
Abstract
Keywords
The number of cancer survivors continues to grow because of advances in screening, diagnosis, and treatment. According to the International Agency for Research on Cancer (2022), there were 19.3 million new cancer cases worldwide in 2020. The overall 5-year survival rate for all cancers continues to increase, suggesting that some cancers can be considered chronic diseases (Aapro et al., 2020). The increasing number of cancer survivors challenges health care providers and systems to provide comprehensive and consistent quality cancer care because cancer survivors face physical, psychological, social, and behavioral issues after treatment conclusion (Chan et al., 2021a; Lewson et al., 2021). The current study focused on adult cancer survivors aged 18 years or older specifically, given that the type of cancer and therapeutic modality can be unique to the age at diagnosis and treatment (Robinson et al., 2022).
Critical gaps remain in survivorship care in terms of providing accessible, sustainable, equitable, and patient-centered services, although researchers have developed and evaluated survivorship care models (e.g., disease-specific, comprehensive, and shared care models) (Chan et al., 2021b; Ganz, 2014; Nekhlyudov et al., 2019) and products (e.g., survivorship care plans) to meet the needs of cancer survivors who have completed treatment (Gast et al., 2017). First, unmet needs related to the psychological domain (e.g., fear of recurrence, stress) remain, with an average of four to five unmet survivorship needs (Kotronoulas et al., 2017; Vuksanovic et al., 2021). Second, there are barriers to the implementation of survivorship care plans (SCPs) for cancer survivors, including adherence, resources, communication, and care coordination (Chan et al., 2021b; Fong et al., 2021). For example, poor adherence to available survivorship care guidelines for surveillance, intervention, and continuity of care, limited knowledge of cancer survivor issues, and lack of an informative SCP tool have been identified as major barriers to implementing various SCP models (Høeg et al., 2019; Tomasone et al., 2016). Third, the COVID-19 pandemic has interrupted cancer care delivery in general and survivorship care services specifically, such that posttreatment cancer survivors may experience increased risks for long-term or late physical effects as well as anxiety and fears of recurrence (Arem et al., 2021; Ashbury, 2021).
Finally, since 1990, the incidence of early-onset cancers specifically has dramatically increased worldwide, indicating that people are likely to experience a higher cancer risk before age 50 (Ugai et al., 2022). Considering changes in demographic patterns of cancer incidence and survival, it may be necessary to develop a comprehensive system for personalized survivorship care plans. For example, middle-aged adults may have easy access to technology to receive survivorship care. As a result, innovative approaches such as technologies need to be considered to provide more efficient and effective survivorship cancer care.
Given the abovementioned challenges, innovative technology-based solutions to enhance survivorship of cancer care and reduce patient risks have received increased attention. Specifically, since COVID-19, models of cancer care have been adapted and implemented with the amplified use of technologies (Koczwara, 2020). Interventions using technology solutions reduce cancer-related fatigue and distress, improve physical activity, and address supportive cancer care needs (Seiler et al., 2017; Ventura et al., 2013). Technology-based strategies in health care are often interchangeably defined as “digital health,” “eHealth,” “mHealth,” “telehealth,” and “telemedicine.” Generally, such terms refer to the use of digital technology, which is an umbrella term that covers many types of technologies used in health care, such as health applications, wearable devices, and electronic health records (Aungst & Murdock, 2023). The development of digital technology has brought changes and innovations to health care in new ways in the context of the content and delivery of health services, allowing patients to stay in contact with health care providers regardless of time or location (Ricciardi et al., 2019). Furthermore, digitalization in health care allows people to have much more responsibility in managing their health, moving to “consumer-centric” health care (World Economic Forum, 2016). Thus, digital technology can offer new opportunities for enhancing the empowerment of cancer survivors and improving the content and delivery of services in health care (Aapro et al., 2020). In this study, we broadly defined “technology-based interventions” as any type of intervention that involves the use of digital technologies in a broad scope of health care, including web-based applications, videoconference, monitoring systems, wearable devices, and social media.
A growing number of technology-based interventions in survivorship care for adult cancer patients have recently been published, including two systematic reviews (Aapro et al., 2020; Marthick et al., 2021) and two meta-analyses (Larson et al., 2018; Wang et al., 2020). For example, Aapro et al. (2020) reviewed 66 studies to clarify the role and impact of digital health solutions in oncology-supportive care, focusing on technical features. Marthick et al. (2021) evaluated 20 digital health randomized controlled trials (RCTs) on supportive cancer care and quality of life. These reviews suggested the efficacy of digital health solutions, indicating that digital health interventions are effective at supporting patients with cancer. In contrast, Larson et al. (2018)'s meta-analysis of nine technology-based RCTs that provided emotional and symptom support in improving the quality of life for cancer patients found no statistically significant differences in effectiveness between telehealth intervention (e.g., telephone, videoconference, and internet-based interventions) and control groups. Wang et al. (2020) performed a meta-analysis of seven RCTs among cancer patients and found that internet-based psychoeducational interventions reduce fatigue and depression.
These studies, while valuable and informative, called for investigators to do the following: First, conduct a systematic review and meta-analysis to evaluate the efficacy of technology-based interventions for only cancer survivors who complete treatment. The effects of technology-based survivorship care interventions differ between patients during and following cancer treatment (Aapro et al., 2020; Larson et al., 2018); however, few studies have focused on posttreatment cancer survivors or demonstrated outcome differences by the stage of cancer treatment. Second, studies have evaluated the efficacy of technology-based interventions according to domains of cancer survivorship care. None of these reviews focused on survivorship care domains categorized by SCP guidelines for cancer survivors, primarily addressing outcome measures. Nekhlyudov et al. (2019) developed a framework for cancer survivorship care quality regarding cancer-related and general care needs with five domains. Gast et al. (2017) also categorized survivorship care into four domains, reviewing innovative technology solutions to enhance survivorship care. The current systematic review and meta-analysis intends to advance the knowledge base related to digital interventions for cancer survivors in that it applies an a priori quality of cancer survivorship care frameworks, which combines Nekhlyudov's with Gast's framework, considering the application of technology in survivorship care: (a) psychosocial effects, (b) health promotion and disease prevention, (c) physical effects, and (d) self-management. Third, it is important to evaluate key moderators such as the types of interventions, survivorship care domains, or participant characteristics (e.g., age and sex). Previous meta-analyses focused on investigating the effects of interventions rather than moderating effects. An analysis of moderating effects will deepen the understanding of whether certain interventions are better tailored to respond to the unique needs of cancer survivors. Fourth and finally, meta-analyses with a strong methodology are needed. Previous meta-analyses were limited by study design issues, including a lack of comparison groups, RCT designs, or inadequate power to detect statistically significant differences. In this systematic review and meta-analysis, we analyzed RCTs that examined the effects of “technology-based cancer survivorship care interventions” on at least one of four survivorship care domains as described by Nekhlyudov et al. (2019) and Gast et al. (2017).
We conducted a systematic review and meta-analysis of RCTs evaluating technology-based survivorship care interventions for posttreatment adult cancer survivors, considering the unique challenges they face. Given the environmental changes and innovations in health care, this study also focused on patient-engaged “digital technology” in survivorship care interventions. The current study is important to create recommendations on how technology-based interventions can be used to increase the sustainability of cancer care and improve survivorship outcomes. The primary objective was to determine whether technology-based survivorship care interventions are effective in terms of patient-reported outcomes according to the types of interventions (i.e., survivorship care domain, intervention modality, the technology used, comparison group, and targeted outcomes) or participant characteristics (i.e., age, sex, and cancer type). Additionally, we examined whether the types of interventions or participant characteristics moderated the treatment effect size of technology-based survivorship care interventions.
Method
An investigative team conducted a systematic review and meta-analysis in technology-based cancer survivorship care using RCTs and the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines (Shamseer et al., 2015) were applied to conduct procedures.
Search Procedure and Study Eligibility
The study team systematically searched RCTs that evaluated the effects of technology-based survivorship care interventions for cancer survivors. For this review, 10 electronic databases and five professional websites were used. Additionally, published review articles regarding technology-based RCTs for patients with cancer were manually searched to identify relevant articles (Aapro et al., 2020; Agboola et al., 2015; Blount et al., 2021; Kiss et al., 2019; Larson et al., 2018; Marthick et al., 2021; Nekhlyudov et al., 2019; Post & Flanagan, 2016; Schaffer et al., 2019; Wan et al., 2022; Wang et al., 2020). Thus, an initial pool of studies was generated for screening. To identify studies focusing on cancer survivors, we used the following key terms: “cancer” or “cancer patient” or “cancer survivor” or “oncology” or “adult cancer” or “adult oncology.” For survivorship care intervention, key terms such as “survivor* care” “follow-up *” “support* care” “health manage*” “health behave*” “health promotion” “physical activity” “patient education” “self-management” “psycho*” “social” “symptom management” were used. All studies were searched between September 5, 2022, and September 23, 2022. The search protocol was preregistered at PROSPERO (Number: CRD42022384208).
The inclusion criteria were as follows: (1) studies were written in English describing an RCT published between January 2000 and August 2022, a period during which most technology-based intervention trials were published; (2) intervention recipients were adults who were older than 18 years old, diagnosed with any type of cancer after the age of 18, and completed active cancer treatment (e.g., surgery, chemotherapy, or radiation therapy); (3) patient-engaged digital technology was utilized as the content or delivery of an intervention (e.g., app and wearable devices) regardless of the involvement of people in interventions; thus, mixed interventions addressing both in-person and technologies were included; and (4) interventions were implemented to provide cancer survivorship care, which covers at least one of four domains of the survivorship care framework, using one or more psychosocial outcomes (e.g., fatigue, depression, distress, and social support). Studies were excluded if they included medical or pharmaceutical treatment or outcomes only, they were not randomized, there was no comparison group in the study, there were no outcome data on the effects of interventions, or recipients were childhood cancer survivors diagnosed under the age of 18 years. Technology-based interventions used text messages or phone calls only without any digital devices were excluded because we are interested in self-directed technologies in which the survivor initiates engagement with the technology as opposed to modalities that are initiated on the clinical side. Additionally, review articles, books and book chapters, qualitative studies, and original studies without full texts were excluded.
Data Extraction
Before reviewing articles, the study team developed a data extraction sheet to systematically code and extract information for all included studies. First, the first author screened all studies by reading study titles and abstracts to find potential eligible articles. Ineligible articles (e.g., non-RCT, childhood cancer, or nontechnology) were removed from the records. Two research assistants then read the full text of the eligible articles using Covidence, that is, a Cochrane-recommended screening platform. Any discrepancies regarding a study's inclusion and exclusion were resolved by discussion with study team members.
Assessment of the Methodological Quality of the Included Studies and Publication Biases
Each study's methodological quality was assessed by the revised Cochrane Collaboration's tool for assessing the risk of bias in RCTs (Risk of Bias 2.0) (Sterne et al., 2019), a commonly used tool to report the risk of bias in each article included in systematic reviews and/or meta-analyses. This tool assesses five major domains, including the randomization process, deviation from intentional interventions, missing outcomes, measurement of outcomes, and selection of reported results. Each domain is rated as “some concerns,” “low,” or “high.” Using this tool, we entered all data into Review Manager 7.0, and a risk of bias graph was generated for all studies.
Publication bias was evaluated first using a funnel plot by plotting individual effect size estimates against their corresponding standard errors, and a visual inspection of the plot's symmetry was used to detect publication bias. Second, we used Vevea and Woods (2005)'s sensitivity analysis with a priori weight functions to empirically evaluate publication bias. The analysis constructs an observed effect size and a theoretical effect size (assuming the funnel plot is perfectly symmetric). A significant difference between the two effect sizes is interpreted as a sign of publication bias.
Meta-Analytic Procedures
Meta-analyses were conducted using meta-regression with a robust variance estimation (RVE) (Hedges et al., 2010). This approach was chosen because meta-regression offers a flexible analytical framework for estimating an overall treatment effect size, subgroup, and moderator analysis. An intercept-only meta-regression analysis calculates an overall treatment effect size estimate, whereas meta-regression models with predictors facilitate moderator analyses (Tipton, 2015). Specifically, in this study, we used intercept-only meta-regression to calculate an overall treatment effect size as well as subgroup analysis, that is, an overall treatment effect size for a subgroup of data/effect size. We then explored important factors, for example, age, gender, and intervention modality, as moderators for technology-based intervention treatment effects for cancer survivors.
Representative elementary volume (RVE) is an important method in this study because multiple effect size estimates from the same study were included in analytical models. Effect sizes from the same study create the issue of within-study dependence, violating the independence of error assumption of regression models (van Houwelingen et al., 2002). RVE effectively accounts for the within-study dependence among those effect sizes from the same study (Hedges et al., 2010; Pustejovsky & Tipton, 2022). In addition, RVE produces valid standard errors regardless of the variance modeling selection, that is, a fixed- versus a random-effects model. Therefore, selecting between a fixed- versus random-effects meta-analysis model becomes not applicable in meta-regression with RVE (López-López et al., 2017).
Based on such procedures, we first calculated an overall treatment effect size across outcome domains. Then, overall treatment effect sizes were estimated using subgroup and intercept-only meta-regression analyses. Finally, moderator analyses were conducted using univariate meta-regression by entering potential moderators once at a time into meta-regression models. According to existing methodological recommendations (Pustejovsky & Tipton, 2022; Tipton, 2015), a p-value of .05 was used as the threshold for statistical significance for point estimates with a degree of freedom of 4 or greater, and a p-value of .01 was used as the threshold for statistical significance for point estimates with a degree of freedom lower than 4.
Results
Study Selection
An initial literature search identified 15,349 records from the electronic database and an additional 35 records from the reference list. After excluding 238 duplicates, protocols, and reviews, 15,146 studies were screened with titles and abstracts, of which 92 studies were retrieved for full-text eligibility reviews. Of these citations, 50 met the eligibility criteria and were included in this systematic review and meta-analysis. The reasons for exclusion are described in Figure 1.
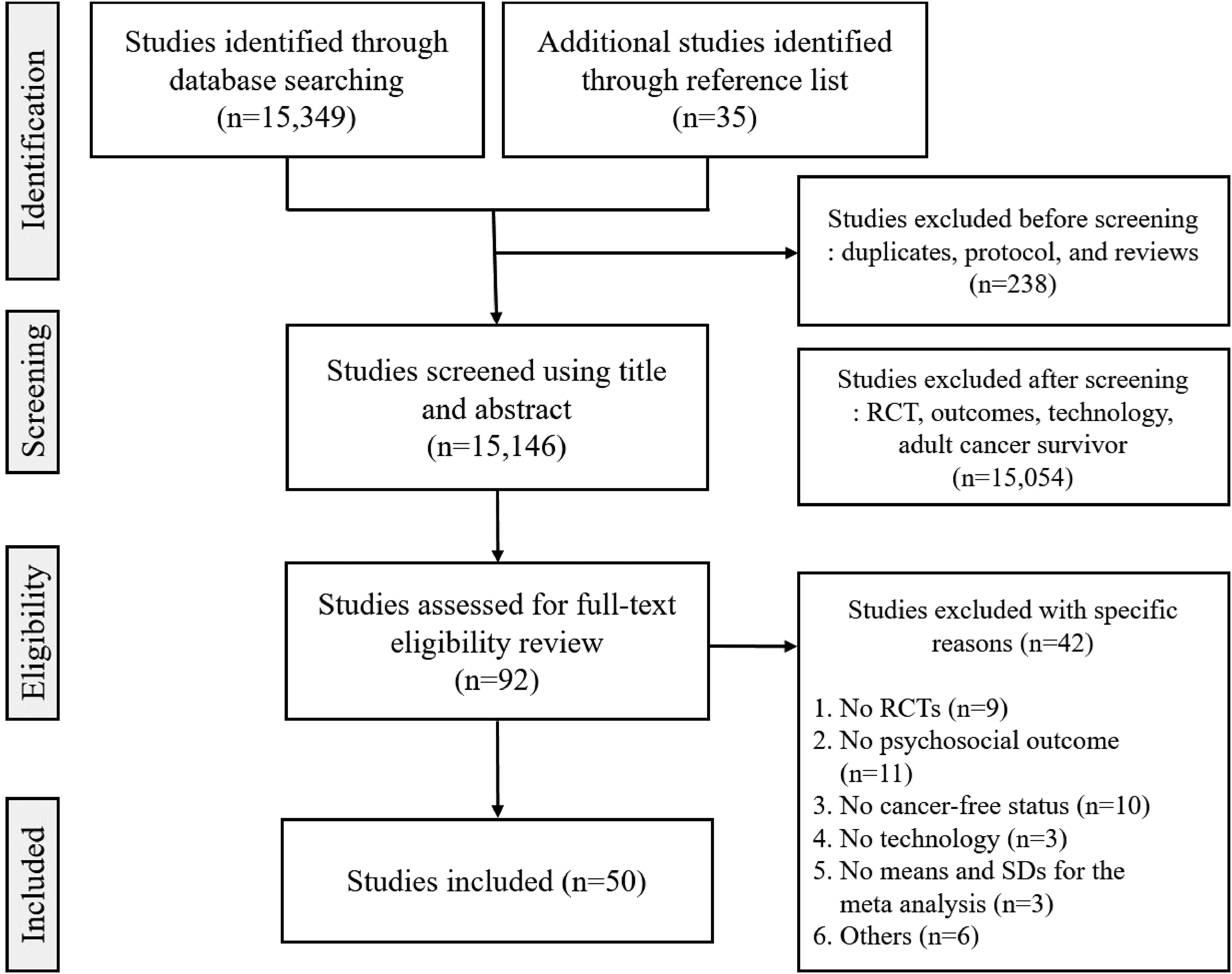
Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flowchart of a process of identification of studies.
Study Characteristics
Tables 1 and 2 describe the characteristics of the 50 included studies. Fifty RCT studies that assessed the effects of survivorship care using technologies for cancer survivors were published between 2012 and 2022. Thirty-nine studies were published after 2016, and in 2021 specifically, 12 studies were published. Almost half of the studies (48%) were conducted in the United States, 28% were in Europe, such as Denmark or the Netherlands, and 10% were in Asia, such as China or Korea. Studies conducted in two or more countries accounted for 8%. Across the studies, the average age was 52.6 years old, and 78.7% of all participants were female. Studies reported that an average of 74.4% of the participants were White. Ten studies exclusively targeted non-White populations, including Chinese, Korean, or Spanish populations. Most studies focused on one of the most common ethnicities (e.g., White in the United States and Chinese in China) rather than considering diverse ethnic groups, indicating that an average of 90% of all studies were comprised of one homogeneous ethnic group. Studies targeting more than one cancer were the most common (44%). In studies that targeted more than one, people with prostate cancer, colorectal cancer, head and neck cancer, Hodgkin lymphoma, or non-Hodgkin lymphoma cancer were included. Of studies including only one cancer type, studies targeting breast cancer were the most popular (38%), and other cancer types were colorectal, prostate, endometrial, esophageal, melanoma, or nasopharyngeal cancer.
Descriptive Summary of Included Studies (N = 50).
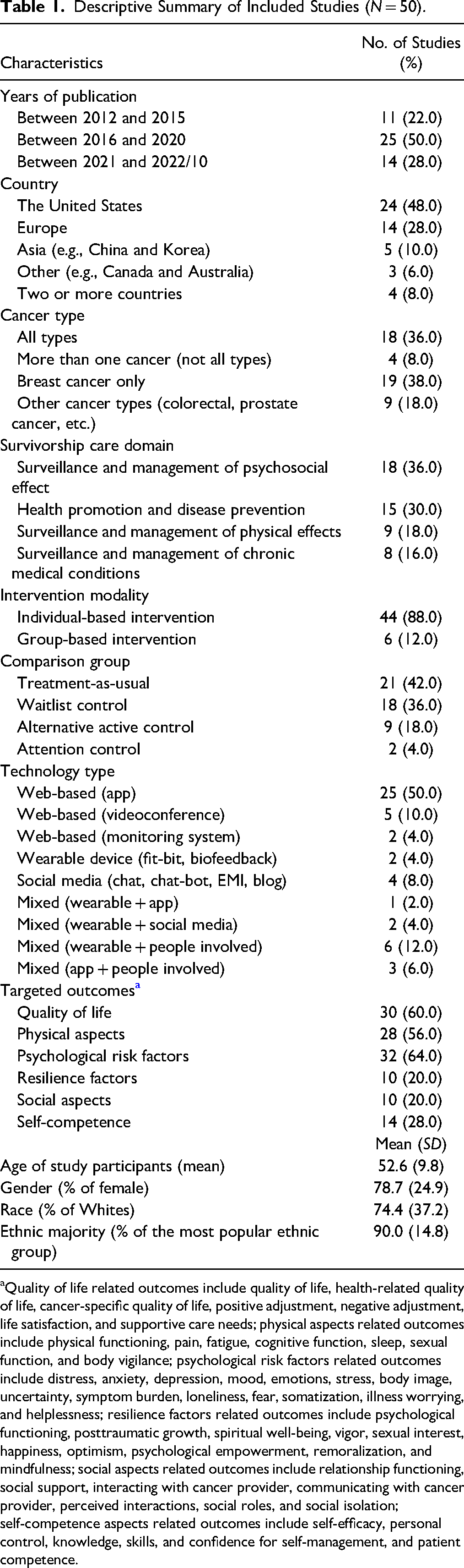
Quality of life related outcomes include quality of life, health-related quality of life, cancer-specific quality of life, positive adjustment, negative adjustment, life satisfaction, and supportive care needs; physical aspects related outcomes include physical functioning, pain, fatigue, cognitive function, sleep, sexual function, and body vigilance; psychological risk factors related outcomes include distress, anxiety, depression, mood, emotions, stress, body image, uncertainty, symptom burden, loneliness, fear, somatization, illness worrying, and helplessness; resilience factors related outcomes include psychological functioning, posttraumatic growth, spiritual well-being, vigor, sexual interest, happiness, optimism, psychological empowerment, remoralization, and mindfulness; social aspects related outcomes include relationship functioning, social support, interacting with cancer provider, communicating with cancer provider, perceived interactions, social roles, and social isolation; self-competence aspects related outcomes include self-efficacy, personal control, knowledge, skills, and confidence for self-management, and patient competence.
Design and Intervention Characteristics of Studies Included in Meta-Analysis (N = 50).

Note. QOL = quality of life; HRQOL = health-related quality of life; PTG = posttraumatic growth; FOR = fear of recurrence; Control. ALT = alternative active control; TAU = treatment-as-usual; ATT = attention control; WTL = waitlist control; RCT = randomized controlled trial.
The number of sample size is based on the baseline of RCT.
In terms of survivorship care domains, 36% of the studies focused on psychosocial effects, 30% on health promotion and disease prevention, 18% on physical effects, and 16% on self-management. Forty-four studies (88%) delivered individual-based interventions, and six studies (12%) administered group-based interventions. Regarding the technologies used in RCTs, 38 studies used one of the technologies, including web-based, wearable devices, or social media, and 12 studies used mixed approaches that combined two or more technologies or other methods. In detail, in web-based technologies, 50% of the studies used apps, 10% videoconferences, and 4% monitoring systems. Two studies used Fitbit or biofeedback as wearable devices, and four studies used social media, that is, chatbot, EMI, or blog. In cases of studies using mixed approaches based on technology, one study used a combination of wearable devices and apps, and two studies used a combination of wearable devices and social media. Meanwhile, nine studies provided technology-based interventions accompanied by people (e.g., research assistants, counselors, physiotherapists, or facilitators). As targeted outcomes, 45 suboutcomes were driven in the reviewed articles, which were reorganized based on six categories. That is, 32 studies reported outcomes regarding psychological risk factors (e.g., depression and anxiety), and 30 studies reported quality of life-related outcomes (e.g., well-being and adjustment). Twenty-eight studies reported outcomes regarding physical aspects (e.g., fatigue and pain), 14 studies for self-competences (e.g., self-efficacy and personal control), 10 studies for resilience factors (e.g., happiness and mindfulness), and 10 studies for social aspects (e.g., social role and social support).
Regarding the use of technology according to survivorship care domains, RCTs focusing on health promotion and disease prevention were more likely to employ wearable devices with the involvement of people (33.3%). In self-management, 87.5% of the studies used web-based apps. Trials addressing psychosocial effects were more likely to use web-based apps (50.0%), videoconferences (22.2%), and social media (16.7%). In terms of the physical effects, most technologies were used evenly.
The Methodological Quality of the Studies
Risk of bias assessment identified an overall low risk of bias for RCTs included in the study, indicating that 76% of the studies demonstrated a low risk of bias. Most biases were in the randomization process. Ten of the included 50 studies presented some concerns (n = 9) or high risk (n = 1). Additionally, some concerns due to both measurements of the outcome and deviations from the intended interventions were identified in three and two studies, respectively. No other concern about the risk of bias was present (Figure 2).

Risk of bias summary for randomized controlled intervention studies (N = 50).
Meta-Analysis: Effectiveness of Technology-Based Cancer Survivorship Care Intervention
The overall treatment effect size across the outcomes included 422 effect sizes from 50 studies averaged at g = 0.251, 95% CI 0.160–0.341, p < .001, indicating a statistically significant although small treatment effect size estimate. On average, cancer survivors receiving technology-based survivorship care interventions were expected to report 0.251 standard deviations more improvement than their counterparts being assigned to the control condition (Table 3).
Overall and Subgroup Treatment Effects.
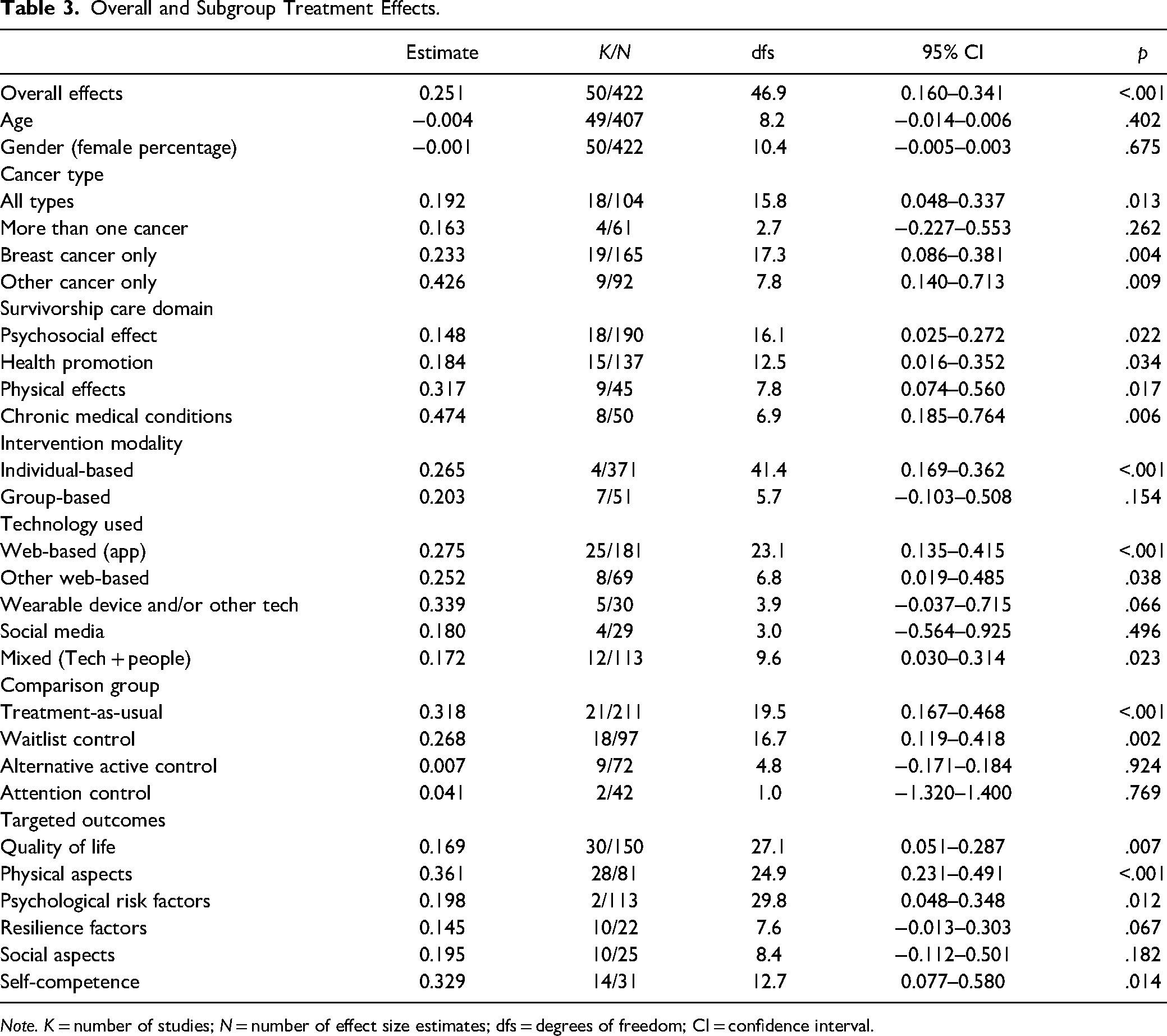
Note. K = number of studies; N = number of effect size estimates; dfs = degrees of freedom; CI = confidence interval.
Subgroup/Domain-Specific Analysis
Subgroup analysis revealed that studies including all types of cancer or focusing on breast cancer only reported statistically significant although small effect sizes, g = 0.192 and 0.233, respectively. Nine studies focused on other specific cancer types showed a significant and moderate treatment effect size, g = 0.426. However, technology-based survivorship care interventions targeting more than one cancer type were not statistically significant.
Studies reported overall statistically significant treatment effects regardless of survivorship care domains. Studies focusing on both psychosocial effects (g = 0.148, p = .022) and health promotion and disease prevention (g = 0.184, p = .034) showed small effect sizes, while those focusing on physical effects (g = 0.317, p = .017) and self-management (g = 0.474, p = .006) reported moderate effect sizes. This indicates that participants who received interventions addressing physical effects and self-management, on average, reported 0.317 and 0.474 standard deviations greater improvement than their counterparts in the control condition, respectively.
In terms of intervention modality, 44 studies including 371 effect sizes using individual-based interventions reported an overall statistically significant although small treatment effect size, g = 0.265, p < .001. However, seven studies including 51 effect sizes using group-based interventions reported an overall statistically nonsignificant although small treatment effect size.
Studies that used web-based technologies, including apps (g = 0.275, p < .001) or other tools (e.g., videoconferences or monitoring systems) (g = 0.252, p = .038), reported overall statistically significant treatment effects. In contrast, the overall treatment effect sizes for studies that used wearable devices (five studies and 30 effect sizes) or social media (four studies and 29 effect sizes) were not statistically significant. Meanwhile, 12 studies that included 113 effect sizes of interventions that used technologies with the involvement of people reported an overall statistically significant, although small, treatment effect size, g = 0.172, p = .023.
Twenty-one studies (211 effect sizes) comparing technology-based interventions with the treatment-as-usual control group reported an overall statistically significant and moderate treatment effect, g = 0.318, p < .001. Eighteen studies including 97 effect sizes comparing technology-based interventions with waitlist control groups also reported an overall statistically significant treatment effect. However, overall treatment effects were not statistically significant when comparing technology-based interventions with alternative active control groups or when compared with alternative control groups.
In terms of targeted outcomes, studies that assessed outcomes regarding the quality of life, physical aspects, psychological risk factors, and self-competence showed statistically significant treatment effects, whereas those that assessed outcomes about resilience factors and social aspects reported statistically nonsignificant treatment effect sizes. More specifically, studies of outcomes regarding physical aspects (g = 0.361, p < .001) and self-competence (g = 0.329, p = .014) reported moderate treatment effect sizes. Thirty studies of quality of life outcomes (g = 0.169, p = .007) and 32 studies of psychological risk factors (g = 0.198, p = .012) reported overall statistically significant, although small, treatment effect sizes.
Moderator Analyses
Moderator analyses identified survivorship care domains, comparison groups, and targeted outcomes as significant moderators (Table 4). First, in survivorship care domains, technology-based interventions focusing on self-management reported significantly greater treatment effect sizes than psychosocial effects-focused interventions, b = 0.327, p = .029. Second, studies of treatment-as-usual control conditions reported significantly greater effect sizes than studies with alternative active control conditions, b = −0.260, p = .026. Finally, the targeted outcome was also a significant moderator, that is, studies that included self-competence-related outcomes showed a significantly greater treatment effect than studies that included quality of life-related outcomes, b = 0.378, p = .018. Meanwhile, age, gender, cancer type, intervention modality, and technology used were not significant moderators.
Univariate Meta-Regression Moderator Analysis.
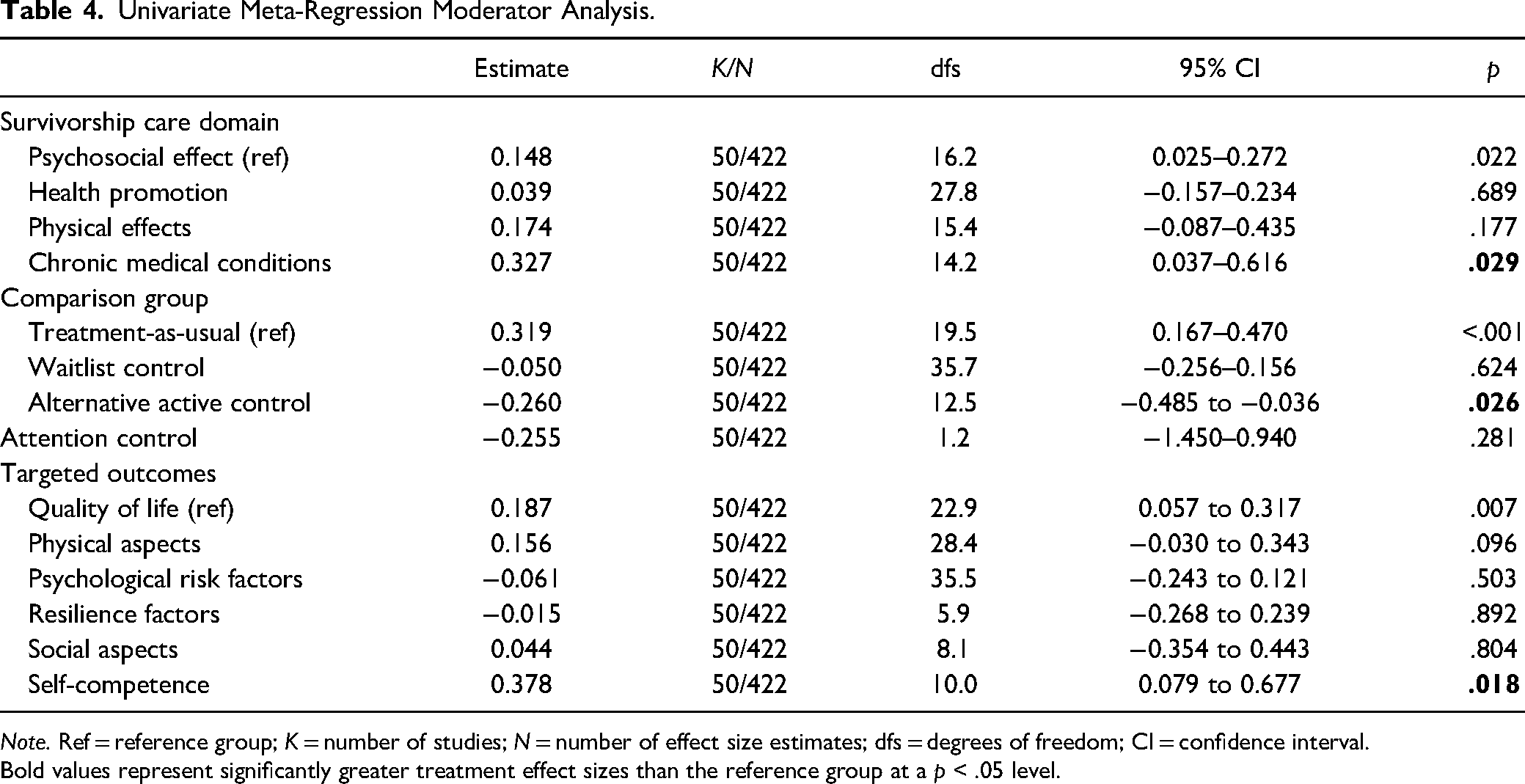
Note. Ref = reference group; K = number of studies; N = number of effect size estimates; dfs = degrees of freedom; CI = confidence interval.
Bold values represent significantly greater treatment effect sizes than the reference group at a p < .05 level.
Discussion and Applications in Practice
This systematic review and meta-analysis examined the effects of technology-based survivorship care interventions for cancer survivors who had completed treatment in 50 RCTs. To the best of our knowledge, the current study is the first to investigate the influences of technology-based digital solutions in cancer survivorship care, considering differences in treatment effects by the types of interventions and participant characteristics. The current study is meaningful in that findings from RCTs and meta-analyses reinforce the value and applicability of technology-based interventions in cancer survivorship care. Furthermore, the current study is important in that it sought a new path in the direction of future SCPs for providing patient-centered care services while considering changes in the environment.
As previous systematic reviews (Chan et al., 2021b; Marthick et al., 2021; Wang et al., 2020) have suggested, technology-based survivorship care interventions improve overall health outcomes for cancer survivors, although differences in treatment effects remain across survivorship care domains. Since the importance of posttreatment survivorship among cancer patients has been recognized since the early 1990s, diverse strategies for achieving optimal health have been proposed and formulated to improve psychosocial and behavioral health care. However, researchers and clinicians still seem to have difficulties comprehensively addressing diverse aspects of survivorship care, including surveillance for recurrence, health promotion, or the management of physical and psychosocial long-term effects. This is also seen in technology-based survivorship care. For example, Chan et al. (2021b) found a lack of evidence on the use of technology in the prevention and surveillance of recurrence and new cancers, specifically. The current study also did not find such a domain in technology-based survivorship care. Nevertheless, the current study showed that technology-based survivorship care interventions focusing on self-management can have positive effects in various aspects, ranging from prevention to health promotion and surveillance of recurrence for cancer survivorship care. Likewise, the current study identified an adequate number of technology-based cancer survivorship care interventions using RCTs with the power to detect statistically significant differences in the effect sizes of interventions regarding predetermined and theoretically derived domains of survivorship. Studies varied in the domains affected as well as in the number of domains affected, thereby suggesting a need for ongoing investigations to evaluate effects on preferred domains or in terms of an intervention's ability to improve multiple survivorship domains simultaneously.
Generally, technology-based interventions are unlikely to be implemented in person or guided by a health professional with an expectation that people can manage their condition and control their symptoms in a cost-efficient manner. Survivorship care interventions for improving self-management might be important for cancer survivors who are ready to return to normative levels of function at home or work specifically, given that such interventions provide an opportunity to increase their self-efficacy. Furthermore, web-based apps have the potential to achieve precision in that they enable survivors to manage their health at a point in time when needed and where convenient for them. As a result, this study suggests that self-management interventions using web-based apps might be useful to survivors who should manage their health by themselves at home as a method of delivering survivorship care. Our suggestion may be a solution to the challenges that Aapro et al. (2020) reported, indicating that a substantial number of digital solutions provide patient self-management programs, and digital solutions suitable for cancer patients to manage their health should be developed and implemented.
Moreover, the reviewed studies reported that psychosocial health interventions were not as effective as self-management interventions in diverse types of technology-based survivorship care interventions. This finding seems to be controversial based on previous meta-analysis findings. For example, Aapro et al. (2020) and Marthick et al. (2021) reported that supportive care digital interventions resulted in significant positive outcomes, while Larson et al. (2018) did not find significant differences in the effectiveness of telehealth interventions providing supportive care between intervention and control groups. Wang et al. (2020)'s study on the effects of internet-based psychoeducational interventions indicated that such interventions had a positive effect on reducing depression and fatigue, but there was no evidence of effects on distress. One possible explanation for the discrepancy is that approaches in technology-based survivorship care interventions might be different across the studies. In fact, previous meta-analyses tended to focus on supportive care interventions rather than psychosocial health interventions without distinguishing the types of survivorship care interventions. Although supportive care interventions might be similar to psychosocial health interventions, approaches and emphases in implementing interventions might be different and in turn influence treatment effects. In carrying out technology-based survivorship care interventions, it seems necessary to propose more effective intervention methods for cancer survivors through interventions focused on specific areas rather than a comprehensive approach.
The reviewed RCTs used diverse types of technology, including apps, videoconferences, monitoring systems, wearable devices, and social media. Such findings expand the findings from Chan et al. (2021b)'s review, which focused on the efficacy and roles of telemedicine in posttreatment cancer survivorship care. Notable findings of this study were that interventions involving people with technologies as well as web-based technologies reported significant treatment effects. This suggests that the involvement of people with technologies in survivorship care interventions may be necessary, expecting that they play important roles in monitoring the progress of survivors, evaluating their emotional responses, and interacting with them. This implies that technology may be used as a tool/medium to supplement skills and human time rather than to replace a human. As a result, this highlights the importance of future research that further examines technology-based survivorship care interventions that are integrated into existing systems (e.g., survivorship clinics and care plans) and adaptable to survivors’ daily lives.
Moderator analysis confirmed that studies that assessed self-competence-related outcomes showed positive effects compared to studies that assessed other outcomes. One possible factor that may influence the difference in targeted outcomes is survivorship care domains. Indeed, most RCTs implemented to improve self-management, which was the most effective in this study, were much more likely to use self-competence-related scales (e.g., self-efficacy and personal control) as targeted outcomes than other scales. As a result, the larger treatment effects of studies that assessed self-competence outcomes were possibly caused by the use of interventions focusing on self-management in survivorship care. Moreover, many RCTs tended to evaluate quality of life-related outcomes regardless of survivorship care domain, expecting overall positive effects from technology-based survivorship care interventions. However, studies that assessed quality of life-related outcomes did not show positive treatment effects, which is consistent with Wang et al. (2020)'s results. This suggests that technology-based survivorship care interventions for cancer survivors should focus on problems and challenges cancer survivors are facing and corresponding measurements for clearly assessing their issues. Future research should be mindful of developing and implementing interventions designed to address multiple survivorship care domains to ultimately improve the quality of life for cancer survivors.
In this study, age and sex were not significant moderators, indicating that such demographic characteristics may not affect the treatment outcome. Given that participants in the reviewed articles had a higher median age and were mostly female, it may be difficult to generalize our findings, such that future studies with larger sample sizes are needed. Moreover, regarding a cancer type variable, “other cancer type” showed a moderate treatment effect size. This suggests that the specific cancer type may be the optimal target group in applying technology-based survivorship care interventions. For example, Manne et al. (2021) implemented an online intervention, called my SmartSkin that focused on the self-management of cancer survivors diagnosed with melanoma. This intervention was tailored to melanoma survivors considering their unmet needs. In contrast, studies that included two or more cancer types were not effective. As a result, specialized technology-based interventions that consider medical characteristics and unmet needs of the specific cancer type will be useful in maximizing the effects of interventions for cancer survivors.
The current study reported statistically significant treatment effects; however, some variables still showed small effect sizes. This may indicate that samples across the study were inclusive of patients who varied in their need or position to benefit from the interventions, although the risk of bias assessment identified an overall low risk of bias for RCTs. Because technology-based interventions are innovative as a newly emerging tool in cancer survivorship care, it would be hard to assume cancer survivors’ responses to technology-based interventions. Thus, the benefits of interventions may be skewed according to the characteristics of participants. Our findings suggest that screening and assessment to identify adequate cancer survivors who need technology-based survivorship care interventions should be developed. Then, technology-based survivorship care interventions will be better adapted to fit the needs of a cancer survivor population or perhaps do a better job of delivering stepped care services that are algorithmically determined to match a particular level of the domain of need.
Consequently, such a process can be useful in that interventions can be delivered to those who are most likely to benefit, providing “optimal and precise supportive care.”
This study had several limitations. First, there is always a possibility that the study team missed relevant articles regarding technology-based survivorship care interventions, although we attempted to find all eligible articles with thorough reviews of other existing systematic reviews. Second, we found various forms of technology in survivorship care interventions. To improve statistical power, similar forms of technology used in interventions were merged and analyzed in the subgroup analysis. Similarly, reviewed articles assessed diverse types of targeted outcomes. Thus, 46 outcomes were reorganized based on six categories and analyzed in the subgroup analysis. Therefore, the findings should be interpreted with caution. Third, we categorized technology-based survivorship care interventions as survivorship care domains according to the survivorship care framework developed by Nekhlyudov and Gast. Although some studies considered two or more survivorship care outcomes, the current study included only one domain based on the purpose of RCTs with thorough reviews to investigate the major effect of survivorship care interventions. Future studies are needed to examine the mixed effects of interventions that include two or more domains. Finally, survivorship-related variables such as the length of survivorship, remission, or relapse may influence the treatment effect; however, the current study did not include the effects of such variables. It is necessary to address the effects of survivorship-related variables on technology-based interventions in future studies.
Despite these limitations, this study highlights the necessity and importance of developing survivorship care interventions using diverse forms of technology with the involvement of people. Furthermore, interventions that address multidimensional domains for cancer survivorship care should be developed with advances in technology, which in turn can enhance cancer survivors’ capacities to address the diverse issues that they face in the survivorship phase. To deal with cancer survivorship care comprehensively, various health care providers that work with cancer survivors, such as physicians, nurses, and social workers, should plan and carry out effective interventions through a multidisciplinary approach. For self-management interventions that enhance self-efficacy, which are known to be the most effective among technology-based cancer survivorship interventions, social work approaches that effectively intervene in improving the behavioral and psychosocial aspects of cancer survivors in the survivorship stage should be considered very important. Future research is urgently needed on the sustainability of the applicability of technology-based survivorship care interventions to clinical practice and supportive care with the combination of technology and people to support cancer survivors.
In summary, the current study conducted a systematic review and meta-analysis of RCTs evaluating technology-based cancer survivorship care interventions. This study confirmed that overall technology-based survivorship care interventions improved outcomes for cancer survivors. Furthermore, survivorship care domains, comparison groups, and targeted outcomes were significant moderators influencing treatment effects. The current study provides strong research evidence supporting technology-based survivorship care interventions that improve self-management skills by enhancing self-efficacy for adult cancer survivors.
Footnotes
Author Contributions
All authors contributed to the study’s conception and design. Material preparation and data collection were performed by Jung-won Lim, and meta-analyses were performed by Anao Zhang. Bradley Zebrack oversaw the entire study, and resolved disagreement. The first draft of the manuscript was written by Jung-won Lim and all authors commented on the previous version of the manuscript. All authors read and approved the final manuscript.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
This article does not contain any studies with human participants performed by any of the authors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.