
Abstract
Background
Hand dominance significantly influences motor skills, with the dominant hand excelling due to better neurological control. Limited knowledge of the non-dominant hand's role highlights the need for on its functional contributions.
Objective
This study aims to evaluate how effectively non-dominant hand performance can predict dominant hand performance in healthy individuals using the Jebsen-Taylor Hand Function Test (JTHFT), offering valuable implications for vocational assessment, rehabilitation planning, and return-to-work (RTW) decision-making.
Methods
This cross-sectional study included 307 healthy adults aged 18–65. Hand performance was evaluated using six JTHFT subtests, excluding sentence writing. Task completion times were recorded in seconds. Paired sample t-tests compared dominant and non-dominant hand performances, while multiple linear regression analyses assessed the predictive value of non-dominant hand performance.
Results
Regression analysis revealed that non-dominant hand performance was a significant predictor of dominant hand performance across all subtests (p < 0.001). Strong predictive relationships were identified in gross motor tasks, such as lifting large light objects (adjusted R2 = 0.642) and heavy objects (adjusted R2 = 0.674). Adjusted R2 ranged from 0.268 (feeding) to 0.681 (lifting heavy objects). Non-dominant hand performance significantly predicted dominant hand performance across all subtests (β = 0.51–0.82; p < 0.001). Age, sex, and handedness showed task-specific effects, but non-dominant hand performance remained the strongest predictor.
Conclusions
The study highlights that non-dominant hand performance significantly predicts dominant hand performance across JTHFT tasks, particularly in gross motor activities requiring strength and coordination. These findings underscore the importance of evaluating non-dominant hand function in occupational assessments and return-to-work programs.
Keywords
Introduction
Hand dominance plays an important role in shaping motor skills, functional performance, and the ability to perform daily living activities. While the dominant hand generally exhibits better motor performance than the non-dominant hand, these differences may be due to both neurological and developmental factors. Research consistently shows that fine motor tasks are often completed more than 10% faster with the dominant hand, highlighting the superior efficiency of the dominant hand over the non-dominant hand.1,2 The development of handedness and its impact on motor skills result from a blend of biological, environmental, and experiential factors. The development of handedness and motor performance is strongly influenced by early sensory-motor experiences and practice-based learning, which are further refined through proprioceptive processes that support consistent and specialized hand use over time.3,4 Moreover, differences in motor execution between the dominant and non-dominant hands are closely tied to cerebral asymmetries. The left hemisphere, which primarily governs right-hand movements, is linked to superior motor control, especially in tasks that demand precision and skilled tool manipulation.5,6 Additionally, pronounced hand dominance, driven by cerebral asymmetries, can impact the recovery of fine motor skills after motor cortex injuries. Individuals with stronger hand preferences may encounter greater difficulties in regaining these skills due to the lateralized nature of motor control. 7 Hand dominance significantly affects functional activities such as writing, eating, and using tools. Tasks performed with the dominant hand benefit from refined motor control and well-established neural pathways, leading to greater efficiency. In contrast, less practiced non-dominant hand skills can create disparities in functional independence. 8
The Jebsen-Taylor Hand Function Test (JTHFT) is a standardized and widely recognized tool for assessing hand function through tasks designed to mimic activities of daily living (ADLs). It is especially useful in clinical settings to evaluate unilateral hand performance and monitor changes in motor skills caused by conditions such as rheumatoid arthritis or post-surgical recovery. Although the JTHFT shows strong test-retest reliability, its ability to directly correlate with patient-reported outcomes related to ADLs is somewhat limited. 9 The JTHFT includes seven subtests designed to replicate activities of daily living, offering a comprehensive assessment of hand function. These tasks involve writing a sentence, turning cards, lifting small objects, simulated feeding, stacking checkers, and lifting both large light and heavy cans. 10 Research has demonstrated that the JTHFT is sensitive to changes in hand function over time, making it a valuable tool for tracking recovery in patients undergoing rehabilitation following hand injuries or surgeries. 11 The JTHFT has been extensively evaluated for validity and sensitivity across various clinical contexts. Notably, it shows strong correlations with other hand function measures, such as the Michigan Hand Outcomes Questionnaire, further establishing its value as a reliable and comprehensive assessment tool. 12 The JTHFT is an essential tool for occupational therapists and rehabilitation specialists, enabling the evaluation of hand performance over time to guide strategies that promote functional independence in daily activities. 13
Beyond its general clinical use, the JTHFT is also frequently employed in work rehabilitation settings to determine an individual's readiness to return to work after hand injuries or upper-extremity impairments. Because its subtests simulate many manual tasks encountered in occupational roles—such as grasping, lifting, and manipulating objects—the JTHFT provides objective, task-based performance data to help clinicians assess work capacity and identify functional limitations relevant to specific job demands.9,14 Studies have shown that improvements in JTHFT scores are associated with enhanced ability to resume occupational activities, especially in physically demanding or dexterity-reliant professions.15,16 Therefore, the JTHFT is recognized not only as a clinical tool but also as a valuable instrument in vocational evaluations, helping guide return-to-work decisions and supporting the design of individualized rehabilitation programs aimed at restoring work-related hand functions.
Although widely used, the JTHFT has shown variability in its predictive value across different populations. In particular, previous studies have reported weak correlations with other established hand function measures, such as the Michigan Hand Outcomes Questionnaire.14,17 While Harte et al. 14 focused primarily on improving test setup accuracy and efficiency, they also highlighted the ongoing concerns in the literature regarding the reliability of JTHFT as a stand-alone assessment tool. These findings underscore the need for further research to validate its clinimetric properties comprehensively. Recognizing the functional differences between the dominant and non-dominant hands has become a key focus in rehabilitation. This approach not only underscores the unique strengths and limitations of each hand but also highlights their interdependence in daily activities. By understanding these dynamics, clinicians can create personalized interventions to enhance bilateral coordination and support optimal functional recovery. 10
Research indicates that grip strength in the non-dominant hand, although typically weaker than the dominant hand, is a reliable marker of overall motor function and coordination. Studies have found that non-dominant hand performance correlates with daily activities and reflects broader functional capacity, especially in aging populations and individuals with neurological impairments.18,19 Occupational therapy prioritizes addressing functional disparities between the dominant and non-dominant hands to enhance bilateral coordination and refine fine motor skills. By targeting the performance of the non-dominant hand, therapists can create interventions that promote greater independence in daily activities and support optimal functional recovery. 20 Differences in grip strength between the dominant and non-dominant hands serve as valuable indicators of motor ability and functional capacity. Research consistently demonstrates that in right-hand-preferent individuals, the dominant hand typically exhibits around 10% greater grip strength, whereas this disparity is less evident or absent in left-hand-preferent individuals. These variations underscore the need to account for hand dominance in both clinical evaluations and research studies of motor abilities.21,22 While the dominant hand typically exhibits greater grip strength compared to the non-dominant hand, this disparity is influenced by factors such as handedness, injury adaptation, and individualized training. Notably, studies indicate that left-handed individuals or those undergoing rehabilitation may exhibit equal or superior performance in their non-dominant hand, highlighting the importance of addressing both hands during functional recovery. These insights are critical in rehabilitation settings to optimize patient independence and recovery outcomes.23,24 Variability in hand performance highlights the importance of personalized assessment strategies that account for individual differences in handedness and motor dynamics. While existing research primarily focuses on clinical populations, such as individuals with neurological conditions, further studies are needed to explore how targeted training for the non-dominant hand could improve functional outcomes and occupational performance in healthy individuals. Moreover, while much of the existing research on hand function has concentrated on clinical populations (e.g., patients with neurological conditions), further studies are needed to determine whether targeted training of the non-dominant hand in healthy individuals could improve functional outcomes and even enhance work-related performance. 25 In addition, age, gender, and the demands of specific occupational tasks play a significant role in shaping non-dominant hand performance, yet their combined effects remain largely unexplored. Research into these factors could offer valuable insights for developing therapeutic interventions aimed at enhancing hand function and promoting balanced motor performance. 26 Bridging these gaps could provide a more comprehensive understanding of motor skills and their practical applications in occupational therapy.
Investigating the interplay between the dominant and non-dominant hand could help fill these gaps in knowledge while also guiding more individualized assessment approaches in rehabilitation. In workplace settings, functional hand performance is critically linked to an individual's capacity to meet job demands—especially in roles requiring bilateral manual dexterity, grip strength, and fine coordination. Understanding the predictive relationship between a person's non-dominant and dominant hand performance can assist occupational therapists, ergonomists, and rehabilitation specialists in evaluating job readiness, designing targeted interventions, and making informed return-to-work decisions following hand injuries or upper-extremity impairments. 5
This study aimed to determine the extent to which non-dominant hand performance predicts dominant hand performance in healthy individuals using the JTHFT. We hypothesized that non-dominant hand performance scores on the JTHFT would significantly predict dominant hand performance in healthy adults, even after controlling for age, sex, and handedness.
Methods
Study design
The study was conducted in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines and employed a cross-sectional research design. All assessments took place at the Cankiri Karatekin University Occupational Therapy Department and the Hacettepe University Occupational Therapy Department between October 2024 and November 2024.
Ethical approval for this study was obtained from the Cankiri Karatekin University Ethics Committee (Approval No: e6ce9251ed7b44c1). Prior to data collection, all participants provided written informed consent in accordance with ethical guidelines.
Participants
The study included healthy individuals who met the eligibility criteria of being between 18 and 65 years of age and free from any neurological, orthopedic, or systemic conditions that could impair hand function. Hand dominance was evaluated using a modified version of the Edinburgh Handedness Questionnaire. 27 To reduce the potential influence of lateralization, only participants with a laterality score exceeding 80% (indicating strong right-handedness) were selected for inclusion. 28 After applying the inclusion and exclusion criteria, a total of 307 healthy participants (181 females and 126 males) were included in the study, with a mean age of 37.69 years (SD = 9.43, range: 20–56 years). Among the participants, 90.9% (n = 279) were right-hand dominant, and 9.1% (n = 28) were left-hand dominant.
Procedures and outcome measure
Participants completed the subtests of the JTHFT, which included simulated page turning, lifting small objects, simulated feeding, stacking checkers, lifting large light objects, and lifting large heavy objects with both the dominant and non-dominant hands, with the exception of the sentence-writing task. 29 All assessments were administered by an occupational therapist and a physiotherapist, both with clinical and research experience with the JTHFT. To ensure familiarization, participants were provided with one practice trial for each subtest. The subtests were first performed with the dominant hand, followed by the non-dominant hand, with a rest period after the completion of each subtest. Task completion times were recorded in seconds, accurate to two decimal places, and noted on the score sheet. A total score for both the dominant and non-dominant hands was calculated by summing the individual scores from each subtest. The entire JTHFT procedure took approximately 10 min to complete and was conducted under consistent conditions for all participants, without inducing fatigue or pain.
The JTHFT, developed in 1969, is a standardized tool designed to evaluate hand function and measure the efficacy of treatments in patients with hand injuries. 30 The JTHFT assesses a wide range of unimanual hand functions required for daily activities and has been validated for use in individuals with various hand disabilities, including rheumatoid arthritis, osteoarthritis, stroke, spinal cord injury, and traumatic brain injury.9,15,16,31–34 The test consists of seven subtests: writing, turning over cards, picking up small (pennies, paper clips, and bottle caps), simulated feeding, stacking checkers, and picking up large light and heavy objects. These subtests focus on manual dexterity essential for everyday tasks and are timed, with longer completion times indicating reduced hand function. The tasks are performed using standardized procedures and verbal instructions. Each task is measured in seconds using a stopwatch, ensuring consistency and accuracy in evaluating hand function. 9
Statistical analysis
Descriptive statistics, including mean, standard deviation, and minimum-maximum values, were calculated for both dominant and non-dominant hand performances across all functional tests. Normality of the data was assessed using the Shapiro-Wilk test to confirm that the data met the assumption of normal distribution. Following this, comparisons between the dominant and non-dominant hand performances were made using paired sample t-tests to evaluate performance differences. All statistical analyses were performed using SPSS (version 27.0) for MacOS. In addition to the statistical comparisons, regression analyses were conducted using Python, leveraging the Matplotlib and Seaborn libraries for visualization, as well as Statsmodels for conducting the linear regression analyses. Matplotlib and Seaborn were used to generate scatterplots that illustrated the relationship between non-dominant and dominant hand performances, displaying regression lines and R-squared values. The Statsmodels library was employed to compute regression coefficients, confidence intervals, R-squared values, and p-values for each functional test. Furthermore, for each subtest, multiple linear regression models were constructed to evaluate the predictive value of non-dominant hand performance, controlling for age, sex, and handedness. Standardized regression coefficients (β), 95% confidence intervals, standard errors, F values, adjusted R2 values, and significance levels were reported to provide a comprehensive understanding of the model outputs. Python was specifically utilized to supplement SPSS by enabling more flexible regression modeling and enhanced data visualization. The scatterplots produced allowed for a clearer depiction of predictive relationships, supporting the interpretation of statistical outcomes.
Results
The results of the JTHFT revealed notable differences in the performance of dominant and non-dominant hands, particularly in tasks requiring fine motor skills. The dominant hand consistently outperformed the non-dominant hand in stacking checkers (2.28 ± 0.74 vs. 2.42 ± 0.71 s, ND/D ratio: 1.09 ± 0.26, p < 0.001), simulated page turning (4.39 ± 1.27 vs. 4.61 ± 1.24 s, ND/D ratio: 1.08 ± 0.29, p < 0.001), lifting small objects (4.82 ± 1.14 vs. 5.21 ± 1.31 s, ND/D ratio: 1.09 ± 0.17, p < 0.001), and simulated feeding (8.02 ± 1.96 vs. 10.65 ± 4.16 s, ND/D ratio: 1.34 ± 0.45, p < 0.001). Conversely, tasks involving larger objects showed less pronounced differences. For example, lifting large light objects showed a small but statistically significant disparity (3.40 ± 0.81 vs. 3.48 ± 0.77 s, ND/D ratio: 1.04 ± 0.15, p = 0.008), while no significant difference was observed in lifting large heavy objects (3.63 ± 0.77 vs. 3.67 ± 0.79 s, ND/D ratio: 1.02 ± 0.13, p = 0.252). These findings underscore the dominant hand's superiority in precision and fine motor tasks, with comparable performance in gross motor activities requiring strength (Table 1).
Descriptive statistics (n = 307).
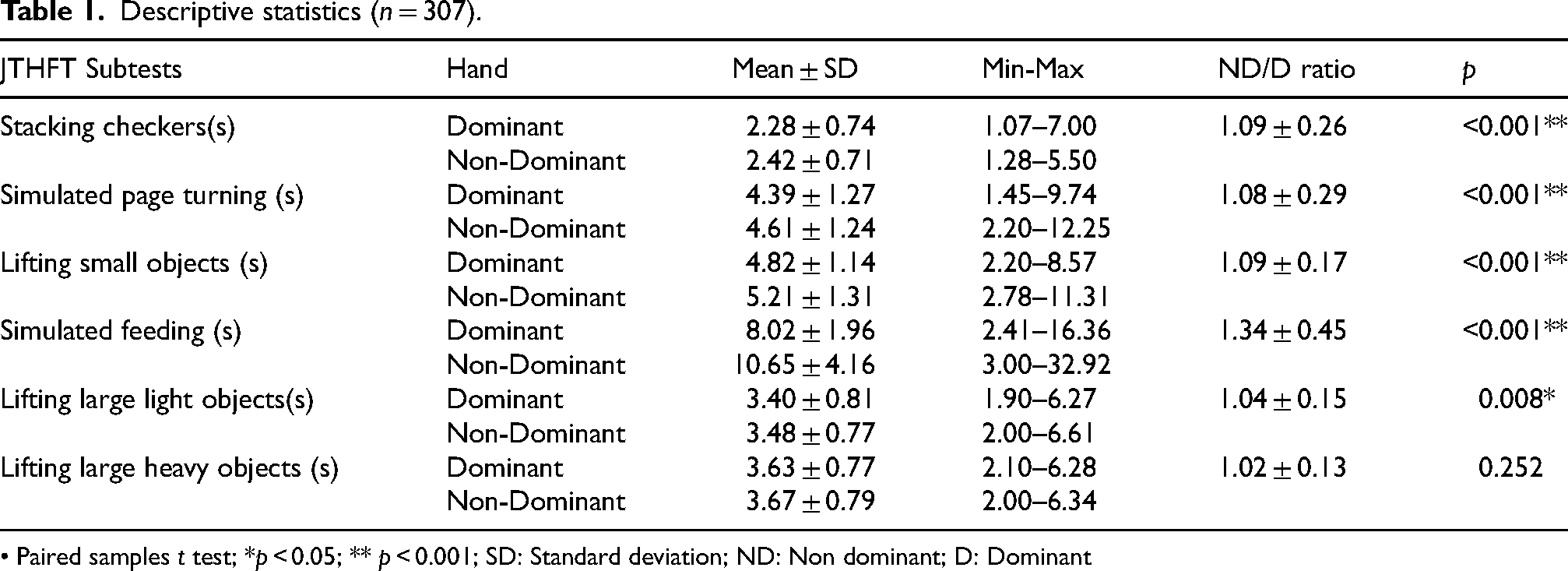
• Paired samples t test; *p < 0.05; ** p < 0.001; SD: Standard deviation; ND: Non dominant; D: Dominant
As shown in Table 2, non-dominant hand performance was a significant positive predictor of dominant hand performance across all six JTHFT subtests (standardized β ranging approximately from 0.51 in the simulated feeding task to 0.82 in the large heavy object task; all p < 0.001). In each regression model, better non-dominant hand performance was strongly associated with better dominant hand performance on the same task. This predictor consistently had the largest standardized coefficient among the variables, underscoring its dominant influence. The models explained a substantial portion of variance in dominant hand performance, with adjusted R2 values ranging from about 0.27 to ∼0.68 across the tasks. The highest explanatory power was observed for the lifting large heavy objects subtest (adjusted R2 on the order of 0.5 or above), while the simulated feeding subtest showed the lowest adjusted R2 (∼0.27). Other factors demonstrated significant effects in specific subtests (p < 0.05).
Multiple regression analysis of dominant hand performance predicted by non-dominant hand performance, age, sex, and handedness across JTHFT subtests.
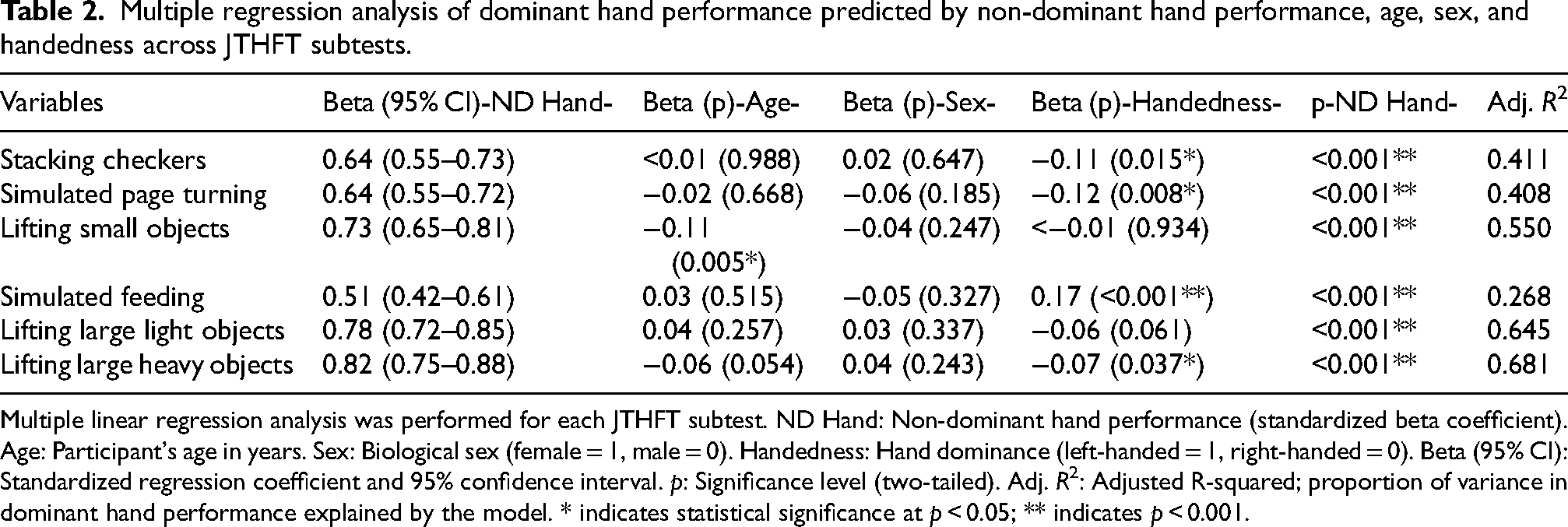
Multiple linear regression analysis was performed for each JTHFT subtest. ND Hand: Non-dominant hand performance (standardized beta coefficient). Age: Participant's age in years. Sex: Biological sex (female = 1, male = 0). Handedness: Hand dominance (left-handed = 1, right-handed = 0). Beta (95% CI): Standardized regression coefficient and 95% confidence interval. p: Significance level (two-tailed). Adj. R2: Adjusted R-squared; proportion of variance in dominant hand performance explained by the model. * indicates statistical significance at p < 0.05; ** indicates p < 0.001.
Age emerged as a significant predictor in the lifting small objects and simulated feeding tasks: in these subtests, older age was associated with longer completion times (i.e., slower performance). For example, in the lifting small objects task, increasing age showed a positive regression coefficient (indicating slower dominant-hand performance with age, p < 0.05), and a similar age effect was evident in the feeding task (p < 0.001). In contrast, age was not significantly related to performance in the other four tasks.
Sex and handedness influenced performance in select tasks. Female sex (coded as 1) was a significant predictor of slower times in the stacking checkers and simulated page turning subtests (p < 0.05), indicating that women took longer to complete these tasks than men, independent of non-dominant hand ability. Handedness (left-handed vs. right-handed) was a significant factor in the page turning and lifting large heavy objects subtests. Left-handed participants (coded as 1) had longer dominant-hand completion times in those tasks compared to right-handed participants (p < 0.05). No other predictors reached significance in the remaining subtests (for instance, in the lifting large light objects task, non-dominant hand performance was the only significant predictor). Overall, while the contribution of age, sex, and handedness varied by task, the influence of non-dominant hand performance was consistently strong across all activities.
The models underlying Figure 1 are based solely on non-dominant hand performance, without adjustment for age, sex, or handedness. Stronger associations were observed in tasks involving gross motor function—particularly lifting large light (R2 = 0.643) and heavy objects (R2 = 0.675)—while tasks requiring fine motor control, such as simulated feeding (R2 = 0.245), demonstrated weaker relationships. Each plot includes individual data points and a fitted linear regression line (red), with non-dominant hand performance on the x-axis and dominant hand performance on the y-axis. The coefficient of determination (R2) displayed in each panel quantifies the proportion of variance in dominant hand performance explained by non-dominant hand performance.

Scatterplots and regression lines showing the relationship between non-dominant and dominant hand performances across JTHFT subtests, with R2 values indicating the strength of association for each task.
Discussion
The study revealed that non-dominant hand performance played a significant role in predicting dominant hand performance in several subtests of the JTHFT. Specifically, non-dominant hand performance in the JTHFT subtests “lifting large light objects” and “lifting large heavy objects” strongly predicted dominant hand performance, explaining 64% and 68% of the variance, respectively. In contrast, the predictive relationship was weaker in fine motor tasks, such as simulated feeding. These findings underline the active role of the non-dominant hand in supporting functional performance, particularly during force-based tasks.
The dominant hand demonstrated consistently superior performance in fine motor tasks, such as simulated feeding and lifting small objects, outperforming the non-dominant hand by over 10%.1,2 This is consistent with previous research linking dominant hand performance to refined neural control and enhanced sensory-motor integration.35,36 The cortical regions of the brain, particularly the left hemisphere, predominantly govern the dominant hand, enabling refined motor control. However, the right hemisphere also plays a significant role in specific motor functions, indicating a complex interplay between hemispheres. 4 The minimal difference in grip strength between dominant and non-dominant hands during tasks requiring larger muscle groups, such as lifting heavy objects, suggests that hand dominance plays a lesser role in strength-based activities. This lack of significant difference likely reflects the symmetrical nature of gross motor strength in healthy individuals. The performance gap between the non-dominant and dominant hand tends to increase when tasks require fine motor coordination. In contrast, the “lifting large heavy objects” subtest primarily relies on general upper limb strength, which results in a smaller performance difference between the two limbs. This supports the notion that general muscle strength, rather than fine motor control, is the primary determinant of performance in such tasks. 21
While less efficient than the dominant hand, the non-dominant hand facilitates coordination during bimanual and complex motor tasks, supporting motor control theories that emphasize the interdependence of both hands. 37 In addition, research highlights that bimanual activities engage specific brain network dynamics, with grip force coordination and kinematics being highly task-dependent. This underscores the brain's ability to adapt its processing strategies based on task demands and the interdependence of both hands in complex motor tasks. The findings emphasize the dynamic involvement of frontocentral and parietal networks in facilitating these task-specific adaptations. 38
Evidence shows that targeted training can significantly enhance non-dominant hand performance, narrowing the gap with the dominant hand. Consistent practice leads to measurable improvements in motor skills, underscoring the adaptability of the non-dominant hand through focused interventions. 39 This finding emphasizes the importance of using both hands together in motor control processes, especially in rehabilitation strategies. Research by Mollà-Casanova et al. highlights the significance of bilateral hand activities and coordination in enhancing motor performance, suggesting that structured assessment and training could support improved hand functionality, particularly after stroke. 40 Strengthening the non-dominant hand may not only enhance its own function but also support improved performance of the dominant hand through bilateral training effects. Rehabilitation strategies that target both hands—rather than prioritizing the dominant hand exclusively—may therefore be more effective in promoting functional recovery. In our study, the weak predictive relationships observed in fine motor tasks, such as simulated feeding, suggest the presence of unmeasured factors influencing task performance. Among the subtests, simulated feeding demonstrated the weakest predictive relationship between non-dominant and dominant hand performance, as reflected by its low adjusted R2 value. This finding suggests that simulated feeding may not reliably reflect inter-hand motor coordination or transferable skill patterns. The task's complexity, which combines fine motor precision with utensil manipulation and potential cognitive demands, may introduce variability not captured by simple linear associations. Future studies should examine whether such tasks require separate modeling strategies or alternative analytical approaches to better account for these multidimensional influences.
Variables such as attention, cognitive load, and sensory feedback are known to affect fine motor skills, and their exclusion may have limited the explanation of performance variance, particularly in tasks involving complex motor control. Future studies could address this limitation by incorporating dual-task paradigms or cognitive load assessments to better capture the multidimensional nature of fine motor performance. Research on dominant and non-dominant hand performance has shown that these relationships are influenced by factors like gender, sports specialization, and training habits. For example, a study on elite shooters revealed a significant positive correlation between dominant hand grip strength and shooting performance in female athletes, whereas this relationship was negligible and statistically insignificant in male athletes. 41 Similarly, research on male handball players indicates that dominant hand grip strength surpasses that of the non-dominant hand and shows a positive correlation with upper extremity neuromuscular control. However, this strength advantage alone does not directly predict performance outcomes, emphasizing the importance of technical and neuromuscular factors in achieving superior results. 42 Building upon these findings, our multivariate regression analyses revealed several additional insights regarding the role of non-dominant hand performance and demographic variables. Our extended regression analyses confirmed that non-dominant hand performance remained the most consistent and robust predictor of dominant hand performance across all JTHFT subtests. The strongest associations were observed in gross motor tasks such as lifting large light and heavy objects, while weaker but still significant relationships were noted in fine motor tasks like simulated feeding. Although age, sex, and handedness showed significance in some subtests, their effects were modest and task-specific. Age was associated with slower dominant-hand performance in lifting small objects and simulated feeding, while female sex predicted slower times in stacking checkers and simulated page turning. Left-handed participants also showed slower performance in selected tasks. These results reinforce the functional importance of the non-dominant hand and support its inclusion in both clinical assessments and rehabilitation planning.
However, due to the cross-sectional design of our study, causal inferences about these relationships cannot be made. Future research should incorporate more extensive datasets and utilize advanced statistical techniques, such as hierarchical regression or structural equation modeling, to better understand fine motor tasks. Additionally, including tasks that require bimanual coordination could provide insights that more closely reflect real-life activities and enhance our understanding of the interplay between dominant and non-dominant hand performances in practical contexts.
The findings from the current study have practical implications for occupational therapy and vocational rehabilitation settings, particularly concerning RTW assessments. Given that the JTHFT's subtests simulate manual tasks common in occupational contexts, understanding the predictive relationship between non-dominant and dominant hand performances may aid clinicians in evaluating work readiness and functional limitations following hand or upper extremity injuries. Therefore, our findings have important clinical implications for vocational rehabilitation and occupational health. Assessing both dominant and non-dominant hand functions together in return-to-work evaluations and rehabilitation planning could enhance clinicians’ ability to more accurately identify functional limitations, design targeted interventions, and determine job readiness following hand injuries or surgical procedures. Although return-to-work evaluations typically focus on dominant hand performance, occupational tasks commonly require coordinated and complementary use of both hands. An injury to the non-dominant hand can significantly affect a person's functional capacity at work, often more than anticipated. Previous research supports the utility of JTHFT in RTW processes, demonstrating that improved performance on this test correlates significantly with an individual's ability to effectively resume occupational duties, especially in professions requiring manual strength and dexterity.9,14 Sharma et al. emphasized that JTHFT scores serve as reliable indicators of work-related functional recovery in patients with rheumatoid arthritis. 15 Similarly, Ferreiro et al. highlighted the test's sensitivity in capturing motor improvements critical to occupational performance in patients recovering from mild hemiparesis. 16 Thus, incorporating JTHFT into vocational evaluations and treatment planning could provide clinicians with objective, work-specific benchmarks, thereby facilitating targeted interventions to optimize both hand function and successful RTW outcomes.
This study has several limitations that warrant consideration. First, the participant sample consisted solely of healthy individuals, restricting the generalizability of the findings to clinical populations, such as those with neurological or orthopedic impairments, or older adults experiencing age-related motor decline. The tasks included in the JTHFT primarily measured specific motor skills, excluding more complex activities requiring bimanual coordination or higher cognitive demands. Additionally, the study focused on short-term performance, without examining the long-term effects of training on both dominant and non-dominant hand function. Key factors such as cognitive load, attention, and fatigue, which are likely to influence hand performance, were not assessed. Moreover, the sample included a predominantly right-handed population, which may affect the generalizability of the findings, particularly to left-handed individuals. Demographic variables, including age, gender, and handedness, were also not explored in relation to the observed outcomes. These limitations highlight the need for future research involving diverse populations, comprehensive task assessments, and long-term follow-ups to better understand the role of non-dominant hand function in motor performance and rehabilitation.
Conclusion
In conclusion, this study underscores the critical role of non-dominant hand performance in predicting dominant hand performance across various functional tasks. While the predictive relationship was strongest in gross motor tasks, such as lifting large objects, it was also evident in fine motor activities, highlighting the interdependence between the hands. Our regression analyses further confirmed that non-dominant hand performance was the most consistent and robust predictor across all subtests, surpassing demographic factors such as age, sex, and handedness. These findings emphasize the importance of assessing both dominant and non-dominant hand functions comprehensively, especially within vocational rehabilitation, occupational evaluations, and return-to-work programs. The strong predictive value observed in gross motor tasks suggests that non-dominant hand evaluations should be integrated into occupational screenings and rehabilitation planning. Such an inclusive approach could improve the accuracy of identifying functional limitations, optimize rehabilitation outcomes, and enable clinicians to make more realistic and informed decisions about job readiness following hand injuries or surgical interventions.
Moreover, the results suggest the potential value of revisiting current motor skill training approaches, encouraging a move beyond a dominant-hand-centric focus toward more inclusive strategies that recognize the contributions of both hands. Adopting this perspective could significantly optimize motor function and independence in daily activities, offering substantial benefits across clinical and therapeutic settings. The weak correlations observed in fine motor tasks, such as simulated feeding, point to the influence of unexamined factors on performance. This underscores the need to investigate variables that might impact fine motor skills—such as attention, cognitive load, sensory feedback, and fatigue—which were not accounted for in this study. Future research should adopt a more comprehensive design to evaluate the effects of these factors thoroughly.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Ethical approval
This study was approved by the Cankiri Karatekin University Ethics Committee (Approval No: e6ce9251ed7b44c1) on October 15, 2024.
Informed consent
All participants provided written informed consent in accordance with ethical guidelines.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.