
Abstract
Background
Work-related musculoskeletal disorders (WMSDs) necessitate addressing physical and organizational risks while comprehending their cause-effect dynamics to reduce their risks.
Objective
This study focused on validating the Persian version of WOAQ, evaluating organizational and workload risks through WOAQ and PWQ, and unraveling interrelationships among organizational factors with WMSDs using Fuzzy DEMATEL analysis.
Methods
Conducted as a cross-sectional study in 2024 among 100 employees in a private company in Kerman, Iran, this research utilized the Forward-Backward method for WOAQ translation. Reliability was gauged via Cronbach's alpha and test-retest methods. The PWQ and WOAQ were used in assessing workload and organizational risks. Fuzzy DEMATEL analysis was employed to elucidate cause-effect relationships between organizational factors.
Results
Analysis of 81 questionnaires (41 men, 40 women) revealed the WOAQ's reliability with Cronbach's alpha and test-retest scores of 0.927 and 0.865. Predominant WMSD prevalence was observed in the lower back. 41.50% and 31.70% of men experienced high and very high organizational and workload risks. The DEMATEL fuzzy analysis identified rewards, recognition, and quality of relationships with management as influential factors.
Conclusions
Understanding factors influencing WMSD prevalence encompasses physical, organizational, and psychosocial facets. Overlooking non-physical aspects contributes to physical risks and subsequent musculoskeletal disorders. Prioritizing improved management relationships and recognition systems was pivotal for effective WMSD prevention strategies.
Keywords
Introduction
Work-related musculoskeletal disorders (WMSDs) encompass injuries and ailments due to occupational risk factors affecting various body parts. These conditions entail discomfort, injuries, or persistent pain in muscles, joints, tendons, nerves, or bones. They can manifest chronically over extended periods or acutely following severe trauma to the musculoskeletal system.1–5
As per the World Health Organization (WHO), musculoskeletal pain contributes significantly to years lived with disability (YLDs), constituting about 17% of YLDs globally. 6 Among these conditions, lower back pain is the most prevalent, followed by neck pain, encompassing discomfort in the neck, shoulders, and arms. 7 Work-related musculoskeletal disorders (WMSDs) rank as the second most common cause of workforce disability, posing substantial challenges in developed and developing nations. 8 These disorders exert a considerable burden on both management and employees due to medical expenses, absenteeism, and enduring musculoskeletal limitations.3,9,10 In the UK, WMSDs accounted for 24% of workdays lost due to occupational diseases in 2021–22. 11 Moreover, in South Korea, WMSDs constituted 56.8% of confirmed cases of occupational diseases in 2021. Notably, among Iranian workers in small and medium-sized companies, the prevalence of WMSDs was reported at 73%. 10 Previous research indicated that in Iran, the costs associated with WMSDs consumed nearly 0.1% of the government's annual budget in 2000. 12
Employees across various occupations often experience debilitating musculoskeletal pain and work-related injuries. 13 Work-related musculoskeletal disorders (WMSDs), being a primary cause of chronic pain and physical disability, significantly contribute to health issues among the working population. These disorders stem from an imbalance between job demands and individual resources, greatly influenced by job characteristics and ergonomic factors.14,15 Besides conventional ergonomic risk factors and physical workload, psychosocial elements and features associated with working hours, such as overwork or shift work, contribute to musculoskeletal pain. 16 Psychosocial risk factors in the workplace encompass the interplay between the work environment, job content, organizational conditions, workers’ capabilities, needs, culture, and personal considerations beyond the job that can affect health, job performance, and satisfaction. Physical factors impacting WMSDs include exerted forces, repetitive tasks, vibrations, and improper postures. 15
Office workers often exhibit symptoms related to work-related musculoskeletal disorders (WMSDs) due to repetitive movements, improper postures, and manual tasks. Numerous studies indicate that the prevalence of WMSDs among office workers ranges from 20% to 60%. This group also encounters psychosocial challenges, including time pressures and occupational stress, which significantly contribute to the development and persistence of WMSDs.17,18 Typically, a combination of ergonomic risk factors such as workstation design, improper body posture, repetitive motions, prolonged static positions, and extended working hours without proper rest, along with psychosocial and physical factors like environmental Noise and lighting, are linked to WMSDs among office workers.19,20 Various studies have identified that WMSD symptoms among office workers are most frequently reported in the lower back and neck, followed by the shoulder, hand, wrist, upper back, and knee.21–24
Celik et al. indicated that among office workers, the most commonly reported pain areas were the lower back, followed by the upper back and neck. 22 Moreover, Chinedu et al. in high education institutions highlighted an overall prevalence of approximately 72% for WMSDs among office workers, with reported issues concerning the lower back, wrists, and shoulders. 23
Given the necessity to explore the prevalence of WMSDs and implement suitable interventions, employing a valid assessment tool is crucial. Various tools have been used by experts to screen and subjectively evaluate the prevalence of these disorders. Questionnaires stand out among these tools as a conventional method to identify WMSDs and the contributing factors and tasks.25–27 Questionnaires and indirect assessment methods are extensively utilized due to their practicality, affordability, minimal participant burden, and wide acceptance. While direct evaluation methods offer more realistic estimations with reduced bias, their application in epidemiological settings is hindered by being time-consuming, expensive, invasive, and complex. 28 Presently, numerous studies have effectively investigated occupational hazards, particularly WMSDs, utilizing indirect assessment methods and questionnaires, showcasing positive outcomes.1,7,19,27,29,30
Physical workload (such as repetitive movements, static or awkward postures, manual handling, and physical exertion) stands as a primary contributor to WMSDs, resulting in disability and work absenteeism. Studies have established a correlation between physical workload and pain experienced in the back, neck, shoulders, and hips. The assessment of physical workload is crucial for the prevention and mitigation of WMSDs. To this end, the Physical Workload Questionnaire (PWQ) devised by Bot et al. serves as a concise and straightforward self-report tool for evaluating physical workload. This questionnaire has been employed in assessing patients with musculoskeletal disorders across various occupational categories with differing levels of physical workload, encompassing professions such as teachers, hairdressers, farmers, civil servants, managers, nurses, and similar occupations.30,31
Additionally, within the scope of office workers’ roles, acknowledging psychosocial and organizational risk factors (including the nature of interactions with supervisors, systems of acknowledgment and compensation, workload management, collaboration with coworkers, and the overall condition of the physical workspace), encompassing human relationships, holds significant importance. The Work Organization Assessment Questionnaire (WOAQ), crafted in 2006 by Griffiths et al., serves as an apt tool for forecasting well-being, mental health, and job satisfaction. 32 Although initially designed for application in manufacturing industries to identify elements linked to work design and management, gauging their influence on employees’ health and well-being, prior studies have demonstrated its successful usage across diverse sectors. These include the medical domain, involving professions like nurses and radiology specialists,1,29,33 public sector 34 as well as the financial sector.
The primary objective of ergonomics is to design and maintain appropriate workstations to enhance employee performance and alleviate work-related stress and fatigue. Office work includes a multifaceted physical environment, intertwining various workstation dimensions, equipment, and job characteristics. Any inadequacies in these aspects could significantly elevate the prevalence of WMSDs among office workers. Notably, numerous studies in Iran have indicated a pronounced prevalence of WMSDs, particularly in the lower back and neck areas, among office workers.21,24,35
The WOAQ primarily captures organizational and psychosocial dimensions such as management practices, reward systems, workload perception, and peer support, factors that have been strongly associated with psychosocial stress and the onset or aggravation of musculoskeletal symptoms. Similarly, the PWQ evaluates the frequency and intensity of physical tasks and postures known to increase biomechanical strain, including lifting, prolonged sitting, and awkward body positions. Several studies have demonstrated that both psychosocial stressors and physical workload can independently and interactively influence the development and persistence of WMSDs.36–38 Thus, by employing these two tools, the present study aims to capture both physical and organizational contributors to musculoskeletal pain among office workers.
To effectively address these ergonomics concern and implement control measures within the work environment, investigating the interplay of risk factors becomes imperative. The investigation of cause-effect relationships among influential factors by using tools such as fuzzy DEMATEL provides an optimal method for understanding their interactions. 39 Numerous studies have employed the Fuzzy DEMATEL method to analyze and mitigate workplace and organizational challenges, yielding valuable insights. 40 For instance, one study utilized Fuzzy DEMATEL to evaluate the causal relationships among shift work, job stress, and job satisfaction, demonstrating its effectiveness in identifying root causes that impact occupational health in industrial settings. 39 In another study, the aforementioned method was employed to reveal the relationship between risk factors affecting WMSDs. 41
In light of these considerations, a comprehensive ergonomic intervention in office environments aiming to boost performance suggests the use of a comprehensive questionnaire to assess the impact of physical workload and psychosocial factors on WMSDs among office workers. Consequently, this study endeavors to evaluate the validity and reliability of the WOAQ questionnaire and explore the correlation between WMSD prevalence and physical workload and organizational factors among office workers. Additionally, the investigation seeks to unveil the cause-effect relationships of organizational factors affecting WMSDs by utilizing the fuzzy DEMATEL method. Aligned with these aims, the research addresses the central question of how physical workload and organizational (psychosocial) factors, assessed through the PWQ and WOAQ questionnaires, are related to the prevalence of work-related musculoskeletal disorders (WMSDs) among office workers.
Methods
Design and procedures
The present study is cross-sectional research conducted in 2024, aimed at ascertaining the reliability and validity of the Persian version of the WOAQ. This study encompassed three key phases:
The translation of the WOAQ followed by an evaluation of its validity and reliability. Examination of the influential factors outlined in the WOAQ and PWQ concerning WMSDs. Analysis of the cause-effect relationships among the factors mentioned in the WOAQ using the fuzzy DEMATEL method.
Translation
Two essential validation phases are required when employing an original questionnaire. Initially, linguistic validity is scrutinized by translating the questionnaire into Persian, followed by an examination of the questionnaire's psychometric aspects. This validation process aims to ensure equivalence between the translated and original versions. When translating a questionnaire from its original language to another, two main methods are typically employed: the Dual-Panel and Forward-Backward methods. 42 This study utilized the latter approach.
In the initial translation phase, referred to as the Forward stage, the English version of the WOAQ was independently translated into Persian by two experts. Upon amalgamating these translations, the first draft of the Persian WOAQ version was formulated. Subsequently, in the Backward stage, the Persian draft of the questionnaire underwent translation back into English by two additional experts. The resulting back-translated versions and the original English questionnaire were then compared by a panel of experts well-versed in the subject matter to ascertain their alignment in terms of semantics and linguistic validity.
Participants
In this research, 100 office employees employed in a private company participated. To meet the prescribed quality standards, a minimum of 100 participants is advised for internal correlation assessment and at least 50 for reliability assessment. 30 Following an explanation of the research's objectives to participants, the questionnaire was disseminated among them. All participants provided informed consent prior to participation. Inclusion criteria encompassed a minimum of one year of work experience, while exclusion criteria involved pre-existing congenital musculoskeletal conditions and a history of musculoskeletal surgery. accordance with ethical guidelines.
Data collection
To gather the required data, a questionnaire comprising four sections was employed. The initial section included demographic details, followed by a musculoskeletal disorder assessment questionnaire adapted from the Nordic questionnaire in the second section. The third section contained the PWQ, and the fourth and final section encompassed the WOAQ.
First and second section
The initial segment gathers demographic and general participant information encompassing age, gender, height, weight, marital status, work experience, working hours, education level, and number of children. The subsequent section introduces a questionnaire based on the Nordic questionnaire, focusing on assessing the influence of musculoskeletal problems and disorders within the past 12 months on various body parts concerning daily activities.
Third section: physical workload questionnaire (PWQ)
The PWQ serves as a self-report questionnaire designed to evaluate physical workload. It encompasses 26 items focusing on assessing force, dynamic and static loads, repetitive tasks, improper postures, sitting, standing, and walking. Each item in the questionnaire is rated on a 4-point Likert scale: rarely or never, sometimes, often, and (almost) always. Certain items, such as kneeling, movement on knees, squatting, working above shoulder level or below knee level, handling loads exceeding 25 kg, applying considerable force with hands and arms, operating vibrating tools, and foot pedaling, were excluded from the final questionnaire as they were not relevant to office-based work. Subsequently, a revised questionnaire with 16 items was presented. Scoring of the PWQ involves summing the score of each item to obtain a raw score ranging from 0 to 48. The final score is computed by dividing the raw score by the maximum possible score and multiplying the result by 100, yielding a score between 0 and 100. A score of 0 indicates no physical workload, while 100 signifies the highest level of physical workload.
Fourth section: work organization assessment questionnaire (WOAQ)
The WOAQ comprises 28 items grouped into five factors, evaluating risks associated with design and management. These factors encompass the quality of relationships with management (9 items), recognition and rewards (7 items), workload issues (4 items), relationships with colleagues (2 items), and the physical environment's quality (6 items). Respondents rate each item on a 5-point Likert scale, ranging from very favorable or sufficient (with the highest score) to very unfavorable or not at all (with the lowest score), assessing the suitability of each aspect within their work environment. The total score, ranging from 28 to 140, is obtained by summing up the scores of all items. Notably, the “workload issues” item involves a reversed scale, hence its score is adjusted for statistical analysis. Interpreting the WOAQ score varies based on the assessment's objective. Generally, a higher score indicates a better work environment with fewer psychosocial risks, while a lower score signifies a poorer work environment with increased psychosocial risks.
Reliability test
In assessing reliability, Cronbach's alpha coefficient is employed to measure internal consistency as follows:

In equation 1, k is number of items (questions or components),
The reliability was also evaluated using the test-retest method. Participants completed the questionnaire twice at a one-week interval. Intraclass correlation coefficient (ICC) was calculated for each question to determine agreement levels: ICC < 0.50 for poor, 0.50 < ICC < 0.70 for moderate, 0.70 < ICC < 0.90 for almost perfect, and ICC > 0.90 for perfect agreement.43–45
Content validity test
The Content Validity Ratio (CVR) and Content Validity Index (CVI) were calculated to assess content validity.
Content validity ratio (CVR)
Following Lawshe's content evaluation panel approach, a group of experts comprising academic faculty members, industry professionals, and PhD students provide their assessments on each question, categorizing them as essential, useful but not essential, or unnecessary. The determination of content validity for each question is achieved through Lawshe's content validity ratio (CVR) equation (2). The minimum CVR value is established based on the number of experts involved, following Lawshe's table.

Where:
N = total number of experts
Content validity Index (CVI)
In this approach, experts evaluate each question based on three criteria: relevance (ranging from not relevant to completely relevant), simplicity (ranging from not simple and clear to quite simple and clear), and clarity (ranging from not clear to completely clear). The index is computed by dividing the number of experts who chose the last two options in each criterion by the total number of experts. If the resulting value is less than 0.70, the question is excluded. If it falls between 0.70 and 0.79, revision is necessary, and values greater than 0.79 are considered acceptable.
Item–total correlation analysis and internal consistency
The examination of item–total correlations is an essential step in evaluating both the reliability and construct validity of a questionnaire. This analysis examines the extent to which each item correlates with the overall scale score. It indicates whether each item measures the same underlying construct as the rest of the instrument. Items with higher correlations demonstrate greater contribution to internal consistency, while low or negative correlations may suggest that the item does not align conceptually with the intended dimension. In translated or culturally adapted questionnaires, this analysis is of great importance for identifying items that may not perform consistently due to contextual or linguistic differences.
Evaluation of the causal relationships among WOAQ risk factors utilizing fuzzy DEMATEL
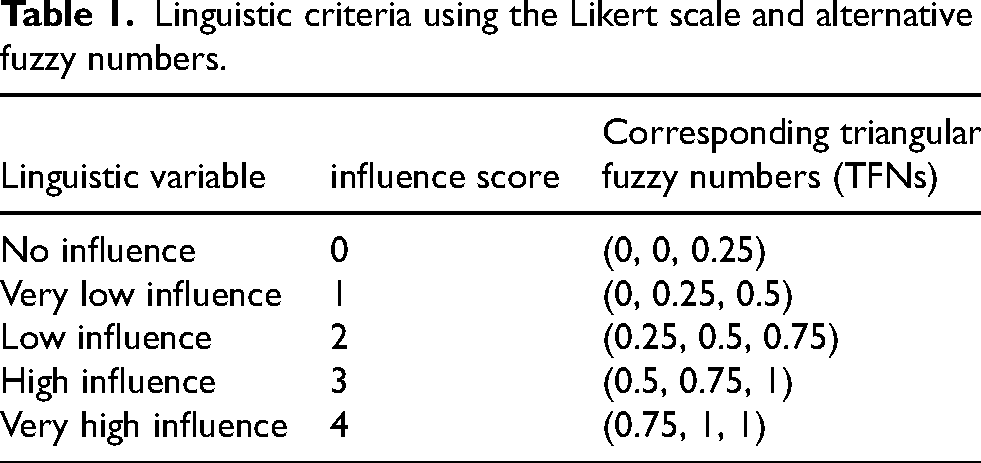
DEMATEL (Decision-Making Trial and Evaluation Laboratory) is a robust method for capturing expert opinions on complex issues, especially for identifying cause-and-effect relationships between variables.47,48 In this method, experts express their views using linguistic criteria on a Likert scale. In order to improve the accuracy of these assessments, fuzzy numbers, detailed in Table 1, are utilized to quantify the linguistic terms. The fusion of the DEMATEL method with fuzzy logic has led to the development of the fuzzy DEMATEL method. 49 One of the primary objectives of this study was to investigate the influence of organizational risk factors outlined in the WOAQ on the prevalence of WMSDs. Considering the diverse applications and high effectiveness of Fuzzy DEMATEL in offering refined control strategies, this methodology was employed to assess the cause-and-effect associations among the mentioned factors.
Linguistic criteria using the Likert scale and alternative fuzzy numbers.
The steps of the Fuzzy DEMATEL method are as follows
47
:
Identifying influential risk factors. Assembling a team of experts. Developing a questionnaire utilizing the Likert scale. Collecting experts’ opinions and scrutinizing the outcomes.
A team of ten experts, including five university faculty members in ergonomics and occupational health and five PhD students specializing in the same field, was selected for the Fuzzy DEMATEL analysis. All experts had a minimum of five years of professional or research experience related to occupational ergonomics. Experts were purposively selected based on their academic background, prior publications, and experience with risk-assessment methods to ensure high-quality and credible judgments. Another goal of this study was to assess the reliability and validity of the WOAQ while exploring the influence of organizational factors on the prevalence of WMSDs. Consequently, these factors were incorporated into the DEMATEL Fuzzy questionnaire.
The questionnaire articulated five primary criteria: the quality of the relationship with management, recognition and rewards, workload concerns, interpersonal relationships with colleagues, and the quality of the physical work environment. This structure was collected in a 5 × 5 matrix for the Fuzzy DEMATEL questionnaire. Subsequently, experts utilized the values outlined in Table 1 to complete the questionnaire.
Afterward the direct-relation fuzzy matrices are calculated using equation 3
47
:
P = the number of experts
The findings were analyzed according to the fuzzy DEMATEL procedure as follows:
Constructing the initial direct-relation fuzzy matrix ( Calculation of the normalized direct-relation fuzzy matrix ( Calculation of the total-relation fuzzy matrix ( Converting the total-relation fuzzy matrix ( Calculating D-value and R-value for each variable based on the components of the non-fuzzy total-relation matrix D-values and R-values were computed to gauge the strength of cause-and-effect links between variables. In the non-fuzzy total relation matrix, each row's sum (D) signifies the variable's impact on others, while each column's sum (R) illustrates the influence of other variables on each specific variable. Calculating D + R and D - R, creating a cause-and-effect diagram and analyzing the results
















D-R indicates the type of interaction (cause or effect) for each variable and D + R indicates the level of interaction between the variables.
Statistical analysis
To assess the agreement and correlation between the initial and subsequent participants’ responses, Kappa and Spearman's tests were utilized. Spearman's test was used to examine the correlation between the third and fourth sections of the questionnaire. To analyze the relationship between demographic factors and the prevalence of musculoskeletal disorders, the chi-square test was employed. Spearman correlation coefficients were also computed to explore the relationships between musculoskeletal symptoms, physical workload (PWQ), and work organizational conditions (WOAQ). All statistical analyses were conducted using SPSS version 27 software.
Results
Demographic information
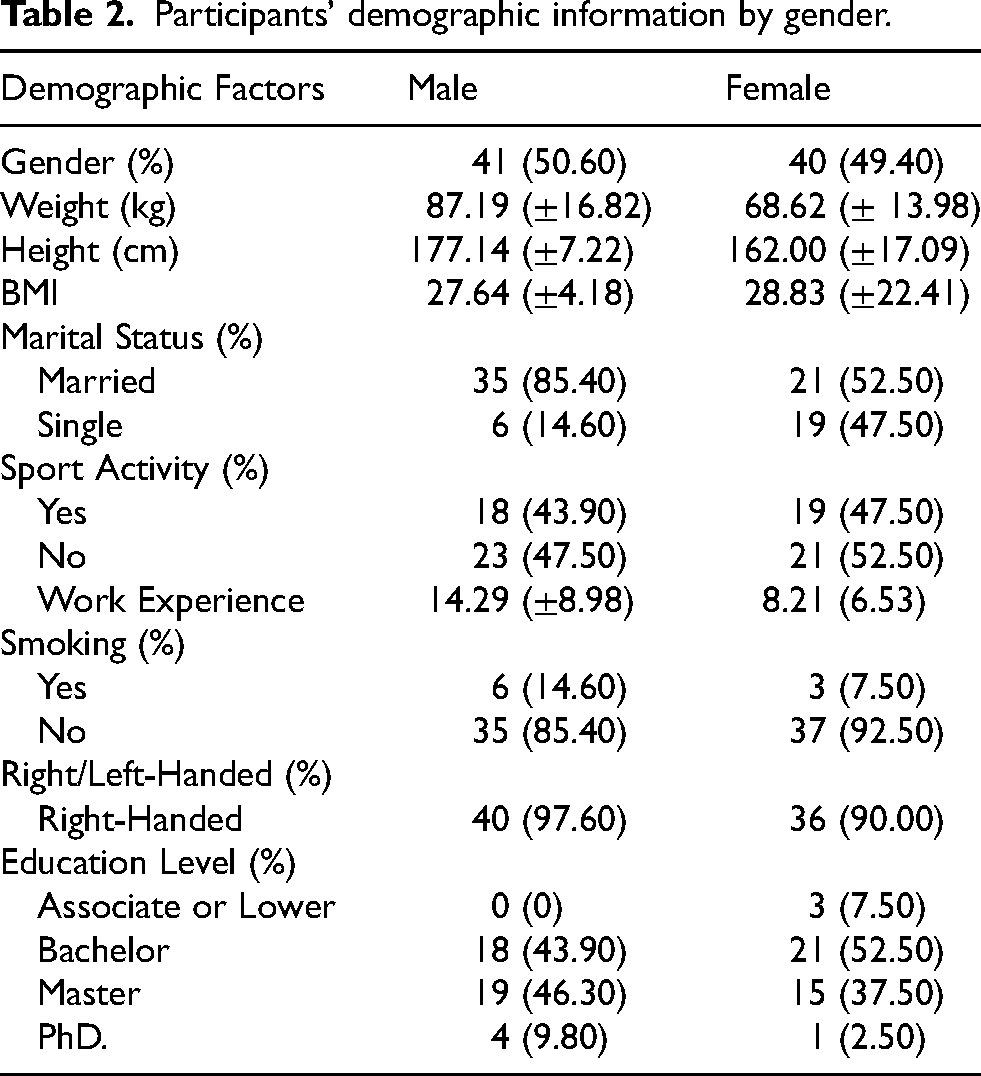
After the distribution and collection of the questionnaires and the removal of incomplete questionnaires, 81 questionnaires were completed accurately (In other words, 81% of the questionnaires were filled out correctly). Table 2 illustrates the participants’ demographic information.
Participants’ demographic information by gender.
Level reliability and validity indices of the Persian version of the work organization assessment questionnaire (WOAQ)
Results indicate that CVR values for all 28 items ranged from 0.75 to 0.94, exceeding the minimum acceptable value of 0.62 based on Lawshe's criteria for 10 experts. Similarly, all items achieved acceptable CVI values (≥ 0.79), with average item CVIs ranging from 0.83 to 1.00 and a scale-level CVI (S-CVI/Ave) of 0.90. Item–total correlation coefficients ranged from −0.11 to 0.82; except for four items (WO–20), all correlations exceeded the 0.30 threshold, supporting adequate internal homogeneity. The “Cronbach's alpha if-item-deleted” values (0.931–0.941) confirmed that the removal of any single item would not meaningfully improve reliability (for further information, refer to Appendix C).
Evaluation of the reliability of the WOAQ by Cronbach's alpha and ICC methods
Table 3 illustrates the reliability of the WOAQ using Cronbach's alpha and test-retest methods.
Reliability of the WOAQ using Cronbach's alpha and test-retest methods.
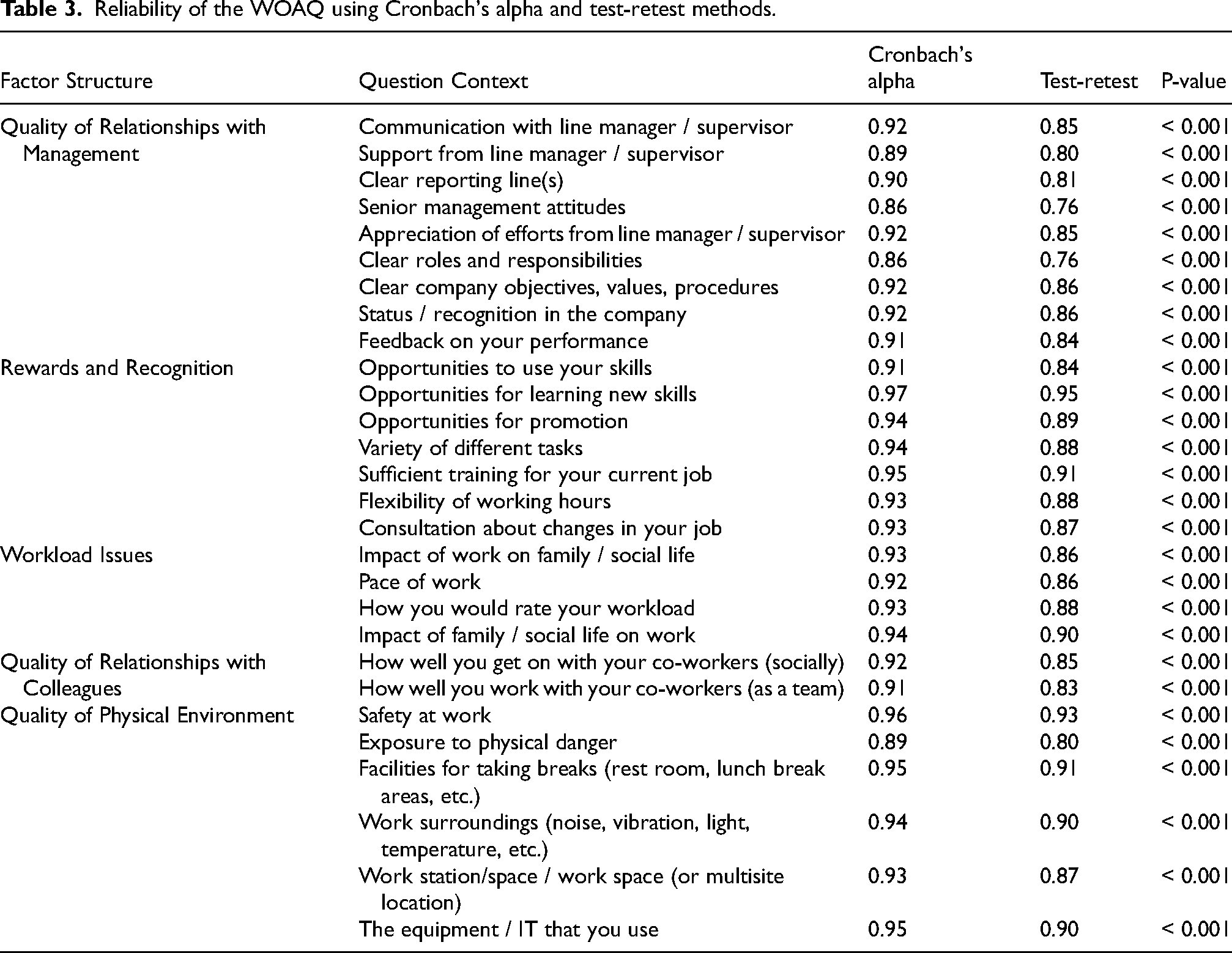
According to Table 3, the average reliability of the WOAQ is 0.927 and 0.865 for Cronbach's alpha and ICC.
Evaluation of validity of participants’ initial and subsequent responses to the questionnaire in ICC test
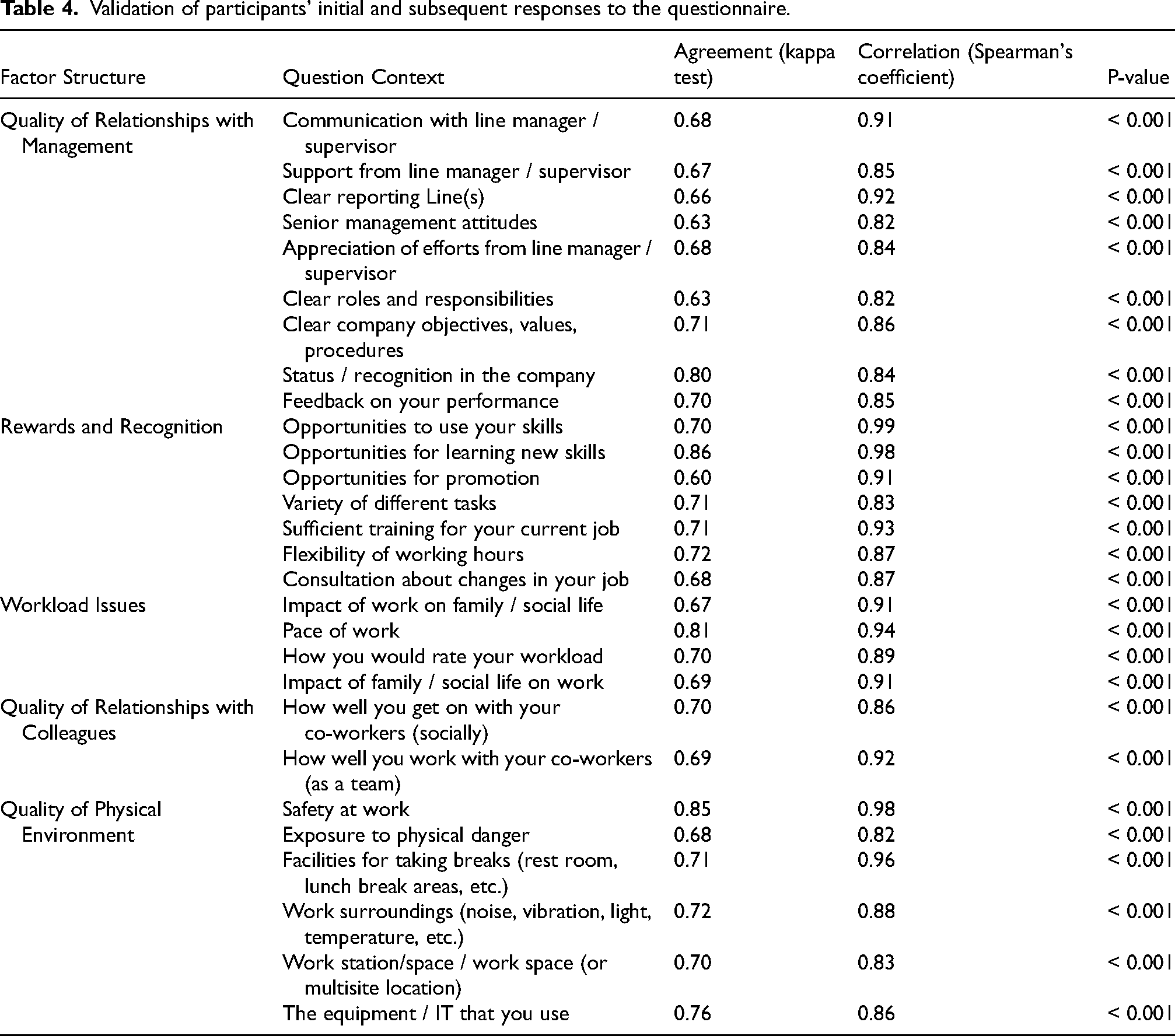
The verification of participants’ responses from the first and subsequent rounds of distribution is outlined in Table 4. In this phase, Kappa and Spearman's tests were utilized to evaluate the agreement and correlation among the responses.
Validation of participants’ initial and subsequent responses to the questionnaire.
Prevalence of WMSDs among participants
In Table 5, the prevalence of WMSDs among two groups of women and men during the last 12 months is presented.
Prevalence of musculoskeletal disorders among the participants during the last 12 months.
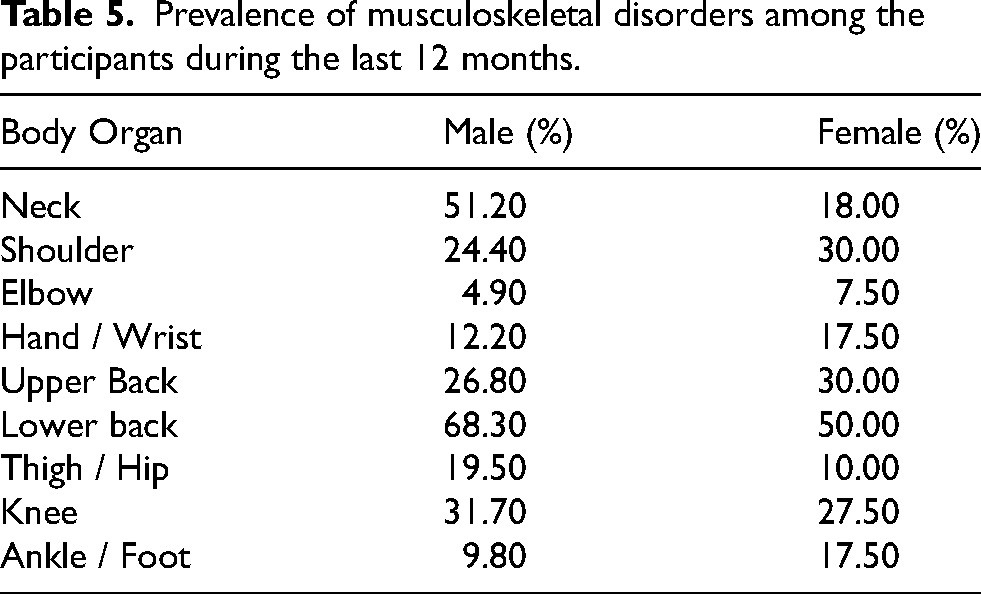
As shown in Table 5, the highest and lowest prevalence rates among both male and female groups were lower back and elbow, respectively.
Risk assessment of workload factors presented in the PWQ
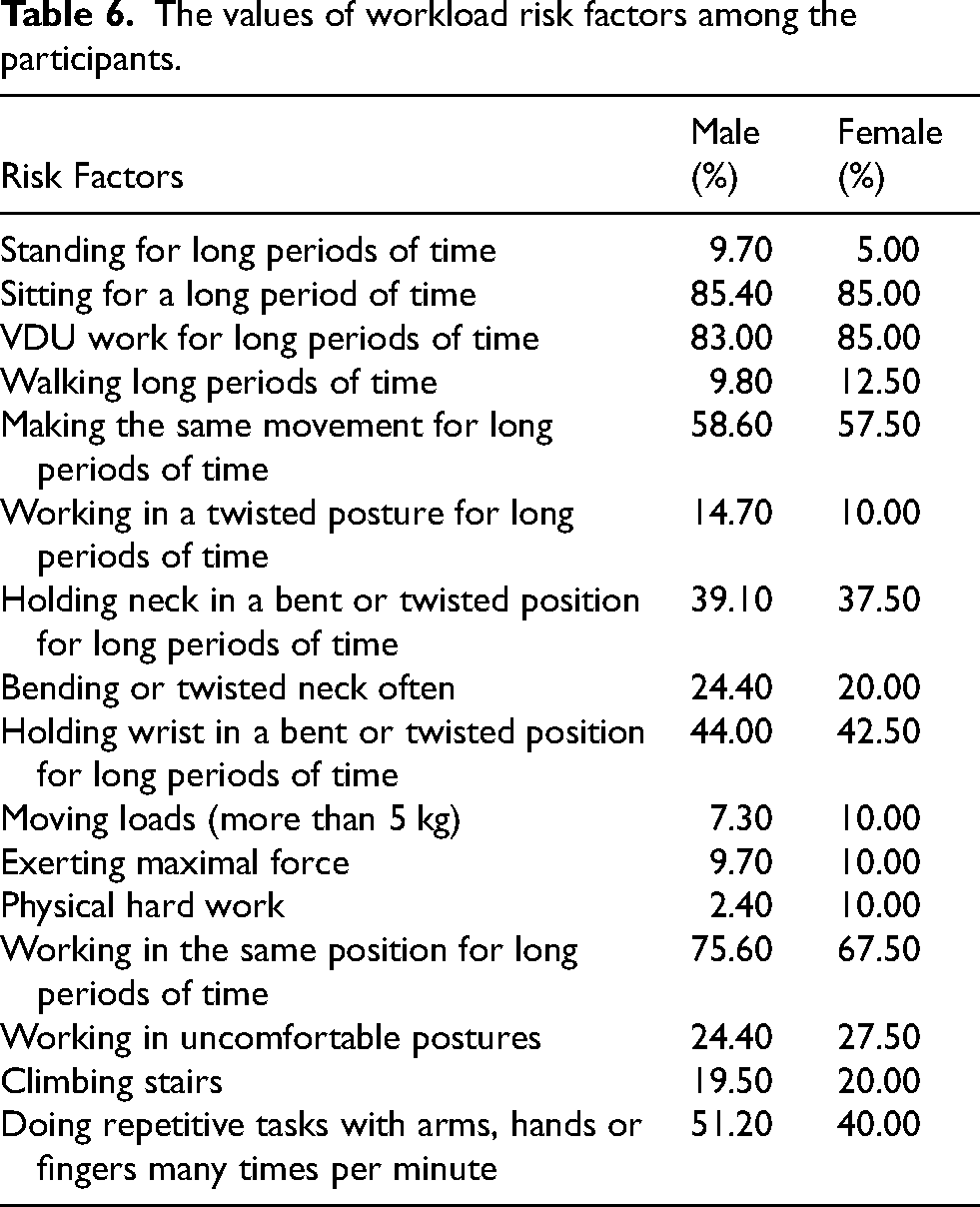
Table 6 shows the risk factors of physical workload for both male and female groups.
The values of workload risk factors among the participants.
Calculation of the final score of WOAQ and PWQ
Table 7 shows the final scores of the WOAQ and PWQ by male and female gender.
Average final score of risk factors of WOAQ and PWQ.
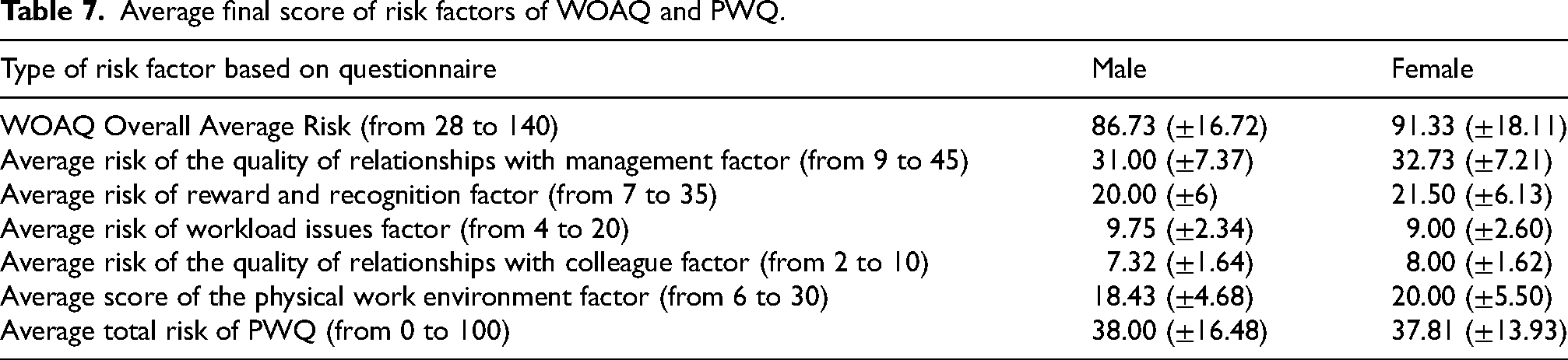
Table 8 specifies Risk score ranges for workload (PWQ) and organizational risk factors (WOAQ). For organizational risk factors, scores of 112–140, 84–111, 56–83, and 28–55 represent low, moderate, high, and very high-risk levels. For workload risk factors, scores of 0–24, 25–49, 50–74, and 75–100 indicate low, moderate, high, and very high-risk levels.
Risk score range of workload (PWQ) and organizational risk factors (WOAQ).

As per Table 8, 41.50% and 31.70% of males face high to very high risks for organizational and workload risk factors. For females, these values are 20.00% and 22.50% respectively.
Correlation analysis between musculoskeletal symptoms, physical workload (PWQ), and work organizational conditions (WOAQ)
According to analysis, a significant correlation was found between physical workload and musculoskeletal symptoms (ρ = –0.33, p = 0.003). Moreover, A significant negative correlation was observed between physical workload and organizational conditions (ρ = –0.36, p = 0.001).
Evaluation of the cause-effect relationships of organizational risk factors of WOAQ
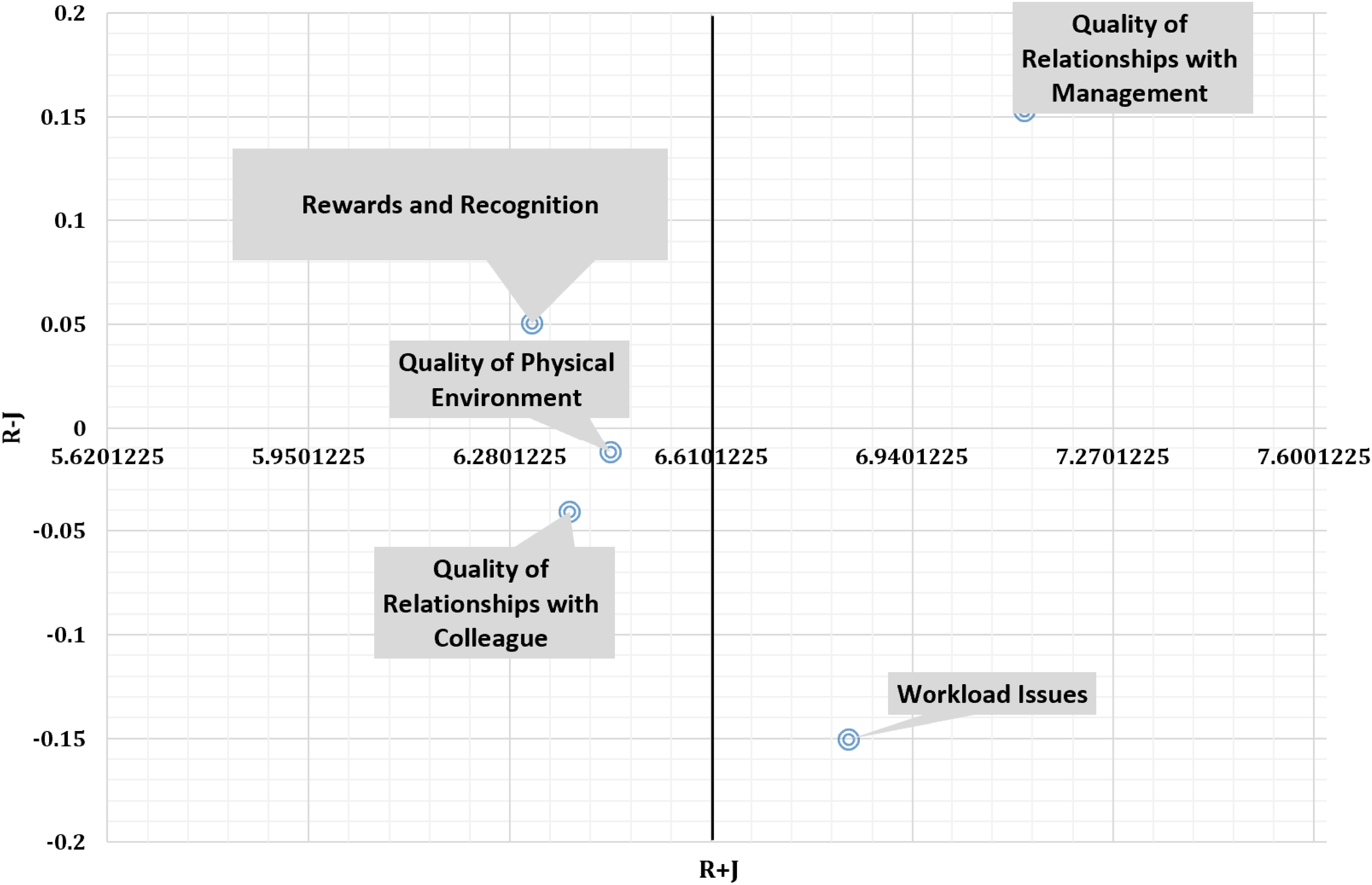
Table 9 represents the results of fuzzy DEMATEL analysis. Additionally, the cause-effect relationships of different risk factors are illustrated in Figure 1. For more detailed information regarding the fuzzy DEMATEL process and its intermediate results, please refer to Appendix A and Appendix B.
Cause-effect relationships of organizational risk factors in the WOAQ.
Defuzzied direct-relation total matrix.
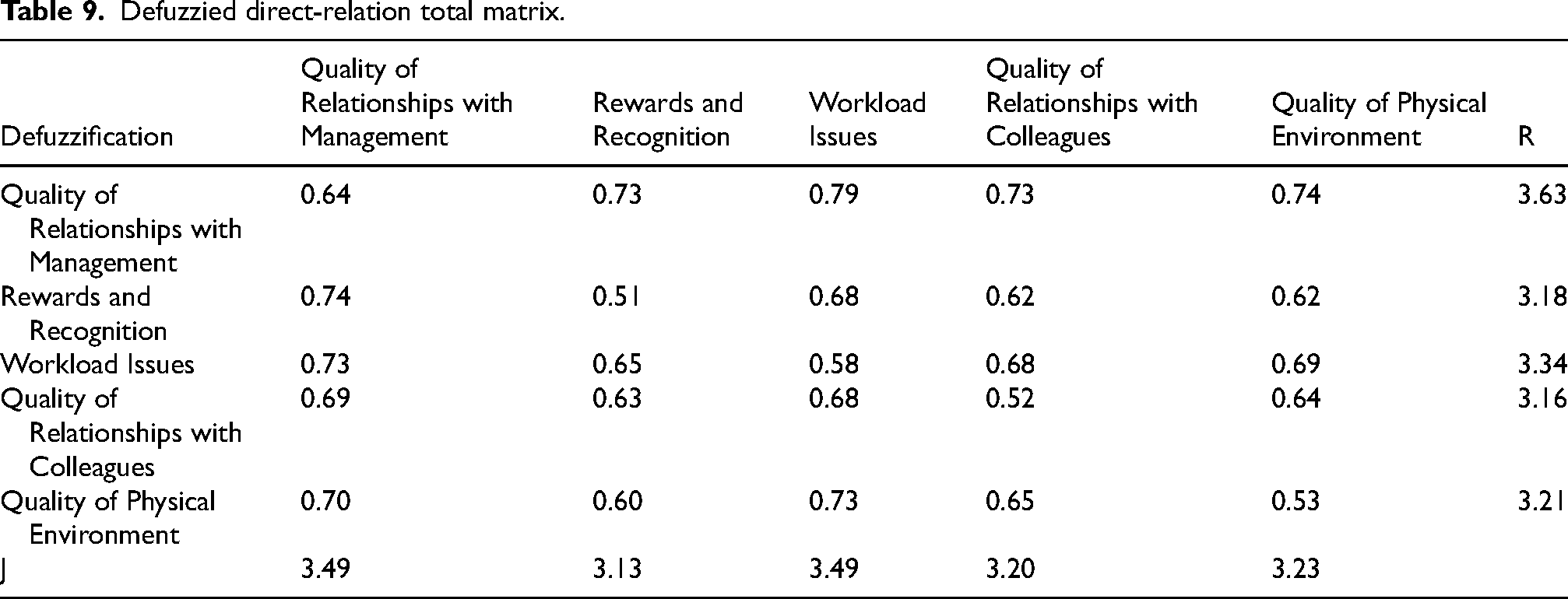
Figure 1 illustrates the cause-effect relationships among organizational risk factors identified in the WOAQ using the fuzzy DEMATEL method. The analysis revealed that “Quality of Relationships with Management” and “Rewards and Recognition” are key causal factors, positioned in the positive region of the R–J axis. These factors exert significant influence over other variables in the system. In particular, “Rewards and Recognition” appears to directly impact the “Quality of Physical Environment” and indirectly affect “Quality of Relationships with Colleagues” and “Workload Issues”, which are identified as effect factors with negative R–J values. “Workload Issues”, despite its relatively high importance (R + J), is primarily an outcome influenced by other organizational dynamics.
Statistical analysis of the relationship between the prevalence of musculoskeletal disorders (Nordic questionnaire) with workload (PWQ), organizational factors (WOAQ), and demographic factors
Musculoskeletal disorders and demographic factors
Upon assessing the connection between demographic factors and the Nordic questionnaire, it was evident that the significance of this relationship is more pronounced in women than in men. Some notable relationships in this regard include:
Women:
Age with neck, elbow and lower back pain Marital status with elbow pain Work experience with neck and ankle pain Having sports activity with shoulder pain
Men:
The only demographic factor that had a significant relationship with musculoskeletal disorders in men was the number of children with thigh/hip pain.
Table 10 delineates the organizational and workload risk factors that exhibited a statistical relationship with at least one of the musculoskeletal pains experienced within the past 12 months. Only significant and meaningful correlations with p-values below the accepted threshold (p < 0.01) are included to ensure clarity and relevance.
Analysis of the relationship between the prevalence of WMSDs during the last 12 months with organizational and workload risk factors.

The P values for all items in both questionnaires were calculated to be less than 0.001.
From an organizational standpoint, the neck and knee were the most affected areas, showing the highest number of significant correlations. Neck pain was linked to nine distinct factors, including Communication with the line manager, Clear roles and responsibilities, and Safety at work. Similarly, knee pain showed eight significant associations, notably with Support from the line manager, Sufficient training, and the quality of Facilities for taking breaks. In contrast, the analysis found no significant relationship between any organizational factors and pain in the shoulder, lower back, or thigh/hip.
Regarding physical workload factors, the upper back and hand/wrist were most prominently impacted, each having five significant correlations. Pain in the upper back was strongly associated with static and awkward postures such as sitting for a long period of time, VDU work, and holding the neck or wrist in a bent position. Hand/wrist pain was linked to a combination of static posture (Sitting), repetitive motion (Making the same movement), awkward posture (Holding wrist in a bent or twisted position), and forceful exertions. Neck pain was also highly correlated with physical workload, specifically with four factors related to repetitive and awkward neck postures. Conversely, no physical workload factors measured in this study showed a significant correlation with pain in the lower back, thigh/hip, or ankle/foot. Overall, these results indicate that organizational factors are most broadly associated with neck and knee discomfort, while physical workload risks are most predictive of pain in the upper back, hand/wrist, and neck.
Discussion
In this research, multiple methodologies were utilized to explore the impact of organizational factors on the prevalence of WMSDs. These approaches encompassed assessing the validity and reliability of the WOAQ, examining the influence of organizational risk factors (WOAQ) and workload (PWQ) on the occurrence of WMSDs, and determining cause-and-effect relationships among organizational factors. The overarching aim was to enhance the implementation of control measures within the relevant organization.
The content validity indices (CVR and CVI) confirmed that all WOAQ items were conceptually and linguistically appropriate for the Persian context, while the item–total correlation and internal consistency analyses further supported the scale's reliability and construct coherence. Together, these results indicate that the Persian version of the WOAQ maintains the psychometric integrity of the original instrument and can be confidently used to assess organizational work factors among Iranian workers. The calculated Cronbach's alpha for the WOAQ reliability stands at 0.927, while the test-retest method yields a score of 0.865. In Griffiths et al.'s study, the questionnaire's reliability, via Cronbach's alpha was between 0.80 and 0.90, deemed acceptable. Additionally, using the split-half test, all 5 discussed factors showed acceptable reliability. 32 In Karimi et al.'s research, the questionnaire's reliability was also acceptable, as determined by model-based reliability and the Rho factor. 33 Several other studies have consistently validated this tool's high reliability.50,51 Moreover, the questionnaire's validity was evaluated to an acceptable level via content validity assessment, analyzing the responses of 10 experts to the WOAQ. Numerous studies also confirm the questionnaire's validity. 32 An assessment of users’ initial and subsequent answers in this study using the ICC test, Kappa, and Spearman's tests revealed a satisfactory average agreement and correlation between the responses, measuring 0.710 and 0.891. 7
The prevalence analysis of Work-Related Musculoskeletal Disorders (WMSDs) highlighted distinct patterns. Men showed the highest prevalence in the lower back, neck, and knee, whereas women exhibited higher rates in the lower back, shoulder, and upper back. Conversely, men reported a lower prevalence of elbow, ankle/foot, and wrist/hand issues, while women had lower rates of elbow, thigh/hip, ankle/foot, and wrist/hand problems. The observed gender differences in WMSD prevalence, particularly the higher incidence of lower back disorders among men, may be attributed to variations in job roles, physical workload, and ergonomic exposure. In many office and administrative settings, male employees may be more frequently assigned tasks involving prolonged sitting without adequate lumbar support, manual material handling, or occasional physically demanding duties, which can increase lower back strain. Additionally, differences in workstation design, seating adjustments, and adherence to ergonomic principles may contribute to uneven biomechanical loading between genders. Organizational factors such as job demands, autonomy, and work–rest patterns may also interact with physical exposures, further influencing gender-specific WMSD outcomes. These findings highlight the importance of gender-sensitive ergonomic assessments and tailored preventive interventions in office environments. Aytutuldu and Calik's studies underscored that office staff predominantly experience WMSDs in the lower back, neck, and upper back.52,53 Office occupations, classified as Sedentary Work, commonly involve tasks such as computer work, long meetings, a lot of reading, phone communication, etc.. 54 Workers in office settings spend more than three-quarters of their work time seated in ergonomically unsuitable workstations, lacking physical activity and engagement in sports (refer to Table 2). Additionally, excessive computer or laptop usage (refer to Table 6) contributes to increased WMSDs prevalence. 53
The prevalence pattern observed in this study, particularly the high rates of lower-back, neck, shoulder, upper-back, and wrist/hand symptoms, is consistent with findings from other studies that used the PWQ. Bot et al. 31 and Kjønø et al. 30 similarly reported that individuals exposed to repetitive movements and prolonged static postures experienced frequent complaints in the neck, shoulders, and lower back. Studies by Kahraman et al. 55 and Noshadha et al. 56 also identified neck, shoulder, wrist/hand, and upper-back pain as the most common symptoms in occupations characterized by computer work and sustained sitting. Compared with occupations involving heavier physical labor, office workers show fewer hip and knee complaints but higher upper-body discomfort, reflecting the dominant influence of VDU work, repetitive arm and wrist motions, and prolonged sitting.
The primary reasons for the highest prevalence of WMSDs in the lower back and neck, according to participants’ responses to the PWQ, encompass prolonged engagement in repetitive movements, extended periods of working in twisted postures, sustained positioning of the neck in a bent or twisted manner, application of maximal force, and frequent bending or twisting of the neck. Notably, there was no correlation between lower back pain and other workload factors as stipulated in this questionnaire. However, several factors, that may be influential, are not mentioned in this questionnaire. For instance, as noted in Aytutuldu's research, insufficient contact of the feet with the ground is cited among the reasons for experiencing lower back and neck discomfort, especially for shorter workers. Additionally, the misalignment of wrists while using a keyboard and mouse contributes to the occurrence of shoulder and upper back pain. 53 Furthermore, Bontrup et al. highlighted in their study that the habits and postural behaviors associated with sitting on chairs significantly contribute to chronic back pain among office workers. 57
As illustrated in Table 7, the final workload risk level for both participant groups is around 38. Furthermore, Table 8 reveals that approximately 32% of men and 20% of women fall within the category of high and very high overall risk. Notably, a notable correlation emerged between the final PWQ score and specific pain areas—neck, elbow, wrist/hand, and upper back for men, and shoulder and knee for women. The observed associations demonstrate that physical workload is significantly related to the presence of musculoskeletal symptoms, consistent with prior evidence linking high physical demands to WMSD risk. Moreover, the significant inverse relationship between WOAQ and PWQ scores further supports the idea that better organizational environments may mitigate physical workload levels and, consequently, reduce musculoskeletal risks. Consequently, considering the final risk score and overall risk level, it becomes imperative to conduct a comprehensive assessment of the work environment conditions, particularly concerning workload risk factors, in the long run. Implementing control measures like reducing prolonged sitting periods, incorporating exercises during work hours, and integrating short break intervals after every 45-min work session should be prioritized.
The examination of the association between demographic factors and the prevalence of WMSDs among women indicates correlations with age, marital status, work experience, and engagement in sports activities, specifically concerning neck, elbow, lower back, ankle, and shoulder pain. King et al.'s investigation similarly confirmed a significant relationship between advancing age and the occurrence of musculoskeletal disorders. 58 Participants engaging in sports activities exhibited a lower prevalence of WMSDs, attributed to the reduction in physical workload due to regular physical activity, thereby enhancing the body's resilience against WMSDs. 59 Koneru et al.'s research highlighted that, individuals with considerably restricted mobility due to sedentary occupations, but engaging in activities such as yoga during the week, experienced notably fewer WMSDs. 60
In light of the WOAQ's organizational risk factors, the overall risk levels for males and females were approximately 87 and 91, respectively. Scores nearing 140 indicate a more favorable work environment concerning organizational and psychosocial risk factors. According to Table 8, 41.50% of men and 20.00% of women were categorized with high to very high overall risk levels regarding organizational factors.
Additionally, Table 10 reveals a significant association between various organizational risk factors and the prevalence of WMSDs. The findings from this Table highlight a compelling distinction in how different types of risk factors contribute to musculoskeletal pain in specific body regions. Overall, work organization is a process during which work or occupation is organized, monitored, and implemented. 61 An organization's procedures and policies wield substantial influence on WMSD prevalence through various avenues. These include issues related to job design, work-rest cycles, work pace, the psychological climate shaped by social interactions among staff, job safety measures, employees’ training levels, availability of job assistance, and communication with supervisors. 62
For instance, the influence of the quality of communication with line managers/supervisors, a component within the quality of relationships with management (See Table 10), contributes to WMSDs. Inadequate or weak communication channels between employees and management can breed misunderstandings, unclear work instructions, and a lack of guidance. These issues subsequently pave the way for work errors, potentially heightening physical strain or incorrect postures, consequently elevating the incidence of WMSDs.
Similarly, the impact of supervisor/managerial support on WMSD prevalence is like this. Insufficient support from managers induces considerable stress among employees. When encountering discomfort, physical problems, or ergonomic challenges, employees are less inclined to seek help or guidance from their supervisors. Overall, insufficient support hampers the timely implementation of ergonomic interventions, preventing the escalation of WMSDs.
The correlation between clear reporting lines and WMSD prevalence manifests in ambiguity and confusion regarding task execution or responsibilities. Such ambiguity leads to an accumulation of mental and physical workload or the inappropriate allocation of job duties. Consequently, unclear reporting lines result in assigning ill-suited tasks to individuals, contributing to the proliferation of WMSDs in various manners. Similar implications on WMSD escalation are observed across other subsets within this risk factor.
Restricted opportunities to apply skills, stemming from a lack of avenues for acquiring new skills, can elevate dissatisfaction levels or impede the effective utilization of individual abilities, subsequently impacting musculoskeletal conditions. Such dissatisfactions indirectly trigger increased stress, affecting working postures or diverting attention away from ergonomic measures, directly contributing to an escalation in WMSDs.
The absence of opportunities for skill development, a consequence of limited job promotion prospects, fosters a sense of stagnation or feeling stuck in one's role, diminishing motivation, engagement, and focus on ergonomic measures. These factors collectively exacerbate musculoskeletal issues. Among other subfactors within this risk factor, consultation regarding job changes significantly correlates with neck, elbow, and wrist pain. This scenario yields multiple outcomes. Firstly, it generates uncertainty and ambiguity among employees regarding their role changes, fostering confusion about their organizational position and escalating stress and anxiety levels. Furthermore, resistance to changes may arise due to individuals feeling undervalued within the organization, subsequently leading to reduced motivation. This uncertainty or resistance indirectly impacts workers’ focus on ergonomic practices and proper task execution, thus increasing WMSDs as a consequence. The association of other parameters within this risk factor with WMSDs follows a similar interpretive pattern.
Regarding the third risk factor, namely workload issues, ample research underscores the adverse impact of work pace and perceived workload on musculoskeletal disorders.63,64 The influence of work-family and social-life balance on WMSDs stems from these factors intensifying stress, strain, emotional pressure, and distractions while diminishing rest time. These elements can significantly impact mental and emotional well-being.
These stressors manifest in two detrimental ways on musculoskeletal conditions. Firstly, they result in heightened cortisol levels and reduced mental tranquility, consequently increasing skeletal-muscular tensions and discomfort. Secondly, such pressures divert attention away from ergonomic concerns, proper body posture, and the application of ergonomic measures.
Regarding the subsequent risk factor, concerning social interaction and teamwork among colleagues, it can be affirmed that favorable social dynamics and efficient teamwork, serve to alleviate stress levels, bolster job motivation, and diminish muscle tension across various areas, particularly the neck and shoulders. Conversely, conducive social and team relations facilitate consultation among co-workers regarding ergonomic concerns and problems. Staff members are motivated to support each other in adhering to ergonomic practices, consequently mitigating potential risks associated with WMSDs.
The organizational patterns identified in this study show strong alignment with findings from earlier research using the WOAQ across manufacturing, public sector, and healthcare settings. Griffiths et al. 32 demonstrated that poor relationships with management, high workload, and limited recognition are major organizational hazards contributing to reduced employee well-being. Similarly, Wynne-Jones et al. 65 found that in public sector workers, deficiencies in managerial support and work design factors were closely related to decreased performance and increased strain. Karimi et al.66,67 also reported that inadequate recognition, weak communication, and insufficient managerial support were significant stress-related factors among nurses. Consistent with these studies, “quality of relationships with management” and “rewards and recognition” emerged as the primary causal organizational factors in findings, shaping downstream conditions such as workload, peer relationships, and the physical work environment.
Nevertheless, within numerous environments, the focus tends to be primarily on physical risk factors and workload, overlooking concealed risk factors like organizational and psychosocial elements that might wield a more substantial impact compared to physical aspects. As elucidated in this study, the majority of physical risk factors emanate from disregarding the organizational and psychosocial dimensions of the workplace. Prioritizing organizational factors enhances staff motivation to address physical risk factors.
The application of the fuzzy DEMATEL method in this study provides a nuanced understanding of how organizational risk factors interact and contribute to the prevalence of work-related musculoskeletal disorders (WMSDs). Unlike traditional correlation-based approaches, fuzzy DEMATEL not only identifies the strength of relationships among variables but also distinguishes between causal and effect factors, offering strategic insights for targeted interventions. The assessment of cause-and-effect relationships within WOAQ organizational factors revealed the considerable influence of “Quality of Relationships with Management” and “Rewards and Recognition” as primary causal factors, which subsequently affect the quality of the physical work environment, relationships with colleagues, and workload issues, all of which are well-known contributors to WMSD risk. This cause-and-effect mapping is particularly critical for designing effective organizational interventions. Rather than addressing only the surface-level symptoms, such as high workload or poor working conditions, DEMATEL enables the identification of upstream drivers within the organizational structure. Prioritizing the enhancement of communication channels and relationships with management, as well as strengthening recognition and reward systems, becomes essential. In practice, this entails investing in parameters such as opportunities for skill development, career advancement, diversified job roles, adequate job-specific training, flexible working hours, and employee consultation regarding job changes. Given the pivotal role of these two causal factors, implementing improvements in these domains can generate downstream benefits, enhancing aspects such as workload management, collegial relationships, and the physical work environment. By making these leverage points explicit, fuzzy DEMATEL strengthens the foundation for workplace health promotion and ergonomic risk control, ultimately contributing to the reduction of both psychosocial strain and physical exposures associated with WMSDs.
Based on the identified causal factors, practical interventions should focus on strengthening communication and trust between employees and management, as well as implementing transparent and meaningful reward systems. Enhancing opportunities for skill development, flexible work arrangements, and employee involvement in job decisions can also improve downstream factors such as workload, peer relationships, and the physical environment. These targeted organizational changes may play a critical role in reducing the risk of WMSDs.
This study is limited by its small and localized sample size and its reliance on self-reported data, which may affect the generalizability and accuracy of the findings. Additionally, no objective ergonomic measurements—such as direct observation or instrument-based assessments—were included, which may introduce reporting biases and reduce the precision of the results. Future studies are encouraged to combine self-report tools with objective assessment methods to provide a more comprehensive evaluation of workplace risk factors. Another limitation concerns the absence of factor analysis for the Persian version of the Work Organization Assessment Questionnaire (WOAQ). The present research was designed to examine the reliability and content validity of the translated instrument without modifying its original structure. However, confirmatory factor analysis (CFA) is recommended in future research to statistically verify whether the Persian version retains the factorial structure of the original scale. The current sample size (n = 81) was insufficient for a robust CFA, which generally requires at least 200 participants or 5–10 respondents per item. Therefore, future studies with larger and more diverse samples are needed to further validate the structural integrity of the Persian WOAQ. Moreover, longitudinal studies are recommended to better understand causal relationships between organizational factors and musculoskeletal outcomes. Incorporating multiple data sources, larger populations, and long-term follow-up will enhance the robustness and generalizability of future findings.
Conclusion
This research aimed to scrutinize the Persian version of the WOAQ's validity and reliability and to assess the influence of workload (PWQ) and psychosocial and organizational risk factors (WOAQ) on the prevalence of Work-Related Musculoskeletal Disorders (WMSDs). The findings underscored the Persian WOAQ's robust reliability, validity, and suitability for assessing organizational risk factors among Iranian office workers. This study indicated that to control the prevalence of WMSDs, not only physical risk factors and workload should be considered, but organizational and psychosocial factors should also be investigated. This is because the root of many musculoskeletal disorders is physical factors caused by neglecting organizational and psychosocial factors in the work environment. Besides, evaluating the cause-effect relationships of organizational risk factors using fuzzy DEMATEL determined that improvement of two factors- the quality of relationships with management, and rewards and recognition- is essential for arranging a control program.
Footnotes
Acknowledgments
We are thankful to everyone providing the necessary facilities for this work.
Ethics approval and consent to participate
We confirm that all procedures delineated in this study were executed in compliance with the pertinent guidelines and regulations, including the Declaration of Helsinki. This study is a part of a broader research project that received ethical approval from the Research Council of Tehran University of Medical Sciences, with reference number IR.TUMS.SPH.REC.1402.238.
Informed consent
Before the commencement of the study, participants expressed their willingness to participate by completing a written informed consent form, having been provided with comprehensive information about the study.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Appendix A
The Average of Experts’ Total Fuzzified Scores.
Appendix B
Normalized Direct Total Matrix.
Appendix C
Item-Level Reliability and Validity Indices of the Persian Version of the Work Organization Assessment Questionnaire (WOAQ).