
Abstract
Treatment as usual has historically been used as control arms for randomized controlled trials (RCTs), but utilizing wellness interventions as active comparison conditions can advance the evidence base of such interventions while increasing access to health promotion content. We use the results from the CONNECT 2 RCT's wellness intervention control arm as a case example of active comparison conditions that can control for dosage or attentional effects in future research. We summarized existing studies on wellness control HIV RCT interventions, introduced CONNECT 2, and discussed recruitment, randomization, and the intervention. Overall, Wellness Promotion participants were more likely to engage in physical activity, eat healthier, and do more vigorous exercise when compared with HIV Risk Reduction. CONNECT 2 Wellness intervention results solidify why wellness interventions can play an important role in treatment guidelines. Developing and implementing this model can be a more ethical, equitable, and holistic approach among underserved communities.
Keywords
The gold standard for evaluating intervention effectiveness is randomized controlled trials (RCTs) (Hariton & Locascio, 2018), but RCTs that include wellness or health-promotion behavioral interventions as control conditions and whose emphasis and core components or outcomes are neither specific to mental health nor conducted in education or work settings are limited and rare, especially in interventions developed by social workers. Researchers have moved away from using “placebo” as a control in which the participant received no intervention and have instead evolved to providing Treatment as Usual (TAU) (Oberjé et al., 2015). TAU is now widely used as a control arm for many RCTs, especially HIV/AIDS or substance misuse prevention interventions. Although there has been some shift to using TAU as a control condition in recent years (Freedland et al., 2011), not much attention has been paid to improving control conditions (Burns, 2009; de Bruin et al., 2009; Freedland et al., 2011). Few researchers have developed alternatives to TAU, and of those who have, there have been even fewer published outcomes and lessons learned from their interventions (Oberjé et al., 2015). With the increase in emphasis on mental and physical health, there is an urgent need to address physical/mental health in the control condition, especially among marginalized communities (Pratt, 2019), but little is known about how wellness interventions can improve study participants’ physical and mental health, especially those most at risk for chronic disease.
Wellness is defined as “the quality or state of being in good health, especially as an actively sought goal,” and wellness is considered achieved “when someone strives for balance in their life by constantly making choices to further their health and fulfillment” and has proven to have a “direct influence on overall health” (Evans, 2014; Merriam-Webster, 2019). Thus, wellness promotion can be defined as “the enhancement of physical, mental, and social well-being and the prevention of disease and disability” (Nader, 1992, p. 485). In contrast, health promotion is defined as “a behavioral, social science that draws from the biological, environmental, psychological, physical and medical sciences to promote health and prevent disease, disability, and premature death through education-driven voluntary behavior change activities that are strategies to improve health knowledge, attitudes, skills and behavior” (Khudair, 2018, p. 1677). Studies on this topic have sometimes used either health promotion or wellness interchangeably, but we recommend consistent use of terms in future research. Throughout this paper, we will use the term wellness for clarity and consistency.
Substance Use, Chronic Disease Co-Occurrence Among Low-Income Communities in the United States
Drug use and a lack of access to care for chronic diseases are two leading causes of poor health outcomes among low-income minority individuals (Hibbard & Greene, 2013). The relationship between illicit drug use and a broad spectrum of chronic diseases is complex and multifaceted. Growing evidence suggests that substance use also impairs judgment and negotiation skills, resulting in an increased risk of engagement in poor health behaviors (Freudenberg & Heller, 2016). Excessive alcohol consumption is directly related to chronic diseases, including diabetes, cancer, digestive problems, heart disease, and many other medical ailments (2013). Additionally, drug-involved populations often suffer poor health outcomes, such as the increased risk of obesity, heart attack, diabetes, HIV infection, intimate partner violence, alcohol abuse, hypertension, and even death (Whiteford et al., 2013).
Substance use and chronic disease are co-occurring public health threats that disproportionately affect low-income urban populations living in the United States (Dumont et al., 2012; King et al., 2018; Webb Hooper et al., 2020). Most research among people who use drugs has focused on reducing the risks for HIV and sexually transmitted infections (STIs) and substance use (Leigh & Stall, 1993; Turan et al., 2019). However, many drug-involved individuals report poor nutrition and physical fitness, and few meet basic wellness promotion guidelines as defined by the Centers for Disease Control (National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, 2013). Regardless, few intervention researchers have focused on general wellness and other health outcomes for drug-involved populations despite their high risk for heart disease, diabetes, and other significant chronic diseases related to stress, diet, and lack of exercise—and, more recently, COVID-19 (Cunningham et al., 2017; Killerby et al., 2020; Kim & Bostwick, 2020; MacDonald, 2012; Noonan et al., 2016; Stokes et al., 2020; Wadhera et al., 2020; Yancy, 2020).
The dilemma of the underrepresentation of minorities in clinical research is an ethical strategy to reach and engage more diverse populations in HIV research and other clinical and translation research (Luchenski et al., 2018; Pratt, 2019; Yu et al., 2021).
Applying a Wellness Intervention as a Strategy to Address Co-occurring Substance Use and Chronic Disease Burdens Among Marginalized Groups
We present a methods paper that supports the principle of equipoise in clinical research, with a lens on integrating wellness interventions into an experimental “control” condition and as a scientific strategy to help address social determinants of health among marginalized groups, including people who use drugs, individuals involved in the criminal legal system, and those at risk for HIV (Jackson et al., 2016). Marginalized groups have been historically difficult to recruit and retain in clinical trials due to their transient nature, heavy supervision requirements, and facilitator training required (Martinez et al., 2014; Witte et al., 2004; Wu et al., 2005). The current study adds to this limited literature by presenting the intervention and results from an RCT and successful strategies and recommendations for designing and implementing wellness-focused RCTs as control arms. We use the wellness intervention control arm for CONNECT 2, an RCT focused on HIV/STI risk reduction for low-income, drug-involved couples, as a case example to guide this proposed strategy for future interventions. Intervention design and future recommendations presented here may help guide other interventionists to implement RCTs with wellness control arms in low-income minority communities.
Implications of Wellness Interventions in Response to Social Determinants of Health
Social determinants, such as high-crime residential neighborhoods, lack of employment and low-wage employment, lack of doctors in low-income minority neighborhoods with affordable care options, lack of health insurance, and lack of affordable housing also predispose low-income urban minorities to poor health and chronic diseases (Geronimus, 2000; Rashid et al., 2009). It is well documented that these adverse social determinants can lead to lower life expectancy and that inequities in health outcomes worsened disproportionately among underserved populations due to the COVID-19 pandemic (Anderson, 2012). In addition, structural racism, including racialized drug laws, has further increased the relative risk of Blacks and Latinx Americans being arrested, convicted, and incarcerated for the same drug-related crimes as whites (Beckett et al., 2005; Kerr & Jackson, 2016). Incarceration further contributes to poor health due to lack of exercise, an unhealthy diet, and interrupted access to regular healthcare services (Zenk et al., 2011).
Two longitudinal observational studies examining county- and census-tract-level associations between social determinants and HIV diagnosis among African-Americans have identified potential moderators of HIV/STI incidents (Gant et al., 2012, 2014). Researchers found that among heterosexual African-American men, rates of HIV varied with increases in housing vacancy, lower educational attainment, and a higher number of non-married individuals in their census tract over a four-year period (Gant et al., 2014). An opposite trend in HIV rates among these men was observed in areas with a greater number of unemployed and married individuals. For African-American women, an increase in incidents of HIV was observed at the county level over two years in areas with greater income inequality and a higher number of unmarried individuals (Gant et al., 2012, 2014) A reverse in the trend was observed for those women residing in counties with a greater proportion of white individuals.
These adverse conditions also have implications for negative outcomes associated with substance use and HIV. For instance, unemployment, housing insecurity, and residing in high-crime areas can place individuals with histories of substance use at risk of relapse (Goldman-Hasbun et al., 2019). In addition, the stress and coping demands of challenging social conditions can be a risk factor for substance use and alcoholism, both of which may reduce inhibitions associated with sexual risk and HIV prevention behaviors (Pence et al., 2008). In addition, substance use has been associated with low adherence to HIV medication (Gonzalez et al., 2013).
Correlations Between Substance Use and Chronic Health Implications
Steady increases in the prevalence rates of opioid and methamphetamine use over the past five years have worsened since the COVID-19 pandemic, and emerging data suggest that Black individuals have been disproportionately represented in overdose deaths (Alexander et al., 2020; Becker & Fiellin, 2020; DiGennaro et al., 2021; Khatri et al., 2021; Larochelle et al., 2021). Therefore, for minority populations overrepresented in COVID-19 infection rates—including Black populations (Webb Hooper et al., 2020)—there is a critical need to not only reduce the risk of substance use (McKnight-Eily et al., 2021) and HIV/STIs but also to address the co-occurring risks of chronic disease, including poor eating habits, which compound health consequences, are a leading contributor to premature death in this population, (Centers for Disease Control and Prevention, 2001; Tai et al., 2021; Webb Hooper et al., 2020) and increase the risk for poor COVID-19 outcomes (Killerby et al., 2020; Nanda et al., 2021; Stokes et al., 2020; Yancy, 2020). Lastly, the COVID-19 pandemic and its associated restrictions have increased the disparity of health outcomes and exacerbated many social determinants of health. For example, some healthcare services for non-COVID-19-related conditions were unavailable, restricted, or disrupted for periods of time (Bojdani et al., 2020; Ferreira-Filho et al., 2020).
In Table 1, we present data on all SIG Wellness interventions as control conditions for RCTs. Information is provided on Wellness Components, theory, sample and settings, study and intervention design, and details on the follow-up period and retention rate for each study.
Social Intervention Group (SIG) Wellness Studies Comparison.
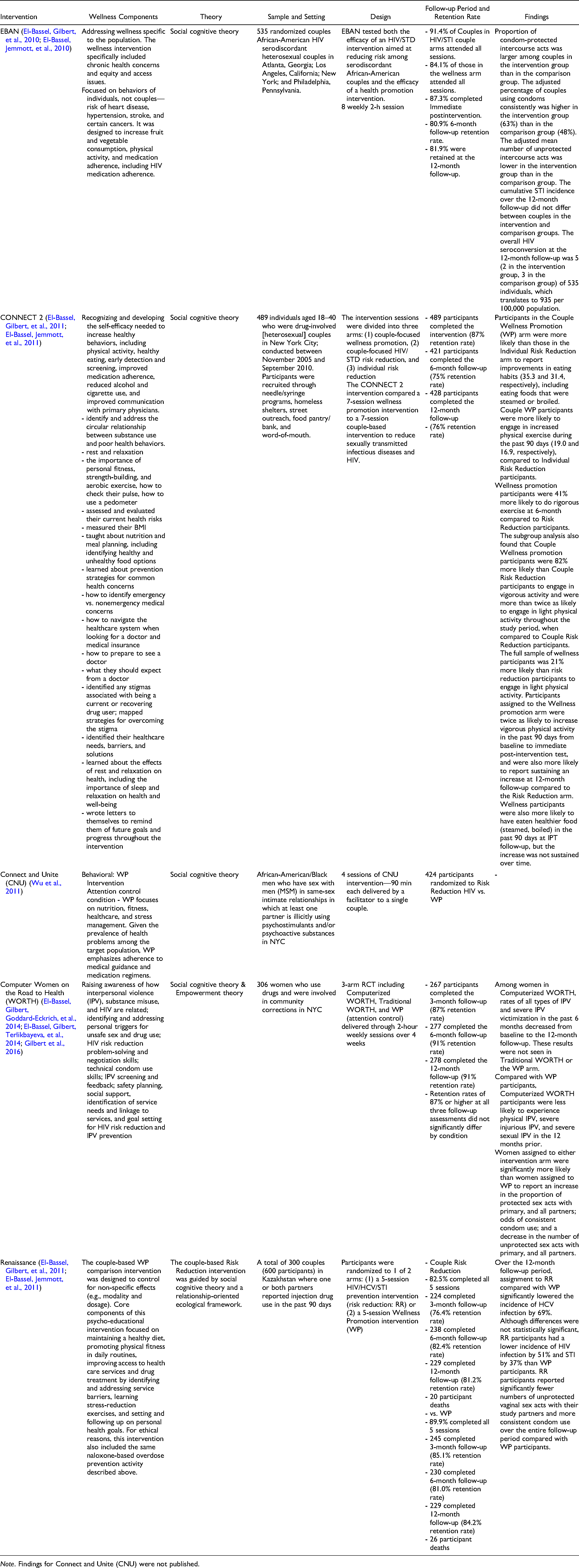
Note. Findings for Connect and Unite (CNU) were not published.
Literature Review
HIV Treatment RCTs with Wellness Intervention Including Couples-Based Wellness Interventions
We identified very few HIV/STI risk reduction RCTs that utilized wellness or health promotion interventions as control conditions (Abe & Abe, 2019; Harawa et al., 2020; Heeren et al., 2018; Oliveira et al., 2020). Despite their clear promise to promote health and prevent or improve HIV outcomes, there is a lack of consensus on how wellness is defined across the few articles written to date. Definitions range from increased service accessibility (Harawa et al., 2020) to healthier lifestyles (e.g., healthy eating and increased exercise) and risk mitigation (e.g., decreased alcohol consumption) (Heeren et al., 2018; Oliveira et al., 2020). Target populations also differ from those at risk for HIV and other STIs (Harawa et al., 2020) to those living with HIV (Oliveira et al., 2020). In the African-American couples study, Eban both arms—HIV/STI risk reduction (intervention) and wellness/health promotion (control)—used a similar structure, which focused on increasing healthful behaviors, including physical activity, healthy eating, early detection and screening, improving medication adherence, and reducing alcohol and cigarette use (El-Bassel, Jemmott, et al., 2011; EBAN NIMH Multisite HIV/STD Prevention Trial for African American Couples Group, 2008a, 2008b, 2008c, 2008d). EBAN was developed using social cognitive theory and had an emphasis on a relationship-oriented ecological framework and Afrocentric paradigms, with an emphasis on improving behavioral intention, self-efficacy, and effective communication and problem-solving skills, which are key to mitigating chronic health conditions (El-Bassel et al., 2016; El-Bassel, Jemmott, et al., 2010). To ensure appropriateness for the target population of African-Americans with HIV or a partner living with HIV, the study tested both the efficacy of an HIV/STI intervention aimed at reducing risk among serodiscordant African-American couples and the efficacy of a health promotion intervention in addressing targeted knowledge regarding heart disease, hypertension, stroke, and certain cancers, and behavioral skills to address wellness outcomes to the population, and specifically included chronic health concerns, equity, and access issues (El-Bassel, Gilbert, et al., 2010).
A growing body of research indicates the potential effectiveness of couples-based interventions for improving health outcomes (El-Bassel et al., 2019; El-Bassel, Gilbert, et al., 2010, 2011; Gilbert et al., 2018; Jiwatram-Negron & El-Bassel, 2014; NIMH, 2010). However, while couples-based wellness behavioral interventions have shown great promise, their representation among RCTs is minimal (El-Bassel, Gilbert, et al., 2011). One study indicated the effectiveness of couples-based wellness, mental health, and psychological well-being interventions for older couples (Carmack et al., 2021). Findings suggest that interventions addressing depressive symptoms and adherence to HIV medication protocols are more effective with couples than if they were administered to individuals (Shtompel et al., 2020; Tuthill et al., 2019). It is important to note that while, at this time, there is naturally limited literature on how COVID-19 might affect couples-oriented substance use interventions, several studies suggest that the necessary isolation during the pandemic worsened mental health conditions, particularly among people in difficult living and working conditions, as well as those under financial stress (Avena et al., 2021).
Utilization of Wellness Interventions as Control Arms
The Social Intervention Group (SIG) has a long history of using wellness interventions as control conditions for HIV/STI behavioral health RCT interventions and culturally tailoring these interventions. Project EBAN included significant Community Advisory Board (CAB) involvement from study design through implementation and interpretation of results, and the intervention staff was reflective of the participants (Mott & Crawford, 2008). EBAN laid the groundwork for additional SIG wellness control interventions, notably CONNECT 2 (described here) in this paper, Connect “N” Unite (Wu et al., 2011), WORTH (El-Bassel, Gilbert, Goddard-Eckrich, et al., 2014), Project Renaissance (El-Bassel, Gilbert, Terlikbayeva, et al., 2014) and, more recently, a peer-based HIV self-testing study among HIV-uninfected female sex workers who inject drugs in Kazakhstan (National Institutes of Health, 2022). While we will not be discussing all of these interventions in this paper, it is worth noting that modifications were made to adapt each wellness intervention for demographic/population differences. Table 1 compares these interventions, the wellness components employed, and other key study details.
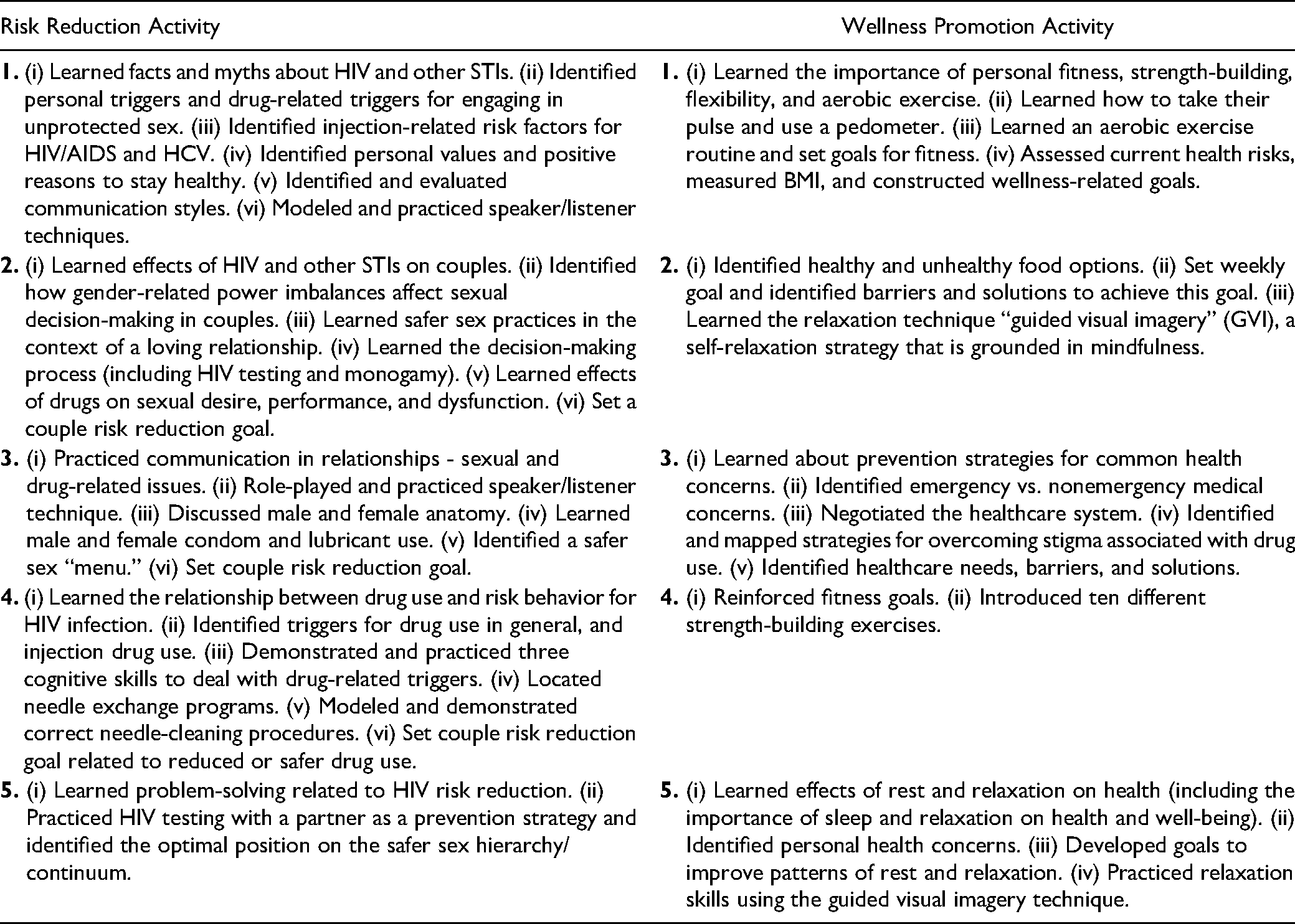
In response to the urgent need to deploy proven chronic disease prevention efforts among low-income men and women who use drugs, this paper reports on outcomes from a wellness intervention that served as one of the comparison conditions in Project CONNECT 2, a NIDA-funded HIV/STI Prevention Trial that tested the efficacy of an HIV/STI risk reduction intervention for drug-involved couples in New York City and was previously published (El-Bassel, Gilbert, et al., 2011). The Wellness arm of the CONNECT 2 RCT was designed to increase healthy behaviors, including increasing physical activity and healthy dietary practices, reducing and ceasing alcohol use, practicing early detection, reducing stress, improving medication adherence for hypertension, and improving communication with primary physicians (El-Bassel, Gilbert, et al., 2011). Table 2 outlines the Wellness Intervention components. We hypothesized that couples assigned to the seven-session wellness promotion intervention that served as an intentional comparison condition would have better nutrition and more physical activity than couples assigned to the seven-session couple-based intervention to reduce STIs and HIV (El-Bassel, Gilbert, et al., 2011).
CONNECT 2 Wellness Promotion Intervention Components.
Method
This paper presents an analysis of the effectiveness of a wellness intervention used as an RCT control arm in a population of heterosexual adults in New York City in an intimate relationship in which at least one person had recent HIV and substance use risk factors. An evaluation of the intervention effect on outcomes among the three RCT arms of CONNECT 2 has been reported elsewhere (El-Bassel, Gilbert, et al., 2011). In this paper, we present measurements and study designs used to analyze the efficacy of wellness interventions as control arms when compared to other intervention arms in RCTs.
Design
We conducted the CONNECT 2 RCT between November 2005 and September 2010 in New York City. The Institutional Review Board of Columbia University approved the study. Research assistants recruited participants through needle/syringe programs, homeless shelters, street outreach, food pantry/ food bank, and word-of-mouth (El-Bassel, Gilbert, et al., 2011). We screened 1,116 individuals, and 282 heterosexual couples were randomized. Eligibility criteria for couples included: (1) both were 18 years of age or older, and at least one partner was between the ages of 18–40; (2) both tested HIV-negative using OraQuick and OraSure assays; (3) both identified each other as their main sexual partner; (4) both reported being together for at least six months; (5) both reported that they intended to remain in a relationship for at least one year; (6) at least one partner reported using illicit drugs in the prior 90 days and was seeking or currently in drug treatment; (7) at least one partner reported having had unprotected intercourse with the other in the prior 90 days; (8) at least one partner had one or more HIV risk criteria. More details on HIV risk criteria are described in a previous publication (El-Bassel, Gilbert, et al., 2011).
We randomized couples to one of three interventions and used the gender of the index partner (i.e., the partner who reported drug use) as a blocking factor to ensure that the number of couples with substance use was balanced across the interventions (El-Bassel, Gilbert, et al., 2011). One partner was randomly designated as the index participant if both partners met substance use eligibility criteria (El-Bassel, Gilbert, et al., 2011).
Intervention
CONNECT 2 Intervention Arms
The intervention sessions were divided into three arms: (1) couple-focused wellness promotion, (2) couple-focused HIV/STI risk reduction, and (3) individual risk reduction. Risk reduction interventions have been previously described in another publication (El-Bassel, Gilbert, et al., 2011). Each arm consisted of seven weekly structured two-hour sessions delivered by a male or female facilitator who was matched to the gender of the index participant (El-Bassel, Gilbert, et al., 2011). All sessions were digitally audio-recorded to ensure that quality assurance (QA) procedures were met in all intervention sessions. In addition, the fidelity of implementation of all three conditions was recorded using session-specific QA checklists that were reviewed. Weekly corrective feedback was provided to facilitators when needed.
CONNECT 2 Wellness Intervention
The CONNECT 2 Wellness Intervention was guided by Social Cognitive Theory (Bandura, 1989; El-Bassel, Gilbert, et al., 2011), which has been applied to other wellness and health promotion interventions (“Eban health promotion intervention: conceptual basis and procedures,” 2008; El-Bassel et al., 2016; El-Bassel, Gilbert, et al., 2011; El-Bassel, Gilbert, Terlikbayeva, et al., 2014; El-Bassel, Jemmott, et al., 2010; El-Bassel, Jemmott, et al., 2011; Heeren et al., 2018; Jemmott et al., 2011, 2019, 2021; Martinez et al., 2017; Tsheko et al., 2021). The components of the wellness promotion intervention focused on (1) maintaining a healthy diet; (2) promoting physical fitness in daily routines; (3) promoting age-appropriate recommendations for screening for common diseases such as cancers, heart disease, and diabetes; (4) improving access to healthcare services by identifying and addressing service barriers; and (5) learning stress-reduction exercises (see Table 2). Participants learned the importance of personal fitness, strength-building, and aerobic exercise, as well as how to check their pulse and how to use a pedometer. Participants also assessed and evaluated their current health risks and measured their body mass index (BMI). They were also taught about nutrition and meal planning, including identifying healthy and unhealthy food options. Participants learned about prevention strategies for common health concerns
The CONNECT 2 Wellness Intervention differed from the HIV risk reduction intervention parent intervention by focusing on improving non-HIV health outcomes by using brainstorming, games, videos, experiential exercises, discussions, and skill-building activities to increase self-efficacy, outcome expectancy, behavioral skills, and wellness knowledge. However, both interventions consisted of five weekly structured two-hour sessions delivered by facilitators. A total of 489 individuals were randomized across the three arms and 190 to the wellness promotion. Attendance and participation at intervention sessions for all three conditions were high (El-Bassel, Gilbert, et al., 2011). More details on participant recruitment and retention are described in a previous publication (El-Bassel, Gilbert, et al., 2011).
Measures
We conducted repeated assessments of sociodemographic and intervention-specific outcomes at baseline before the intervention, Immediate Post-Test (IPT), and at six months and 12 months post-intervention via Audio Computer-Assisted Self-Interviewing (ACASI) at a centrally located community research office. The ACASI enabled participants with low literacy to respond to questions by providing audio of the question and response options. Participants were reimbursed for completing assessments and intervention sessions.
Both Risk Reduction arms assessed outcomes related to substance use and HIV risk reduction. The Wellness arm assessed outcomes related to nutrition/diet, exercise/physical activity, engagement in health care, and ratings of participants’ comfort with handling their medications, navigating stigma associated with drug use, and seeking medical care at baseline and all follow-ups; these outcomes constitute the focus of this paper and analyses presented herein.
Researchers collected data at baseline and all follow-ups on physical activity and eating behaviors in the past 90 days, including the number of fruits and vegetables consumed and the amount of physical activity performed. The National Cancer Institute’s seven-item food frequency questionnaire assessed fruit and vegetable consumption (El-Bassel, Gilbert, et al., 2011). To assess physical activity, we used the CDC three-item questionnaire to measure physical activity and strength-building activities (El-Bassel, Gilbert, et al., 2011).
Healthy versus Unhealthy Eating Habits
To assess “Healthy versus Unhealthy Eating Habits,” we used the seven National Cancer Institute for five-a-day studies seven-item food frequency questionnaire to assess fruit and vegetable consumption (Thompson & Byers, 1994). This primary outcome was a binary variable that measured if participants met the five-a-day guideline of consuming five or more servings of fruits and vegetables daily in the previous 30 days. We also measured the number of daily servings of fruits, vegetables, and a combination, as well as daily consumption of fatty or fried food (eating and cooking with fat) in the previous 30 days.
Exercise Habits
We assessed physical activity with three items developed by the Centers for Disease Control and Prevention (2001), which assessed the number of days participants participated in at least 20 minutes of vigorous-intensity aerobic physical activity, strength-building activities, and moderate-intensity aerobic physical activity for at least 30 minutes. The primary outcome was a binary variable on whether participants engaged in strength-building activity on two or more days and engaged in at least four days or 30 minutes of moderate-intensity activity or 20 minutes of vigorous-intensity activity on at least five days (U.S. Department of Health and Human Services, 2008) Other outcomes included strength-building activities and the number of days of moderate or intensive cardiovascular activity over the previous seven days.
In addition, sociodemographic characteristics were collected, including gender, age, race/ethnicity, marital status, years of education, employment status, monthly income, history of homelessness, types of community correction settings in which they had enrolled in the past 90 days, and the number of times they were arrested or incarcerated.
Statistical Analysis
To test the hypotheses that wellness efficacy was increased, scores in healthy eating and exercise habits, and reductions in poor eating habits, multilevel linear models were used due to nonindependence in observations. Random effect parameters were included in the model to account for dependencies due to dyadic data and repeated measures. Each model included treatment assignment and follow-up time point and interaction terms between treatment assignment and time point, and also adjusted for gender and the baseline measures of the outcomes. The regression coefficient and its corresponding 95% confidence intervals (CIs) were reported as intervention effects for the total sample (i.e., couple wellness promotion vs. combined risk reduction [combining couple risk reduction and individual risk reduction]) and the subgroup analysis (i.e., couple wellness promotion vs. couple risk reduction) (Figure 1).
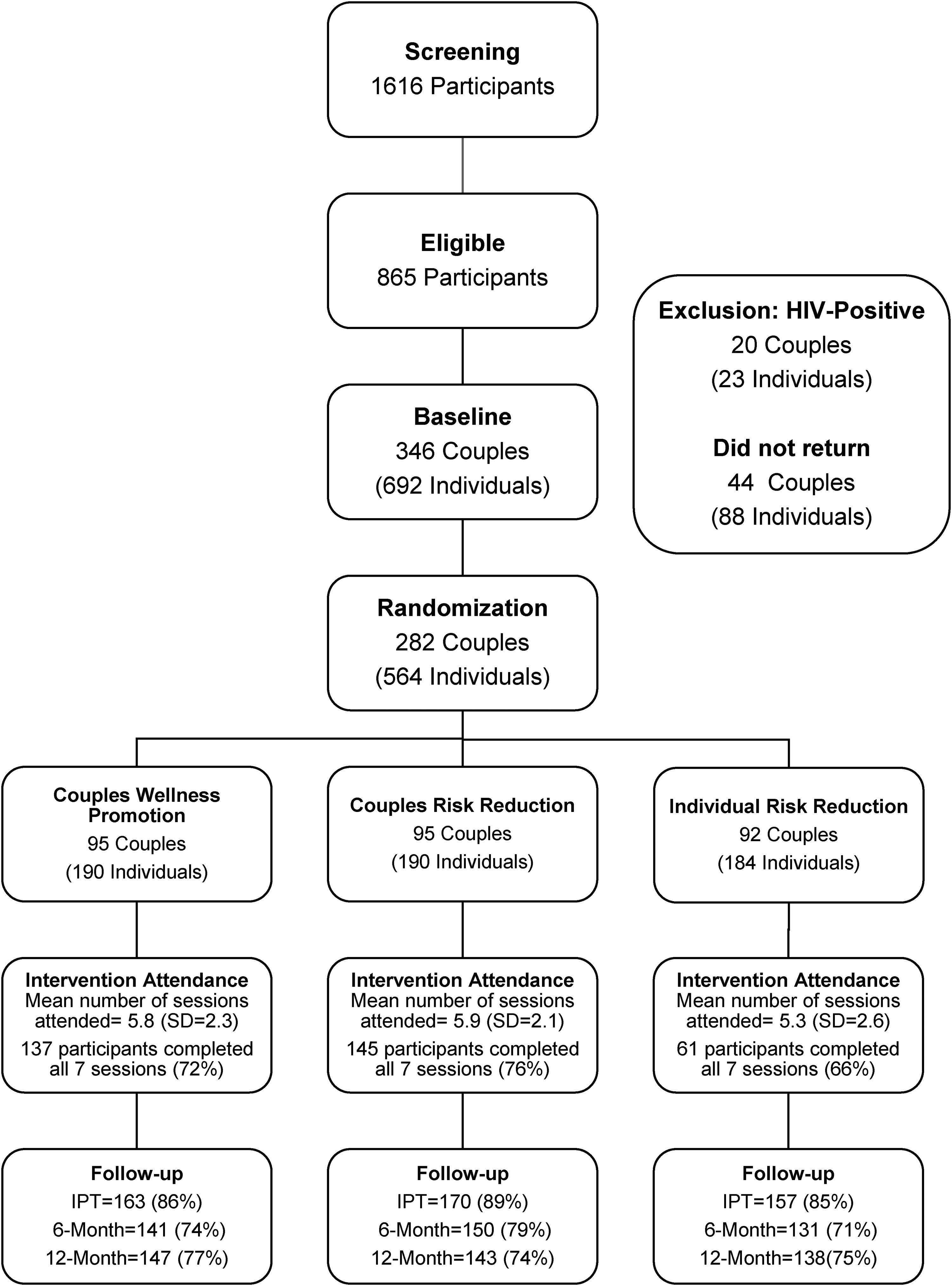
CONNECT 2 CONSORT form by intervention arm.
Results
Background Characteristics
The participants” sociodemographic characteristics, substance use, and criminal justice history are reported in Table 3. The mean age of participants was 36.48 years (SD = 7.12). Almost half (N = 268; 47.60%) of participants identified as Black or African-American, 158 (28.06%) identified as Latino, and 65 (11.55%) identified as white. Close to half (N = 241, 42.81%) were married. Most of the sample (N = 357; 63.41%) finished high school or higher education. The majority of the sample (N = 423; 75.13%) participants were low-income, reporting less than $400 in income a month, and 311 (N = 55.24%) participants reported a history of homelessness. More than half (N = 326; 57.90%) of the participants had been in prison or jail. Almost all (N = 542; 96.2%) participants reported using illicit drugs in the past 30 days. No significant differences were found in any of the characteristics by study condition.
Demographics, Reported Substance Use, HIV/STI Status, and Criminal Justice Involvement in the 30 Days Before Baseline.
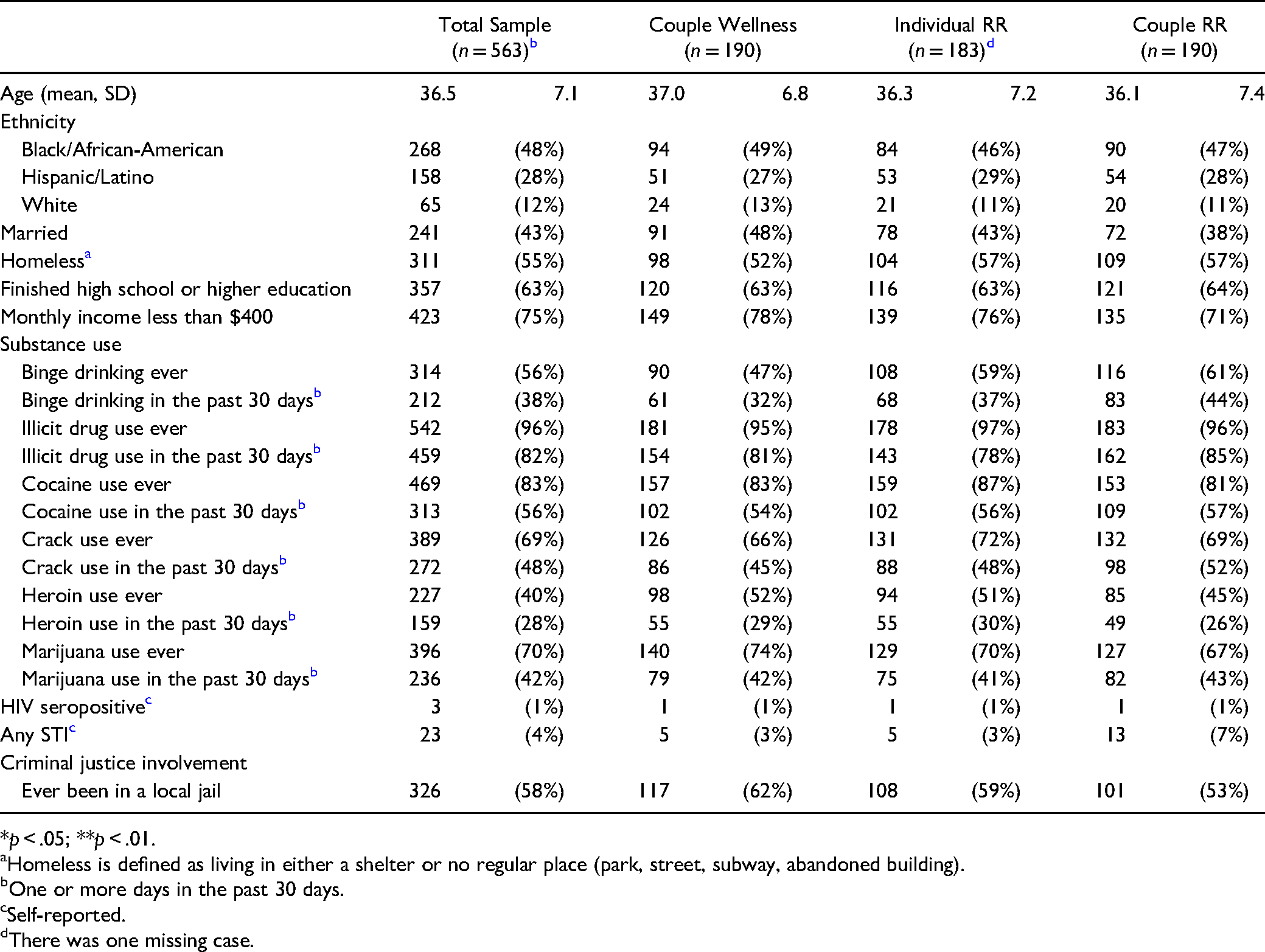
*p < .05; **p < .01.
Homeless is defined as living in either a shelter or no regular place (park, street, subway, abandoned building).
One or more days in the past 30 days.
Self-reported.
There was one missing case.
Figure 2 shows the means and 95% confidence intervals for eating habits and physical exercise at the baseline and each follow-up assessment by treatment assignments. Couple Wellness Promotion participants reported significantly more frequencies for exercise in the past 90 days than the participants assigned to Couple Risk Reduction at IPT (23.1 [95% CI = 19.8, 26.4] vs. 15.8 [95% CI = 12.7, 18.9]) and 12-month follow-up (19.0 [95% CI = 15.5, 22.6] vs. 12.5 [95% CI = 9.6, 15.4]).
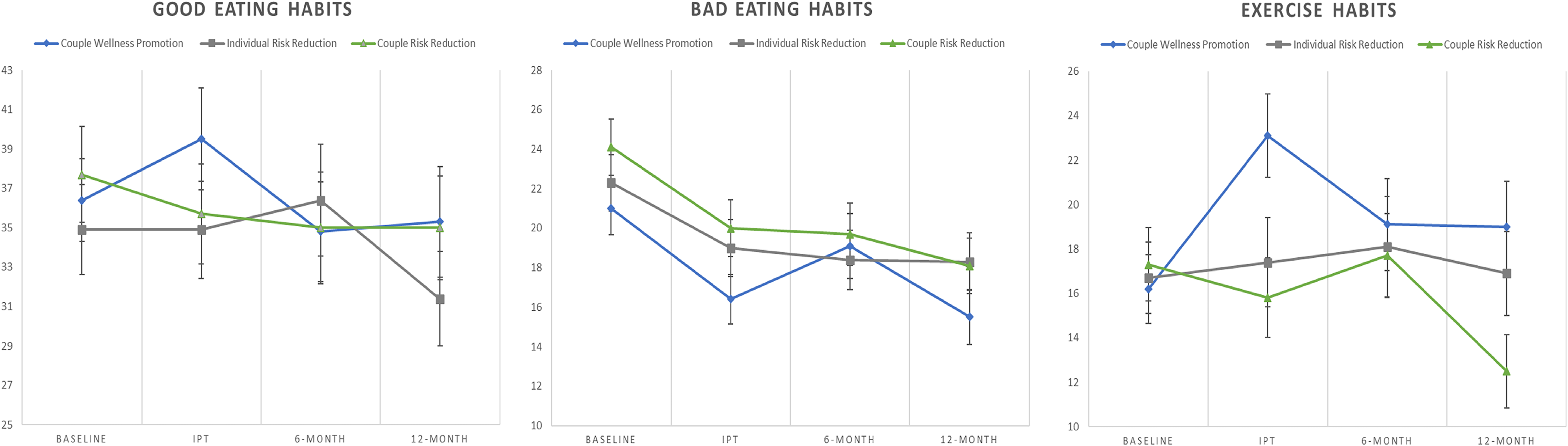
Summary of eating habits and exercise (frequency per month) at baseline, immediate post-intervention test (IPT), and 6- and 12-month follow-up assessments with 95% confidence intervals.
Wellness Outcomes
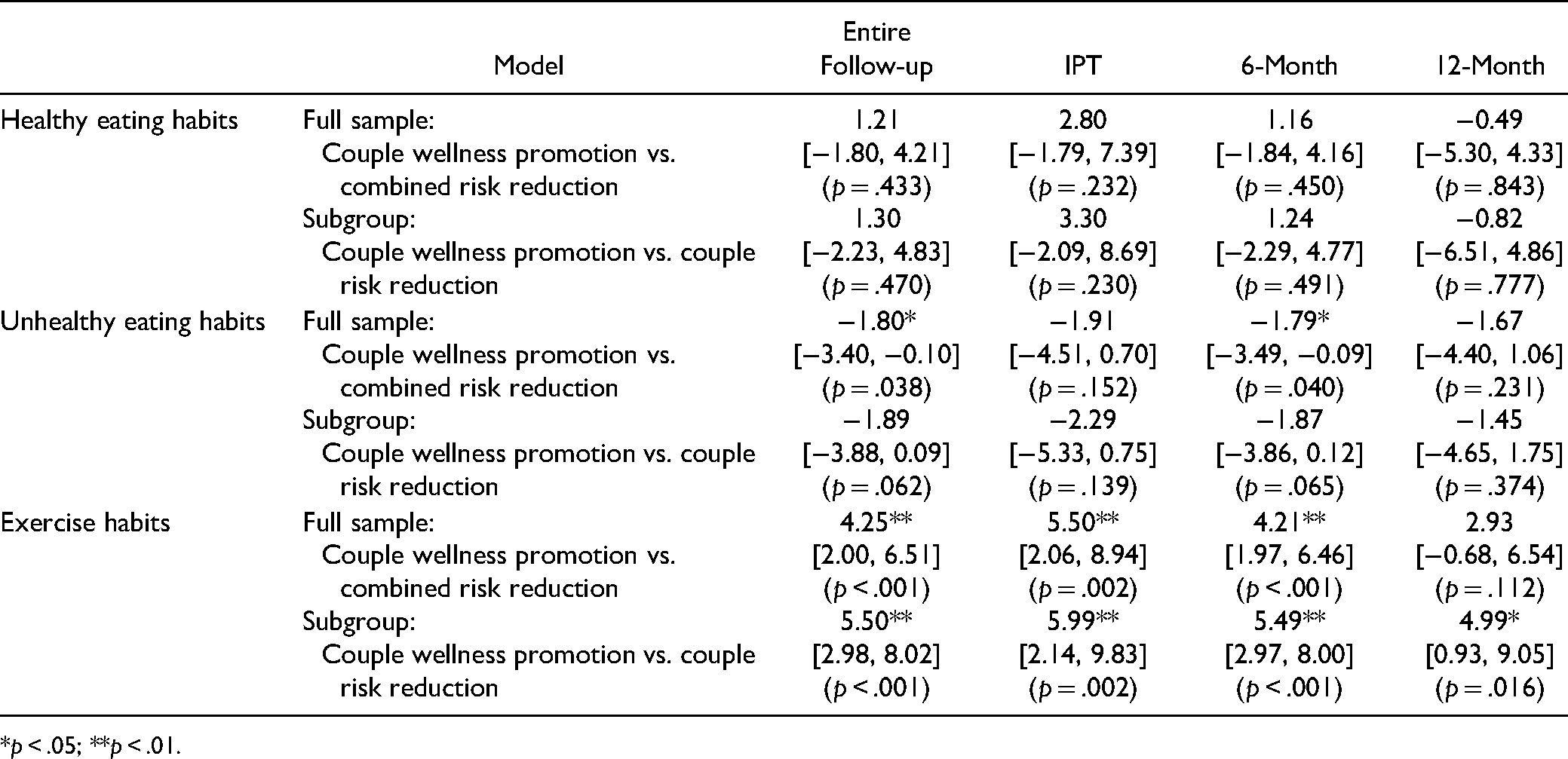
Table 4 presents results from multilevel regression models for eating habits and physical activity outcomes for the total sample that compares couple wellness promotion versus Combined Risk Reduction (combining Couple Risk Reduction and Individual Risk Reduction) and the subsample that compares couple Wellness Promotion versus couple Risk Reduction. Couple wellness promotion participants reported significantly lower frequencies of unhealthy eating habits than combined risk reduction participants during the entire follow-up period (b = −1.80, 95% CI = −3.40, −0.10; p = .038). Participants in couple wellness promotion also reported significantly more exercise per month than participants in combined risk reduction across the entire follow-up period (b = 4.25, 95% CI = 2.00, 6.51; p < .001), at IPT (b = 5.50, 95% CI = 2.06, 8.94; p = .002), and 6-month follow-up (b = 4.21, 95% CI = 1.97, 6.46; p < .001). From the results of the subsample group analysis, participants in couple wellness promotion had significantly more exercise in the past 90 days than couple risk reduction participants over the entire follow-up period (b = 5.50, 95% CI = 2.98, 8.02; p < .001), and also at IPT (b = 5.99, 95% CI = 2.14, 9.83; p = .002), 6-month follow-up (b = 5.49, 95% CI = 2.97, 8.00; p < .001) and 12-month follow-up assessment (b = 4.99, 95% CI = 0.93, 9.05; p = .016).
Results from Multilevel Models for Eating Habits and Exercise (Frequency per Month) in the Past 90 Days: Effect Estimates, 95% Confidence Intervals, and p-Values.
*p < .05; **p < .01.
Discussion and Applications to Practice
These study findings advance the evidence base of couple wellness interventions and wellness interventions as active comparison conditions. To our knowledge, this is the first RCT to find significant effects of a couples’ wellness promotion intervention for improving the frequency of physical fitness as well as reducing the frequency of poor eating habits among low-income couples who use drugs. The high rates of poor nutrition and low physical activity at baseline underscore the critical need to focus on chronic disease prevention and treatment efforts among those impacted by HIV risk and substance use. This study addressed key priorities of the Healthy People 2030 strategy (Hasbrouck, 2021; Levine, 2021); the NIH All of Us initiative, including reducing chronic disease, mental illness, and health disparities (Jones-Schenk, 2019); intensifying prevention efforts in heavily at-risk populations in concentrated areas (Hasbrouck, 2021; Levine, 2021); and increasing access to a continuum of evidence-based chronic disease prevention and treatment services for low-income populations (Lazar & Davenport, 2018).
Overall, the CONNECT 2 couple wellness promotion intervention was more efficacious than the risk reduction interventions collectively at reducing unhealthy eating habits across the entire follow-up observations, as well as specifically at the six-month follow-up time point. The couple wellness promotion intervention was more efficacious than the risk reduction interventions collectively, as well as the couple risk-reduction specifically, at improving exercise habits across the entire follow-up observations, as well as specifically at the IPT and six-month follow-up time points. Altogether, the magnitude and consistency of findings across wellness behavior outcomes in this study promote confidence in the efficacy of this wellness promotion intervention, ultimately providing support for the couple wellness promotion intervention being able to improve self-reported wellness behaviors among low-income couples who use drugs.
CONNECT 2 wellness promotion results are consistent with EBAN and prior research that has used wellness promotion interventions as attention control conditions (El-Bassel, Jemmott, et al., 2010; Mott & Crawford, 2008; NIMH, 2008). Therefore, there are important implications for future research about how to advance the evidence base and scale up these wellness promotion interventions (e.g., hybrid type 1 and 2 implementation trials of evaluating these interventions in real-world settings). First, there is a need for future research to examine the impact of improved general health outcome attainment on risk behaviors such as substance use and HIV. Second, a greater examination of a couples-based wellness intervention's effects on reducing healthcare distrust, which was highlighted during the COVID-19 pandemic, may provide an opportunity to increase general engagement in care and prevention recommendations for communities of color. Interventions that aim to improve health need to include core components of strengths and resiliency, social support, community networks, and access to federally qualified health centers, local clinics, and faith-based organizations. These organizations may play a role in promoting wellness interventions among their congregants and communities among some racial minority groups. The role of faith-based organizations in this arena increased significantly during the COVID-19 pandemic, where we saw and still see faith-based organizations being a hub for vaccine distribution and COVID-19 testing sites (Evans et al., 2021; Levin et al., 2022; Thompson et al., 2021).
The challenges of engaging low-income communities of color who use drugs when conducting clinical research are complicated, and include medical mistrust, fear, cultural differences, extra costs, and lack of awareness or knowledge of clinical trials; further, research language often excludes minorities (Ard et al., 2003; 1996; Jaiswal & Halkitis, 2019; National Academies of Sciences, Engineering, and Medicine et al., 2016; Rivers et al., 2013; Thompson et al., 2021). Additionally, many communities do not want to be associated or labeled with particular problems like high HIV/STI rates or substance use problems. Despite these challenges, we found high retention rates among both studies described. Although there is limited literature to guide the implementation of wellness interventions as control conditions for RCTs with drug-involved populations, including couples, we anticipate that there will be growing attention to this matter in light of increasing awareness of national health disparities. Further research is needed to determine whether wellness interventions such as EBAN and CONNECT 2 enhance effective case management and social work practice, especially in nonclinical settings and settings with limited supervision.
Several study limitations must be considered when interpreting these results and justifying wellness interventions as control arms for future RCTs and social work interventions. First, while self-reported data introduces the risk of participants providing socially desirable responses, the use of ACASI may have reduced that risk to self-report validity. Second, the effects we note are likely generalizable to a similarly vulnerable, substance-using, low-income population; however, participants who were motivated to receive study incentives may have been more likely to enroll in, and complete, study components. The small sample size prevents generalizing the findings to other people who use drugs.
The CONNECT 2 Wellness intervention controlled for Hawthorne effects (special attention and group interaction) which should be considered for future wellness intervention control conditions (Sedgwick & Greenwood, 2015). Lastly, the costs of funding wellness interventions as control arms need to be considered as a potential limitation. However, it is estimated that obesity costs between $147 billion and $210 billion a year in the United States, as well as loss of productivity due to illness and premature death (Faruque et al., 2019). Therefore, cost-effectiveness should be included in the outcomes of future wellness control interventions (Wang et al., 2011). Some researchers have been critical of Wellness interventions, specifically if they address the multiple challenges of research, including study design in relation to addressing the research question, how bias can be addressed in the control, and if they are feasible and ethical, as these need to be addressed to maximize validity in future research (Byrd-Bredbenner et al., 2017; Kinser & Robins, 2013; LaFave et al., 2019). Finally, the suggested intervention model was tested in one country and was tested on two minority groups (Black and Latinx). Therefore, to generalize the present study results, it would be essential to test the suggested bicultural model in social work with other ethnic minority, immigrant, and racial groups.
CONNECT 2's findings have important implications for implementing and disseminating general health information to this population, which may be integrated with HIV/STI risk reduction, substance use treatment, and even Covid-19 interventions. High rates of session attendance and retention at the 12-month follow-up may indicate high motivation among low-income, drug-involved couples to participate in wellness interventions.
Two primary conclusions emerge from our findings. First, a focus on wellness that had significant findings, comparable to that of the risk reduction intervention. This finding is relevant for public health interventions, especially for communities of color and underserved populations. Second, the couple-oriented intervention enjoyed sustained gains over the individual intervention, offering the potential for promoting resilience among couples during a time of prolonged duress such as substance abuse or during a pandemic (e.g., COVID-19). Please note that pandemic-related risk avoidance fatigue may blunt the effectiveness of risk reduction interventions even more than our findings suggest.
As the efficacy of couple-based wellness interventions continues to be solidified, we recommend that CONNECT 2's findings be used to improve health outcomes in low-income populations via the use of wellness interventions as control arms. These intervention strategies may be scaled up to curb the continued increase in substance use, chronic disease, and HIV among low-income populations while offering sustained gains in health-promoting behaviors, including engagement and adherence to healthcare recommendations. In addition, these strategies are compatible with a range of substance use and harm reduction settings to reduce chronic disease and other poor health behaviors among low-income, urban neighborhoods whose residents are at risk for morbidity and premature mortality from chronic diseases. Given the disproportionate impact of the COVID-19 pandemic on marginalized populations, wellness interventions like CONNECT 2, which focuses on health research equipoise and is a practical strategy to address the under-representation of marginalized groups in RCTs, are sorely needed and will provide worthwhile evidence for researchers, practitioners, and policy-makers.
SIG leadership has worked with marginalized populations for over 30 years, so we hope this description of our positive outcomes and intervention core components of the CONNECT 2 and EBAN trials help social workers, and other researchers, consider and plan for similar interventions for future RCTs to evaluate social and behavioral interventions. Future studies need to examine more deeply the specific social determinants that cause poor outcomes OR are barriers to positive health outcomes including the many layers of structural and institutional racism. By doing so, wellness interventions have an opportunity to be a system change model that should utilize community-based participatory research strategies to target culturally tailored interventions to serve not only low-income marginalized populations. EBAN and CONNECT 2 prioritized community involvement in all study design and development components, and staff included high numbers of people of color from the community. This equity lens is key to engaging hard-to-reach populations for future research. These practices and partnerships can also help increase response to community needs, community trust, quality of intervention development, and testing and uptake of the interventions. Researchers should be encouraged to publish results of control arms, particularly wellness control arms, in academic and nonacademic literature. By publishing the results of wellness control arms, researchers may advance health equity in study design and the evidence base for wellness interventions as a replacement for TAU. Future research should also include a systematic review and meta-analysis assessing the impact of wellness control arms and look at the impact of these wellness control arms for future uptake/considerations and sustainability.
By replacing TAU for HIV/STI RCTs with wellness interventions, we hypothesize that medically underserved populations in the United States and those internationally impacted by chronic illness, substance use disorders, and COVID-19, will have increased access to care, social support, and improved health outcomes, which may not have otherwise been accessible to them. Thus, a call is needed to encourage social work researchers to take the lead in developing and testing wellness interventions to improve health outcomes, to test the impact of different modalities for vulnerable populations aggressively, and measure the benefit to society.
Footnotes
Authors’ Note
This paper was submitted as a contribution to the special issue of Research on Social Work Practice. It consists of research originating within the Social Intervention Group, School of Social Work, Columbia University, guest edited by Nabila El-Bassel and Louisa Gilbert.
Amar Mandavia, Department of Psychiatry, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA, USA.
Acknowledgments
The authors also want to thank the facilitators of the CONNECT 2 intervention and project Research Assistants. Finally, we wish to acknowledge the editorial contributions of Allison Krug, MPH.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by funding by the National Institutes of Drug Abuse to Dr. N.E.B. (NIDA R01DA16993). This study is registered with Clinical Trials.gov number NCT01285349.