
Abstract
Objectives
Despite tremendous gains in the U.S.’ fight to end the HIV epidemic, health equity goals of “reducing—and, ultimately, eliminating” HIV disparities and its determinants among marginalized Black and Indigenous People of Color (BIPOC) remain largely unrealized (Braveman, 2014; CDC, 2019a). In fact, “progress has stalled” among BIPOC at greatest risk for new transmission and the need for culturally tailored prevention interventions remains paramount (CDC, 2019b). Among cisgender Black/African-American women (hereafter referred to as “Black”), the risk for new transmission remains most acute when compared to all other women (CDC, 2021). Encouraging declines notwithstanding, Black women remain 13 and 5 times more likely to be living with HIV/AIDS when compared with their White and Latina counterparts, respectively (CDC, 2021; KFF, 2020). Nationwide, six out of 10 new HIV cases remain among Black women despite making up less than 15% of the U.S. population (CDC, 2021; Ojikutu & Mayer 2021). Nine out of 10 new cases among women aged 18–25 years old are among Black women, 84% of which result from heterosexual encounters (Pittman, 2019).
Cis-Black women who use drugs and alcohol and complete criminal legal sentences while living in the community (e.g., probation, parole, court-ordered drug stays, etc.) have long been identified as an especially vulnerable subgroup (El-Bassel et al., 2014; Gilbert et al., 2021). Substance use among Black women on probation and other forms of criminal legal problems are also disproportionately high. Three-fourths of a recent sample of 243 African-American women in carceral settings reported a drug problem (Oser et al., 2016), when compared with 45% of all women on probation (The Pew Charitable Trusts, 2018) and 15% among women in the general population (NIDA, 2020). Largely attributed to intersecting individual, interpersonal, and highly racialized systemic risks, those who face these challenges concurrently also report significantly higher levels of system mistreatment (Whiteside-Mansell et al., 2021). They are far more likely to be unfairly targeted by racialized drug laws, aggressive- and over policing, and disproportionately high criminal legal system sentences (Whiteside-Mansell et al., 2021). Identified as key social and structural drivers of the HIV/sexually transmitted infections (STI) epidemic (Seeley et al., 2012), these racialized criminal-legal risks are also positively associated with high levels of system distrust (Dyson et al., 2017), a decreased desire to engage in prevention and intervention services (Hoff et al., 2022), and are believed to be significantly associated with lags in the U.S.’ efforts to attain health equity goals among BIPOC women (McCree et al., 2016). It is therefore not at all surprising that Black women who experience these barriers at once (i) have been characterized as “hard to engage” (Windsor et al., 2014); and (ii) are less likely to endorse “one size fits all” HIV prevention interventions (Hoff et al., 2022).
Although peer-reviewed literature suggests that culturally tailored HIV prevention interventions are more effective for Black women in general there have been no evidence-based HIV prevention interventions designed for the large number of Black women in community supervision programs who remain at high risk for HIV and other sexually transmitted infections (El-Bassel et al., 2010; Jemmott, Jemmott, & O’Leary, 2007; Wingood et al., 2013a; Wingood et al., 2013b). And given this gap, to date, Black women in community corrections have yet to be engaged as health equity partners in the adaptation of an HIV prevention intervention tailored specifically for them. A 2017 scoping review of evidence-based HIV interventions delivered to criminal legal system-involved populations underscored this critical gap in evidence-based interventions (EBIs) (Meyer et al., 2017). Only one out of the 42 interventions reviewed, or less than 3%, specifically targeted drug-involved women in the criminal legal system. Women on the Road to Health (WORTH), the intervention identified, was shown to be efficacious in reducing HIV/STI risks among women in community corrections from various racial and ethnic backgrounds who misuse substances (El-Bassel et al., 2014). As illustrated by a 2018 systematic review of adaptations of evidence-based public health interventions that took into consideration all domains of adaptations from content to context, cultural modifications, and delivery, a significant gap remains regarding interventions targeting drug-using, Black women in community corrections specifically (Escoffery et al., 2018).
Little to no attention has also been paid to microlevel strategies for redressing health equity gaps (CDC, 2010; McCree et al., 2016; National Academies of Sciences, 2017). In terms of HIV EBIs specifically, there are no HIV EBI development or adaptation models that have explicit health equity in focus. None, for example, describe how to equitably share power with at-risk BIPOC individuals as a whole, and Black women in particular, in determining the content and direction of interventions targeting this group.
Enhancing engagement and shared decision-making power of peers with lived experience and other key community stakeholders is critical to designing interventions that are positioned to achieve health equity. Although no peer-reviewed manuscripts have been published to date with “health equity” and “HIV prevention” in the title, manuscripts have long described ways to operationalize health equity when engaging populations at increased/higher risk for health disparities. In addition to shared decision-making power, recommended strategies include ensuring a multidimensional focus on outcomes at the community, policy, and personal levels, the centering of diversity and inclusion, and ensuring that health equity was included as an explicit outcome of partnerships (Organizing Committee for Assessing Meaningful Community Engagement in Health & Health Care Programs & Policies, 2022). Other criteria include ensuring equity in terms of voice and decision-making power fostering mutual trust and value and establishing shared goals (Organizing Committee for Assessing Meaningful Community Engagement in Health & Health Care Programs & Policies, 2022; Woodward et al., 2019). In terms of HIV-related health equity prevention efforts targeting Black women, scholars have also emphasized the need to proactively identify social and structural determinants that may impede engagement (Bradley et al., 2019).
This article addresses these gaps in two ways. First, it describes processes used to adapt the 2009 version of WORTH intervention from an intervention designed for a general population of drug-using women in community corrections, to one targeting Black women specifically using an integrated ADAPT-ITT health equity adaptation framework (Wingood & DiClemente, 2008). Funded by the National Institutes of Drug Abuse, the newly adapted intervention (Empowering African-American Women on the Road to Health or “E-WORTH”) features an expanded tablet-based, multimedia platform, HIV/STI-specific Afrocentric themes of risk and resiliency, and an electronic narrator. Second, these authors employ a novel approach to adaptation by identifying equity considerations and challenges that emerged amidst efforts to engage substance-using Black women in community corrections with recent substance use histories (also referred to hereafter as “peers”) during the adaptation process. This approach advances the U.S. Department of Health and Human Services’ current health equity goals, defined in part as the “attainment of the highest level of health for all people…by…valuing everyone equally with focused and ongoing societal efforts to address avoidable inequalities” (CDC, 2010).
Methods
Application of ADAPT-IT Framework
We utilized the ADAPT-ITT adaptation framework (Wingood & DiClemente, 2008) to guide adaptation processes. ADAPT-ITT is an 8-phase model that details recommended steps when systematically adapting EBIs: (i) Assessment of target population; (ii) Decision (selecting which EBI to adapt and if it should be adopted as is, or adapted); (iii) Adaptation (adapting the intervention through the use of focus groups with target population); (iv) Production (creation of an adaptation plan); (v) Use of topical experts; (vi) Integration of feedback from topical experts; (vii) Training personnel; and (viii) Testing piloting adapted materials. Although not specifically health equity-focused, ADAPT-ITT engenders opportunities to collaborate with target populations in the adaptation process. The study was approved by the Columbia University (CU) institutional review board.
Original WORTH Intervention
The 2009 version of the WORTH intervention has been described in detail in earlier manuscripts (El Bassel et al., 2014), along with the study protocol (Johnson et al., 2018) and outcomes (Gilbert et al., 2021) for the effectiveness trial of E-WORTH which was conducted between 2014 and 2019. Designed for delivery in low-resourced community correction settings, the multimedia version consisted of four 90-minute group sessions and includes the use of narrative videos of four fictional characters portraying life stories of women affected by HIV/STIs, substance use, and legal system involvement. For the current effectiveness trial, WORTH was tailored for delivery in a “real world”, community reentry setting, by community reentry facilitators.
Below, we describe the steps we employed to develop the E-WORTH adaptation of WORTH guided by the ADAPT-IT framework with a health equity lens that included the prioritization of proposed enhancements made Black women in community corrections, full engagement in (i) designing the look and feel of the intervention, (ii) selection of narrative characters; and (iii) script preparation.
Development of Community Partnerships for E-WORTH
We partnered with Black women with recent substance misuse and criminal legal system involvement histories to serve as focus group participants and members of a Community Advisory Board (CAB) created to help guide the study design. CAB members also included (i) Black men with similar histories; (ii) leadership and frontline personnel from the largest nonprofit provider of behavioral health, educational, vocational, and HIV testing and counseling services to men and women on community corrections in New York City, many of whom themselves have similar histories; (iii) senior staff from the NYC Department of Probation; and (iv) representatives from various other nonprofits and city agencies serving legal system-involved populations.
We also entered into a service subcontract agreement with the nonprofit provider. The provider, which we refer to in this article as a “Non-governmental (NGO) community reentry provider” or “NGO”, has been in existence for 50 years and has service locations in Manhattan and Queens, New York. Both sites were designated as E-WORTH study locations. New York City Department of Probation sites served as recruitment locations and Columbia's Center for Technology and Learning (CTL) was charged with revising the multimedia platform used during the prior WORTH trial.
Table 1 shows the specific changes made to the WORTH intervention, as guided by each ADAPT-ITT step. It also describes microlevel health equity considerations when engaging peer partners, associated with each ADAPT-ITT phase, where applicable.
Integrated ADAPT-ITT Framework With a Health Equity Lens.
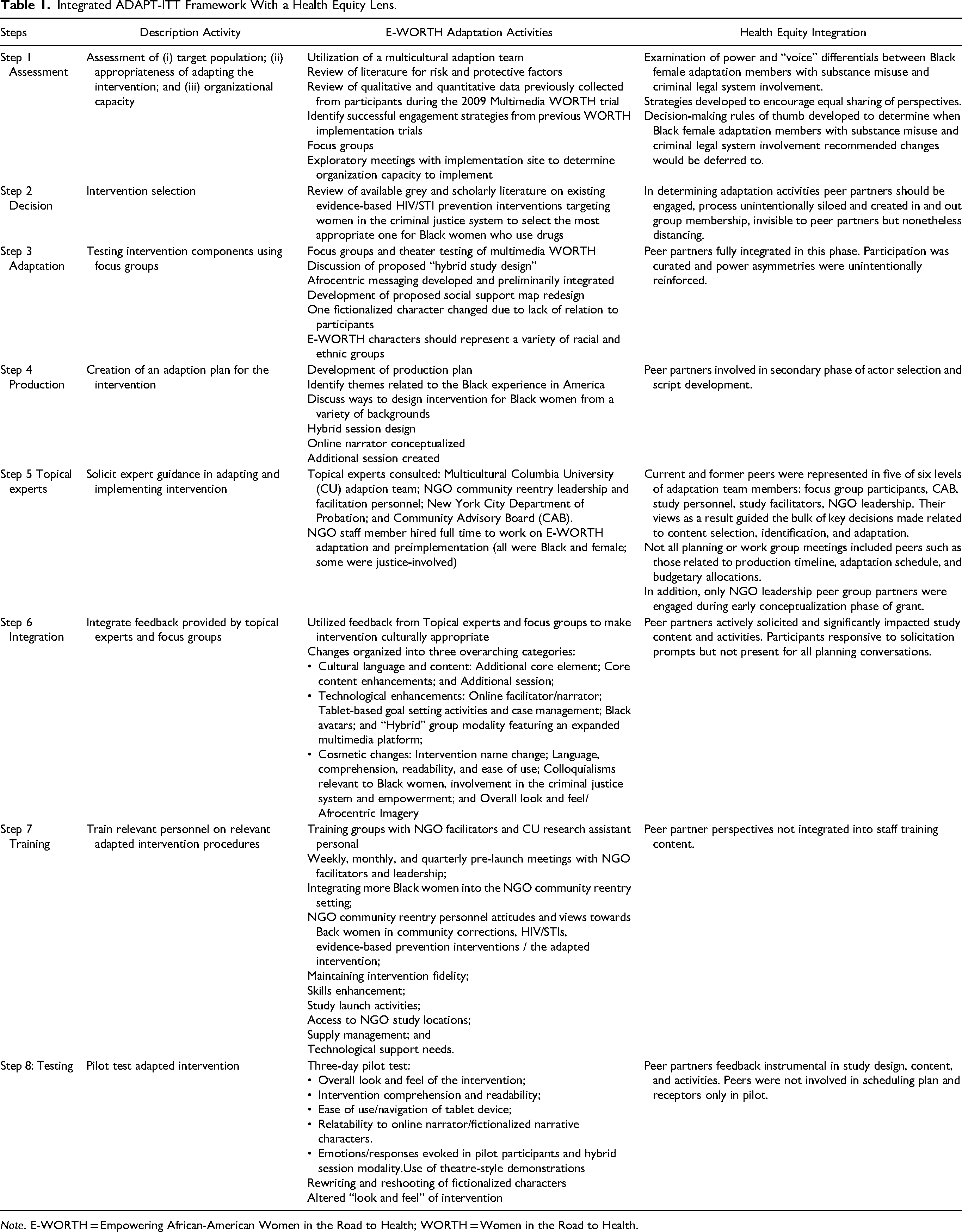
Note. E-WORTH = Empowering African-American Women in the Road to Health; WORTH = Women in the Road to Health.
Phase 1—Assessment
During this phase, an eight-member multicultural CU adaptation team made up of four Black and four non-Black assembled for the project. The four Black were women from a variety of socioeconomic and criminal justice backgrounds, one of whom had spent time in prison and the remaining three were CU graduate students. The four non-Black team members were of different racial and ethnic backgrounds—two White, one Palestinian, and one of Asian descent. The adaptation team met approximately 1 year before the implementation. Through the lens of intersectionality (Crenshaw, 1991), eight CU adaptation members discussed intersecting identities (e.g., poverty, oppression, discrimination, and racism) that increases drug-using, legal system-involved Black women's risks for HIV/STIs to ensure that those identities were infused throughout the intervention. Four of the eight were Black women from a variety of socioeconomic and criminal legal system backgrounds.
Two focus groups were also held during this phase with five to six peer partners, between the ages of 20 and 60 years. Groups were held over nonconsecutive days and were facilitated by the study's project director and a Master's level student, both of whom were cisgender Black women. Participants spoke openly about overwhelmingly negative and/or violent encounters they have had with police, parole, and correction officers and paying and nonpaying sexual partners, their use of substances, and other risky sexual practices. They recommended the use of the term “Black” (vs. “African-American”) and reported no sensitivity in terms of references used in the multimedia platform categorizing criminal legal system involvement (e.g., community supervision, probation, parole, etc.).
Guided by ADAPT-IT, Black female team members varied with respect to years of research experience, authority and decision-making power, educational attainment, and socioeconomic status. Overall, peer and non-peer Black adaptation team members had less of each of these statuses when compared with their White counterparts. Although the ADAPT-ITT model does not provide specific guidance on how to negotiate team heterogeneity in terms of class, race, educational attainment, power, and status, a concerted commitment was made to encourage equal sharing of perspectives. In terms of health equity, in particular, recommendations made by peer and non-peer Black, female adaptation partners were prioritized when discussing proposed enhancements that were Afrocentric in nature (e.g., newly drafted language focusing on themes of race, risk, and resiliency, the overall look, and feel of the adapted intervention). The group also readily deferred to investigators regarding scientific decisions. Peer partners were not directly involved in the formulation of the grant or funding, or in the review of grey and scholarly literature to guide content which was a limitation of the adaptation process.
Phase 2—Decision
Leveraging data gathered during the Assessment Phase, through team consensus, we confirmed that Multimedia WORTH was the best intervention to select for this population. Team members also deemed it necessary to “adapt” the 2009 version of the WORTH intervention (another key tenet of the Decision Phase). Towards this end, non-peer team members reviewed 2009 Multimedia WORTH trial activities and core elements when considering how to infuse relevant cultural, historical, and social Afrocentric content.
While the selection of WORTH was optimal since it was the only evidence-based HIV prevention intervention of its type and deemed highly efficacious across trials for women in community corrections, peer team members were integrated into the study after the decision had been made to adapt WORTH for use by Black women only. For this reason, peer adaptation members were not involved in the development of core elements or core activities.
Phase 3—Adaptation
Dramatic (or “theatre-tested”) demonstrations were held with focus group members to identify content to be adapted, added, or removed. Demonstrations included playing videos of all four fictional narrative characters used during the 2009 multimedia version of the WORTH intervention and reviewing the scripts for each video to determine if the race and ethnicity of fictionalized characters should be changed. Participants provided critical feedback regarding the cultural appropriateness, level of believability, and the degree of relatedness of the four fictional narrative characters. (Two of the four characters developed were Black, one was Hispanic/Latina, and one was White.) In light of feedback received from focus group members, one narrative character was subsequently replaced in its entirety, and another was newly created. Scripts were developed and refined with feedback from participants and refined iteratively during the ADAPT-ITT-guided Production (phase 4), Integration (phase 6), and Testing (phase 8) phases we followed.
Focus group participants were unanimous in recommending that narrative characters from all racial and ethnic groups were used in the adapted intervention, emphasizing the need to convey that HIV/STIs affected women from all racial/ethnic groups. Participants also spoke about positive strategies they utilized when confronting these challenges. Countering strategies included ones that were collectively employed (e.g., from “taking care” of each other and building and strengthening informal social support networks with other women similarly affected by these systems) to ones that were individual (e.g., writing their story in poems and short stories). Participants discussed their desire to leverage support from trusted professionals working within the systems from which they received professional services.
As shown in Table 1, focus group members provided feedback on the planned “hybrid” group design envisioned for the adapted intervention which features traditional group beginnings and endings for each group session (sessions 2–5), and tablet-based session activities delivered via a web-based multimedia platform. Participants also critically reviewed an enhanced social support map which graphically displayed the extent to which participants felt close to individuals they add to their map. Feedback was solicited regarding a newly proposed language intended to characterize different types of support participants report receiving from those in their social support networks (e.g., “practical support”, “emotional support”, and “financial support”). Peer adaptation partners were integrally involved in this phase and provided rich feedback on the design and look and feel of the intervention.
Phase 4—Production
Planning meetings explored questions related to “Blackness” in America as informed by race, ethnicity, and country of origin. Discussions also focused both on rich histories of survival and resiliency alongside discussions centered on the impact of poverty, racism, and oppression on Black women specifically that increases their risks for HIV/STIs. The team developed a detailed production plan to guide the adaptation of the web-based multimedia components of the intervention, complete with clear timelines. The production plan integrated feedback gathered from peer and non-peer adaptation partners.
The team also auditioned and hired actresses and video-recorded the revised and newly created fictionalized narrative characters approved by both the focus group and adaptation team members. Newly created and edited videos were shown in pilot meetings, held later in the adaptation process. Edited characters featured a stronger focus on injurious intimate partner violence and the risk of getting STIs from an intimate partner. The newly created character was a Black woman in her 30s who was recently released from incarceration and had multiple sexual partners, had a same-sex relationship, experienced violence from an intimate partner, and had low family support. (The same-sex component was incorporated due to high levels of bisexuality reported by 2009 Multimedia WORTH participants, revealed in 2009 WORTH data reviewed by Columbia's investigative team.) Although peers determined which actors and characters would be used and the content of newly written scripts, they were not present for actor auditions nor were they involved in preparing initial scripts.
Phase 5—Topical Experts
Topical expertise was solicited from CU's research team, NGO leadership, NGO reentry staff trained to serve as facilitators, the New York City Department of Probation leadership team, and E-WORTH CAB members. Focus group and pilot participants (during the Testing Phase) also provided expert guidance regarding intervention content development (e.g., narrative character creation/refinement), effective engagement of Black women in community corrections, and service usage patterns of women in the criminal legal system.
The selection criteria for NGO facilitators are enumerated in the protocol paper for this study (Johnson et al., 2018). Although not expressly required, several facilitators selected to deliver the intervention were themselves previously involved in the criminal legal system, a practice consistent with the philosophy of the NGO. In addition, CU recruited an NGO staff peer member to work full-time on the adaptation and the study. Columbia co-investigators, along with the E-WORTH's project director, led all training and orientation sessions.
Peers were represented in five of six levels of adaptation team members: focus group participants, CAB, study personnel, study facilitators, and NGO leadership. Their views as a result guided the bulk of key decisions made related to content selection, identification, and adaptation. As noted, not all planning or work group meetings included peers, such as those related to production timelines and adaptation schedules and activities.
Phase 6—Integration
Suggested changes from focus group participants and other topical experts were brought to the larger adaptation planning meetings for discussion and as necessary, were again addressed with focus group members. As shown in Table 1, changes made fell into two overarching categories: (i) cultural core content and language and (ii) technological enhancements.
Among cultural core content and language changes made, an element entitled “critical consciousness” was introduced to increase awareness of the relationship between substance abuse, HIV, and the larger context of power and oppression, consistent with the empowerment framework that guided E-WORTH (Freire, 1973). To address this element, language and videos created by HIV activist groups featuring HIV-positive and at-risk Black women were introduced to the 2009 multimedia platform. These added elements were introduced to frame the intervention within a larger context of structural stigma, racism, criminal legal system involvement and race, the interconnection between each and the resultant barriers for drug-using, court-involved Black women in navigating systems, and accessing services. Statistics relevant to Black women and new content reflecting the latest in HIV/STI prevention science (i.e., PrEP and PEP) and approaches (i.e., intimate partner violence screening, brief intervention, safety planning, and referral) were also integrated within all remaining core elements.
Technological enhancements include the creation of an electronic facilitator (or e-facilitator). For this role, we intentionally recruited an actress who was an older Black woman to convey an “auntie-like” feel since the average age range of participants in the Multimedia WORTH trial was between the mid-20s to mid-30s. In addition to providing key instructions to intervention participants on completing tablet-based activities, the e-facilitator (i) extends the reach of the traditional “in room” facilitators by relaying more detailed information on HIV, and screening and addressing IPV and (ii) increase participant level of comfort in disclosing highly sensitive issues around HIV risks and highly risky sexual behavior. The e-facilitator also guides participants through establishing “S.M.A.R.T.” (Specific, Measurable, Attainable, Realistic and Timely) goals at the close of sessions 1–4 (Doran, 1981). Goal activities focused on one of three categories: (i) reducing risks for HIV (sessions 2–4); (ii) increasing social support (sessions 3 and 4); and (iii) general goal setting (sessions 1–4).
As noted, a novel “hybrid” group design was also introduced featuring 45-minute-long tablet-based activities sandwiched between traditional group beginnings and endings. Guided by E-WORTH's e-facilitator, participants reflect on personal HIV/STI risks resulting from high-risk drug-, sexual-, and violent encounters (e.g., transactional sex, sex while under the influence, and intimate partner violence) during electronically delivered sequences. Group beginnings and endings are facilitated by the in-person, NGO facilitator who remains in the room during the tablet-based component to provide emotional and technical support as needed. Where solicited, the views and recommendations of peer partners were fully integrated into the intervention's design.
Phase 7—Training
Training sessions focused on the core elements and content of the newly adapted intervention, engagement skills, the study's unique hybrid design, group and tablet management strategies, case management, and retention techniques. Strategies to ensure seamless integration of intervention activities and NGO community reentry processes and procedures (e.g., HIV/STI treatment, case management, and referrals) were also discussed to optimize the fit of the intervention within the agency setting. Recommendations from CAB members regarding effective outreach, recruitment, and retention strategies for Black women in community corrections were also integrated into the training program. Peer partners were not present for the training session, nor did they review the planned training content before each being held.
Phase 8—Testing
A 3-day pilot, held several months before the study's launch, was conducted with 10 Black female participants. The pilot was facilitated by three CU research study staff who identified as Black women. Participants included all available focus group participants (four women in total), three additional Black women with similar risk profiles recruited from current and past CU research studies, and several peer and non-peer NGO E-WORTH facilitators. Participants were universally positive and found the Afrocentric messaging inspirational, the characters relatable, and testimonials of empowerment and resiliency effective. Additional topics discussed are enumerated in Table 1.
The 5-week session was held over the course of 3 days with two sessions demonstrated in full on day 1, two sessions on day 2 and the fifth session piloted on the third day. Peer adaptation partners expressed some fatigue at the close of day 2. In addition, peer partners did not assist in demonstrating the intervention.
Results
A total of 352 participants who identified as Black/African American were enrolled, including 79 (22.5%) who also identified as Latinx. The mean age was 32.4 (SD = 11.0). Compared to control participants, E-WORTH participants had 54% lower odds of testing positive for an STI at the 12-month follow-up and reported 38% fewer acts of condomless sex over the study's 12-month follow-up period (Gilbert et al., 2021). The study findings also suggest high rates of participation (78% of participants who screened eligible for the study enrolled) and retention over the 12-month follow-up (86% completed the 12-month follow-up) as an indicator of participant satisfaction.
Discussion
A critical need remains for culturally congruent HIV/STI prevention interventions that are designed by Black women with lived experience (Pinto et al., 2018). To achieve health equity goals, there is also a need to engage Black women more fully in the criminal legal system who misuse substances as health equity partners in shaping interventions. Contributions summarized in this article highlight key adaptation and health equity implications. First, E-WORTH meets a significant need. Adapted for and by Black/African-American women with combined histories of substance misuse and criminal legal system involvement, E-WORTH's richly resonant messaging and targeted HIV/STI prevention messaging speaks directly to the lived experiences of Black/African-American women currently challenged by both. Women traditionally labeled as “hard to reach”, worked collaboratively to approve critical content such as story, character and actor selection, and African diasporic look, feel, and imagery.
Second, while drug-using Black women in community corrections and Black female community reentry personnel were integral to E-WORTH's adaptation, power differentials and siloed communication and processes were also noted. Associated with different levels of authority possessed by those with and without higher levels of educational attainment and academic status, these peer and non-peer team differences draw attention to pitfalls to be avoided when adapting prevention interventions. While the ADAPT-ITT adaptation framework is useful for adapting HIV-related evidence-based prevention interventions, it does not examine the impact of power dynamics on adaptation processes, and how to negotiate those dynamics. It also does not make clear strategies for countering those challenges. HIV intervention design and adaptation models are needed that are explicitly health equity-focused and provides guidance on how to more fully partner with peers. Failure to do so may result in unintentionally siloed processes, reinforcement of power asymmetries, missed opportunities in learning from peers, and realizing the U.S. health equity goals. In the absence of a clear national strategy that makes clear microlevel health equity goals, how these efforts relate to Health Equity gap mitigation must also be fully explored.
Third, although not an adaptation model, the Health Equity Implementation Framework (Woodward et al., 2019) draws attention to factors that may adversely impact the uptake of EBIs by BIWOC and other traditionally marginalized and disenfranchised groups. These include how the construct of power is exercised by those in power in clinical and other encounters, serving to undermine efforts to reduce health inequities and marginalization. Ensuring that power decision-making processes privilege the voice of those who are in the best position to represent the target population during adaptation processes and beyond is a critical component in ensuring responsive evidence-based prevention interventions that redress ongoing HIV/STI racial disparities (Barac et al., 2018).
Limitations
Although the adaptation process resulted in producing an intervention that was effective in reducing both STIs and condomless sex as primary outcomes among this sample of Black women in community corrections, there were several steps where peers had limited or no involvement in the process as highlighted in the methods. Most significant is the lack of peer involvement and decision-making power in the design of the grant which is in response to a time-limited NIDA request for application (RFA). Such RFAs don’t allow the time to build community partnerships and engage peers in the design. Full engagement of peers in adapting interventions requires a paradigm shift from inviting peers to researcher-driven table and agenda to creating a table and agenda where peers have the same decision-making power as researchers.
Despite this limitation, the outcomes suggest that the adaptation of E-WORTH resulted in significantly fewer STIs and fewer condomless sex acts. The significant effects on primary outcomes found for E-WORTH are stronger than the average effect from a meta-analysis of 17 HIV/STI interventions conducted among Black women that observed a 19% reduced odd of STI incidence among intervention participants relative to comparison participants (Crepaz et al., 2007).
Conclusions
Despite marked decreases in the rate of new transmissions among “hard to reach” populations in recent years, risks among drug-using, Black women in community corrections remain persistently and disproportionately high. Bio-prevention strategies alone remain largely un or under-endorsed by this group, further underscoring the need for culturally congruent, evidence-based, HIV/STI prevention interventions like E-WORTH. Given the high rates at which EBIs fail in real-world settings (after an initial period of successful implementation), greater engagement with impacted populations during adaptation processes may be required to support the health equity goal realization (McCree et al., 2016).
Footnotes
Acknowledgments
The authors would like to thank E-WORTH study participants, NGO reentry corrections agency personnel, New York State Department of Probation personnel, Community Advisory Board members, Columbia CTL personnel, and other adaptation personnel. A special thanks to Blondell Jackson, Chermaine Black, and Vanesa Ranjandaran for their role in assisting with the adaptation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Drug Abuse (grant number R01DA025878).
Research Involving Human Participants and/or Animals
This article does not contain any original study results with human participants or animals performed by any of the authors.
Informed Consent
Informed consent is not applicable for this adaptation manuscript.