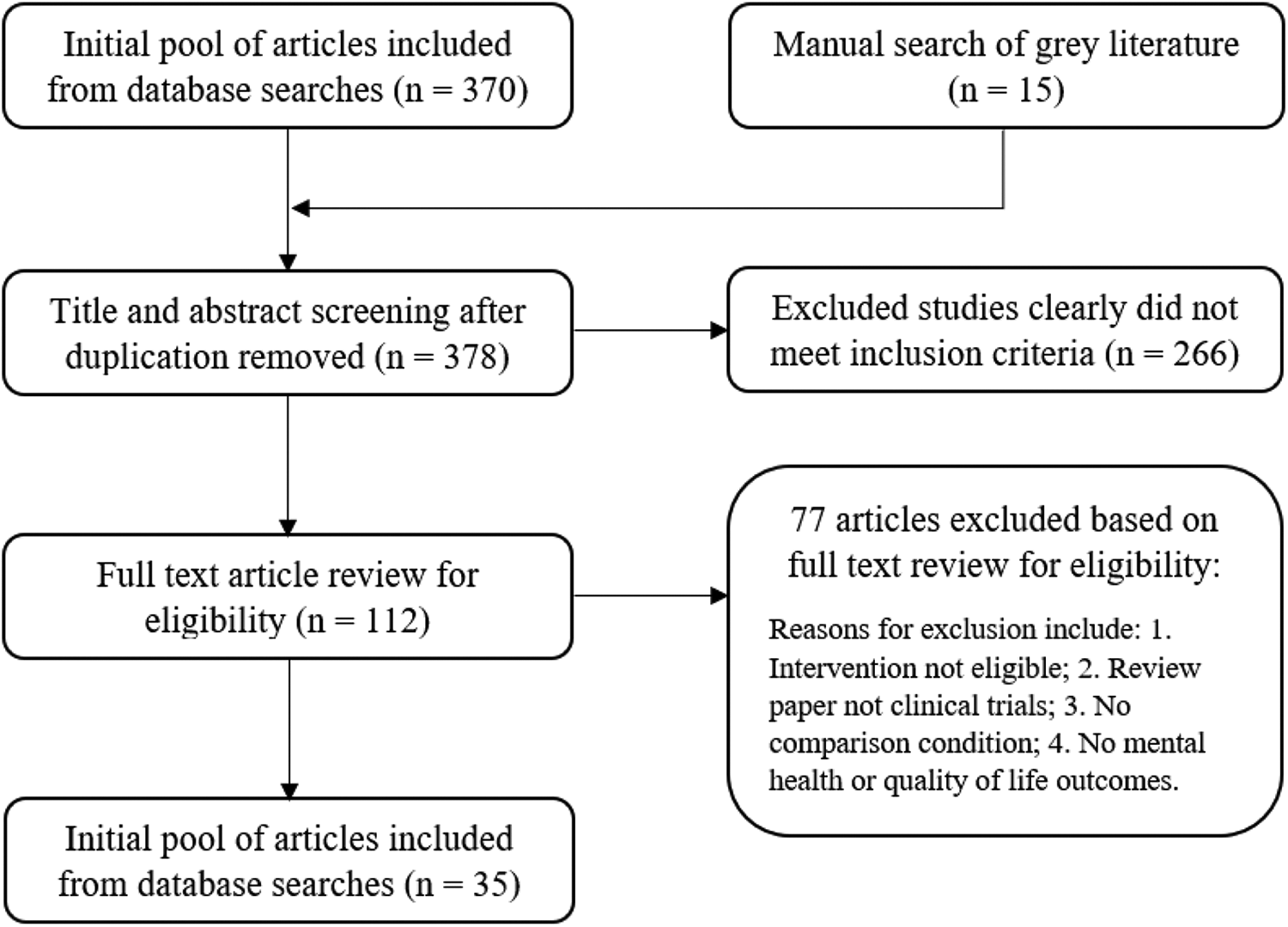
Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) literature search flow diagram.
Risk of Bias and Publication Bias
Study risk of bias was assessed using RoB 2 for randomized controlled trials (n = 28) and ROBINS-I for nonrandomized controlled trials (n = 7) as presented in Table 1. Except for seven studies that reported mild or moderate analysis concerns due to missing data, all studies reported a low risk of bias. The funnel plot in Figure 2 was reasonably symmetric which suggested low concern for publication bias. Vevea and Woods (2005) sensitivity analysis further confirmed such a conclusion as evidenced by an observed overall treatment effect (the thick line) not significantly different from the theoretical treatment effect (the thin line) which assumes the funnel plot is symmetric, that is, the distance between the two lines was very small.
Risk of Bias of Included Studies.

Note. MOD = moderate risk; LOW = low risk of bias; S-C = some concerns.
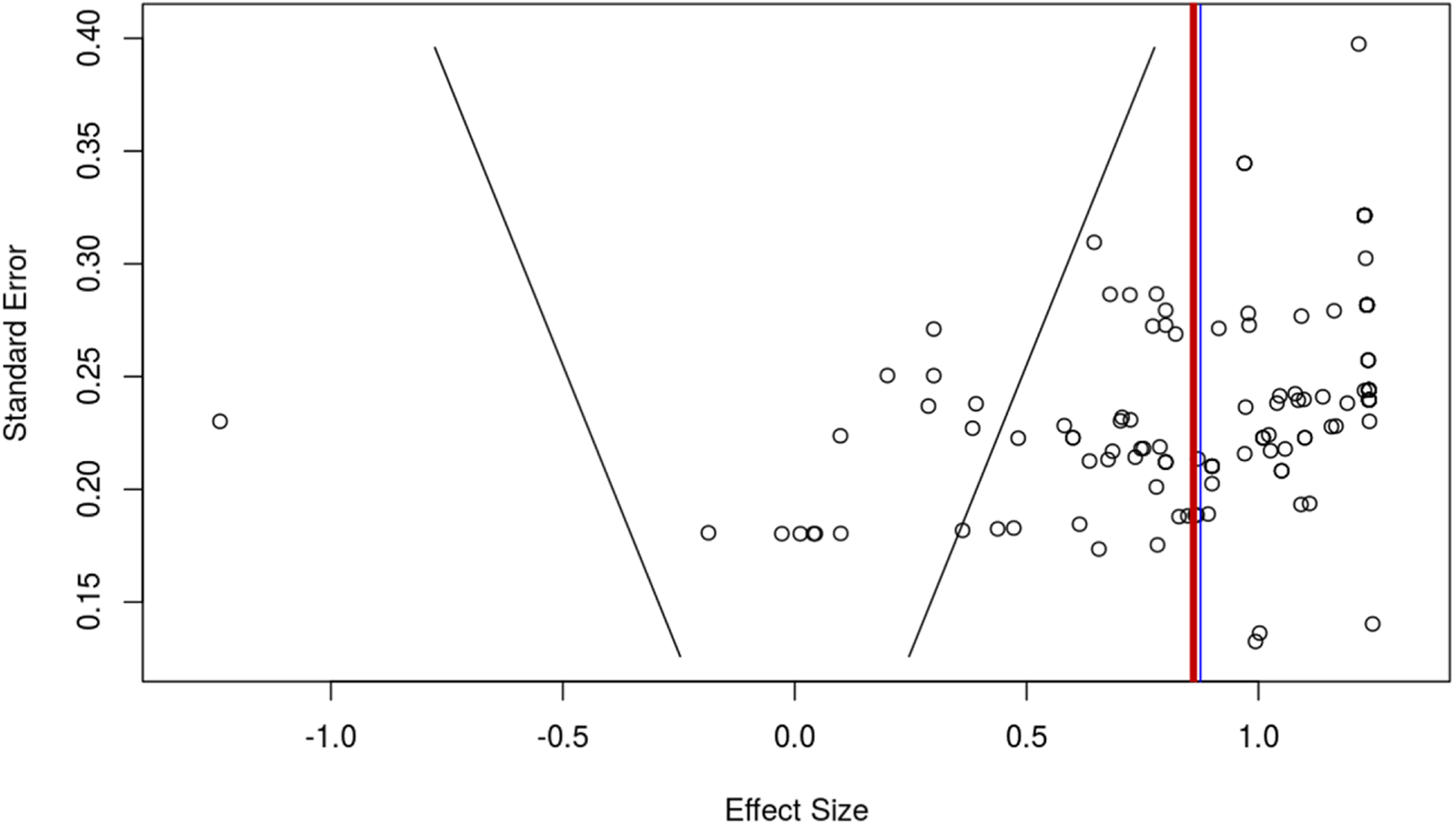
Funnel plot.
Study Characteristics
A total of 35 clinical trials were included, with 3,100 participants having an average age of 45.91. All studies were peer-reviewed articles in academic journals. Each study focused on Chinese breast cancer patients receiving active cancer treatment, with nine studies including cancer patients in various disease stages, that is, from early to Stage IV breast cancer. Apart from two trials comparing mindfulness-based intervention with an alternative intervention, all trials employed treatment-as-usual for the control condition. More than half of the studies (n = 20, 57.1%) delivered group-based mindfulness interventions with 15 studies delivering an individual-based mindfulness intervention. Almost three quarters of the studies (n = 26, 74.3%) implemented mindfulness-based intervention for therapeutic improvement, leaving nine studies delivering mindfulness-based intervention as a supportive or behavioral skill training intervention (e.g., practicing breathing exercises for relaxation).
Twenty-four studies employed providers to administer mindfulness-based interventions to improve breast cancer patients’ mental health and quality of life. An additional 11 studies had providers teach mindfulness skills and techniques for patients to practice on their own. Thirty-three studies reported an average session frequency of 10.5 sessions per month, ranging from 2 to 30 sessions every month. Thirty-one studies solely delivered mindfulness-based interventions, while four studies provided mindfulness-based intervention in conjunction with other components (e.g., psychoeducation or case management). Average session length of the 33 studies reporting was 90 minutes per session, with a range of 15 min to 2 hr.
There were a total of 126 effect size estimates across the 35 clinical trials. Thirty-two studies (71 effect sizes) included mental health outcomes and nine studies (55 effect sizes) had quality of life outcomes. Specifically, 26 studies evaluated mindfulness-based intervention for depression (28 effect sizes), while 28 studies evaluated for anxiety (31 effect sizes). Eleven studies (12 effect sizes) evaluated the effect of mindfulness-based interventions for psychological distress among Chinese breast cancer patients. Study characteristics are presented in Online Supplemental Table 1.
Meta-Analytic Results
Meta-analytic and subgroup analyses results are presented in Table 2. Heterogeneity across effect size estimates was assessed using multilevel modeling with the result indicating a significant amount of between effect sizes heterogeneity, Q(125) = 454.59, p < .001. A statistically significant and large treatment effect size for Chinese breast cancer patients’ mental health and quality of life was identified, g = 0.963, p < .001. In comparison to the control condition, participants who received mindfulness-based interventions were on average 0.921 standard deviations higher (improvement) in mental health and quality of life outcomes. Specifically, for mental health outcomes, mindfulness-based interventions were not only statistically significant but also had a large treatment effect, g = 0.981, p < .001. Similarly, for quality of life outcomes, mindfulness-based interventions reported a statistically significant and large treatment effect, g = 1.01, p < .001.
Overall Treatment Effect and Subgroup Analysis.

Note. Estimate = point estimate of standardized mean difference using small sample size corrected Hedges’s g across all effect sizes, and for all subgroup of effect sizes; SE = standard error; K = number of studies; N = number of effect size estimates; dfs = degrees of freedom; RCT = randomized controlled trial; nRCT = controlled trial without randomization.
a If degrees of freedom is lower than 4, a more stringent p value, that is, p < .01, should be used for inference.
Subgroup analyses were conducted using study design (random vs. nonrandom assignment), treatment modality (individual vs. group), treatment approach (therapeutic vs. supportive), and treatment component(s) (solely mindfulness interventions vs. mindfulness interventions plus other components). A large and statistically significant treatment effect was identified for both randomized controlled trials and controlled trials without randomization, g = 1.01, p < .001 and g = 0.831, p < .001, respectively. Similarly, a large and statistically significant treatment effect was identified for both individual and group mindfulness-based interventions, g = 0.863, p < .001 and g = 1.164, p < 0001, respectively. Studies with therapeutic or supportive intervention approaches reported large and statistically significant treatment effects, g = 1.061, p < .001 and g = 0.846, p < .001, respectively. Studies that delivered solely mindfulness-based interventions reported a large and statistically significant treatment effect, g = 0.967, p < .001, whereas studies that delivered mindfulness-based interventions in addition to other treatment components reported a statistically nonsignificant treatment effect, g = 0.925, p = .024. It should be noted that the degrees of freedom associated with the effect size of mindfulness intervention with other components were lower than 4. Consequently, a p value of .001 was required to determine statistical significance.
Moderator Analysis
Moderator analyses, presented in Table 3, evaluated whether participant demographics, study design, and intervention characteristics significantly moderated treatment outcomes. Analyses found that treatment modality was a significant moderator for treatment effect size, b = 0.252, p < .01. Group-based mindfulness interventions reported on average 0.252 standard deviations higher (more effective) than individual-based mindfulness interventions. Treatment approach was also a significant moderator for treatment effect size, b = −0.201, p < .01. Supportive mindfulness-based interventions reported on average 0.201 standard deviations lower (less effective) than psychotherapeutic mindfulness interventions. All other moderators were statistically nonsignificant.
Moderator Analysis.
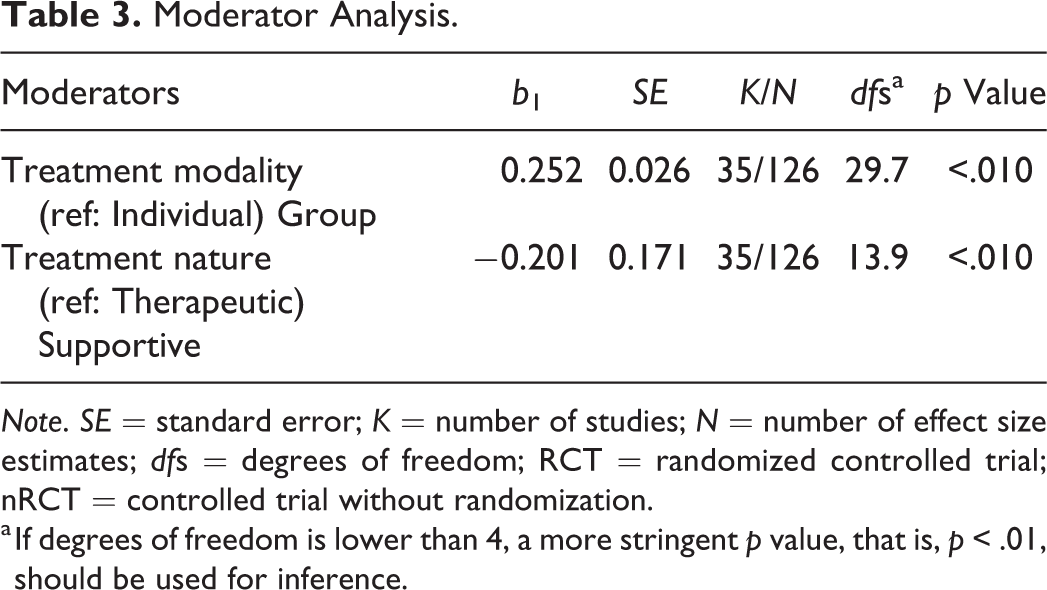
Note. SE = standard error; K = number of studies; N = number of effect size estimates; dfs = degrees of freedom; RCT = randomized controlled trial; nRCT = controlled trial without randomization.
a If degrees of freedom is lower than 4, a more stringent p value, that is, p < .01, should be used for inference.
Discussion
Although there was support from existing systematic reviews and meta-analyses studies for mindfulness-based interventions for breast cancer patients, little is known about its effectiveness for Chinese breast cancer patients. In this review of Chinese literature on mindfulness-based interventions for breast cancer patients in China, we identified an overall statistically significant and large treatment effect for Chinese breast cancer patients’ mental health and quality of life. Mental health wellness is often correlated with breast cancer patients’ quality of life. Therefore, it is important to evaluate interventions’ treatment effects for both of these outcomes.
It is worth noting that mindfulness-based interventions reported large and statistically significant treatment effects for both mental health and quality of life outcomes among Chinese breast cancer patients when evaluated separately. These findings support the robustness of mindfulness-based interventions for Chinese breast cancer patients. With the treatment effect not differing significantly between interventions for mental health versus quality of life outcomes, it is reasonable to infer that mindfulness-based interventions are equally effective for both types of outcomes.
When compared to existing Western literature, findings in this study are consistent with previously published meta-analyses on mindfulness-based stress reduction programs for breast cancer patients’ mental health outcomes, g = 0.71 and g = 0.73 for distress and anxiety, respectively (Zainal et al., 2013). Furthermore, unlike the large treatment effect size observed in this present review, Western reviews on mindfulness-based interventions reported small or moderate effect sizes for cancer patients (Cillessen et al., 2019; Piet et al., 2012). Although we did not formally evaluate the difference between the Chinese and Western literature, the interpretation of effect size magnitude (large vs. small to moderate) does preliminarily indicate that mindfulness-based interventions seem to be more effective for Chinese breast cancer patients, a topic worthy of future formal empirical investigation.
Although generally effective, subgroup analysis found that mindfulness-based interventions solely delivered reported a significant treatment effect. The same effect was not found among mindfulness-based interventions that were administered in conjunction with other treatment components. Based on available data, the nonsignificant finding was most likely caused by low statistical power, that is, small number of studies and effect sizes being analyzed. This conjecture was further supported by the p value (p = .024) associated with the overall effect size of mindfulness-based interventions (with multiple components). However, a more stringent p value of .01 is required for statistical inference for any effect with small degrees of freedom (df < 4). In other words, if we had more studies (and effect sizes) with greater than 4 degrees of freedom, a statistically significant treatment effect may well have been identified. But, given the limited number of studies focusing on evaluating the treatment effect of multiple-component mindfulness-based interventions for breast cancer patients in China, a future systematic review should consider reevaluating these types of interventions as more studies become available.
Moderator analyses identified two significant moderators: treatment modality (individual vs. group) and treatment approach (therapeutic vs. supportive). These findings revealed that mindfulness-based group interventions had a significantly greater treatment effect than did mindfulness-based individual interventions. This result is consistent with the existing Western literature, where group-based mindfulness interventions received the strongest empirical support (e.g., mindfulness-based stress reduction programs; Ledesma & Kumano, 2009; Zainal et al., 2013). Additionally, mindfulness-based interventions providing therapeutic treatment were significantly more effective than those delivering supportive treatment. This finding suggests that the provision of therapeutic mindfulness-based interventions may attain more positive treatment outcomes when supporting Chinese breast cancer patients’ mental health and quality of life.
Application to Social Work Practice
Meta-analytic and moderator analyses findings in this review provided important practice implications for oncology social workers. First, when providing psychosocial support to cancer patients or survivors of Chinese descent, mindfulness-based interventions are an empirically supported treatment and should be prioritized in psycho-oncology practice, given the statistically significant and large treatment effect identified in this review. For oncology social workers to engage in evidence-based practice, mindfulness-based interventions are well verified as supporting Chinese breast cancer patients’ mental health and quality of life outcomes. Second, considering the significant treatment effect difference between group- and individual-based mindfulness interventions, oncology social workers who work with Chinese breast cancer patients are highly encouraged to deliver group-based mindfulness interventions in order to maximize treatment effect. When group-based interventions are not feasible, individually delivered mindfulness interventions are also supported by research evidence, given the robustness of effectiveness of mindfulness interventions for Chinese breast cancer patients regardless of delivery format. Third, whenever feasible, oncology social workers should consider delivering mindfulness-based intervention as a therapeutic rather than a supportive treatment to optimize intervention outcomes for Chinese breast cancer patients. Consequently, oncology social workers who primarily teach patients mindfulness-based skills and techniques (e.g., breathing and relaxation) as a supportive intervention need to consider developing a deeper understanding of the change process for mindfulness-based interventions and possibly delivering such interventions by emphasizing psychotherapeutic treatment. With that said, it is important to reiterate that both therapeutic and supportive mindfulness-based interventions were found to have a statistically significant treatment effect for breast cancer patients. This means, that when delivering mindfulness-based interventions as therapeutic treatment is not feasible (e.g., due to lack of training or workforce shortage), supportive mindfulness-based interventions need to still be considered as an effective approach to improving Chinese breast cancer patients’ mental health and quality of life.
Strengths and Limitations
The present review is among the first to systematically synthesize mindfulness-based interventions for Chinese breast cancer patients based on Chinese published literature. Notable strengths of this study include a comprehensive scope (i.e., the inclusion of 35 clinical trials), high interrater reliability of reviewers, and the use of advanced meta-analytic strategy (i.e., meta-regression with robust variance estimation) that enabled meta-analysis of 126 effect sizes and provided sufficient power for moderator analyses. Risk of bias in the analyzed studies was low with minimal concerns for publication bias, further strengthening the validity of the findings. Despite these strengths, certain limitations inherent to systematic review and meta-analysis need to be noted when interpreting study results. First, there is always a chance that not all eligible studies were included, in spite of the comprehensive and systematic search strategy employed for the present study. Second, for certain subgroup and moderator analyses, this review still suffered from low statistical power (small number of studies or effect sizes), which may have contributed to the statistically nonsignificant findings. Thus, nonsignificant findings should be interpreted with caution.
This comprehensive systematic review and meta-analysis of mindfulness-based interventions for Chinese breast cancer patients identified overall statistically significant treatment effect on mental health and quality of life outcomes. Subgroup analyses, in general, supported the significant treatment effects of mindfulness-based interventions over the control condition, regardless of the outcome, study design, intervention modality, and treatment orientation. Moderator analyses identified group-based mindfulness interventions as significantly more effective than individual-based interventions and mindfulness-based interventions delivered as therapeutic treatment as significantly more effective than ones delivered as supportive treatment.
Supplemental Material
Supplemental Material, sj-docx-1-rsw-10.1177_10497315211000449 - Mindfulness-Based Intervention for Chinese Breast Cancer Patients: A Systematic Review and Meta-Analysis
Supplemental Material, sj-docx-1-rsw-10.1177_10497315211000449 for Mindfulness-Based Intervention for Chinese Breast Cancer Patients: A Systematic Review and Meta-Analysis by Anao Zhang, Shijie Jing, Phyllis Solomon and Anna Brose in Research on Social Work Practice
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.