
Abstract
Parkinson’s disease (PD) profoundly impacts the everyday lives and relationships of those affected. This is especially the case when the caregiver is a family member of the person with PD. With disease progression, caregiving needs increase, prompting its description as a family disease. While caregiving is frequently viewed as burdensome, the role of hope remains underexplored. Hope is vital in serious illness; understanding carers’ hope across PD stages is essential. Drawing on ethnographic fieldwork in Danish PD support groups and interviews with 15 relatives, we explore the everyday life of PD relatives, sources of hope, and nuances of care across disease stages. We introduce the notion “evolving care” to illustrate how caregiving tasks, roles, and emotions change over time, requiring ongoing adaptation. Hope, too, was dynamic, assuming multiple forms. Psychotic episodes and dementia marked critical tipping points, where hope faltered and care became precarious. Our findings underscore how hope, deeply rooted in social relationships, offers vital strength but can become fragile when caregiving demands intensify. Furthermore, we show how an attention to hope may reveal to professionals specific situations where help is needed.
Background
“Care evolves,” one of our informants reflected, “from being lovers, spouses it slides into—well almost a parent-type relation.” He had gradually taken over tasks and obligations and now cared for his wife, who has Parkinson’s disease (PD). This article explores care and hope among family carers of persons with PD, one of the fastest growing neurodegenerative disorders worldwide (GBD 2016, 2018). PD is often called a “family disease” (Solimeo, 2009; Tonnesen & Nielsen, 2024) because its gradual, unpredictable progression-marked by tremor, rigidity, slowed movement, balance problems, cognitive challenges, and sometimes psychosis (Pagonabarraga et al., 2024) demands continual adaptation by relatives. The degenerative aspect makes PD different to other more functionally “stable” diseases in the sense that relatives must continuously take on new tasks and roles, learning about new symptoms and generating strategies to cope with the impact of PD. PD has its own way of showing in an individual, as a “designer disease” (Solimeo, 2009) in which no two experiences are the same. Medication, exercises or training, and Deep Brain Stimulation can help ease some symptoms, but PD is a progressive, incurable disease.
As PD relatives gradually take over tasks and responsibilities, intimate and social life may change. Experiences of PD family carers underscore how caring can be a chronic life stressor (Chen et al., 2021). Carers report fear, confusion, helplessness, and grief of losing a loved one; challenges include a heavy burden of care, social limitations, and financial stress (Aamodt et al., 2024; Geerlings et al., 2023). Some receive support, while others feel alone because of a lack of societal understanding about PD (Chen et al., 2021; Walga, 2019), or because they feel they have lost their loved one and the life they had together, intimate life included (Habermann, 2000). Structural aspects influence care; for example, limited general health coverage or a scarcity of affordable access to PD-competent healthcare professionals and PD medications can add to carers’ stress (Fothergill-Misbah et al., 2024; Solimeo, 2009; Walga, 2019). While the research literature tends to accentuate PD caregiving as a burden (Aamodt et al., 2024; Geerlings et al., 2023), studies have shown that although PD does put strains on significant others, caregiving in PD trajectories is complex and bidirectional (Solimeo, 2009; Warren & Sakellariou, 2020), with possible silver linings, that is, an upside to PD trajectories (Alonso-Canovas et al., 2022), such as living more intensely. Reviews have identified a knowledge gap concerning the impact of caregiving at specific disease stages (Hulshoff et al., 2021), particularly in late-stage PD, and an absence of male carer perspectives (Read et al., 2023). This article incorporates data from different disease stages and gives voice to men to ensure a more gender-balanced knowledge.
As hope can help carers deal with the day-to-day challenges of caregiving for people with terminal illness (Revier et al., 2012), it seems relevant to explore the sources of hope among PD relatives. Knowledge of sources of hope can be valuable to support carers. However, the understanding of hope in the context of PD is limited (but see Larsen et al., 2024; Murdoch et al., 2020; Soundy et al., 2014; Tonnesen & Nielsen, 2024; Warren & Addison, 2020). Research has found that persons with PD carry many hopes, beyond medical hope (i.e., hope for cure); hope could be existential, specific and future-directed, individual, or social (Tonnesen & Nielsen, 2024). PD studies exemplify how hope can be worked with explicitly through professional-led interventions (Larsen et al., 2024; Murdoch et al., 2020) or implicitly in practices performed by clinicians with persons with PD (Tonnesen & Nielsen, 2024). Some have suggested that healthcare professionals can help persons with PD draft their own “hopamine” (hope of mine), alongside dopamine therapy, arguing that hope may empower individuals to better manage everyday life with PD (Noordegraaf et al., 2023). Less is known about the role of hope among PD relatives. In fact, we struggled to find literature specifically on PD relatives and hope. We believe it is valuable to explore hope at specific stages of PD to understand how hope develops over time in the context of a neurodegenerative disease. Attending to hope and the opportunities afforded by care can help address an important ethical issue: while informal carers provide the vast majority of care, often bringing underrecognized benefits to health systems, caring may cause harm to their own well-being.
In this article, we aim to explore the everyday life of living with PD as a relative, examining the nuances of care in different stages of the disease and relatives’ experiences of hope and exploring sources of hope. We develop the concept of “evolving care” to illustrate how tasks, roles, and emotions unfold among relatives in a neurodegenerative illness trajectory.
Care and Hope
The title, Relative Care, Relative Hope, carries a double meaning: first, it refers to care and hope among PD relatives. Second, it signifies that care and hope change in intensity and evolve over time and are thus experienced as relative to the stages of the disease progression. We here unfold the notions in the title semantically and theoretically.
Relative is pårørende in Danish. The word på means “on” and rørende means “touching”—so a literal translation would be “touching on.” Etymologically, pårørende comes from pårøre, meaning “to be close” or “to have family ties” (https://sproget.dk). While the term is generally associated with family, pårørende can also include significant others, that is, those with whom the patient shares a deep emotional bond, regardless of biological or legal relationship. In everyday language, pårørende often refers to relatives who assist a family member in need of care, typically due to illness or frailty, though some informants noted they were mostly called pårørende in institutional settings. In this article, we focus on family-related pårørende, that is, spouses.
Care is a complex phenomenon, a multifaceted concept with various and historically shifting definitions (Mol, 2008), encompassing everyday intersubjective practices, engagements with biomedicine, biopolitics, and the responsibilities of the state or family (Buch, 2015). Care engages people at different levels. Politically, Danish patient organizations have appealed for more political focus on relatives as carers, accentuating how insufficient carer support can have socioeconomic consequences due to exhaustion, stress, and reduced workforce participation (DanskePatienter, 2024). On the relational level, care can encompass tenderness and love but also be controlling and distancing (Sand Andersen et al., 2024). Care can refer both to “care for”—the practical actions involved in looking after someone—and to “care about”—the personal and emotional investment in another person (Manderson & Warren, 2013). Care can be seen as an interactive open-ended process that is shaped and reshaped (Mol, 2008), and as necessary for the upholding of a meaningful life (Tronto, 1993). Carers can refer to formal, paid carers to informal, unpaid carers either living apart and helping out now and again or, as our informants, family carers (spouses) who are main carers, living with the person with PD. Our study is set in a welfare state, Denmark, where citizens have free access to healthcare, paid by general taxes, and medical expenses partly covered. Although the welfare state structure provides mechanisms to ease, for instance, the strenuous economic aspects of caregiving, it has been noted how, in a welfare state, the moral and practical responsibilities associated with care can become blurred, for example, between professional and relative responsibilities (Sparre et al., 2024).
In our study, we explore care from the relative’s perspective, viewing care as an everyday intersubjective practice, enmeshed in emotions, obligations, morals, and practicalities. While there are generic aspects to care across illness trajectories, we emphasize the particular way that care evolves out of necessity in the neurodegenerative disease trajectory of PD.
When living with a serious disease such as PD, hope can be an important life force. Like care, hope is a complex phenomenon. Existential philosopher Marcel (1951) argues that hope is an ontological phenomenon that is essential for overcoming the trials of life. Marcel distinguishes between hope as something concrete and future-directed, “to hope that,” and the absolute statement “I hope” (1951, p. 32). In PD, the first aligns with a medical hope, such as the hope of a cure (Graven et al., 2021). The second refers to a dimension of hope with no determinate object. This ontological aspect of hope is received from being in the world and transcends concrete future-directed hopes (Marcel, 1951). The hopeful person relies on hope as a creative force that is to be found in the world with others in spite of illness and death. Ontologically, hope is relational. As Marcel points out: “Hope is only possible on the level of the us” (1951, p. 10). Thus, hope is to be found incarnate in lived experiences with others. Hope cannot take away the suffering that accompanies illness. However, it can take away the meaninglessness of that suffering (Graven & Brødslev Olsen, 2018).
The relational nature of hope points to the importance of exploring hope as closely connected to social life. In this article, we focus on PD as a social matter of which hope is a necessary driver for living a meaningful life, even with the losses that everyday life with PD entails. We emphasize the intersubjective aspect of hope as something that is nurtured, mobilized, shaped, and reshaped in connectedness. However, while hope can be a source of strength and a life force, we acknowledge that hope can become fragile in a disease trajectory such as PD.
Study Design
To explore how relatives of people with PD experience hope and care in everyday life, we conducted an ethnographic study (Desjarlais & Throop, 2011) combining participant observation in support groups with in-depth interviews. Participant observation enabled close attention to the relational, embodied, and temporal aspects of care and hope-aspects not easily accessed through interview data alone.
Three considerations guided our design. First, support group members are involved at different points in the PD trajectory, offering a unique opportunity to experiences of care over time; a longitudinal study was not feasible due to the dynamic nature of support group membership-people join and leave, or participate then withdraw, in response to PD diagnosis, progression, and outcomes. Second, because hope often emerges tacitly-through gestures, tones, and shared atmospheres we sought a method attentive to sensory experience. Drawing on prior hope research and insights that small acts of hope can be revealed through observing interactions (Mattingly, 2010), and that “finding” hope requires active listening and sensitivity to subtle cues of hope (Larsen et al., 2007), we entered the field prepared to listen, observe, and feel for these moments. Third, insights from observations informed the interview guide. Interviews were used to gain more coherent narratives of care and hope.
Methods
Participant observation was conducted for six months in 2024 in three in-person support groups organized by the Danish Parkinson’s Disease Association, attending meetings every fortnight in two groups (six participants each), and once a month in the third group (10–14 participants). This method enabled access to relatives’ experiences over time and supported attention to the intersubjective and temporally informed ways that people engage in the world (Desjarlais & Throop, 2011), when living with PD.
Access was arranged through local association representatives. Noticeably, support groups may not fully represent the broader carer population. Immigrants and carers who were not spouses (e.g., children and friends) were not represented. MT introduced the project to each group, and participation was continuously renegotiated. Group members welcomed the study to “shed light on life with PD.”
Observations focused on how relatives described daily life, responded to one another, the topics they raised, and emotions and dynamics within the group. With an interest in hope, MT attended to gestures, interactions, linguistic cues, and bodily expressions associated with hope, such as observing the visible acts of hope (a smile and a comforting hand on a shoulder), listening attentively to small hope words, that is, the linguistic unfolding of hope (well, I hope he …), and the felt, shared sense of hope that emerged in certain moments. For instance, when a member shared feeling hopeless, others acknowledged this and suggested ways forward—here, MT sensed the shared hope through embodied awareness (Pink, 2009).
Being familiar with PD from previous research, MT sought to bracket prior knowledge to remain open to relatives’ perspectives. In particular, the familiarity with medication, diagnostic processes, disease trajectory, and support structures—or their absence—helped contextualize conversations and may have facilitated access, as participants noted the sustained, yearlong engagement with the PD field.
MT engaged in informal conversations with participants, but positioned as a researcher during meetings, writing fieldnotes, that is, the spoken words and descriptive notes (Emerson et al., 1995) on the room composition and dynamics, gestures, and emotions, signs or words concerning hope. Fieldnotes were reviewed after each session, analytical jottings added. Referred to as “our secretary,” MT was sometimes asked to check fieldnotes on a specific topic.
In the final meeting attended, preliminary findings were shared with participants to acknowledge their contributions and validate interpretations.
Informants and Fieldwork Settings
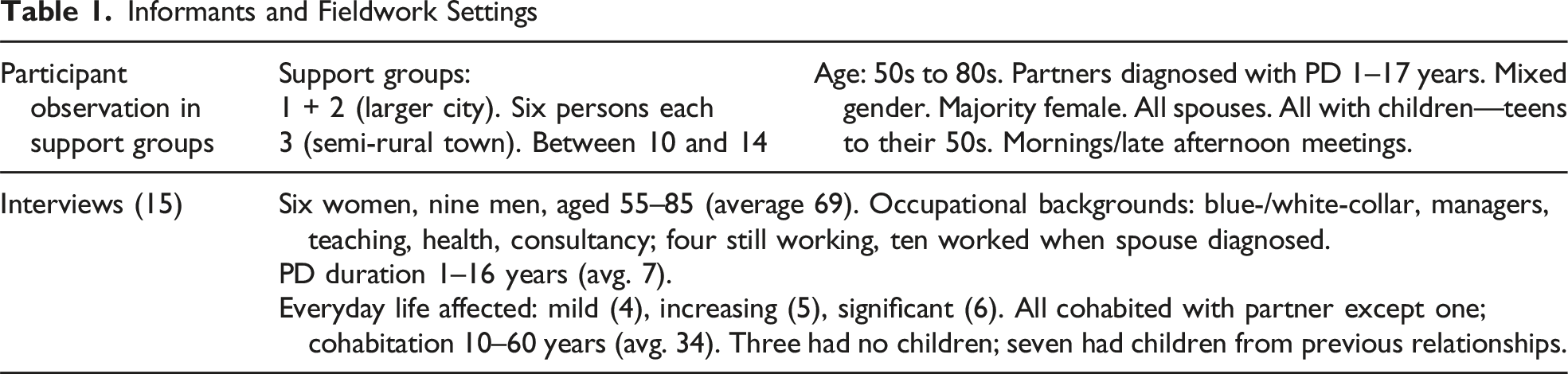
Analysis of Data
The analysis developed in an inductive, iterative process between interview transcription and a continuous reading and interpretation of data and relevant literature (Hammersley & Atkinson, 2007). The empirical material encompassed interview transcripts and fieldnotes. A first round of broad coding was followed by more fine-grained coding to refine categories (Madden, 2010), including themes related to care and hope. Particular attention was paid to vernacular expressions (Jackson, 2012), such as “living with,” variations in PD’s impact over time, and to verbal and embodied expressions of care and hope (Larsen et al., 2007; Mattingly, 2010). Disparities in the material were important markers (Kvale, 1997).
Co-authors critically discussed findings to ensure a reflexive, transparent approach. Three peer groups were also invited to discuss the developing analysis, strengthening the trustworthiness and credibility of the findings.
Vignettes are used to present the results, focusing on narratives of care and hope. Based on observations of 60 PD relatives and 15 interviews, these vignettes offer partial but illustrative examples (Bloom-Christen & Grunow, 2024) that highlight central issues related to care and hope and illuminate emotions that permeated the fieldwork but may otherwise remain tacit. Though only sparsely referring directly to data from participant observation, we have used the data extensively to inform the interview guide and to underpin the central issues and choosing of vignettes. Elsewhere, we elaborate on hope in relation to participation in support groups.
Approval was granted by the Danish Data Protection Agency: reference number 1-16-02-19-24, and conducted in accordance with the American Anthropological Association’s ethical guidelines. Informants received oral and written information and provided written consent to study participation. Pseudonyms are used. ChatGPT was used for language editing of selected paragraphs.
Evolving Care
Living with a neurodegenerative disease means that symptoms evolve over time; as symptoms cannot be readily disentangled from the care needs they prompt, care therefore also evolves over time. In the first two to five years after diagnosis, most informants described their lives as “normal.” However, as Parkinson’s disease symptoms progressed, relatives’ responsibilities and care tasks increased, relationship roles and intimacy changed, as did hope.
In the following, we unfold informants’ reflections on care, hope, and everyday life with PD, illustrated by four vignettes describing evolving care, that is, how care unfolds in different stages of PD, and showing the dynamics of hope, that is, how hope changes with progression of the disease, assuming a multiple and dynamic form. Each vignette exemplifies life as a relative in a particular stage of PD (from mild to severe symptoms) and illustrates four themes from our analysis: navigating the intertwinement of certainty and uncertainty, feelings of loss and trying to control the uncontrollable, care work and change in roles, and tipping point of care and hope.
Navigating the Intertwinement of Certainty and Uncertainty
Uncertainty often accompanies illness trajectories. However, with a neurodegenerative and incurable disease such as PD, uncertainty about the timing and severity of disease progression is intertwined with the certainty that PD will progress. Informants found this intertwinement difficult to navigate: Sonia’s husband, ten years her senior and retired, drinks coffee and listens to the radio in the kitchen during our interview. Closing the door to the kitchen, Sonia shares her thoughts about being a PD relative. While her husband tires easily and has some mobility issues due to Parkinson’s, their daily life remains largely unchanged since diagnosis one year ago. Sonia still works, and they maintain their social life and household roles, though small changes in social interactions are evident: she recalls his shaking hand and trouble finding words at a family event, noting “it affects me when we’re with others.” They try to live in the moment, but small hints of the future, like phrases such as “for now, we’re lucky,” reveal her underlying anxiety. She wipes away a tear when asked what preoccupies her most, “it’s about what the future will bring—the future is so uncertain so I guess that’s what affects me—how will the future be, how long will he live.” With disease progression, she anticipates having to reduce her working hours though she finds her job fulfilling, and perhaps abandoning their shared hobby, “We’ve talked about how long we can continue sailing. But we'll just have to take it one day at a time.” She finds hope in noticing her husband’s relative well-being compared to others with PD, and hopes for a slow PD progression, “that it will be tolerable for as long as possible, that we still experience things together, do some things. Even if it gets more and more difficult.” Recalling how her mother sometimes got mad at her father, living with Alzheimer’s disease, she hopes she will remain kindhearted. Upon leaving, I small-talk with Sonia’s husband, noticing his stiff movements. Outside their home, Sonia looks around the garden and says: “I think we can stay here even when PD gets worse.”
At this stage, PD causes only minor disruptions to everyday life. Sonia and other relatives generally found hope in experiencing that life was livable with PD. However, noticing subtle changes in her husband’s condition prompted Sonia to think about the uncertain future. While Sonia cared about but not yet for her husband, she was acutely aware that this was certain to change over time. For now, care was mostly emotional but drawing on her family’s experiences of caring in another neurodegenerative disease, she knew that later, concrete care tasks would be added. Such awareness makes relatives consider whether their current living situation will remain suitable long-term. As the average age of PD diagnosis in Denmark is 62, many couples face decisions about work, retirement, pensions, and insurance.
Indeed, Sonia referred to PD in collective terms, reflecting the shared impact of the disease. The intersubjectivity of the disease manifests in her using we-terms phrases like “for now, we are lucky,” “when we see the neurologist,” or “we disclosed the diagnosis gradually.” This highlights how, in the beginning of the PD trajectory, decisions like how, when, and to whom to disclose the PD diagnosis, were shared as was the managing of PD. Relatives generally attended neurologist appointments to support their spouses and gain some certainty about symptoms and progression of PD.
Generally, at this stage, relatives hoped that PD progressed in slow-motion, and some expressed a medical hope, a hope for a cure or medication to slow down the disease. Other hopes derived from connectedness to their loved one: still being able to share experiences with their loved one reflects the hope nurtured by Sonia and her husband in their attempt to find ways to continue their shared interest in sailing.
Feelings of Loss and Trying to Control the Uncontrollable
Many informants spoke of the frustration of living with an uncontrollable disease while yearning for some control and the ability to plan. Morten, whose husband was diagnosed with PD in his 50s (about six years ago), finds the unpredictable nature of PD deeply challenging. “You need to make peace with the fact that you cannot control it, you cannot organize and plan your way out of it, because it moves all the time,” Morten says. His husband stopped working three years ago, with Morten attending job and pension related meetings. His husband, physically appearing much older due to tremors, rigidity, and a stiffened expression, remains committed to uphold his training regime rigorously. However, it is the decline in his cognitive skills that concerns Morten; struggling to withhold tears, he says, “I am afraid of losing him.” On a recent vacation, he noticed his husband’s condition had worsened; he could not navigate a familiar town, and lacked his usual curiosity to explore new places. Morten adds that with these cognitive changes, “His world diminishes and so does his energy, mentally … It’s become harder for him to navigate the world.” Their conversations have lost the intensity and depth they used to have, and his husband’s expressed interest in Morten’s wellbeing has waned. They have scaled back their social life to accommodate his husband’s PD symptoms. Morten repeatedly emphasizes his love for his husband and considers reducing his working hours to spend more time together. However, he struggles with never being alone at home and tries not to get too irritated with his husband leaving drawers open or getting confused at the hardware store. He believes the cognitive decline is less visible to others: “it’s a difficult balance; I notice things others don’t, and only share them with my closest friends when my heart gets too heavy.” He feels a sense of hopelessness, as PD is a one-way path with no improvement. While he holds out some hope for medical advances, he is doubtful. Still, he does not feel completely hopeless, “I hope we have many more shared experiences and fulfilling years ahead of us. I hope he will not get dementia.”
At this stage, care involves more practical matters as relatives gradually take on more tasks, adapt routines, and adjust their social lives to PD’s demands while they seek to simultaneously maintain social connections for their own well-being.
Now, Morten, like other relatives, realized that PD increasingly controlled many aspects of everyday life, influencing the temporal dynamics. Midday rests and medication times indexed the days and nights, while symptoms fluctuated unpredictably (between days, within days), making it hard to plan activities. Most were determined to support their spouses in yielding some control of the disease and prolong functioning in everyday life, such as medication, training, and rest.
Several informants mentioned that being there, living closely, physically, and emotionally with someone with PD, enabled them to witness the changes that doctors and others may miss. Morten pointed to cognitive challenges as invisible aspects of PD’s progression, common in later stages of PD and a shared concern among informants. When experienced, cognitive decline evokes a sense of loss as it alters the essence of their loved ones, at times leading to greater self-absorption, and disrupts the relationship’s cohesion and balance. Some even felt a loss of their self and the spouse they wished to be, as their partners’ lack of initiative, slowness, or confusion often triggered anger and frustration in themselves.
One participant listed the tasks her husband used to handle, saying, “Today, I do it all. Our relationship has gone from being balanced to extremely unbalanced … and it just keeps getting worse.” Her husband now relied on her to-do list. “Please cut the lettuce,” she texted him, as preparing a salad had become too complicated. Both she and Morten experienced a premature aging of their partner and even themselves, affecting their social, sex, and working lives.
Like other informants, Morten preferred managing challenges privately to protect their intimate sphere, to preserve dignity and avoid exposing their partner’s PD-related struggles or their own coping difficulties, thus managing not only presentation of self but also mediating presentation of their partner. This is a time of potential loneliness as tasks, decisions, and conversations once shared with their partner subtly change.
As PD symptoms worsen, hope alters as relatives face a future they had hoped to avoid. Hoping to still have many good experiences ahead of them, they now hoped that their partner would not suffer cognitive decline or end up in a nursing home. Most spoke of medical hope in magical or supernatural terms, like this informant, “[the neurologists] don’t talk about a cure of tomorrow, they know what the likelihood is-well that would be a miracle.” Their hopes were nested in training, rest, and available medication as mechanisms that could ensure that PD progressed in slow-motion, thus prolonging functioning in everyday life. One informant said, “I see hope as a force to keep a process going, keeping an optimism that something can change, or you can do something yourself and hope is then a force that keeps the process going.”
Physical training was an example of doing “something yourself.” One informant showed me his wife’s busy training schedule. “Beat PD” was their motto. He believed their efforts significantly improved his wife’s functioning, even a decade after her diagnosis. Others expressed frustration if their partner missed training or didn’t put in enough effort.
Informants described many sources of hope, for instance, attending support groups or faith, that is, an absolute dimension of hope nursed by connectedness to life with others and/or God. One informant said, “As long as we are here, we know that God will be there for us. That’s what hope means to both of us, I believe.” “I believe” marks how hope appears tacit or implicit, rather than explicitly discussed in couples.
Care Work and Change in Roles
When PD became severe, informants talked of care as work, emphasizing how roles shifted in the relationship. Describing their carer role, informants used words associated with support functions, hospitality, or health: secretary, project manager, chauffeur, personal assistant, servant, nurse, Florence Nightingale, and caregiver, as well as double brain (have to think for both of us), or having a parent-like role. Hans’ wife, his childhood sweetheart, was recently diagnosed with PD-related dementia. They are both in their 70s. Care evolves, he explains, “Among relatives, this mental load,
1
completely overwhelms you as relatives must take care of-well, everything. In the beginning, the medication makes it possible to continue your everyday life activities, more or less. You are spouses, lovers, but then it slides into, well, almost a parent-type relation […] it becomes more demanding, right. I have gradually taken over, like planning of appointments, social life-she used to do all the planning.” He sighs, “I am deprived of my freedom.” The interview is online. He turns the camera to show that he drove to their summerhouse for the interview, while someone stays with his wife. He performs the care tasks, “not with pleasure, but out of necessity. But also, with love and care, as it is an obligation we owe each other; I owe my wife a lot and, in that sense, it is no burden at all.” Nevertheless, the love and care can be hard to keep up. While Hans feels they still can have some good time together, he sometimes gets irritated saying things a bit harsh: “that’s a devastating development, both to me and my wife.” He finds it hard, and at times a lonely process, to stay positive and show strength. He does not want to burden their children with his challenges, finding it important to “protect one’s intimate sphere,” and says, “like many men, I don’t have friends I confide in. Maybe that’s a mistake.” He oscillates between hope, “hope links to things close to you [he puts his hand onto his heart], like everyday life. And tomorrow. That we can still share experiences” and hopelessness, “her dementia crushes the hope of having a meaningful, good life, you know, share life.” However, he emphasizes other sources of hope, such as spending time with their children and grandchildren.
At this stage, Hans and other relatives tended to talk about care in terms of work, for example, that being a carer was “a full-time job” with “no free time.” “It’s like being in a prison,” another relative said, “sometimes I wish it would end soon, so I could have peace and freedom. I know it’s selfish to think like that, but I do.” At this stage, the couples share more physical proximity but less experiences and social life. Semantically, the I increasingly replaces the we, as relatives had to take most everyday life decisions, make social arrangements, and care for their spouse. Care interactions could include hygiene, making safety measures to avoid falls, or making sure to be around in social interactions to translate muffled words. Some emphasized that they had to stay fit to continue caring for their spouse.
Hans referred to a mental load but would not call it a burden to care for his wife. Relatives living with similar strains of PD differed in their perception of finding a burden of care appropriate to their situation. They perceived a burden as not-wished-for-but-have-do- activities or “something negative that is enforced onto you.” Many invoked reciprocity; in a marriage you give and take, exemplifying life situations when they had leaned on their partner for support. Now their partner leaned on them. Care was perceived as part of the marital contract, up to a certain point. In support groups, relatives negotiated among them what care entails and who is responsible. Some drew the line at personal care (hygiene) expecting healthcare workers would do that, while to others this was part of the marital contract. Several stressed how caring for their partner affected other caring relations (for instance, grandchildren).
Many informants noted that, while they were not the patients, they lived with PD and its impact. However, like Hans and Morten, they were selective about whom they confided in and faced a delicate balance of when to involve adult children, often seeking to shield them from the challenges experienced.
At this stage, hope shifts to still having small moments of shared experiences or that their partner would die peacefully before having to go to a nursing home. Or other hopes took center stage: for instance, Hans’ concrete hope that children or grandchildren would fare well in life.
Tipping Point of Care, Tipping Point of Hope
Tipping points are the moments where small changes and incidents have accumulated so significantly that a drastic change in the relationship occurs. Tipping points of hope and care are transitional situations-either psychotic episodes (described below) or when cognitive decline impedes sharing new experiences; when the immediate reciprocity of the relationship is no longer present, and caring for seems to absorb and control everyday life to an extent where the relative can not cope emotionally and physically. In such transitions, informants found it difficult to mobilize hope for a life together and contemplate caring for until death. Sarah had, as a nurse, seen “the worst cases of PD” but upon her husband’s diagnosis, she told herself, that she could not know how his PD progression: “We hoped we’d manage-PD should not take control of our life-we would control our life, with a healthy diet and training.” Things turned out differently, though. After more than a decade of living with PD, Sarah’s husband had psychotic episodes which Sarah describes as “living a horror movie that you couldn’t escape. It’s been terrible, he didn’t trust me, thought I had an affair. He has followed me, woken me at night and interrogated me.” These episodes changed her. She has become short-tempered and more emotionally cold, not protecting him when they are with other people, to “let them see just how bad his condition actually is.” Her facial expression shifts from tearful to determined as she says, “I cannot cope with more, so if he gets worse and needs a lot of care, he must go to a nursing home. It’s hard for me to say this, and it’s against my nature. But this has been so tough, and the kids back me up here. I won’t-or rather I cannot [continue to care] it pains me, because I really miss him. For a long time, I thought: I am strong, I will manage. We belong together. But I feel differently now.” She finds that hope has diminished and become difficult to mobilize, “I have no more energy and that takes away hope. The hope that appears in small glimpses becomes less and less. Now I do not think ‘it’s gonna be okay’ because I don’t believe it will.”
Psychotic episodes often mark a tipping point for relative care. Such episodes, involving hallucinations, delusions, mistrust, and treatment in psychiatric wards, could even require police involvement. Care became a matter of personal security. In narratives, the tone shifted and became harder, and relatives lost hope in coping with the situation and felt their personal boundaries had been overstepped. At this point, they needed help from someone knowledgeable about PD psychosis but were unable to get the support needed. Children got involved, though not straight away, as informants found their spouses’ acts unrecognizable and also shameful. In several instances, relatives phoned their children during episodes to bear witness to the psychotic episodes. David, whose wife was in a nursing home, kept a phone recording to show their children her psychotic behavior. When the psychiatric ward insisted on discharging her, he simply left the meeting, “adamant that I could not cope with it.” Visiting daily, he changed her diapers. The staff encouraged him to call them, but he found them understaffed, and besides, that was the only way he could be close to her.
When PD symptoms are severe, care concerns tenderness and love, enacted through small acts of affection like David bringing his wife flowers each week. However, care also contains anger, irritability, and the basics of human life-taking safety measures and being hyper vigilant to avoid falls, or serving easy to swallow, nutritious food.
In later stages, formal care sometimes supplemented informal caregiving, offering relief but also posing challenges, as relatives had to coordinate with external care and no longer had the home to themselves. For many couples, a nursing home was taboo, symbolizing both failure in spousal care and fear of inadequate institutional care. In support groups, relatives shared experiences from spouses’ temporary stays in nursing homes, at hospitals, or in psychiatric wards, including poor medication management and limited PD knowledge among staff. Some persons with PD specifically asked not to be sent to a nursing home or refused to consider it. Up to a point, relatives strove to keep their spouse at home. However, with psychotic episodes and dementia, something tipped. As in Sarah’s and David’s cases, nursing home care could be a source of relief. At this stage, relatives expressed exhaustion, with hope materializing mostly in small glimpses. Hope is now difficult to find and nurture through the relationship and the risk of despair understood as increased disconnectedness from a meaningful life together is threatening.
Summary: Evolving Care, Dynamic Hope
Our analysis illuminates how care is evolving and hope is dynamic among family carers (spouses), and how care and hope appear relative to the PD progression. While many informants stressed that there is more to everyday life than PD, as the neurodegeneration became severe, PD tended to be all-encompassing to everyday life. Relatives cared about their loved ones, but as PD progressed, they also increasingly cared for their loved one, care tasks increasing and roles changing, as illustrated in Figure 1. Evolving care—family carer tasks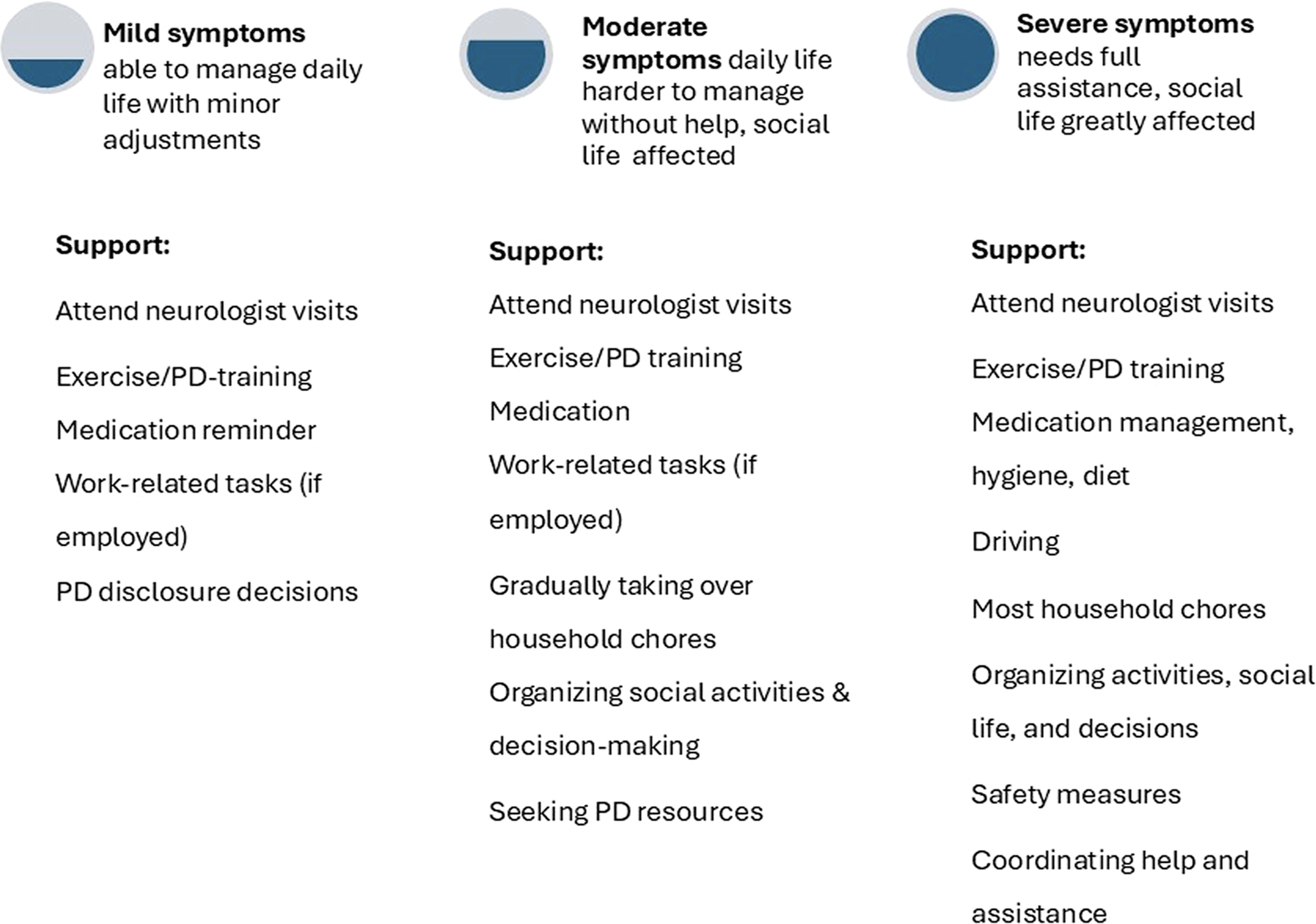
Across stages, living with PD was often overwhelming. While most found support in family, friends, other PD relatives, or professionals, some felt a lack of support in their caregiving. Few readily identified any potential silver linings (Alonso-Canovas et al., 2022.). However, some felt that PD had brought them closer to their partner, family, or friends, while others emphasized the friendships formed within the PD community.
Hope was important to informants, as indicated by Hans, putting his hand to his heart when talking about hope. Hope was also dynamic, as informants’ concrete and future-oriented hopes seemed relative to the stages of the disease (see Figure 2). Dynamic hope
In the beginning of the PD trajectory, relatives had hope that training, rest, and medication could help functioning and postpone degeneration. As the disease progressed, hope seemed to evolve; hope could involve a peaceful death at home. As emphasized by Marcel (1951), hope is rooted in and nurtured through our social being and engagement. The findings indicate the overwhelming care tasks and changed personalities challenge the sources of hope that used to be nurtured by a loving and meaningful relationship.
Discussion
We have explored the everyday life of PD relatives by examining the nuances of care in different stages of PD and exploring the development of hope and sources of hope. Our title, “Relative Hope, Relative Care,” reflects our finding that hope and care appear relative to the stages of the disease progression, both changing in intensity and evolving over time as experienced by family carers living with PD as a spouse.
We have shown how PD creates a domino effect, gradually and profoundly impacting nearly all aspects of life. While studies often emphasize the uncertainty that permeates life with PD, we emphasize the intertwining certainty: the disease will progress though it varies between individuals exactly how. We argue that this intertwinement is vital to understanding informants’ temporal agency, as PD affects the present and also imaginings of the future. As a result, relatives accentuate living in the moment, continuing to share experiences, and taking measures to secure the future.
We introduce the notion, evolving care, to emphasize the particularity of PD care, where tasks, roles, and emotions evolve throughout the progression of the neurodegenerative disease, necessitating PD relatives to continuously revise, refine, and redefine their care efforts. Evolving care means noticing the signs of progression to be one step ahead, continuously adapting the rhythm of everyday life to the requirements of the disease, and taking on new roles as the disease progresses (or resign from one’s working role). We found that care evolves from emotional support and caring about in the beginning of the PD trajectory, to increasingly taking over tasks, to caring for and attending to basic needs of one’s loved one as symptoms get severe. Care then manifests physically and becomes care work.
The concept of care as work, noted in previous PD and chronic disease research (Lennaerts-Kats et al., 2020; Mattingly et al., 2011; Solimeo, 2009; Warren & Manderson, 2016), raises the question of whether care is a burden, emphasized in much PD research (e.g., Geerlings et al., 2023). While some informants viewed care as burdensome, especially in the later stages of PD, most considered care a part of the marital contract, inherent to the reciprocity of marriage. If immediate reciprocity diminished due to cognitive decline, informants relied on what we may call temporal reciprocity, that is, reciprocity grounded in past experiences of care and support from their partner. Simultaneously, a couple’s history also became a symbol of loss of control over daily life and their imagined future, if the partner changed personality, with whom shared experiences could hardly be created.
Tracking care through the stages of PD, we observed how the progression of symptoms affected the sense of togetherness in relationships. While informants still performed care tasks that maintained a sense of “we,” they shared less of their intimate lives and decision-making. This shift was evident language wise, as informants used “I” rather than “we” to describe decisions and concerns. In contrast, Bolland et al. (2015) found that PD carers often used collective terms, feeling so enmeshed in a shared “we” that they questioned if there was room for “me.” To some extent aligning with our findings, we observed, however, a more pronounced shift away from collective terms as PD advanced and reciprocity in the relationship weakened.
Our study highlights the critical tipping points in caregiving, transitional moments when informants struggled to sustain hope for a shared future and faced challenges in contemplating care until death. These tipping points occurred when loved ones became unrecognizable, the intimacy and reciprocity of the relationship eroded, and relatives’ resources were exhausted. At this stage, external help became necessary. Care demands in the latter stages of PD are complex, requiring healthcare coordination (Kalampokini et al., 2022). Informants felt unprepared for the forcefulness of psychosis or dementia and often struggled to navigate the welfare system for timely support. This highlights the clinical need to providing assistance to prevent relatives from feeling stranded and shows that questions about hope can indicate to professionals where help is needed.
Our findings align with Deutsch et al.(2021); delusional psychosis disrupts trust, intimacy, and even love in relationships. However, unlike Deutsch’s findings, our informants eventually involved adult children for support, for safety, and as witnesses to the situation.
PD has been referred to as a family disease (Solimeo, 2009; Tonnesen & Nielsen, 2024), which seems relevant to explore, in light of our findings. We found that spouses “lived with” PD in much the same way as the person whose body inhabits PD, as the disease with time affected most spheres and rhythms of life (see also Sakellariou et al., 2021). Informants used an emic term being there to describe how especially cognitive changes could be invisible to those not living with the disease. Living closely alongside their spouse with PD meant that those changes were felt by family carers, which can be seen through microlevel impacts such as the shrinking social worlds, eating a softer diet necessitated by increased swallowing difficulties, the modifications to the interior of their home to mitigate gait instability, or the ongoing vigilance of another’s body.
Most preferred to preserve the couple’s intimacy and avoid burdening their children. However, some had teenagers who were there, while adult children tended to engage during key transitions: diagnosis, psychosis, dementia, or moves to nursing homes. Gendered caregiving was not prominent, which may reflect sample characteristics and the cultural norms of Danish society which emphasizes gender equality and caregiving as a marital obligation; few Danes live in extended households where other women assume primary care roles. Both men and women undertook household and social tasks, assisted with hygiene, and found ways to adapt to declining functioning. Women tended to confide in close friends; men kept hardship more to themselves, a finding that warrants further investigation in future research. Importantly, care can be fragile when individuals live in relational vulnerability with few or no relatives to rely on for care. Who, then, is responsible for care provision? Expectations of who cares, how, and why varied, but generally expressed as both a marital and societal obligation, with greater reluctance to involve, for example, children.
Most informants spoke about hope as a necessity for life. We highlight the dynamic of hope, understanding dynamic as transformable, shifting, and as a creative force that potentially stimulates progress, and inspired by an informant who defined hope as a force to keep a process going. The dynamic of hope shows in different ways. First, in its concrete and future-directed mode, we found that the intensity and content of hope shifted over time. Hope had a temporal dimension and was relative to stages of the disease. Second, hope appeared multiple, assuming several modes and dimensions in a person and between persons (see also Dufault & Martocchio, 1985). Interviews revealed a wide range of hopes, also beyond the PD context. Third, we found a dynamic in the intersubjective aspect of hope as hope can be nurtured, mobilized, shaped, and reshaped in togetherness (see also Mattingly, 2010). This dynamic was evident in interview accounts and through observations where attention to sensory interactions revealed how a light touch on the shoulder or a shared laugh could communicate “you are not alone,” offering hope in situations that might seem hopeless.
Early in PD, phrases like “our hope” reflected a sense of shared hope in couples. As communication and cognition declined, hope shifted and evolved through interactions with, for example, family and peers. Our results echo Duggleby et al.’s (2010) review, highlighting hope as transitional, situational, and temporal—where some hopes are lost, and new ones emerge, creating a continuum of hope. Informants exemplified how hope could be mobilized in different ways—by making the most of everyday life and continue to create and share new experiences, or through social connections with loved ones and the PD community.
Sources of hope included proactive steps to slow degeneration (medication, training, and a healthy diet), promising medical trials, a slow disease progression, or others coping well with PD, as well as meaningful aspects of life that were considered life-affirming: children, grandchildren, PD relatives “in the same boat,” belief in God, and continuing to create new shared experiences. With serious cognitive decline, sources of hope included fleeting glimpses of the person they once knew. Hope was a source of strength and a life force but could be fragile. Barriers to hope included the loss of the person once so familiar due to dementia and psychosis and limited access to professional help and guidance.
Informants explained that knowing PD is a one-way path with no improvement could lead to hopelessness. However, rather than equating hopeless with “all hope is over,” it may be conducive to notice the less in hopeless. Because hope is dynamic, and informants thus had several hopes to draw on, feeling hopeless regarding PD did not necessarily mean feeling hopeless in all life matters. Furthermore, in the beginning of the trajectory, the uncertainty of the disease progression did yield some hope of a slow and manageable progress. Thus, hope can reside in uncertainty.
Our findings on evolving care, dynamic hope, and tipping points of hope (psychotic episodes and dementia) may be relevant in other geographical contexts and resonate across neurodegenerative trajectories beyond PD, though the possibilities for, for example, formal care and access to neurologist will differ according to setting.
Our study design enabled us to gain unique insights into how care and hope evolve over time in life with PD. However, revisits to the support groups while finalizing this article made it evident that longitudinal studies would be conducive for knowledge on hope and care evolvement over time in individual trajectories. Attending to senses and the reflective interaction between the participants exposed the intersubjective aspect of hope as something that is nurtured in connectedness. Perspectives from relatives living apart could have expanded the scope of our findings and remain an important topic for future research, given the limited knowledge about individuals with PD who live alone. Another topic for further exploration concerns the interplay of informal and formal care, and the care tasks performed by formal carers. Our informants had diverse backgrounds, but may represent a select group of relatives choosing to participate in support groups.
In conclusion, our study highlights the evolving nature of care and hope in PD caregiving, appearing relative to the stages of the disease progression, as hope and care change in intensity and evolve over time. Hope, deeply rooted in social relationships, serves as a vital source of strength for relatives. Knowing sources of hope can be valuable to support carers.
Hope becomes fragile during critical moments like psychotic episodes and dementia. Support is crucial during these tipping points. We find care intersubjective and relational, and emphasize a need to acknowledge and support the care work of relatives, paying attention to individuals living in relational vulnerability.
Footnotes
Acknowledgements
We thank all informants for sharing their reflections on hope and care.
Ethical Considerations
The project was approved by the Danish Data Protection Agency (reference number: 1-16-02-19-24).
Consent to Participate
All participants gave informed consent.
Author Contributions
All authors contributed to the project idea. MT conducted the fieldwork and analyzed the data, with inputs from VG and NW. All authors reviewed the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was funded by the Danish Parkinson’s Disease Association, grant number: R63-A1581.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.