
Abstract
Background
Effective management of low back pain requires a biopsychosocial approach, integrating physical, psychological, social, and occupational elements. Although moderate evidence supports multidisciplinary biopsychosocial rehabilitation and workplace interventions individually, the impact of combining these approaches for employees on sick leave due to low back pain remains unexplored.
Objective
This systematic review investigated the effectiveness of biopsychosocial rehabilitation including workplace interventions for employees on sick leave due to low back pain.
Methods
Structured literature search were conducted in MEDLINE, EMBASE, CINAHL, PEDro, PsycINFO and supplemented with grey literature. Eligible studies were randomized or non-randomized controlled studies involving employees on partial or full sick leave due to non-specific low back pain in subacute or persistent phases. Two reviewers independently performed screening, data extraction and risk-of-bias assessment. Interventions were described using the TIDieR checklist, and certainty of evidence was graded according to GRADE.
Results
Four publications representing three randomized controlled trials with 346 employees included. Evidence quality was low to very low for pain, return to work, and sick leave, but moderate for improvement of disability at 12 months follow-up.
Conclusion
Limited available evidence suggests that incorporating workplace interventions into multidisciplinary biopsychosocial rehabilitation may improve long-term disability for employees on sick leave due to low back pain. However, evidence for effects on pain, return to work and sick leave remains low or very low. This review identifies critical gaps in existing interventions and provides practice-based foundation, underscoring the need for further research to optimize rehabilitation for individuals with low back pain.
Keywords
Introduction
Low back pain (LBP) is the leading cause of disability worldwide, affecting an estimated 619 million individuals in 2020 alone, and its prevalence continues to rise.1–3 The condition places a substantial burden not only on individuals but also on health systems, workplaces, and the broader economy.1–4 In working populations, LBP is a significant contributor to long-term sick leave, premature retirement, and loss of productivity, with annual societal costs reaching billions of euros in high-income countries. 4 LBP is typically categorized by symptom duration as acute (< 6 weeks), subacute (6 to < 12 weeks), and persistent or chronic (≥ 12 weeks) pain.5,6 LBP develops and persists through a complex interplay of biophysical, genetic, psychological, social, and lifestyle factors.7–10 Given this multifactorial etiology, clinical guidelines recommend a multidisciplinary rehabilitation approach grounded in the biopsychosocial model of health.11–13
Biopsychosocial rehabilitation of LBP is typically defined as an integrated program involving a physical component (e.g., an exercise program) and at least one other psychological, social, or occupational component.11,14 While this approach has shown moderate effectiveness in reducing pain and disability, its impact on work-related outcomes remains inconsistent. Several systematic reviews have synthesized evidence on multidisciplinary or biopsychosocial rehabilitation for LBP, including Kamper et al. (2014), Marin et al. (2017), and Bernaers et al. (2023), all of which highlight considerable variability in intervention content and outcome focus.14–16 This heterogeneity, combined with a lack of detailed descriptions of the intervention components, makes it difficult to determine which aspects of biopsychosocial programs are most effective. 17 When looking at improvement of work-related outcomes, such as reduced sick leave or sustained return to work, one component that appears particular promising is the integration of workplace intervention. In their Cochrane review, Van Vilsteren et al. (2015) demonstrated moderate evidence of workplace interventions on work-related outcomes among employees with musculoskeletal disorders, including LBP. 18 Similarly, Williams et al. (2007) found that workplace interventions were effective in managing work-related outcomes, indicating the possible benefit of including worksite involvement in the rehabilitation of LBP. 19 However, more recent findings by Russo et al. (2021) reported less favorable effects of workplace interventions specifically on work-related outcomes for individuals with LBP. 20 These discrepancies may reflect inconsistent definitions of workplace interventions. Van Vilsteren et al. (2015) define workplace interventions as modifications to equipment, work design, organization, working conditions, or the work environment. 18 In contrast, Russo et al. (2021) employed a broader definition, considering any activity delivered at the workplace as a workplace intervention, even if it is not directly work-related, such as general exercise programs or pain education sessions. 18 Therefore, it seems crucial to distinguish between general activities provided in the workplace setting and interventions that directly address work-related factors. 18
To our knowledge, no previous review has specifically evaluated workplace interventions as an integrated component of biopsychosocial rehabilitation programs where work-focused strategies are embedded alongside physical, psychological, or social components. Clarifying this integration is essential for understanding which combinations of interventions best support work reintegration among employees with LBP.
The objective of this systematic review was to identify, evaluate, and synthesize evidence regarding the effectiveness of biopsychosocial rehabilitation programs that explicitly incorporate workplace interventions for employees on sick leave due to LBP. In addition, we aimed to describe the content and structure of the included programs to provide a clearer basis for interpreting their effects on work-related and functional outcomes and to enable more transparent comparisons across studies.
Review question
What is the effectiveness of biopsychosocial rehabilitation interventions that include workplace interventions compared to interventions without workplace interventions, in reducing sick leave, improving work status, decreasing disability and pain levels, and enhancing quality of life and psychological functioning in employees on sick leave due to LBP?
Methods
This systematic review was conducted according to a pre-specified protocol, which was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO; CRD42023397329). The methodology followed guidance from the Joanna Briggs Institute, 21 and reporting adhered to the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) statement checklist. 22
Databases and search strategy
A comprehensive search strategy was designed together with an experienced information specialist and conducted on March 21 2023 in MEDLINE (Ovid), EMBASE, CINAHL, PEDro, and PsycINFO. The search was repeated on 17 March 2025 to capture recent studies. The systematic search was adapted for each database and conducted from the earliest year of availability in each source. The search terms used were: “low back pain”, “workplace interventions”, and “randomized controlled trial or controlled clinical trial” (Appendix 1). These search terms and corresponding synonyms were identified from two former Cochrane reviews.14,18 A pilot test of the search was conducted to assess relevance before performing the final search. A search strategy for grey literature was also included (Appendix 2). This involved identifying organizations, experts, and government agencies involved in workplace interventions for employees with LBP. In addition, a web search was conducted using Google Scholar and OpenGrey. All reference lists of included studies were screened for additional studies, and Web of Science was used to search for citations.
Eligibility criteria
Eligible studies enrolled adults aged 18 years or older who were on partial or full sick leave due to non-specific LBP. Sick leave referred to temporary work absence and did not include individuals receiving permanent work disability benefits. Studies focusing on specific spinal conditions (e.g., infection, neoplasm, inflammatory arthritis, spinal stenosis, vertebral fracture), radiculopathy, or recent back surgery (within 12 months) were excluded. Studies focusing exclusively on acute (<6 weeks) pain were excluded. Eligible interventions were programs that combined a workplace component with at least one additional biopsychosocial element, such as a physical, psychological, or social component. Workplace interventions were defined as modifications in tasks, equipment, organization, working conditions, or the broader work environment, and required active involvement of both the employee and the employer or supervisor. 18 Comparators could include usual care, no treatment, or single-disciplinary interventions without integration of other biopsychosocial elements.
Studies were included only if they reported at least one relevant outcome, such as sick leave, work status, disability, pain, quality of life, or psychological outcomes like depression, anxiety, or fear-avoidance beliefs. This broad outcome range was necessary to reflect the biopsychosocial framework underpinning the review and to align with previous systematic reviews, which emphasize that clinical, functional, and work-related outcomes together provide the most meaningful evaluation of rehabilitation programs.
We accepted outcome data at short-term (up to three months), medium-term (more than three but less than twelve months), and long-term follow-up (twelve months or more). When multiple time points were reported, we extracted those closest to three, six, and twelve months. Both randomized controlled trials and non-randomized controlled studies with a control group were eligible for inclusion. Publications had to be written in English, Danish, Swedish, or Norwegian.
Types of interventions
Based on the definition used in the Cochrane review by Kamper et al., relevant rehabilitation interventions were defined as interventions that integrated at least two different components from the biopsychosocial model, that is physical, psychological, social or occupational.11,14 For the selected interventions, one of these components should be a workplace intervention. The definition of workplace interventions was based on the former Cochrane review by van Vilsteren et al., and thereby defined as modifications to the workplace, equipment, work design, work organization, working conditions, or work environment. 18 Changes should at least involve the employee and the employer or supervisor. 18 The setting for the workplace component was explicitly restricted to the workplace, whereas no setting limitations were imposed on the other components of the intervention program, allowing their implementation in diverse settings such as the workplace, primary health care, community, or home.
Selection of studies
Two reviewers independently screened titles and abstracts of the articles found in the literature search. Articles were selected for full-text screening based on their adherence to the inclusion criteria. The same two reviewers conducted the full-text screening and registered reasons for exclusions. Any disagreements were solved by consensus or involving a third reviewer who made the final decision on whether to include or exclude the article. The screening process of articles was conducted using Covidence. 23
Data extraction
Data were extracted independently by two reviewers and cross-checked by a third. A standardized form captured: (1) author, year, country; (2) study design, sample size, follow-up duration, outcomes; (3) participant characteristics (age, sex, pain duration, chronicity, work setting); and (4) intervention details described according to TIDieR. 24 Authors were contacted for clarification where needed. Data management was performed in Covidence. 23
Risk of bias assessment
To ensure consistency with the subsequent GRADE evaluation, the risk of bias in randomized trials was appraised using the RoB 2 tool. 25 This instrument examines key methodological domains, including randomization procedures, adherence to assigned interventions, completeness of outcome data, outcome measurement, and selective reporting. Each domain was judged as low risk, some concerns, or high risk of bias. Two reviewers assessed all studies independently, with disagreements resolved through discussion or, if necessary, adjudication by a third reviewer.
Data synthesis
A meta-analysis was not conducted due to heterogeneity in interventions and reporting formats. Instead, a descriptive narrative synthesis was performed. For each included study, effect estimates, 95% confidence intervals, and p-values were extracted and reported. Statistical significance was defined as p ≤ 0.05.
Evidence synthesis
The overall certainty of the evidence for each outcome was appraised with the GRADE approach 26 using GRADEpro software. 27 Evidence was classified into four levels—high, moderate, low, or very low—based on a holistic judgement that considered possible limitations such as risk of bias, variation across studies, indirectness, imprecision, and potential publication bias. The procedure for determining final ratings followed guidance described by Murad et al. 28
Results
Identification and selection
Figure 1 shows the selection of studies. We identified 3.326 records, along with an additional 208 conference abstracts and sources from grey literature. Of these, 1198 duplicates were removed. In total, 2.336 records were subjected to title and abstract screening, of which 93 articles were included for full-text screening. Four studies29–32 were ultimately included, representing four RCTs, one of which reported on the same intervention. The reasons for exclusion are detailed in Figure 1. A comprehensive list of studies excluded at the full-text screening stage, along with the corresponding reasons for exclusion, is presented in Appendix 3. Neither the update search nor citation/reference searches added additional publications.
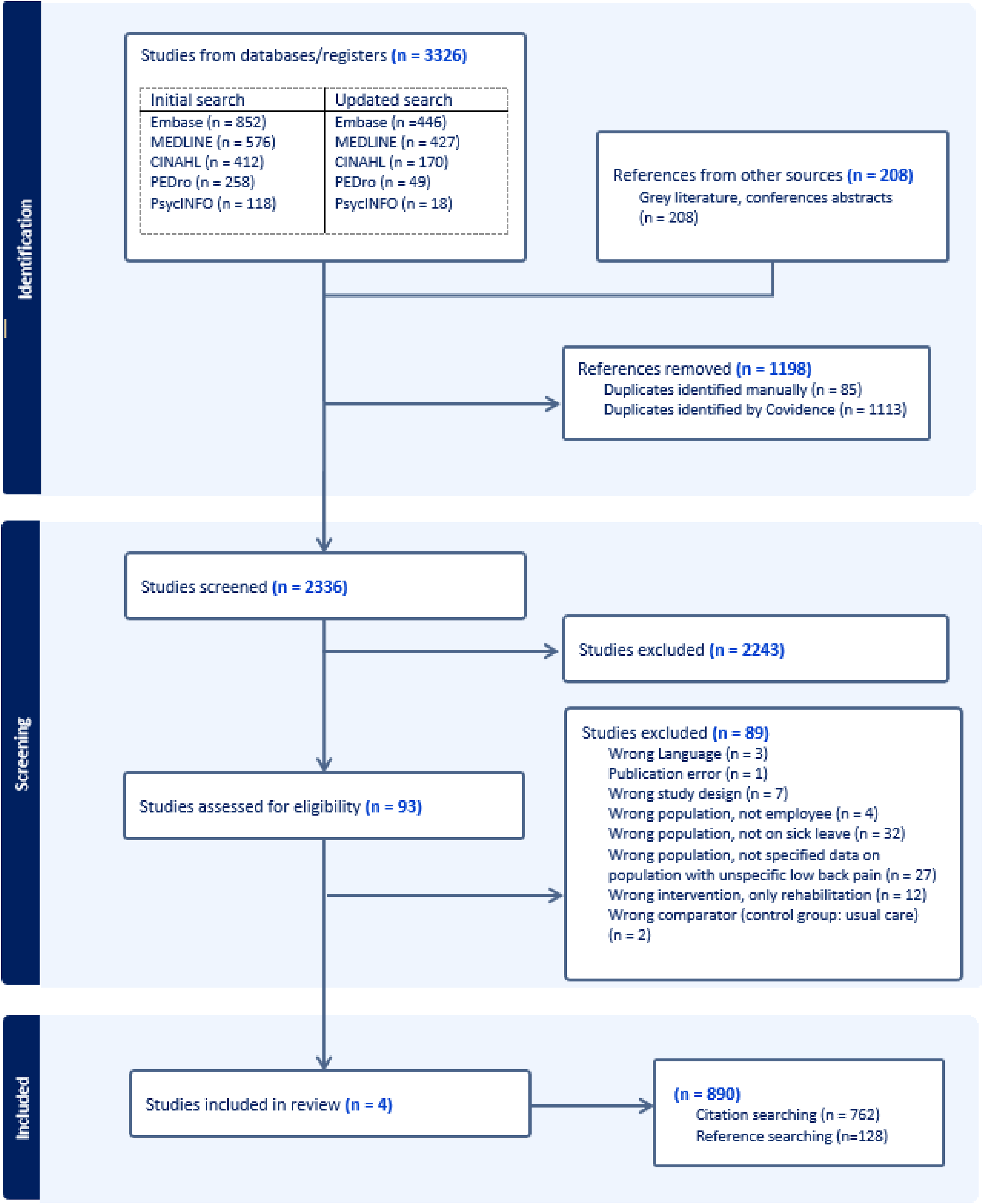
PRISMA flow diagram of the study selection process.
Characteristics of the included studies
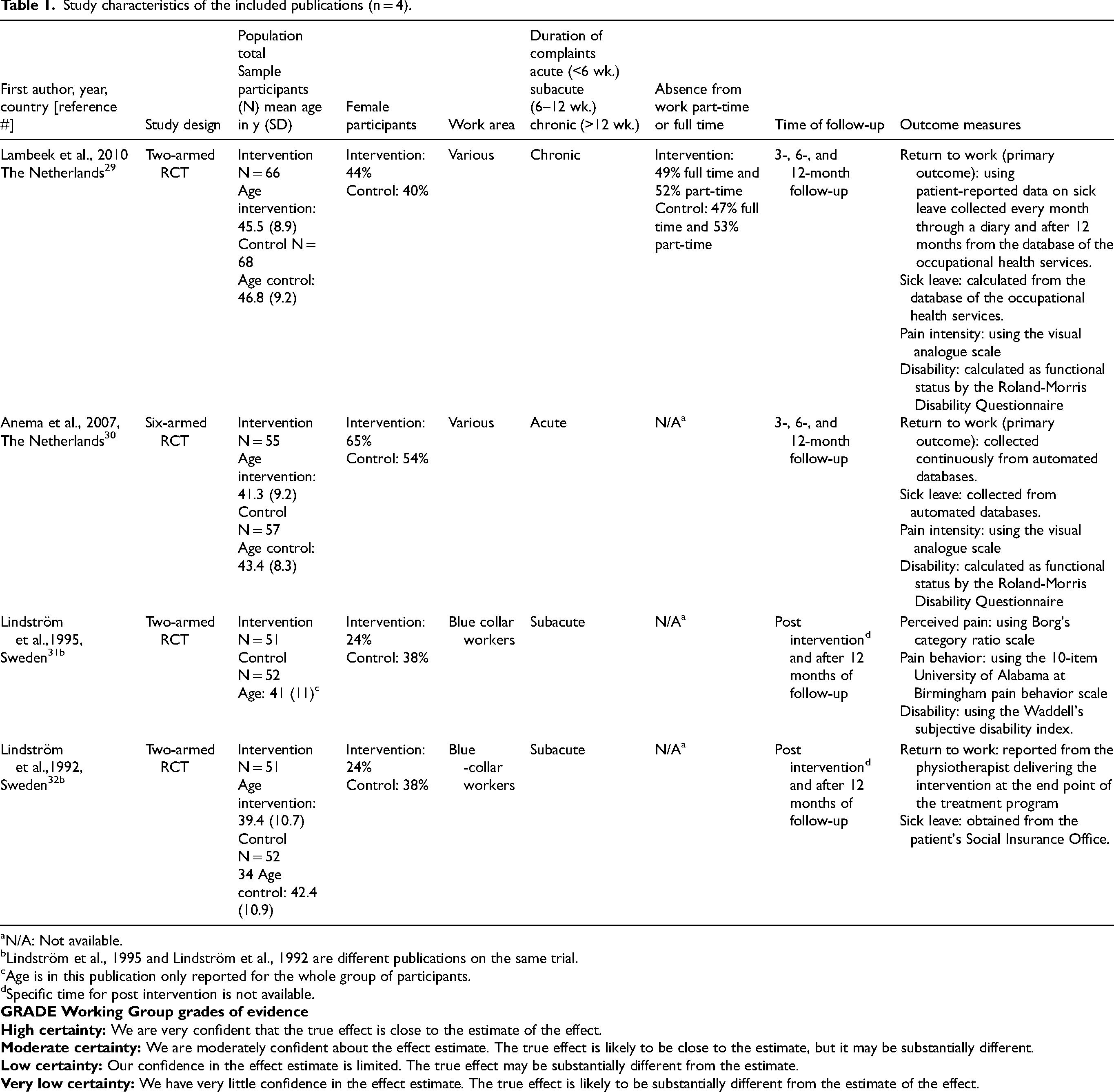
The characteristics of the included studies are presented in Table 1. All included studies focused on adults with non-specific LBP of subacute or persistent duration
Study characteristics of the included publications (n = 4).
N/A: Not available.
Lindström et al., 1995 and Lindström et al., 1992 are different publications on the same trial.
Age is in this publication only reported for the whole group of participants.
Specific time for post intervention is not available.
Across studies, return to work was the primary outcome in three of the four studies.29,30,32 However, definitions and measurement methods varied; return to work was measured as the duration of sick leave in calendar days from either the first day of sick leave 30 or randomization, 29 and as the time until a full return to the same or equivalent work for at least four consecutive weeks without recurrence. Sick leave was reported as the cumulative duration in days during the follow-up period. These variations in definitions and measurement methods limited comparability across studies and contributed to the decision not to conduct a meta-analysis.
Other outcomes included pain intensity, functional status or disability, and pain behavior, most of which were self-reported.29–31 None of the included studies assessed psychosocial or quality-of-life outcomes, thereby narrowing the biopsychosocial scope of the evidence base.
Description of the interventions
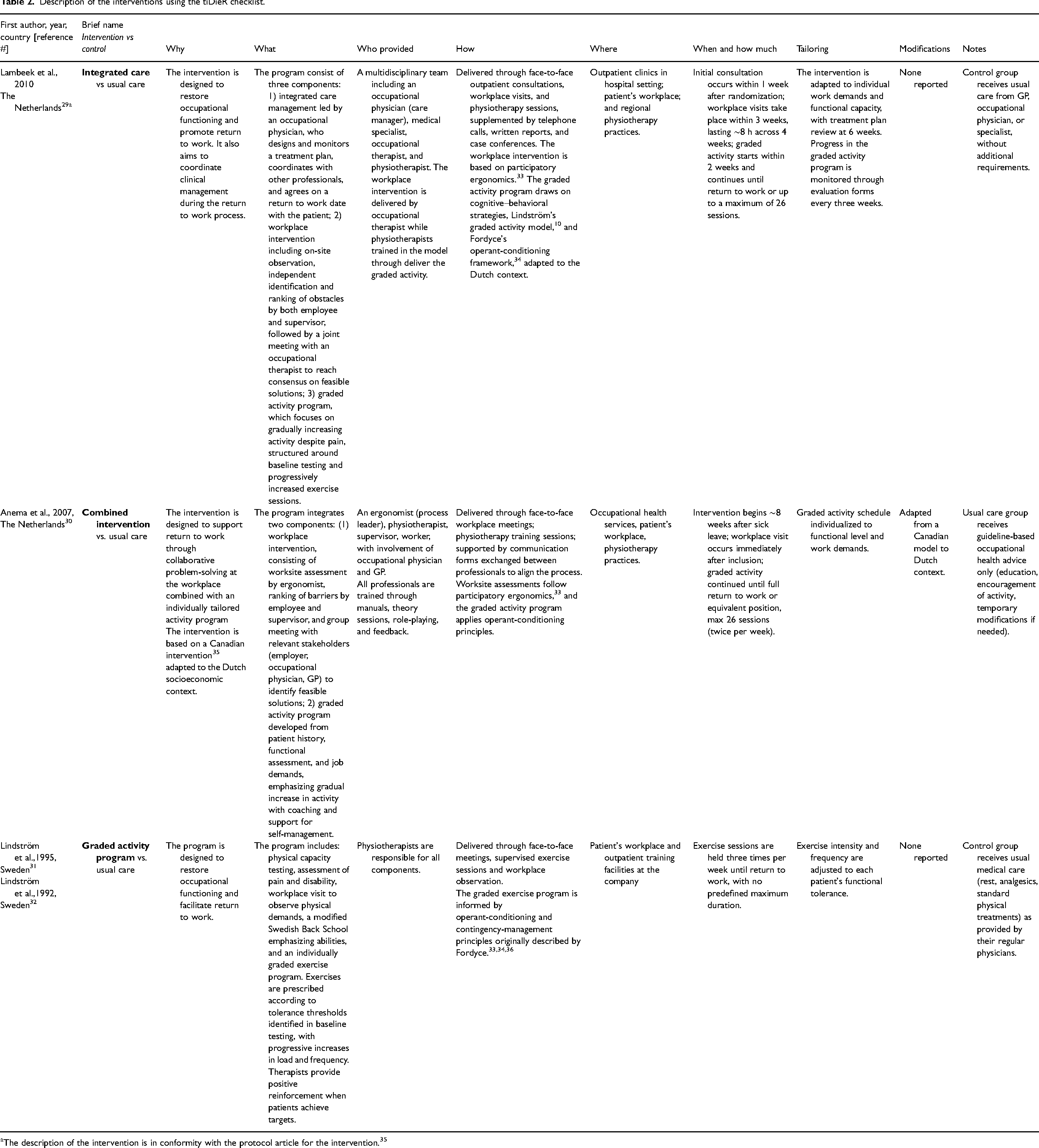
Table 2 presents a detailed description of the three included interventions using the TIDieR checklist. 24 Overall, the rehabilitation interventions included in the studies consisted of a workplace intervention in combination with an individual, gradually increasing exercise program.29–32 This integration of workplace strategies with the physical component of the biopsychosocial model was central to all included interventions. However, none of the interventions combined a workplace intervention with a psychological or social component of the biopsychosocial model.
Description of the interventions using the tiDieR checklist.
The description of the intervention is in conformity with the protocol article for the intervention. 35
A central part of the workplace intervention consisted of observation at the participants’ workplaces. This included assessing the physical work demands and identifying obstacles to return to work.31,32 For two interventions, this was supplemented by a collaborative process between the employee, supervisor/employer, and occupational physician to find possible solutions.29,30 The two studies from the Netherlands stated that the workplace intervention was based on “participatory ergonomics”.29,30 This approach emphasizes active participation and strong commitment from both workers and management in identifying workplace risk factors. 32
All included rehabilitation interventions incorporated a graded activity program tailored to the patient's capacity and work demands.29–32 The exercise programs typically consisted of two29,30 or three31,32 sessions a week, continuing until full return to work29–32 or up to the predefined maximum number of 26 sessions.29,30 All included interventions were based on cognitive behavioral principles.33,36 This approach utilized operant conditioning techniques, activity pacing, graded activity, cognitive strategies, social support to promote adaptive behaviors and self-management of pain.33,36
Multidisciplinarity was handled differently in the included interventions. One intervention was monodisciplinary, led solely by a physiotherapist.31,32 In other interventions, a multidisciplinary approach was used, involving occupational physicians, physiotherapists, occupational therapists, and general practitioners.29,30 Some interventions emphasized care management, either through a process leader 30 or integrated care management. 29
Study outcomes
Tables 3,4, and 5 summarize the results on outcomes regarding return to work, sick leave, pain, and disability of the included studies. One study showed a statistically significant faster return to work in the intervention group compared with the control group, 29 and another reported a borderline difference in the same direction. 32 For sick leave, two studies found a statistically significant reduction in total days of sick leave in the intervention group relative to the control group,29,32 whereas one study reported no between-group difference. 30 Across all studies, no significant between-group differences were observed for pain at any follow-up point, irrespective of the measurement method.29–32 For disability, two studies demonstrated statistically significant improvements in the intervention group compared with the control group at 12-month follow-up, while short- and medium-term differences were non-significant.31,32
Study outcomes: return to work and sick leave.
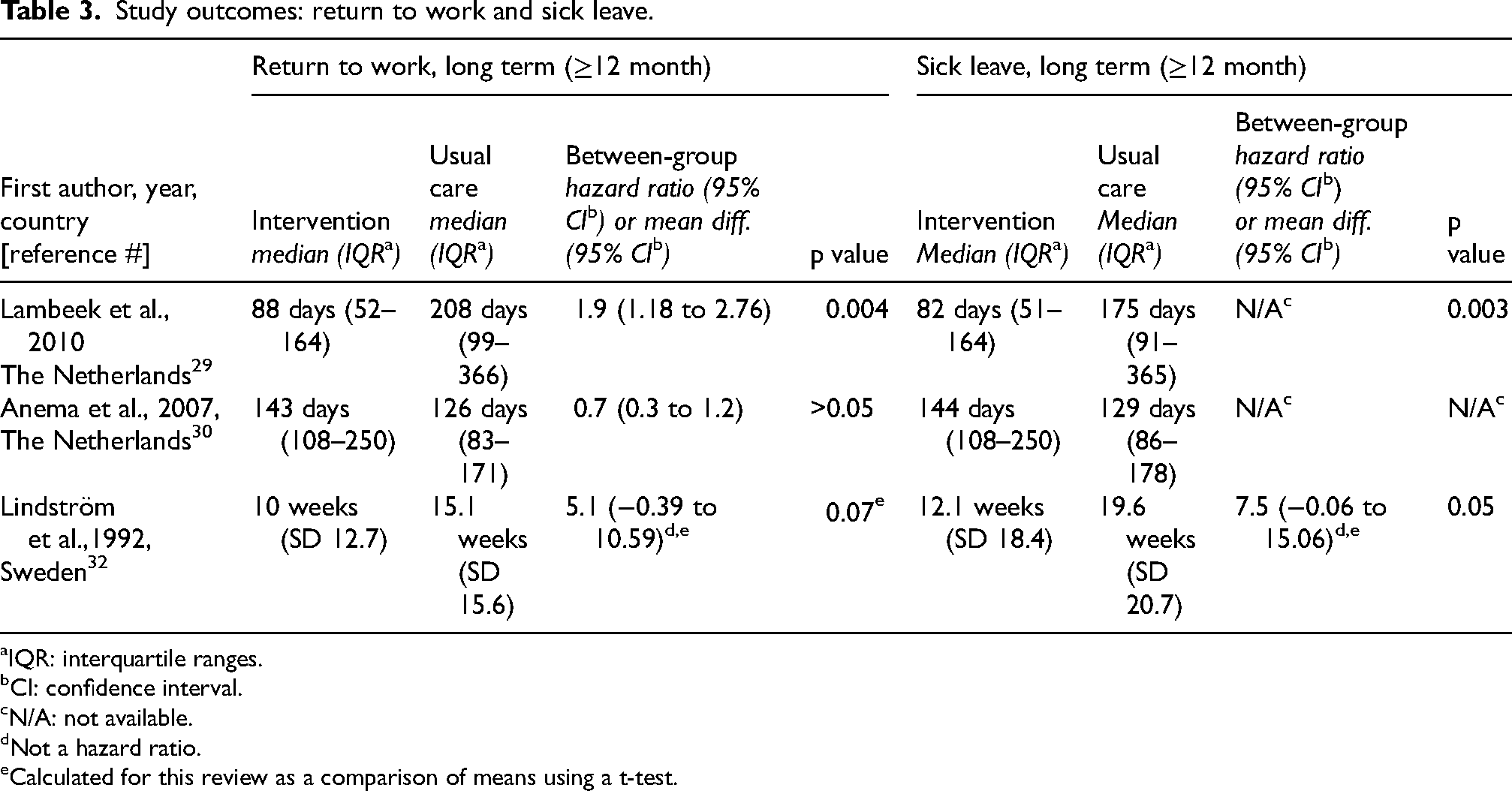
IQR: interquartile ranges.
CI: confidence interval.
N/A: not available.
Not a hazard ratio.
Calculated for this review as a comparison of means using a t-test.
Study outcomes: pain.
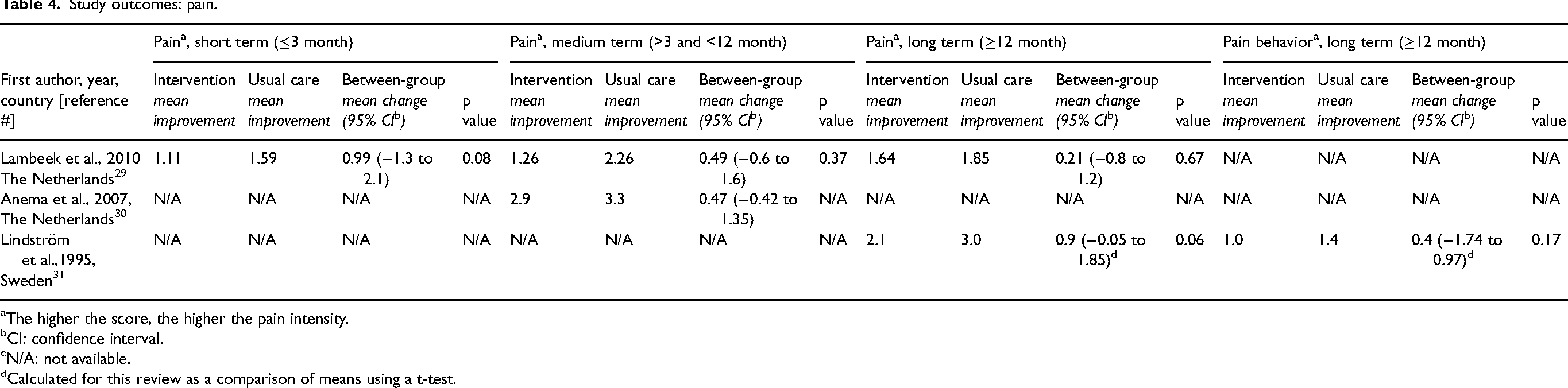
The higher the score, the higher the pain intensity.
CI: confidence interval.
N/A: not available.
Calculated for this review as a comparison of means using a t-test.
Study outcomes: disability.
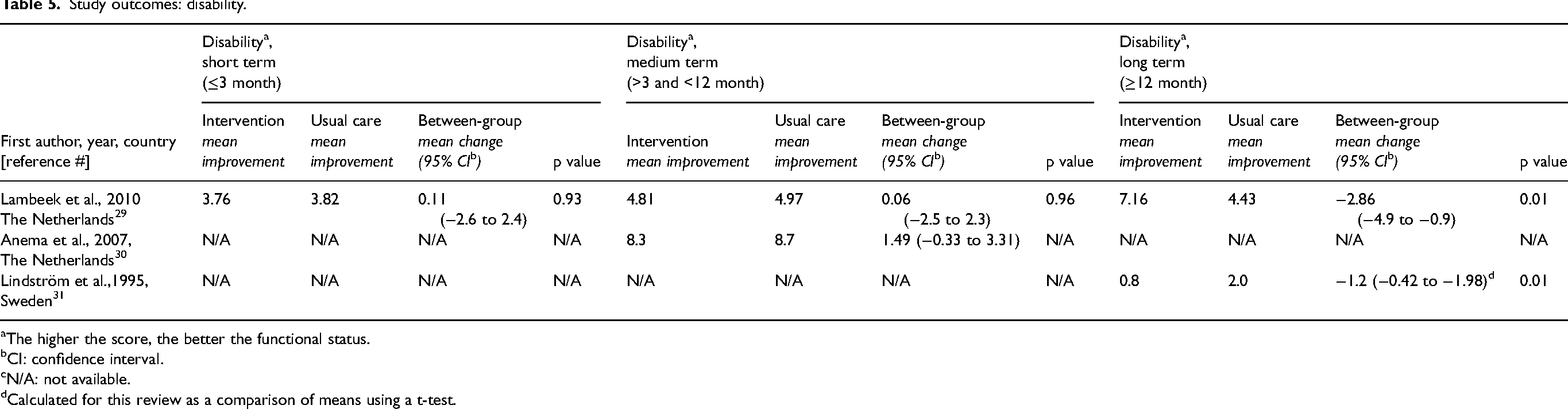
The higher the score, the better the functional status.
CI: confidence interval.
N/A: not available.
Calculated for this review as a comparison of means using a t-test.
In one study, 3 of 66 participants in the intervention group and 7 of 68 in the control group were lost to follow-up for return to work and sick-leave outcomes, and 8 and 9 participants, respectively, had missing pain and disability data at 12 months. 29 In two studies, register-based outcomes were available for all randomized participants,30,32 whereas patient-reported outcomes showed slightly lower follow-up (Anema: 51/55 and 54/57 30 ; Lindström: 49/51 and 49/52 31 ). These patterns of attrition should be considered when interpreting the magnitude and certainty of long-term effects.
Risk of bias analysis
Figure 2 summarizes the risk of bias assessments for each outcome. Overall, the analysis indicated a low risk of bias regarding return to work outcomes. However, there were some concerns about potential bias in the measurement of sick leave, pain, and disability, primarily because these outcomes were gathered using self-reported instruments. One study was assessed as having a high risk of bias regarding measuring perceived pain. 31
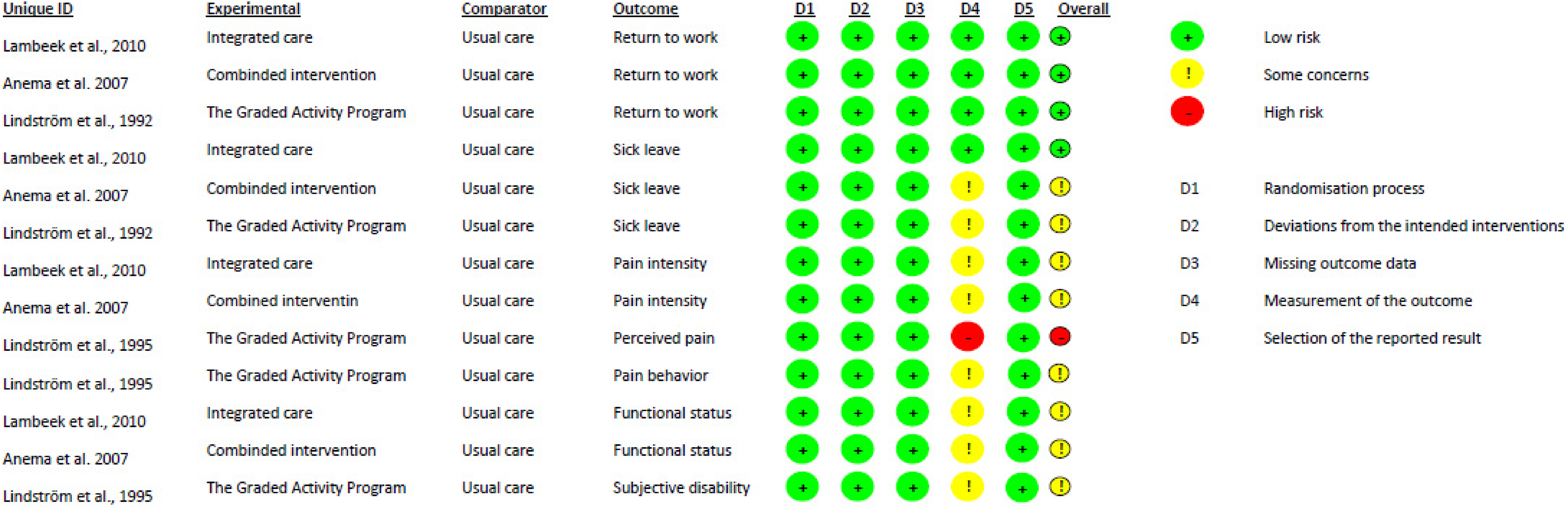
Cochrane risk of bias analysis for each outcome in the included studies.
Evidence synthesis
Table 6 presents a summary of the findings from the evidence synthesis. Overall, the certainty of evidence was generally low or very low. For long-term disability, the certainty of the evidence was rated moderate. Although the GRADE assessment resulted in a moderate rating, this conclusion is based on only two studies, which introduces some uncertainty. The available evidence therefore suggests a possible improvement in disability over time for individuals on sick leave due to LBP who received a rehabilitation intervention integrating workplace intervention with other biopsychosocial components.
Summary of findings regarding evidence synthesis.
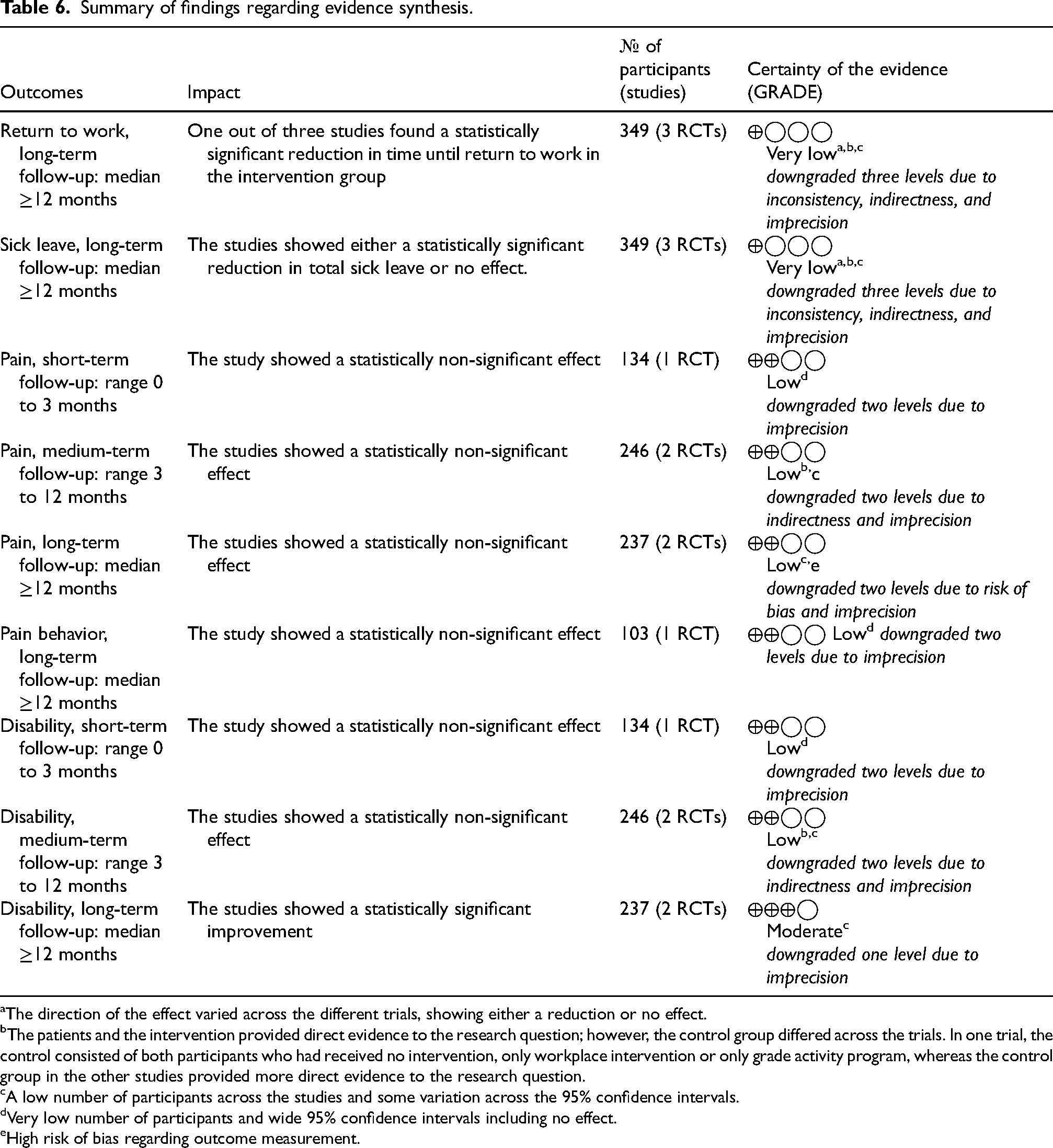
The direction of the effect varied across the different trials, showing either a reduction or no effect.
The patients and the intervention provided direct evidence to the research question; however, the control group differed across the trials. In one trial, the control consisted of both participants who had received no intervention, only workplace intervention or only grade activity program, whereas the control group in the other studies provided more direct evidence to the research question.
A low number of participants across the studies and some variation across the 95% confidence intervals.
Very low number of participants and wide 95% confidence intervals including no effect.
High risk of bias regarding outcome measurement.
The quality of evidence was downgraded primarily due to imprecision and indirectness. For outcomes related to work status (return to work and sick leave), there was inconsistency in the results across the studies, which impacted the certainty of the evidence.
Discussion
This review provides the first systematic synthesis of biopsychosocial rehabilitation programs that explicitly integrate workplace interventions for employees on sick leave due to LBP. Although biopsychosocial rehabilitation is widely recommended for LBP and shows moderate evidence for effects on pain and disability, the contribution of work-related components remains insufficiently understood due to variation in how such interventions are defined, delivered and clinically implemented.
Only four studies met the inclusion criteria,29–32 representing three unique interventions. All interventions combine a workplace component with an individually tailored exercise program. None integrated a workplace intervention with psychological or social components of the biopsychosocial model. Across these studies, the certainty of evidence was low or very low for pain, return to work, and sick leave, whereas moderate-quality evidence indicated improvements in long-term disability. Previous systematic reviews have investigated the effectiveness of either multidisciplinary biopsychosocial rehabilitation or workplace interventions separately. Consistent with our findings, the Cochrane review by Kamper et al. (2014) found moderate-quality evidence that multidisciplinary biopsychosocial rehabilitation improves disability in patients with chronic LBP over time. 14 However, they found low-quality evidence for pain reduction, regardless of follow-up duration. 14 These findings were confirmed in WHO's updated review from 2023, 11 which builds on the work by Kamper et al. (2014). 14 In contrast, a systematic review by Russo et al. found high- or moderate-quality evidence of workplace interventions on pain, disability, and fear-of-avoidance beliefs in employees with LBP. 20 Yet, none of these previous systematic reviews demonstrated strong evidence for improving work outcomes such as return to work or sick leave.11,14,20 This aligns with our findings, which show very low-quality evidence for these work-related outcomes.
However, a Cochrane review by van Vilsteren et al. (2015) has demonstrated moderate- to high-quality evidence that workplace interventions can reduce the time to return to work and the duration of sick leave. 18 These inconsistencies may reflect differences in study populations, as van Vilsteren et al. included a wider range of musculoskeletal disorders, not exclusively focusing on patients with LBP. 18
One explanation for the limited evidence observed in our review is the small number of published studies within the specific field. Nonetheless, when considered alongside previous systematic reviews, our findings suggest that multidisciplinary biopsychosocial rehabilitation, with or without a workplace component, may contribute to improvements in disability and pain. However, the lack of consistent effects on return to work and sick leave suggests that the occupational component of the biopsychosocial approach requires more targeted development, implementation and evaluation. This is supported by Williams et al. (2007), who found significant variation in the design, content, and delivery of workplace programs, complicating cross-study comparisons. 19 This aligns with Kokkonen et al. (2024), who emphasized that implementation of workplace collaboration in occupational health services remains inconsistent, limiting opportunities for robust evaluations and generalizable findings. 37 A qualitative research by Dionne C et al. (2012) shows that employees suffering from back pain perceive occupational factors, such as being understood by their employer, as essential for their return to work process. 38 Such psychosocial and relational factors are difficult to address through physical rehabilitation alone.
Table 2 presents a detailed overview of the included interventions, showing an apparent similarity among the three unique interventions, all of which combine a workplace intervention with a physical element described as a graded activity program.29–32 The physical focus in the included studies appears somewhat unidimensional. In light of current guidelines, this may reflect the ongoing shift in LBP management, which increasingly emphasizes the need for a broader integration of psychological and social components alongside physical care.11–13 Two of the included interventions utilized participatory ergonomics as the foundation of the workplace intervention.29,30 Yet, when considering multidimensional phenomena like LBP, the effectiveness of such traditional ergonomics and other unidimensional solutions has been questioned. 20 It appears that components beyond the physical rehabilitation, particularly those addressing psychosocial functioning, are important for achieving meaningful improvements in disability and work status.13,39
Despite the growing recognition of the complexity of LBP management, it has historically been dominated by a more biomedical model. 10 Many people with LBP report difficulties in maintaining their social roles and managing daily activities at home, yet the psychosocial aspects of LBP are still poorly addressed in rehabilitation.40,41 For the included interventions, cognitive behavioral principles were exclusively applied within the physical activity program, without addressing any psychosocial issues.29–32
A meta-synthesis of qualitative studies by Froud et al. (2014) emphasized that living with LBP can have “life-changing” consequences affecting work identity, relationships, social roles and emotional well-being, while also generating concerns about the future. 42 Other studies indicate that individuals living with LBP find it challenging to carry out household chores or engage in social activities due to pain and fatigue, which force them to prioritize their energy.40,43 The additional effort required to manage everyday life at home and engage in social activities may impair their ability to effectively manage their work life. This highlights the importance of incorporating a broader biopsychosocial framework that supports individuals across all aspects of their lives.
Such a biopsychosocial framework requires structured assessment, interdisciplinary teamwork, and a shared understanding of the person's rehabilitation needs and goals.44–47 Yet, among the interventions included in the current review, the level of interdisciplinary teamwork varied significantly. Some interventions relied solely on a monodisciplinary delivery by physiotherapists,31, 48 while others made only limited mention of a “process leader”. 30 In contrast to the other interventions, Lambeek et al. (2010), provided a more comprehensive description of “integrated care management”, including clear interdisciplinary roles. 29 Notably, this study reported promising results on return to work, reducing sick leave, and disability. 29
The findings of this review, in particular the limited certainty of evidence for most outcomes and the substantial variation in how interdisciplinary teamwork was incorporated across interventions, suggest that current programs do not fully reflect a biopsychosocial rehabilitation approach. Future rehabilitation programs for employees on sick leave due to LBP should emphasize interdisciplinary teamwork and comprehensive integration of psychological and social components. Only then can rehabilitation fully reflect the biopsychosocial complexity of LBP to include meaningful support for navigating everyday life at work and at home.
Strengths and limitations
The main strength of the present study lies in its unique focus on biopsychosocial rehabilitation programs that explicitly integrate workplace components. This distinguishes the review from previous syntheses examining either biopsychosocial rehabilitation or workplace interventions in isolation and highlights a clear research gap regarding how workplace strategies are integrated within multidisciplinary rehabilitation.
Methodologically, the review followed a well-defined protocol and systematic approach using a throughout the review process. The review employed a comprehensive literature search conducted with assistance from an expert librarian and was based on two previous systematic Cochrane reviews.14,18 Another strength is the use of the TIDieR checklist to ensure a detailed and transparent description of the included interventions. This thorough description of the interventions enhances the interpretation of the results and supports the transferability to clinical practice.
By focusing on a specific population, i.e., employees on sick leave due to non-specific LBP with subacute or persistent symptoms, the review achieved a relatively homogeneous study population, which strengthens the clinical relevance of the findings. However, this homogeneity is relative, given the small number of studies and remaining variability in pain duration and work sectors. The findings cannot be generalized to acute LBP or to specific spinal conditions. Despite the narrow definition of the population, some degree of heterogeneity remained, particularly in terms of work area and duration of pain. A broader population definition, encompassing all patients with LBP or other musculoskeletal disorders, might have increased the number of eligible studies and offered a more comprehensive understanding of the effectiveness of rehabilitation interventions integrating workplace strategies with other biopsychosocial elements. However, such a broader definition would likely have introduced an even higher degree of population heterogeneity, reducing the specificity of the review's conclusions.
Language restrictions also represent a potential limitation. Only studies reported in English, Danish, Norwegian and Swedish were included, which may have led to the exclusion of relevant studies in other languages.
Additionally, the included studies span nearly 3 decades, from 1992 to 2010.29–32 The lack of recent studies is surprising given the evolving understanding of the multifactorial causes of LBP. 11 This development may have influenced the content provided to the control group. Notably, all three included trials described the control conditions as adhering to applicable guidelines for LBP treatment. Still, the generalizability of the findings may be limited to high-income countries with similar healthcare systems.
In addition, the absence of psychosocial or quality-of-life outcomes in the included studies limits the comprehensiveness of the biopsychosocial perspective. Combined with variation in how “return to work” and “sick leave” were defined and measured, these gaps constrain the ability to determine the effectiveness of integrated workplace interventions.
A clear limitation of this review is the restricted evidence base. Only four studies were eligible, which constrains the ability to explore heterogeneity between interventions or to conduct subgroup analyses. In contrast, the Cochrane reviews by Kamper et al. (2014) and van Vilsteren et al. (2015) were supported by substantially larger evidence bases that allowed subgroup analyses to address heterogeneity.14,18 In the present review, such analyses were not feasible.
Similarly a formal meta-analysis was not conducted due to the nature of the available data. The included studies reported outcomes using different summary measures, with most presenting medians and interquartile ranges (IQRs) rather than means and standard deviations (SDs). These distributions were clearly right-skewed. Although statistical methods exist to estimate means and SDs from medians and IQRs, such transformations rely on assumptions of normality that were not met in this case. Furthermore, in studies that reported means and standard deviations (SD), the data were also skewed, raising concerns about validity and interpretability. To avoid introducing bias through inappropriate statistical pooling, we chose to present the results descriptively.
A meta-analysis would have been both feasible and informative if sufficient comparability across datasets had been present, as it could have increased statistical power, improved the precision of effect estimates, and enabled visual presentation through forest plots. Although the absence of a meta-analysis restricts the quantitative synthesis, it does not undermine the overall validity or transparency of the review.
Finally, the possibility of publication bias should be mentioned as studies with positive outcomes, in general, are more likely to be published. Although at least one included study reported non-significant findings, the potential for publication bias cannot be ruled out. These limitations should be considered when interpreting the findings results.
Future research
This review highlights the evidence gap regarding multidisciplinary rehabilitation interventions combining a workplace intervention with other biopsychosocial components. There is an evident need to develop and evaluate interventions that target a broader perspective of biopsychosocial rehabilitation for employees on sick leave due to LBP. Future research should adopt a more comprehensive view of the target population's rehabilitation needs, ensuring that interdisciplinary teamwork is fully integrated and sustained throughout the entire rehabilitation process. When developing such interventions, it is essential to focus on understanding the mechanisms through which the interventions will improve both work outcomes and the everyday lives of people living with LBP.
Conclusion
Moderate evidence suggests that biopsychosocial rehabilitation including workplace interventions can improve long-term disability for people on sick leave due to LBP. However, this conclusion is based on only two studies and should therefore be interpreted with caution. Furthermore, the evidence is limited to low or very low regarding the effect on pain, return to work, and sick leave. This review shows that the evidence for ensuring workplace interventions in multidisciplinary biopsychosocial rehabilitation is still in its early stages, particularly concerning the combination of workplace strategies with psychological and social components. Further research is needed to enhance our understanding of effective approaches to support individuals with LBP in their everyday lives.
Supplemental Material
sj-pdf-1-wor-10.1177_10519815261423506 - Supplemental material for Effectiveness of multidisciplinary biopsychosocial rehabilitation including workplace interventions for employees on sick leave due to low back pain: A systematic review
Supplemental material, sj-pdf-1-wor-10.1177_10519815261423506 for Effectiveness of multidisciplinary biopsychosocial rehabilitation including workplace interventions for employees on sick leave due to low back pain: A systematic review by Katrine Schilling Andersen, Anne Petrea Hansen, Pernille Pedersen, Vivian Langagergaard, Claus Vinther Nielsen, Claus Løvschall and Marc Sampedro Pilegaard in WORK
Footnotes
Acknowledgements
The authors would like to thank Aarhus University, the Department of Social Medicine and Rehabilitation at Gødstrup Hospital, and DEFACTUM for supporting this study. The authors also thank librarian Helene Sognstrup for assistance with the literature search and emeritus Morten Pilegaard for specialized editing support.
ORCID iDs
Ethical approval
Not applicable. This study is a systematic review based exclusively on published literature and did not require ethical approval.
Informed consent
Not applicable. This study did not involve human participants or the collection of primary data.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.