
Abstract
Contemporary transgender youth in the U.S. today face increasing stigmatization as extraordinary legislative attacks intensify discrimination and exclusion of these young people in healthcare, recreation, and school life. These attacks reflect broader political, religious, and cultural ideologies embedded in systems of power that regulate the provision of healthcare for American transgender youth. We apply Foucauldian discourse analysis and a theory-driven conceptual framework for structural analysis of transgender health inequities—Intersectionality Research for Transgender Health Justice—to identify discourses youth encounter within healthcare practice. We analyzed data from interviews conducted in Western Washington State with youth ages 13–17 (n =11) and asked how transgender subjectivity was constructed in their accounts and in what ways youth made use of the discursive resources available to them when navigating systems of care. Three sets of discourses—discourses of normativity, discourses of temporality, and discourse of access—characterized participants’ narratives. We discuss how participants negotiated discursively situated systems of power in order to ensure their safety and access to care.
Introduction
Transgender (henceforth, trans) youth face increasing stigmatization as extraordinary legislative attacks intensify discrimination and exclusion of these young people in healthcare, recreation, and school life. In 2021 alone, lawmakers across 35 U.S. states brought forth 127 anti-trans bills and nine states passed some form of anti-trans legislation (Levin, 2021). In 2022, state legislatures across the U.S. continue to seek more measures than ever specifically targeting trans people across a range of issues (American Civil Liberties Union, 2022). These measures mark transgender Americans for discrimination, including prohibiting changing sex on birth certificates (e.g., MO HB2086), barring trans people from participating in sports (e.g., MO HB2735, SC H4608, AK SB140), and withholding medical treatment from trans youth while simultaneously criminalizing providers and parents who support their health and well-being (e.g., TX SB1646) (Conron et al., 2022). Importantly, trans people face discrimination and violence throughout much of the world, and in many countries trans identities are criminalized (Savage & Greenhalgh, 2019).
The escalating legislative attacks on trans youth in the U.S. today follow decades of increasing attention among researchers and clinicians to gender non-normative children, which began in the 1960s and ‘70s as they started to study what was perceived to be a mental health crisis of feminine boyhood following World War II (Bryant, 2006). Researchers at the time were interested in identifying “pre-homosexual” children and goals of treatment were aimed at aligning children’s gender expression with existing social norms (Bryant, 2006). Recent shifts in pediatric treatment models throughout the U.S. have been regarded widely as a paradigm shift from gender pathology to gender affirmation (Pyne, 2014), with multiple professional organizations (e.g., American Academy of Child and Adolescent Psychiatry, American Academy of Pediatrics, American Psychological Association) issuing policy statements confirming that diversity in gender expression and identity represent “normative developmental processes for children and adolescents and are not inherently pathological aspects of human experience” (Leibowitz et al., 2020, p. 111).
Previous research has shown that adult trans patients are frequently made aware of broader political, religious, and cultural ideologies through their medical experiences and that knowledge of broader socio-structural processes effects how they navigate healthcare systems (Dewey, 2008). For example, trans people who seek to modify their bodies are routinely denied access to medical interventions if they fail to persuasively produce set narratives that align with how trans patients are discursively constructed in existing diagnostic criteria (J. R. Latham, 2016). Medical logic both produces trans patients as distinct from non-trans patients who access the same procedures and is implicated in producing the very problems it is designed to treat (J. R. Latham, 2017a). In an attempt to gain credibility and avoid stigma, trans adults often prepare how they will approach healthcare professionals or alter their behavior in order to improve the likelihood of receiving appropriate care (Dewey, 2008). It is likely that trans minors approach healthcare in ways that are strategically similar to trans adults, meaning that when possible they construct narratives most likely to ensure their safety and access to care.
These narratives—or discourses—are influenced by broader political, religious, and cultural ideologies that play crucial roles in producing policies and practices related to the provision and regulation of healthcare for trans youth. We adopt a Foucauldian definition of discourse in which the word discourse refers to “practices that systematically form the objects of which they speak” (Foucault, 1972, p. 49). In Foucauldian terms, discourse makes it possible to think some thoughts and not others, as well as empower some speakers and disqualify or invalidate others (McHoul & Grace, 2015). Dominant discourses work to promote viewpoints and uphold ideologies that codify existing power relations, hierarchies, and social structures (van Dijk, 2013). Foucault was primarily concerned with power; specifically, how power, discourse, and social identities—what he termed “subject positions”—are constructed. Foucault’s work was directed at entire systems of thought or “knowledge systems” (Hacking, 2004) (e.g., medicine, religion, psychology, law) and was concerned with the dynamics through which individuals become—or are forced to become—institutionally recognizable types of subjects. Foucault argues that discourse can be both an instrument and an effect of power, serving to both reinforce power and also undermine and expose it (Foucault, 1978, pp. 100–101). Rather than merely represent or mirror reality, discourses construct social reality and are enacted and contested at the site of the body (Mills, 2003).
Trans youths’ discursive approaches to health and social services (i.e., what they say in exchanges with adults in order to get their needs met) must be understood within the context of widespread health and social policies that render legal minors unable to make autonomous decisions about their bodies and health and within a political landscape where policies regarding their rights to access care are changing rapidly and vary considerably from state to state, even when conditions of parental consent are met. In this study, we understand “transgender” not as a predetermined category into which individual identities or bodies are inherently formed or “ready-made,” but as a shifting discursive category that is produced through medical, legal, and cultural practices over time (Beauchamp, 2019; Borba, 2019). One’s self-identity and one’s identification by others are interwoven and shaped by relations of power (Valentine, 2007) that, as Stryker writes, “operate on actual bodies, capable of producing pain and pleasure, health and sickness, punishment and reward” (Stryker, 2016, p. 3).
In response to increased anti-transgender discourse that appears in the news, negative mental health outcomes (e.g., disproportionately elevated rates of anxiety, depression, and suicidality) among trans youth have been exacerbated (Hughto et al., 2021; Pham et al., 2020). Many trans youth also experience family rejection, bullying, intimate partner violence and homelessness (Day et al., 2018; Reuter et al., 2017; Simons et al., 2013; Sterzing et al., 2017). Access to care improves long and short-term health outcomes for these youth, yet research shows that few are actually able to access health services appropriate for their needs (Gridley et al., 2016). Researchers have argued that the fractured policy landscape in the U.S. today subjects trans people, and their health, to the judgment of service providers, insurance companies, and legislators who decide what transgender-specific healthcare will or will not be covered (Bakko & Kattari, 2021). Previous studies have demonstrated that multiple structural level factors create barriers to care, including: geographic disparities in the availability of qualified medical and mental health providers able and willing to offer appropriate care, fear of discrimination from healthcare practitioners, and disparities in health insurance reimbursement that are likely to disproportionately exclude youth from poor and working class backgrounds (Kimberly et al., 2018; McCann et al., 2017; Padula & Baker, 2017; Romanelli & Hudson, 2017; Safer et al., 2016). The present policy landscape is also complicated by varying non-discrimination laws in each state that either explicitly protect or exclude transgender-specific healthcare coverage for different types of insurance (Bakko & Kattari, 2021).
Among the studies that have explored institutional and provider level issues impacting contemporary trans youths’ abilities to access care (i.e., barriers to care), researchers have generally recruited participants from within existing clinical samples (i.e., youth who already have some point of entry into care) and often focus on the perspectives and experiences of parents and caregivers (Chen et al., 2016; Nahata et al., 2017; Olson-Kennedy et al., 2016; Stevens et al., 2015; Vance et al., 2014). Particular types of experiences have been privileged, with most studies focused on individuals who seek and are able to access biomedical intervention before the age of 18, largely because of parental support and access to private insurance (Frohard-Dourlent et al., 2017). As Latham has argued, transgender subjectivity “is being constituted by practices that require resources: money and time, stress, pressure, clinic visits, tests…” (Latham, 2017b, p. 185), and in the case of legal minors, parental consent.
It is possible that framing access to care primarily in terms of access to pubertal suppression, hormones, and surgeries renders invisible the range of healthcare needs of many trans youth, particularly within a healthcare system in which racial and economic disparities exist. Diagnostic disparities have been documented in pediatric mental health, for example, particularly for African American and Latinx children and it has been suggested that the specific terminology used for screening and diagnostic measures may influence identification of minority individuals in need of treatment (Alegria et al., 2010; Dilsaver, 2001). Additionally, children from poor families are less likely to use physician services and have more difficulty getting a referral to a specialist than children from middle- and high-income families (Newacheck et al., 1996). A recent population-based comparison of transgender and cisgender youth found that in addition to poorer health, transgender youth have differential usage of healthcare, including lower usage of checkups and other preventative healthcare (Rider et al., 2018). Importantly, while use of histrelin acetate implants (i.e., puberty blockers) has increased dramatically since 2004, treated transgender youth were more likely to be White (Lopez et al., 2018).
While significant advances have been made to support the health and well-being of some trans youth, studies of health issues impacting trans youth today tend to approach gender (i.e., ‘transgender’) as an apolitical dimension of identity. This framing may obscure or render invisible the mechanisms via which systems of power produce social identities (e.g., race, gender, sexual orientation) as well as the ways that systems of power are enacted through health and legal systems and reinforced via everyday socio-structural practices. Therefore, we sought to better understand how systems of power operate in the discursive and material management of health resources when those resources are considered treatment for trans minors. We were particularly interested in better understanding how youth under the age of 18 discursively managed their access to care (i.e., how they strategically employed language and narratives to navigate institutional systems and socio-structural processes to get their health needs met). We analyze youths’ accounts of navigating healthcare through qualitative interviews. Analytically, we aimed to identify the types of discourses youth encountered about who they are within various processes of health service provision, as well as the types of narratives they constructed in order to ensure their safety and access to care.
Conceptual and Analytic Frameworks
Our study simultaneously employed two conceptual and analytic frameworks to elucidate how relations of power produce social identities and inform how trans youth strategically employ language and narratives in accessing care. These are the Intersectionality Research for Transgender Health Justice (IRTHJ) framework (Wesp et al., 2019) and the Foucauldian concept of governmentality (Foucault, 1991).
Intersectionality Research for Transgender Health Justice is a theory-driven conceptual model rooted in intersectionality and structural injustice. We apply this framework to examine how structures of domination (e.g., cisnormativity and adultism) are enacted through institutional systems (e.g., health and legal systems) and reinforced through everyday socio-structural practices (e.g., pathologizing, gendering, medicalizing). Cisnormativity refers to the epistemological framework that approaches gender as a system comprised of two supposedly stable and naturally occurring biological sexes—male and female—with two fixed and normative social categories—man and woman (Stryker, 2016). It represents the dominant discourse against which all other discourses about gender are situated and is grounded in the historical privileging and naturalization of cisgender bodies and psychic experiences (Karkazis, 2008; Meyerwitz, 2002). Adultism—also referred to as youth oppression (DeJohn & Love, 2015)—refers to practices and perspectives based on the assumption that adults are superior to young people (i.e., people younger than age 18) and as such entitled to act upon young people (e.g., punishing, threatening, revoking privileges, controlling, disciplining) without their agreement (Bell, 2010). Like cisnormativity, adultism is reinforced via social institutions, laws, and attitudes. Intersectionality Research for Transgender Health Justice establishes three actions for advancing transgender health justice—naming intersecting power relations, disrupting the status quo, and centering embodied knowledge. Each of these were addressed in both the conduct and analysis of this study and we identify the various actions throughout the methods and discussion sections.
The Foucauldian concept of governmentality in many ways parallels IRTHJ in tracing how power structures are enacted and reinforced through institutions and social practices. Governmentality describes the complex processes by which a society polices and shapes the conduct of an individual or group of individuals and is an activity that links three forms of power—the states of domination (sovereignty), disciplinary power (discipline), and the government of other and self (government) (Foucault, 1991). Foucault’s conception of power holds that power is pervasive, socially distributed and discursively managed. In a Foucauldian sense, “power is not something that people possess – instead, it circulates throughout social relations and constitutes people into certain kinds of subjects suitable to a prevailing political order” (Sutherland et al., 2016). The production of knowledge is an integral part of struggles over power and Foucault championed the notion that the production of information by the marginalized themselves can alter the status quo. Relatedly, in addition to the various theoretical and methodological steps we took to operationalize the IRTHJ action “centering embodied knowledge,” our analytic approach reflects a trans studies framework, which considers the embodied experience of trans people to be an essential component of analyses of the political dynamics and everyday issues that impact their lives (i.e., experiential knowledge is as legitimate as other forms of supposedly objective knowledge) (Stryker, 2016).
Key to this study is the Foucauldian concept of disciplinary power, a form of power enacted on individuals or groups of individuals that is meant to produce certain effects on their behaviors, attitudes, and capabilities (Hindess, 1996). In IRTHJ terms, disciplinary power can be located as a socio-structural process. Socio-structural processes (e.g., gendering, pathologizing, etc.) reproduce inequality by maintaining the status quo and enforcing norms within and across institutional systems. Discpline is concerned with a particular kind of control that is internalized by the individual and which results in disciplinary pressure to act or behave in a particular way (Mills, 2003). According to Foucault, discipline is a set of tactics, procedures, and ways of behaving that are negotiated within institutional contexts, which then flow through individual ways of thinking and behaving. These tactics simultaneously produce the individual as an institutionally recognizable type of subject—they bring the subject into being. In this study we were primarily interested in the intersection of two axes of power/structures of domination—namely those related to age/adultism and gender/cisnormativity—and how they manifested and were discursively managed by the youth we interviewed. See Figure 1 for a diagram of how each intersectional cause of health inequities in the IRTHJ framework is linked to a parallel Foucauldian concept we employed in our analysis. Relationship of intersectionality research for transgender health justice framework and parallel Foucauldian concepts.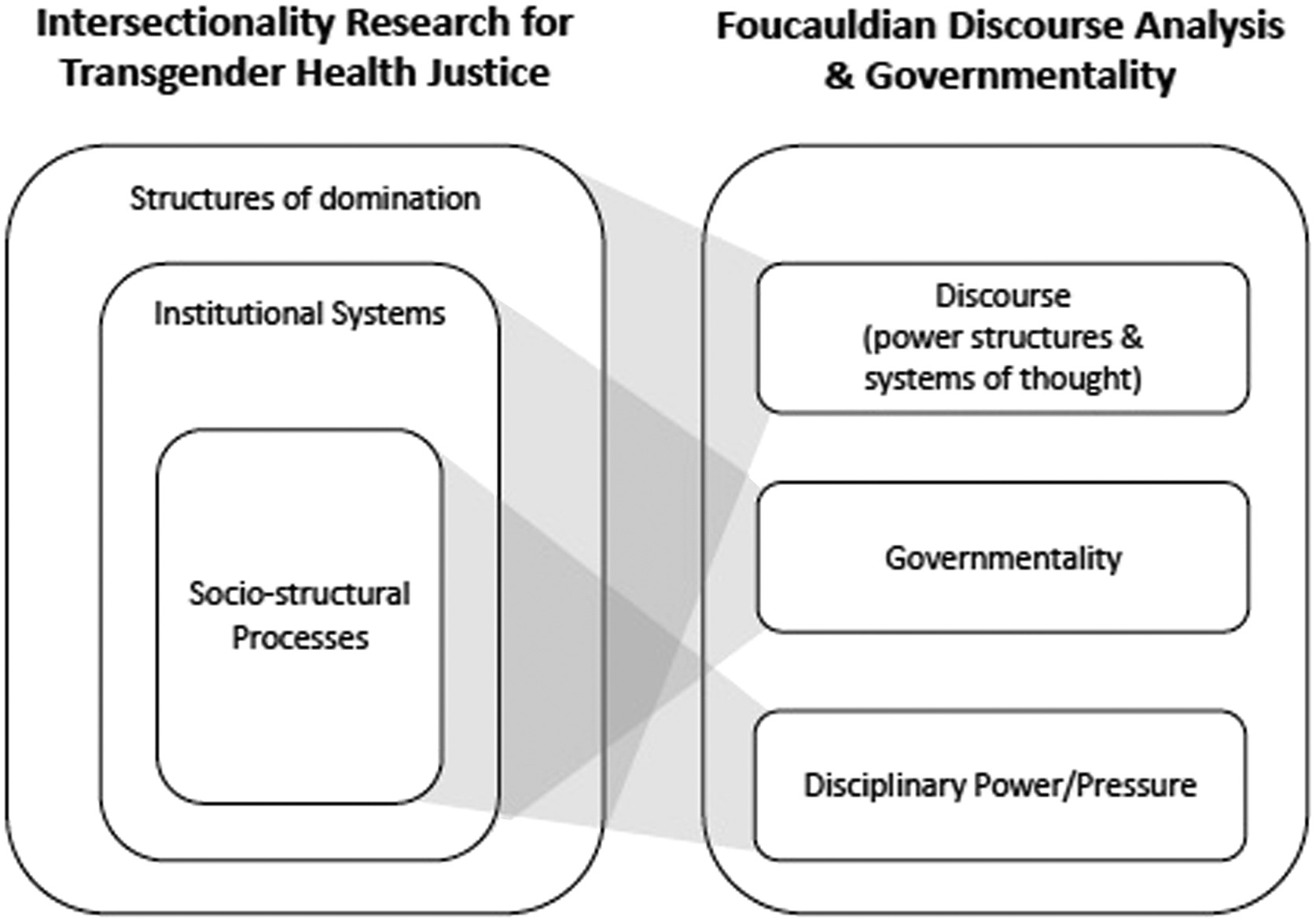
Methods
Recruitment
We recruited trans youth in Western Washington State for participation in one-on-one interviews about navigating healthcare. Inclusion criteria were age 13–17 at the time of interview, English-speaking, transgender-identified, and having sought care in Washington State. Our goal was to recruit a subset of trans youth with a diversity of accounts of healthcare access, including youth who may have difficulty accessing care because of insurance status, limited or lacking parental support, and/or geography. Recent evidence shows that cyberspace plays a critical role in the lives of queer and trans youth (McDermott & Roen, 2012). Accordingly, our recruitment strategy included posting information about this study electronically via online social media (e.g., Instagram). Hard copy materials were also distributed at local organizations that serve youth (both LGBTQ+ specific and not) as well as at LGBTQ+ youth advocacy and community organizing events. Additionally, information about this study was posted electronically to existing parent support groups and shared with adults in various supportive roles in youths’ lives (i.e., parents, teachers, school counselors, therapists, etc.). Of the 11 youth who participated in interviews, seven were given information about the study through a trusted adult, whether that be a teacher, counselor, or parent.
Ethical Considerations & Waiver of Parental Permission
Ethical approval was obtained from the BLINDED Institutional Review Board (IRB STUDY00005443). We obtained a waiver of parental permission, which permitted the enrollment of youth under age 18 without parental involvement or consent. While parental consent is a hallmark of pediatric research ethics, especially for vulnerable children, requiring parental consent for participation in this study could promote a selection bias in favor of youth with supportive parents and would be problematic for youth who may not feel comfortable asking parents’ permission or speaking about their gender identities in the presence of parents (Flores et al., 2018). Youth were given the option to interview in the presence of a youth advocate. The use of youth advocates has been proposed as a substitution for parental consent, particularly when disclosure to parents of the goals of a study could negatively impact the parent/child relationship, particularly in ways that might provoke parental rejection or emotional distance from the child (Panfil et al., 2017). Obtaining a waiver of parental permission, the optional use of the youth advocate, and our emphasis on supporting youth in choosing the specific interview conditions that would make them most comfortable and keep them safe was an operationalization of two IRTHJ actions, disrupting the status quo and centering embodied knowledge. Of the 11 participants, seven chose to participate without their parents present. Three of these youth requested the presence of the youth advocate during consenting, and an additional two youth requested her presence during the interview itself. The youth advocate is a doctoral candidate in the Department of Epidemiology at the BLINDED School of Public Health with over 10 years of experience supporting and advocating for queer and trans youth. Participants provided written informed consent prior to interviews. Youth participants received a US$25 retail gift card for participating in interviews.
Data Collection
Data collection occurred between November 2018 and September 2019. The principal investigator conducted in-depth, semi-structured interviews in person at confidential locations chosen by participants. Prior to interviews he disclosed his transgender status and invited participants to ask any questions they had about his experience, identity, and the goals of this study. The youth advocate, when present, also shared her identity as a queer cisgender woman and discussed her relationship to transgender communities. This practice is consistent with discursive interviewing techniques, which are more informal conversational exchanges than other interviewing techniques and involve interviewers as active participants rather than positioning them as neutral “speaking questionnaires” (Kvale & Brinkmann, 2009, p. 156). Situating ourselves as active participants both helped to establish rapport and allowed us to address how interviews frequently serve as a technique for the public construction of the self (Kvale & Brinkmann, 2009). The power relations that exist between interviewer and interviewee, researcher and researched, construct a particular relationship that shapes how interviewees present themselves. This dynamic was especially important to address in this study because trans people are frequently called upon to legitimize their value and authority of knowledge via extensive medical and mental health evaluations in order to receive a medical diagnosis (gender dysphoria) (Dewey & Gesbeck, 2017). In fact, mandatory referral of trans people to psychological evaluation may violate patients’ rights to self-determination and constitute a form of discrimination (Latham, 2013, p. 648). In an effort not to reproduce this socio-structural process via interview dynamics, during the consenting process we explicitly stated that we were not asking youth to legitimize their experiences in terms of gender or prove themselves to us and that there were no right or wrong things to say. In many cases we affirmed and actively engaged with youths’ accounts and analyses of healthcare system navigation, also consistent with discursive interviewing techniques.
Interview Guide.

Throughout the data collection phase, reflexive discussions between the interviewer and youth advocate were conducted in a non-linear, back-and-forth manner and centered on transparency in the research process, addressing youth–adult power dynamics in interviews and the research more broadly, and the varying ways that our social positions impacted how interviews were conducted. The interviewer kept a reflexive journal during the data collection and analysis phases of this project. A central point of reflection was the intergenerational nature of interviews, particularly regarding how his position as a trans researcher—one who is also studied and researched—might directly influence the collection and analysis of data for this study. He paid particular attention to any possible transference that occurred during interviews and the impact this might have on what was rendered permissible or forbidden for participants to say during the interview process. Interviews lasted between 60–120 min and were audio-recorded and transcribed by a professional transcriptionist. Participants were given an electronic copy of the transcript and invited to make edits or additions to original interview material. This simultaneously reflected the methodological objective of member checking and was a way of operationalizing the IRTHJ action centering embodied knowledge (i.e., the transcript operates as a kind of story-as-data where youth were given an additional opportunity to craft their narratives in words of their own choosing as much as possible). One participant chose to edit the interview transcript, which involved the inclusion of additional details regarding a healthcare encounter they narrated during the original interview.
Data Analysis
All youth participants were invited to participate as members of the data analysis team. Of the 11 participants who participated in one-on-one interviews, two chose to participate as data analysts. While this study did not adopt a community-based participatory research (CBPR) approach in the traditional sense—meaning youth were not involved at every stage of the research process, for example, conceptualization—our decision to include youth in qualitative data analysis and interpretation is consistent with the tenets of youth-led participatory action research (YPAR). Youth-led participatory action research is a type of CBPR that engages young people in conducting research to better understand issues and injustices that affect their lives, and advocating for change based on research evidence (Ozer, 2016; Wallerstein et al., 2018). Youth-led participatory action research may be especially useful for research with marginalized youth, such as trans youth, for a number of reasons: (1) It can help to support collective senses of identity and purpose (Ozer & Piatt, 2018), (2) it can empower youth to contribute to knowledge generation about their lives, particularly youth who have not historically been consulted about research conducted about them (Katz-Wise et al., 2019), and (3) it allows for a reconceptualization of youth as experts of their lives and co-creators of knowledge rather than as problems to be fixed (Bettencourt, 2020; Ozer & Piatt, 2018). Including youth in data analysis and interpretation was both a way of thinking beyond traditional approaches to representation in qualitative research and an operationalization of the IRTHJ actions disrupting the status quo and centering embodied knowledge. Given that discourse analysis focuses on how knowledge and truth are generated and on the power relations embedded within discourses, we viewed inclusion of youth in the data analysis and interpretation phases of this study as an important intervention for disrupting traditionally held power dynamics that situate research subjects as objects of study rather than as agentic co-creators of knowledge in research processes, particularly when those research subjects are legal minors.
We utilized Willig’s framework for Foucauldian Discourse Analysis to guide the analytic process (Willig, 2008). Prior to the analysis phase of this project the primary researcher hosted three educational sessions for youth participant-researchers and the youth advocate, each of which lasted approximately 2 hrs. The goals of these sessions were to situate discourse analysis epistemologically, understand the types of knowledge it aims to produce and the role that discourse analysts perform in the research process. Prior to the analysis of interview data, analysts collectively participated in practice coding sessions using media texts. Notably, both youth participant-researchers had prior exposure to discourse analysis as it is employed in literary criticism and performative theories of language (Mills, 2004). The analysis team was comprised of the primary researcher and interviewer, the youth advocate, two youth participant-researchers, and a senior researcher with experience conducting discourse analyses. Three members of the analysis team identified as transgender and two as cisgender. All of the data analysts were white.
According to Willig, “Foucauldian discourse analysts focus on the availability of discursive resources and the implications of this for those who live within [a particular discursive economy]” (Willig, 2008 p. 130). Thus, our analytic goal involved identifying discourses that both constrained and enabled participants’ access to care, as well as how youth did and did not engage these discourses in order to negotiate the power relations implicit in their interactions with systems of care. The primary researcher was responsible for organizing the data and coding process. The analysis began with each analyst reading and rereading the transcripts carefully. The text was initially coded by multiple analysts, with each transcript being coded by at least two analysts. Codes were then reexamined and reviewed—read and reread line by line and word for word—in order to ensure that codes reflected the identification of the text that contributed to the discursive object(s). We then began grouping codes to identify discursive constructions related to participants’ narratives (i.e., what they said and how they said it). During this process, the coding and discursive constructions were discussed by authors in-depth on multiple occasions. All voices were considered equally, and discord was viewed as an important opportunity to reflect on how our varying social positions (e.g., as trans individuals, as youth, as nurses, epidemiologists, researchers, etc.) informed how we differentially coded various segments of data. When disagreement occurred between researchers about coding individual segments of data, youths’ analytic perspectives were privileged.
Discursive constructions were then analyzed for identifying what Foucault refers to as discourses. At this stage of the analysis, we closely examined the discursive contexts in which the different constructions of objects were being deployed (e.g., in conversations with parents and providers, via insurance codes, in electronic health records). Discursive constructions were then analyzed for the purpose of identifying broader discourses. While Willig’s framework for Foucauldian Discourse Analysis does not address Foucault’s concern with the evolution of discursive formations over time (i.e., their genealogy), throughout our analysis and particularly at this stage we frequently discussed the evolution of language to describe the bodies of transgender individuals and transgender-specific procedures (e.g., “transsexual” vs. “transgender,” “sex-reassignment surgery” vs. “gender-affirming surgery”) and the implications this might have for participants. The final stage of analysis involved a higher level of abstraction, in which we theorized the meaning of the discourses and the functions they served. Discussions between the authors were continuous throughout the analytic process, which took place over a series of 3 months and was conducted via a back-and-forth approach rather than a linear manner.
While a number of parents’ accounts of healthcare navigation were present in the text, specific analysis of parents’ accounts is beyond the scope of the present analysis. Parents’ accounts were not excluded from the text but were not interpreted analytically—just as comments by the interviewer and youth advocate were not interpreted analytically. In the present analysis, parents’ accounts were considered attempts to assist their children in the telling of their stories. Notably, when parents were present for interviews (n = 3, where n = interviews) they actively supported their children’s authority of knowledge and on each occasion offered to leave the room if youth preferred to talk with the interviewer one-on-one. Future studies might evaluate the discursive exchanges between parents and trans youth during the interview process itself.
Results
Participant Characteristics
A total of 11 youth participated in interviews and ranged in age from 13 to 17 years. Participants lived in a variety of locations throughout Western Washington State, including in both urban (n = 9) and rural (n = 2) settings. Rural versus urban designation was based on self-identification by participants. Participants represented a variety of gender identities including transgender male (n = 6), transgender female (n = 3), queer/gender non-conforming (n = 1), and transmasculine/FTM (n = 1). The majority of participants were white (91%; n = 10). One participant was multiracial.
Normativity
Participants were overwhelmingly met with cisnormative and transnormative discourses when navigating healthcare services. Cisnormativity and transnormativity are two interrelated normative, or dominant, discourses that are produced and reproduced in institutional systems such as healthcare, education, and the legal system. Discursively, cisnormativity is based on the assumption that cisgender is the norm, which is privileged over other forms of gender identity (Stryker, 2016). Transnormativity, like cisnormativity, is a normative ideology that pressures trans people to perform normative identities and fixes a hierarchical order of legitimacy in trans identities. It privileges a medical model of transgender identity and marginalizes and delegitimizes trans and gender non-normative people who cannot or do not wish to medically transition (Johnson, 2016). In anticipation of normative discourse, participants talked about preparing scripted approaches for how they talked about themselves when interacting with healthcare providers. Normative discourse also showed up as barriers in broader structural and systemic processes such as electronic health record systems and insurance coding and billing. Normative discourse manifested in patient-provider interactions as talk of social ideals about gender that went unquestioned by providers, and sometimes parents, and that were presumed to be normal and healthy.
Participants talked about the need to prove or explain their genders to providers and parents, and frequently recounted being questioned about being “trans enough” or being “really trans.” Youth were aware that receiving a gender dysphoria diagnosis was contingent upon convincing providers of their authenticity as trans subjects, which was largely dependent on the reproduction of certain narratives of gender identity development and discomfort about one’s body. These narratives both did and did not accurately reflect youths’ lived experiences. “I remember I was really nervous because I didn’t want to do or say anything wrong that would make [the doctor] say, ‘Well, no. I think we can wait a little bit longer.’ The feeling going into it – I was like, ‘I have to say everything right. I have to dress correctly, like my hair has to look good. I need to talk as well as I possibly can. I didn’t want to act or portray as though I was at all feminine…[The doctor] needs to know that I’m uncomfortable in this body. I wanted to portray that as much as I could.”
Participants framed themselves as active agents in these interactions. They also talked about how their social positions as young people and as legal minors influenced their discursive exchanges with healthcare providers. “I think the big question I’ve come back to over and over again… [the physician] asked me, ‘What does being a girl mean to you? What does that mean when you say you’re a girl?’ I didn’t have an answer. He was very skeptical of my lack of an answer. He said, ‘I feel like you should be able to talk about this. I think you might be moving too fast if you can’t talk about this.’ And I was like, ‘Well, no. I think it’s just a stupid question.’ But I didn’t say that because I was 14 and small and nervous. Cis[gender] people don’t have to answer this question – ‘How do you know you’re a woman?’ I don’t know how I can be expected to.”
Youth frequently encountered normative discourse in providers’ talk about goals of care. Successful surgical outcomes, for example, were framed as those in which the bodies of trans people were made to be the most cisgender passing. “[Medical providers] do assume that your goal is to achieve some level of cis[gender] passing-ness. One thing I haven’t loved is that almost every time I’ve done surgery stuff, I’ve had surgeons’ main focus [be on] scarring. I feel like surgeons often come from a place of trying to make you look cis[gender].”
Normative discourse also showed up in participants’ lives in broader social settings, and participants talked about how normative discourse delegitimized their subjectivities. “For a long time when I was first coming out [as trans], I was moving inside a lot of trans circles that had this kind of path where you realize you’re trans, you come out to your parents, they put you on hormones, they buy you a new wardrobe, and then you’re you. And you forget that you ever weren’t [you] and everything is dandy. And I’m like, ‘Well I failed step one. Can’t come out to parents. What now? Guess I’m not making any progress.’”
In the Foucauldian conception of discourse—where discourse refers to “practices that systematically form the objects of which they speak” (Foucault, 1972, p. 49), discourses of normativity produced trans youth as a category distinct from cisgender youth who require medicalized gender transition in order to be ‘real’ and thus reinforced the powerful role that medicine plays in regulating sex/gender (i.e., the status quo) (Spade, 2003). As dominant discourses, cisnormativity and transnormativity operated on bodies by foreclosing many trans possibilities beyond medicalized gender transition and maintaining the status quo in terms of gender and age (i.e., discourses of normativity were produced through intersecting power relations related to both cisnormativity and adultism). Young people’s authority of knowledge was called into question because of their age, at the same time they were required to be certain of themselves in terms of gender.
Temporality
Discourses of temporality showed up in conversations youth had with providers, and with parents, about risks and benefits of biomedical intervention (i.e., talk about puberty blockers, hormones, and/or surgeries). These discourses were present as talk about waiting to access care and the permanence of puberty blockers, hormones, and surgeries. Like discourses of normativity, waiting to access care was frequently talked about in relation to participant’s status as minors, particularly with regard to treatment guidelines that regulate when and at what age youth are able to access particular interventions. Waiting was often reflected in talk about insurance access, approvals, denials, and exclusion. Most participants talked about how other aspects of their experience influenced how quickly and in what ways they were able to navigate healthcare structures. In other words, aspects of youths’ social positions such as race, insurance status, and parental support, for example, operated in conjunction with youths’ age as intersecting relations of power that influenced for how long and for what reasons they were made to wait. This has been reflected in other studies that address the subjective experiences of medicalized gender transition through a temporal lens (Pitts-Taylor, 2019). “If you’re a person of color that’s trans or if you’re low income and trans or if you’re low income and a person of color that’s trans…even not being a straight trans person can set you back. I feel like that happens a lot with lower income trans youth. It’s like their entire experience is impacted by their parents’ income, which I don’t think is fair. I have a friend who has…worse insurance than me…for like people that are lower income than I am. And he waited an entire year to get on [testosterone]. I feel it’s not a fair system because it’s based on what your income is. I think it sucks they just have to wait longer because they weren’t as privileged to be born into a rich family. It just sucks that it’s an unfair system.”
When participants spoke about “the system,” as above, they referred flexibly to broad social hierarchies, specific health and clinic systems, and normative ways of thinking about gender that are embedded throughout all aspects of everyday life. They talked about the powerlessness they felt regarding wait times, often because of their status as legal minors who were also trans. They referred most frequently to waiting for puberty blockers or hormones, but a few participants spoke about waiting in the context of surgery as well. Waiting was also talked about as a strategy for protecting oneself from the possible reactions of others when they anticipated rejection, exclusion, and violence, frequently by parents and other family members. This included waiting to disclose their identities and waiting to “be trans.” Possible parental reactions figured heavily into how youth negotiated disclosure of their gender identities. “When I first realized I was trans my instinct was like, ‘I’ll wait and then I’ll just run away from everyone and do this on my own.’ Because I [didn’t] really want to deal with other people. I was really resistant to like, being trans…like I don’t want to be trans. I wanted to disappear and transition and just like not deal with being ‘the trans person’ in the family, or whatever. I didn’t want that for myself. Because who does? I mean you’re told that being trans is not something people generally…[cis]gender people generally don’t love trans people, I think.”
Conversely, many participants talked of waiting as a waste of time that required them to remain in a state of protracted and unwanted liminality. “Initially I was like, ‘Oh I’ll wait until I’m 18 and then I’ll transition, and I won’t have to deal with coming out to my parents. I had this total fantasy about how I was going to disappear and go be trans. Then I kind of realized… I don’t really want to wait that long. Every minute I don’t work towards this is wasted.”
In their interactions with providers, the possible permanence of intervention was used to both justify and caution against puberty blockers, hormones, and surgeries. Biomedical intervention was frequently framed by providers and sometimes parents as more or less permanent and thus, more, or less risky. Arguments about risk were used to support particular timelines about when and how youth were allowed to access particular types of interventions. Participants were often cautioned against moving too quickly because of the permanence associated with the initiation of hormones or when seeking surgeries. “[The pediatrician] was like… ‘I will give you a recommendation [to a gender specialist] if it’s what you really want but I’m really’ – He wanted to caution us against moving too quickly because he’s against permanent changes in children at a young age. He said he doesn’t think it’s a good idea. He hasn’t seen it work out well in the past. He just doesn’t think there’s enough science behind it to back it up. At the time I was just starting like ‘assigned male at birth puberty’ kind of stuff. And he didn’t conceive of that as a permanent change at all in any way.”
Discourses of temporality involved negotiations of subjectivity via which youth both resisted and embraced “being trans.” As a function of governmentality (i.e., complex processes via which societies police and shape the conduct of individuals and populations), discourses of temporality governed not only how youth could “be trans” (i.e., normativity), but when youth could “be trans.” Waiting was talked about as a structural impediment to young people’s self-determination, a form of discipline constructed via intersecting power relations related to youths’ age and gender meant to keep participants “in their place.” Importantly, discourses of temporality were often grounded in normative ideologies regarding development (e.g., that growth is always linear, that normal gender identity development is cisgender and somehow less “permanent” than transgender identity development).
Access
Discourses of access were present in youths’ narratives as talk about pathways around or pathways through the healthcare system. Participants frequently named backdoor channels, or avenues via which they were able to access services or providers through channels that arose from community and peer connections. These connections—what has been referred to as transgender community connection (TCC) in other studies of how trans people navigate healthcare (Sherman et al., 2020)—facilitated passage through unknown or infrequently traveled routes through systems of care. Knowing when and how participants might be confronted with exclusion or denial when navigating insurance reimbursements, for example, and learning of others’ strategies for successfully navigating such denials represented possibility for many youth and helped them to conjure futures where their health needs would be met. Participants spoke to the porous nature of the systems they navigated and the practicality of being guided by people within and outside them, often other trans youth or parents of trans youth, as well as healthcare workers responsible for insurance billing and coding. Transgender community connection was key to helping youth and their families identify alternate pathways with multiple possible entry points—discursive portals through “the system”—as well as strategies for discursively framing their narratives in line with what was required to access care. “I was thinking about going to one bottom surgeon and then [another trans person] told me that I shouldn’t go to that bottom surgeon. The only reason that I found the names of the people that I’m going to [now for surgery] was because I happened to see a transgender man who is a therapist. If we didn’t know the steps to [navigate] the insurance [denials] we might have just given up.”
Participants talked about preparing for healthcare encounters through participation in online discussion forums specific to trans youth. These discussions served as a place where youth could identify discursive resources available to them and how and when to deploy particular narratives (i.e., how to tell their stories, what to say to providers, what not to say, etc.). Legal documentation, when participants had it, also figured prominently in how they presented themselves to providers, and many participants talked about folders they kept with documents so that they could prove their case when needed. Participants also talked about how relationships with trans adults provided context for their experiences with healthcare navigation and roadmaps for deploying particular narratives at specific time points.
Access, however, was not always constructed as a possibility. Youth also talked about the systems they navigated as inflexible and inequitable. Depending on the channels or pathways through which they were able to access services, a variety of different policies and institutional guidelines impacted participants’ wait times and the accessibility of services. “It’s just kind of isolating because I can’t go to the same place I’ve always gone since I was a kid. And now I have to go far away. And even this clinic that I go to in [redacted town name]… I don’t feel like as safe or as comfortable there just because it’s not what I’m used to. It’s a different town. [The provider] is the only one licensed in our area to treat trans people and… like assign us onto hormones. So, she’s the only one who can look at you and say, ‘okay, your [assigned] gender [at birth] is not for you.’”
Additionally, participants often talked about pivotal experiences with providers who spent a considerable amount of time helping them understand insurance reimbursement processes. These providers were talked about as people who “went out of their way” and were constructed as doing the right thing or invested in changing the system. “One of the things that I liked about [the surgeon] is [that] he spent a fair amount of time talking about fighting with the insurance system to get them to reimburse us – not just to help reimburse us but with trying to correct the system so that the system is more cooperative. [He said], ‘Expect to have to appeal three times. Then you’ll go to a state mediation board. By the time you get to the state medication board then you’ll…’ He made it very clear that he was on the right side.”
Participants frequently spoke of one provider in particular, whether or not they had directly interacted with him. Talk of this provider centered on his approach to the consent process and his willingness to discuss divergent or alternate pathways (i.e., non-normative pathways) for accessing puberty blockers and hormones. “I feel like he was very understanding and didn’t really ask me to prove [I’m really trans]. I’ve had doctors who wanted me to explain to them how I feel [in terms of gender]. And he didn’t even really ask that I don’t think. I was kind of just like, ‘I want this,’ and he was like, ‘Okay.’ I think that’s why it stands out to me. I’ve heard people talk about informed consent and I think he knew that I knew what I was getting myself into.”
At the heart of youths’ talk about access was the centering of embodied knowledge and lived experience of other trans people—including that of providers of healthcare who were also trans—to guide their way(s), to chart a path, to bring forth a future. In this sense, discourses of access were often imbued with incredible generative power, where discourse—which makes it possible to think some thoughts and not others, to move in certain ways and not others—served to alter the status quo and undermine and expose the normative and oppressive ideologies that constrained participants’ passages through systems of care. Discourses of access represented renegotiations of the discursive landscape, where finding, opening, and moving through discursive portals, points of entry, served to expand what is presently possible for trans youth to do and to be.
Discussion
Presently, access to pubertal suppression, and gender-affirming hormones and surgeries are considered primary health interventions for addressing disparate mental health outcomes among trans youth (Tordoff et al., 2022; Weiselberg & Shadianloo, 2019). In order to access these services, youth must first receive a diagnosis of gender dysphoria (Weiselberg & Shadianloo, 2019). While transgender-related diagnostic terms (i.e., gender dysphoria) facilitate access to clinical care and insurance coverage, they can also have a stigmatizing effect and involve negotiating systems of power (Wesp et al., 2019). According to the IRTHJ framework, transgender identities are pathologized by means of this medical diagnosis, which continues to be categorized as a mental health condition and is a function of cisgenderism, or cisnormativity (i.e., a socio-structural process—pathologizing—which is filtered through a structure of domination—cisnormativity).
In this study, discourses of normativity most frequently characterized participants’ accounts of negotiating and presenting themselves to providers when seeking a gender dysphoria diagnosis and in negotiations with parents regarding parental consent. Youth talked about crafting narratives that would differentiate them from gender non-normative young people who might be categorized as masculine girls or feminine boys and who might not be considered appropriate candidates for pubertal suppression and other biomedical interventions. Participants frequently recounted being questioned about being “trans enough” or being “really trans,” feeling that they were required to produce narrative histories that demonstrated a certain level of pain or distress that would be interpreted by providers in alignment with existing diagnostic criteria for gender dysphoria. Latham has shown how “framing treatment practices in this way leaves no room for people for whom ‘gender dysphoria’ (or other experiences of being trans) does not amount to suffering or discomfort” (Latham, 2017a, p. 49) of the kind outlined in both existing diagnostic criteria and throughout much of trans medical literature (Latham, 2019).
Returning to Foucault’s conception of discipline, which is concerned with a kind of control that is internalized by individuals, we theorize normative discourses (i.e., cisnormativity and transnormativity) as kinds of disciplinary pressures that insist youth present themselves in terms that are consistent with existing diagnostic criteria whether or not this accurately represents their lived experiences. Participants reported that they literally felt pressured—by providers, by parents, and by “the system”—to make their experiences intelligible within a normative framework of transgender identity in order to ensure their access to care. Notably, youth commented that this process of self-discipline often produced intensified feelings of embodied distress. Participants talked about doing extensive research in anticipation of their healthcare encounters and talking to other trans people in their attempts to craft believable narratives. They entered into negotiations with discourses of normativity before, during, and after the healthcare encounters in which these discourses presented themselves.
We understand this to be an example of what Foucault means by discipline flowing through individual ways of thinking and behaving, where certain sets of disciplinary procedures coming from outside of individuals ultimately aim to produce discipline of the self by the self. Notably, participants frequently recognized this process operating. They were able to negotiate their healthcare encounters in ways that allowed them to both produce the narratives required and also resist the discourses they encountered—before, during, and after the encounters via which they manifested. Our attention to youths’ agency and to power negotiations in these situations, however, is not meant to minimize the negative impact these encounters may have had on participants. They are likely to have profound and lasting consequences. A study in the UK, for example, found that “20% of [trans survey respondents] had wanted to harm themselves in relation to, or because of involvement with, a Gender Identity Clinic or health service” (McNeil et al., 2012, p. 88). Normative discourses as they operate in patient–provider and adult–youth interpersonal encounters condition youth to choose certain statements out of necessity because they will be more productive in terms of establishing their safety and garnering support for their identities.
Implicit in the narratives that youth talked about producing is the making of the institutionally recognizable subject. Youth were required to make themselves known in particular ways within healthcare settings. At the same time, they were excluded and erased from healthcare systems. Both discourses of normativity and discourses of access highlight the processes by which contemporary trans youth are made intelligible in healthcare contexts and illuminate the processes through which they are erased or excluded from institutional knowledge. The concept of erasure (Bauer et al., 2009; Namaste, 2000) has been reflected in other studies that have explored how trans individuals navigate and engage in healthcare services and represents “a defining condition of how [transgender] is managed in culture and institutions, a condition that ultimately inscribes transgender as impossible” (Namaste, 2000, pp. 4–5). Prior studies have suggested that erasure is why trans individuals are required to navigate healthcare in ways that are different from cisgender individuals (Poteat et al., 2013; Roller et al., 2015). Youth talked about not fitting “the system” and having to learn how to discursively negotiate and navigate it in response. This was both a function of discipline and a renegotiation of power. Many participants consciously entered into discursive negotiations intended to mold or remake the system. Discursively navigating structures of domination as they are filtered through institutional systems took time, energy, and both discursive and material resources, which frequently meant that youth did not receive the services they needed when they needed or wanted them.
Discourses of temporality often framed embodied processes which showed up in youths’ talk about waiting for their bodies to change and in participants’ accounts of how risks and benefits of treatment were framed in conversations with providers. Health service inaccessibility prolonged waiting as did the time that participants spent discursively negotiating access. This is consistent with other studies of waiting in medicalized gender transition, which situate the waiting trans patients must do within a broader biopolitical context of profound inequality (Pitts-Taylor, 2019). Accordingly, structures of domination, institutional systems, and socio-structural processes sort, classify, and administer “the inclusion of some [transgender] bodies and subjectivities, while leaving others abject or illegible” (Pitts-Taylor, 2019, pp. 659–660). Youth and parents talked about the constant and time-consuming negotiation of discursive resources—finding out what to say, who to say it to, presentation of legal documents at court hearings, medical forms to fill out, medical forms to resubmit, and insurance rejections to appeal—which had both temporal and administrative implications. Temporally, these kinds of negotiations required that youth “recalibrate their bodies and psyches to institutional time” (Pitts-Taylor, 2019, p. 657) and were associated with their sense of social recognition—in school settings, for example—or lack thereof. Administratively, these negotiations should be understood as forms of administrative violence at the population level. Spade argues that administrative violence is enacted on trans subjects via overt transphobia as well as through institutional systems and socio-structural processes—such as insurance coding as it functions to operationalize diagnostic criteria (Spade, 2011). Notably, discourses of access had temporal qualities, were framed non-linearly, and were characterized by talk about starts and stops, movement forward and backward, which is consistent with other analyses of how trans patients are made to wait (Pitts-Taylor, 2019). In Figure 2, we map our findings onto the IRTHJ framework and the key Foucauldian concepts we employed in our analysis. This figure also represents one of the key IRTHJ actions for advancing transgender health justice—naming intersecting power relations, which both literally intersect through the body and conjoin various systems of power in the figure. In Figure 3, we further explain the various ways that each of the IRTHJ actions was addressed in this study. Intersectionality research for transgender health justice, discursive pathways, and effects on trans youth. Implementation of Intersectionality research for transgender health justice actions for advancing transgender health justice.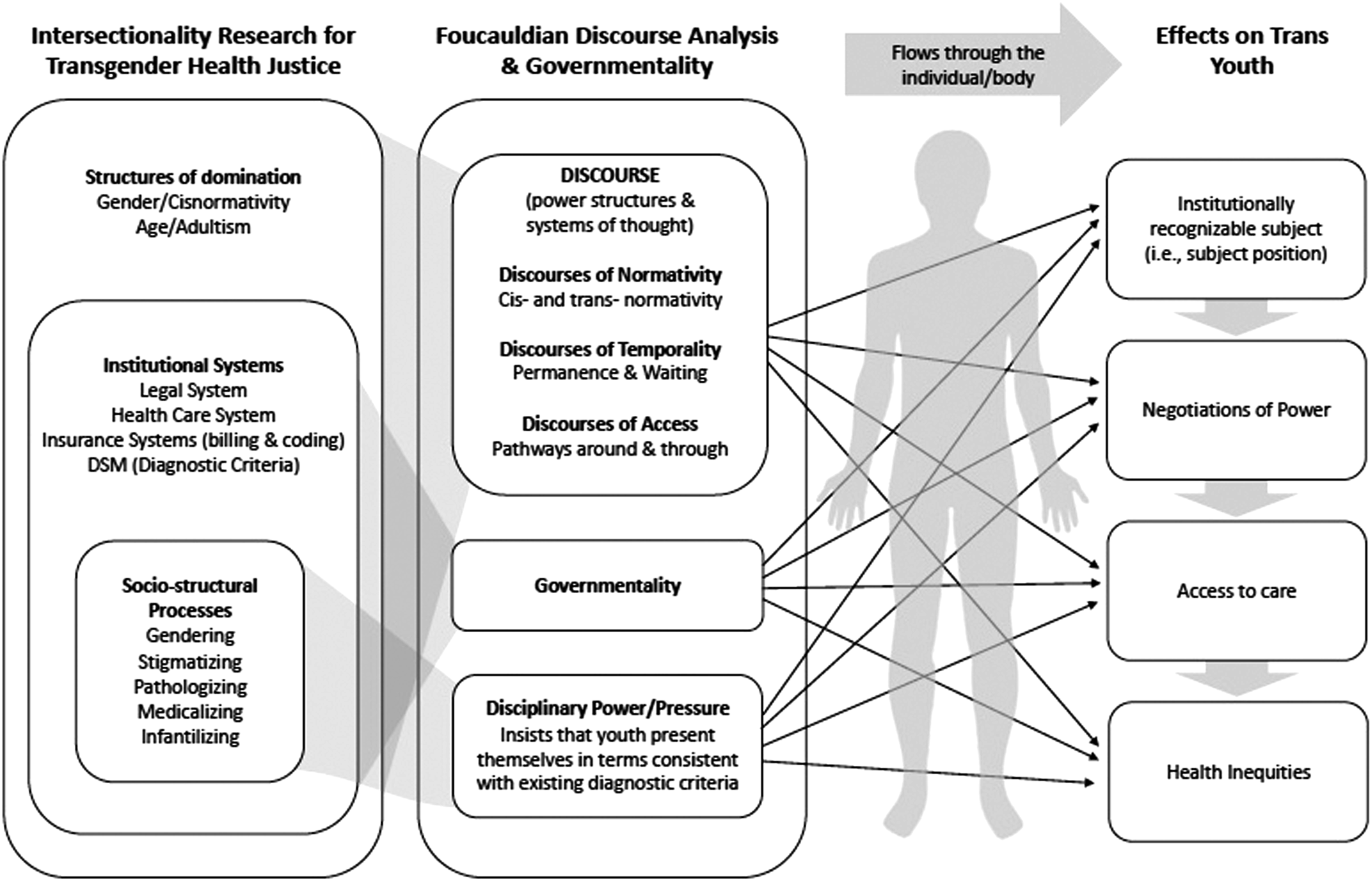

Limitations
Particular limitations must be considered when interpreting our findings. Participants were predominantly white. Thus, these results are not likely to fully address the complex web of power relations that Black, Indigenous, and People of Color (BIPOC) youth encounter when navigating healthcare services, particularly as they relate to white supremacy and colonialism in the making of discourses of normativity as well as the role of structural racism in the production of disparities in access for BIPOC trans youth. Participants represent a cross-section of the varied experiences of trans youth. There is a selection bias in favor of participants who were interested and willing to talk about navigating healthcare, which may not include many trans youth who have reasons to believe they cannot or should not share their stories. At the center of our analysis was a concern with the role of language in the construction of social reality. This was both a strength and limitation of this research. For example, not all youth whose embodied experiences of gender transcend binary categories of boy/man or girl/woman use the word transgender to describe themselves. These youth may be less likely to respond to study recruitment materials seeking transgender participants. While discourse analysts agree that there is a relationship between discourse and material reality, the relationship is a complex one and it is not possible to name all the effects of the discourses we identified in the construction of healthcare for trans youth. We address this limitation of Foucauldian discourse analysis by grounding our analysis in the IRTHJ framework with the goal of demonstrating how relations of power work together to produce transgender health inequities. Lastly, our analysis is limited by our analytic standpoints as researchers. In other words, power relations have influenced our language choices, study design, and analytic and authorship decisions. We acknowledge, in particular, that all analysts for this study were white. Our analysis team was comprised of individuals with varying relationships to the power hierarchies present in research (e.g., doctoral candidate, doctoral student, assistant professor, researcher, research subject) and in most cases, each of us occupied more than one position within these relations of power.
Conclusion
Findings from this study suggest that the trans youth participants we interviewed discursively managed their access to care by both performing normative subjectivities and by resisting them. In other words, participants negotiated with the structures of domination/systems of power they encountered rather than simply submitting to them. This is consistent with the Foucauldian conceptualization of power as a network or web of relations which are distributed throughout society (Foucault, 1978). Rather than simply constraining individuals, power orders and structures certain forms of behavior and brings about certain events. This conceptualization of power both served to cement youths’ instrumentality as active agents negotiating systems of care and reinforced within their accounts of healthcare navigation the understanding that many systems of care are not currently designed to meet their needs. Given the fractured policy landscape in the U.S. today, we suggest that trans youth discursively manage their safety and access to care in ways that are both temporally and geographically specific.
We have named discursively situated and intersecting systems of power that have material effects for how trans youth present themselves and self-censor their experiences in clinical encounters. Frequently, the narratives trans youth produce within clinical encounters are taken as a given rather than responses to the complex ways that power operates via youths’ engagement with adults and healthcare systems. As a result, trans young people’s self-presentation within clinical encounters—and frequently in research about their health and well-being—are decontextualized and interpreted without consideration for how structures of domination/systems of power are enacted within those clinical and research encounters. This results in the production of health inequities for trans minors and the maintenance of the status of the quo.
Central to our analysis was the notion that trans youth are capable of generating expert knowledge about their lives and experiences and that this knowledge is integral to the transformation of issues and institutions that impact their everyday lives. Given the implicit power relations in youth–parent–provider triads and data demonstrating that a significant portion of trans individuals experience explicit rejection from family members as a result of their gender identity (Bradford et al., 2013; Factor & Rothblum, 2007; Graham et al., 2014; Koken et al., 2009), more research is needed to understand how the intersecting power relations/structures of domination related to cisnormativity and trans youths’ status as legal minors impact their abilities to access a wide variety of health services across a diversity of health systems throughout the U.S. today. Such research should include waivers of parental permission that permit the participation of youth under the age of 18, both with and without parental support, as a necessary and fundamental strategy for recognizing youths’ authority of knowledge and for understanding intersectional power dynamics related to age, gender, and other aspects of trans youths’ social identities that impact how they navigate research participation and healthcare systems as legal minors. Additionally, more research is needed to understand the presence of discourses of normativity in existing diagnostic criteria for gender dysphoria, particularly as they are operationalized in clinical practice and insurance billing and coding. Given that the way in which we talk about lived experience and social structures has implications for the ways in which we physically and psychologically experience the world, more research is also needed to elucidate how discourses of normativity are internalized and impact trans young people’s health and well-being, how particular health services are constructed as interventions in response, and how discourses of normativity are taken up in family systems.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Robert Wood Johnson Foundation and University of Washington School of Nursing.