
Abstract
Background
Textile spinning mill workers are exposed to airborne cotton dust and particulate matter, which are associated with respiratory symptoms and impaired lung function.
Objective
This study aimed to evaluate the prevalence and severity of respiratory symptoms among textile spinning mill workers and to assess the impact of occupational dust exposure on pulmonary function.
Methods
A cross-sectional study was conducted among 180 textile spinning mill workers. Data were collected using a structured questionnaire to assess respiratory symptoms and through pulmonary function tests to evaluate lung function. Indoor air quality was monitored by OIZOM Polludrone to measure particulate matters (PM2.5 and PM10 concentrations), which were compared to permissible thresholds.
Results
The study found that the levels of PM2.5 and PM10 in the textile spinning mills were much higher than the recommended limits, averaging 186.02 µg/m3 for PM2.5 and 826.66 µg/m3 for PM10. The results showed a high rate of respiratory problems among workers. About 15–20% had byssinosis, 10–12% had chronic bronchitis, and 8–10% had asthma.
Conclusion
Many workers also reported frequent coughing, chest tightness, and shortness of breath. Pulmonary function tests indicated reduced lung function in workers exposed to cotton dust. Key measures like FEV1 and FVC were lower than normal, and the FEV1/FVC ratio suggested obstructive lung conditions. The study highlights the severe respiratory health risks associated with cotton dust exposure in textile spinning mills. The findings emphasize the need for improved occupational health and safety measures to reduce dust exposure and protect worker health.
Keywords
Introduction
Occupational lung disease represented a significant concern in occupational health, being identified as one of the primary issues impacting workers globally. 1 Rapid industrialization and inadequate pollution control measures had exacerbated indoor air pollution, particularly in emerging nations. 2 A key factor contributing to the rise in indoor air pollution was the lack of awareness regarding its harmful effects on human health. 3 Respiratory disorders had increasingly become a critical issue in various industrial sectors, especially in environments with high airborne pollutants. 4 Occupational respiratory diseases remain a significant global public health concern, particularly in industries involving exposure to organic dust such as the textile sector. Textile workers are routinely exposed to cotton dust, endotoxins, fibers, and airborne particulate matter generated during bale opening, carding, drawing, roving, and textile spinning processes. 5 Chronic inhalation of cotton dust has long been recognized as a cause of respiratory morbidity, most notably byssinosis (brown lung disease), as well as chronic bronchitis, asthma-like symptoms, chronic obstructive pulmonary disease (COPD), and both obstructive and restrictive lung impairment. 6 The textile spinning mill, involving the processing of raw fibers into yarn, was particularly affected by dust and particulate matter exposure. This exposure was a known risk factor for respiratory health issues, including chronic bronchitis, asthma, and reduced lung function. 7 Low awareness about dust exposure was also a reason for unsafe working condition. 8 Despite advances in industrial hygiene and safety measures, the prevalence of these respiratory symptoms among textile workers remained a pressing concern. 9 This issue was particularly acute in the textile spinning industry, where substantial quantities of cotton dust were generated. In textile spinning mills across India, inadequate dust control measures and poor ventilation systems exposed workers to high levels of cotton dust for 8 to 10 h daily. Such exposure led to the accumulation of dust in the pulmonary system, resulting in respiratory and occupational lung disorders.10,11
The traditional textile spinning industry in India, which attracted unskilled labor from rural areas, posed significant health risks due to its labor-intensive nature. Despite its importance, the health hazards associated with this sector were often underestimated compared to other industries. 12 Workers, frequently illiterate and uninformed about health and safety standards, faced substantial risks exacerbated by management's lack of emphasis on occupational health and safety (OHS). 13 These conditions contributed to severe respiratory health issues, including worsened respiratory and cardiovascular disorders, lung tissue damage, and increased mortality rates. 3 The textile spinning process involved multiple stages—carding, textile spinning, and weaving—that generated substantial amounts of dust. This dust, comprised of fibers, contaminants, and chemical residues, contributed to poor air quality in the workplace, leading to the inhalation and deposition of particles in the respiratory tract. 14 Long-term exposure to such an environment posed a significant risk to workers’ respiratory health, potentially resulting in chronic conditions that affected their quality of life and productivity. 15
Byssinosis is considered the classical occupational lung disease of textile workers and is characterized by chest tightness, breathlessness, and progressive airflow limitation associated with cotton dust exposure. 16 The meta-analyses conducted in India showing a pooled byssinosis prevalence of approximately 24%, highlighting the substantial occupational health burden among Indian textile workers. However, beyond byssinosis, textile workers frequently report chronic cough, wheezing, phlegm production, dyspnea, and reduced lung function parameters such as forced expiratory volume in one second (FEV1) and forced vital capacity (FVC). These symptoms reflect both inflammatory and fibrotic responses of the respiratory system to sustained dust exposure. 17 The textile industry involved several processes: yarn formation (textile spinning), fabric formation (weaving), wet processing, and fabrication. 18 Among these, the textile spinning sector, which included stages such as bale opening, blowing, carding, drawing, and ring framing, generated the highest levels of cotton dust. 19 Although advancements in dust control had reduced byssinosis prevalence in developed countries, the situation remained severe in developing nations. Studies from the United Kingdom had shown varying byssinosis prevalence rates among different job roles within the textile sector, while developing countries continued to experience higher rates of respiratory diseases. 20
The most recent evidence of high methodological rigor, based on a systematic review undertaken by Nafees et al. (2022) that summarized the evidence of 26 individual studies in 12 low- and middle-income countries, suggests that the prevalence of byssinosis among textile workers is 8 −38%, the prevalence of airflow obstruction is 10 −30%, and the prevalence of chest tightness is up to 58%. More importantly, the review showed that there was a strong positive correlation between the levels of cotton-dust exposure and prevalence of byssinosis (r of 0.72), which proves the existence of a definite exposure-response relationship. 21 Moreover, in a study by Nafees et al. (2023) focusing on a MultiTex trial, over 2000 textile workers were recruited, and it was determined that 56 per cent of respondents had at least one respiratory symptom, and that there was a significant association between dust-exposure levels, years of employers, and indicators of impaired pulmonary ability. These findings confirm that occupational respiratory disease remains a substantial and ongoing burden in textile industries, particularly in low- and middle-income countries. 16 For instance, an Ethiopian study reported byssinosis prevalence rates as high as 53.2% among blowers and 47.5% among carders, with significant instances of bronchial asthma. 22 Similarly, research from China and other developing countries highlighted high prevalence rates of byssinosis and related respiratory conditions. 23
The prevalence of respiratory symptoms among textile workers worldwide often exceeds 50%, but there is significant variability depending on the concentration of dust in the air, duration of exposure, and whether other occupational safety measures are implemented. 16 The prevalence of byssinosis has decreased dramatically in high-income countries, where engineering controls and dust regulation have been implemented. 24 In contrast, the developing world still has much higher prevalence numbers owing to poor ventilation systems, minimal adherence to safety regulations and inconsistent use of personal protective equipments. 21 India, one of the world's biggest textile producers, has millions of workers in its textile spinning and weaving industries. In India, studies reported varying rates of respiratory conditions among textile spinning mill workers, with byssinosis ranging from 8 to 15%, chronic bronchitis or asthma at 3.6%, and poor lung function between 20 to 38%. 25 A study from Maharashtra noted that 57–78% of cotton-ginning employes experienced chest tightness, 52–65% had chest pain, and 37–45% frequently coughed. 26 Despite these findings, comprehensive data on respiratory issues and pulmonary function among Indian textile spinning mill workers remained limited. A recent study from Tamil Nadu revealed PM2.5 and PM10 concentrations in textile spinning mills were 186.02 µg/m3 and 826.66 µg/m3, respectively. 3 Several studies have also reported high prevalence of chronic bronchitis, asthma-like symptoms, and reduced lung function among cotton-exposed workers, indicating a significant occupational health burden within the country.21,27
Several epidemiological studies have shown a dose–response relationship between exposure to cotton dust and reduction in pulmonary function. 24 Longer duration of employment and higher dust concentration are linked to progressively lower FEV1, FVC, and FEV1/FVC ratio. 28 Longitudinal studies additionally show that the annual decline in lung function is more rapid for cotton-exposed workers than for unexposed controls, indicating cumulative and potentially irreversible respiratory damage. These findings are consistent with the biological plausibility that cotton dust–induced inflammation, oxidative stress and structural changes to the lung result in chronic respiratory disease.13,29 Despite the extensive literature documenting respiratory symptoms and byssinosis prevalence, significant knowledge gaps still exist. First, previous studies have mostly used self-reported symptom-based measurement without objective indoor air quality monitoring. Second, little is known about real-time particulate matter concentrations (PM2.5 and PM10), respiratory symptoms, and spirometry assessments of pulmonary function in the same occupational context. Third, the existing contemporary data from Indian textile spinning mills that triangulate environmental exposure assessment with valid respiratory questionnaires and spirometry is sparse.
Thus, the current study attempts to fill these gaps in knowledge by exploring a comprehensive analysis of indoor air quality and its association with respiratory health among workers in textile spinning mills in Tamil Nadu, India. In particular, this study aims to (i) quantify PM2.5 and PM10 (i) concentrations at discrete sections of the textile spinning mill, (ii) prevalence and severity of respiratory symptoms using validated questionnaires and (iii) spirometric pulmonary function impairment. By integrating environmental monitoring with clinical assessment, this study provides a more robust evaluation of occupational respiratory risk and contributes to strengthening evidence-based occupational health interventions in textile industries.
Methodology
Study design
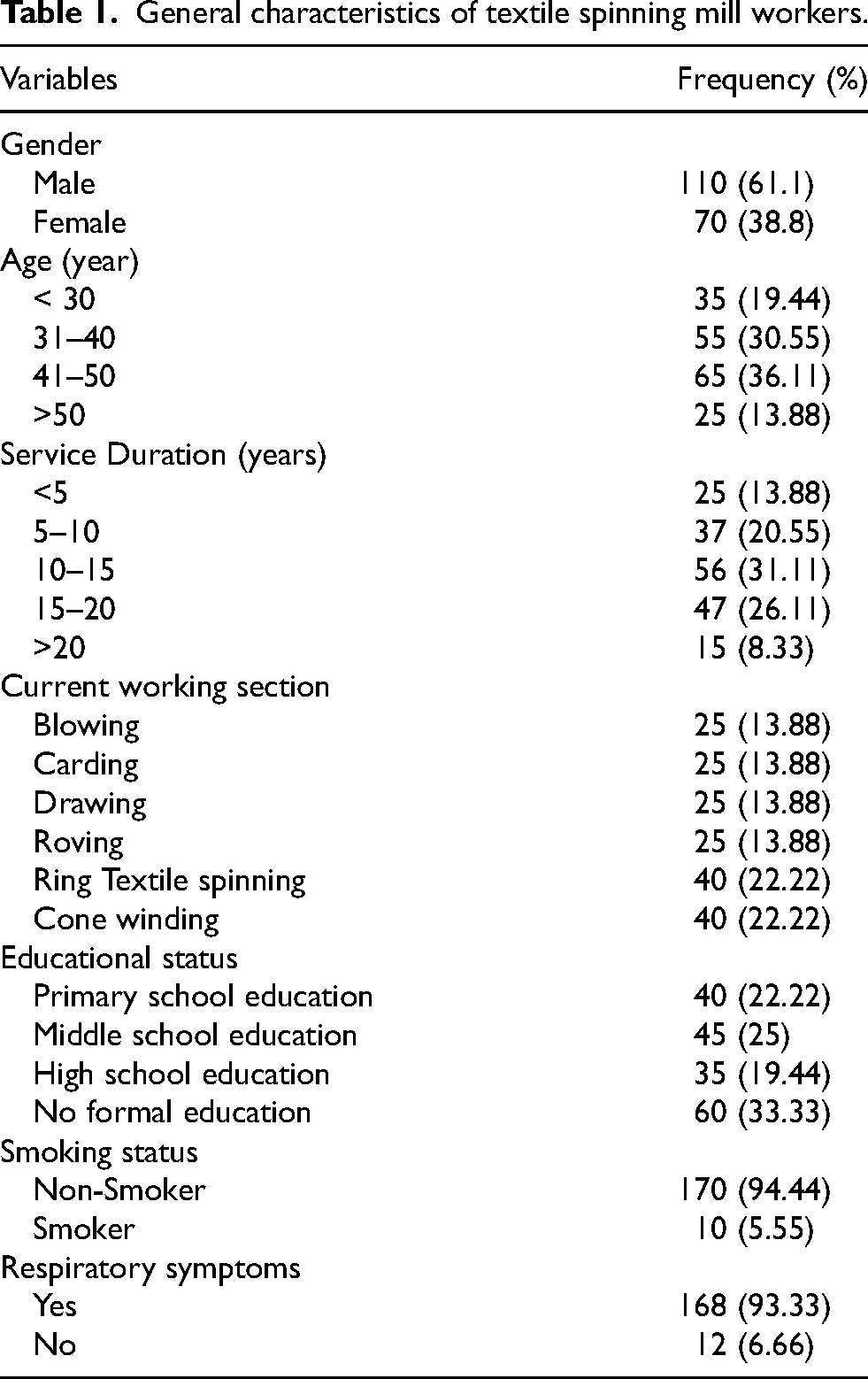
This cross-sectional study was conducted in the textile spinning unit of the textile industry in Erode district at Tamil Nadu state of INDIA. The study population consisted of 180 workers with a minimum of three years of experience in the textile spinning mill sector. The general characteristics of textile spinning mill workers is shown in Table 1. Data was collected through a combination of surveys and pulmonary function tests conducted at a single point in time, allowing for an assessment of the prevalence of respiratory symptoms and the extent of lung function impairment. However, participants who had recently had treatment for any respiratory ailment, chronic lung infections, persistent coughs, heart conditions, or thoracic surgery were excluded in this study.
General characteristics of textile spinning mill workers.
Indoor air quality measurements
The indoor air quality (IAQ) was investigated by using an OIZOM Polludrone (OIZOM Limited, Gujarat, India) 28 across six sections of the textile spinning mill: cone winding, ring textile spinning, roving, drawing, carding, and blowing. PM2.5 and PM10 concentrations were monitored to assess exposure levels to fine and coarse particulate matter. The monitoring device was positioned at worker breathing zone height (approximately 1.5 m above floor level) to represent occupational exposure. Continuous measurements were recorded for 15–30 min at each location. Multiple readings were obtained at each workstation and repeated across different time periods to account for exposure variability. Average values were calculated to represent exposure levels. The study utilized descriptive statistics to present the mean, median, standard deviation, and range of particulate matter concentrations in each section were used to represent the monitoring setup, the average concentration levels, and the variability across different sections. The IAQ results were compared with National Ambient Air Quality Standards (NAAQS) and WHO (World Health Organization) standards to evaluate compliance and potential health risks. 30 According to WHO guidelines, the recommended limits are 15 µg/m3 for PM2.5 and 45 µg/m3 for PM10 (24-h average). The Indian CPCB standards specify limits of 60 µg/m3 for PM2.5 and 100 µg/m3 for PM10. 31
Questionnaire based data collection on respiratory symptoms
For the data collection on respiratory symptoms, a structured questionnaire based on British Medical Research Council questionnaire's and American Thoracic Society's standard.27,28 The questionnaire was designed to gather detailed information on the respiratory health of textile spinning mill workers. It will include questions regarding the frequency, duration, and severity of respiratory symptoms such as coughing, wheezing, shortness of breath, chest tightness, and phlegm production. The questionnaire will also capture information on the onset of symptoms and any temporal variations, such as symptoms worsening during specific work shifts or after exposure to certain materials. To ensure comprehensive data collection, the questionnaire will incorporate both closed-ended and open-ended questions, allowing for quantitative analysis and qualitative insights. Additionally, the questionnaire will include sections on the workers’ medical history, smoking habits, occupational history, and exposure to potential respiratory irritants both inside and outside the workplace. This approach will enable us to correlate the presence and severity of respiratory symptoms with various risk factors and environmental exposures, facilitating a detailed assessment of respiratory health status among the study population.
Pulmonary function test
For this study, pulmonary function tests (PFTs) were conducted by spirometry to assess the respiratory health of the textile spinning mill workers. The PFTs were performed using a standardized spirometer,27,28 which measured various aspects of lung function, including forced vital capacity (FVC), forced expiratory volume in one second (FEV1), and the FEV1/FVC ratio. These parameters were critical in diagnosing and evaluating the severity of obstructive and restrictive lung diseases. The procedure was carried out in a controlled environment following the American Thoracic Society (ATS) guidelines to ensure accuracy and consistency. Each participant was instructed to perform a maximal inhalation followed by a rapid and forceful exhalation into the spirometer. To minimize variability, each participant was given detailed instructions and allowed a practice attempt before the actual test. At least three acceptable maneuvers were recorded for each participant to ensure reproducibility, with the best effort being used for analysis
Statistical analysis
Statistical analysis was conducted to examine the association between these symptoms and various factors such as age, working section, work experience, and education level. The analysis also utilized logistic regression to determine factors significantly associated with the presence of respiratory symptoms, presenting the results in terms of odds ratios (OR) and confidence intervals (CI).
Results
Socio-demographics characteristics of textile spinning mill workers
This cross-sectional study was conducted in the textile spinning unit of the textile industry in Erode district at Tamil Nadu state of INDIA. The study population consisted of 180 workers with a minimum of three years of experience in the textile spinning mill sector. The textile spinning mill consists of blowing, carding, drawing, roving, ring textile spinning, and cone winding sections. The study comprised 180 participants, with a majority being male (61.1%, n = 110) compared to females (38.8%, n = 70). The mean height of the participants was 168 cm (SD = 5.8 cm), and the mean weight was 68 kg (SD = 4.56 kg). The age distribution indicated that 19.44% of the participants were under 30 years old, 30.55% were between 31–40 years, 36.11% were between 41–50 years, and 13.88% were over 50 years. Regarding service duration, 13.88% had less than 5 years of service, 20.55% had between 5 to 10 years, 31.11% had between 10 to 15 years, 26.11% had between 15 to 20 years, and 8.33% had more than 20 years of service. Participants were distributed across various working sections, with 13.88% in Blowing, 13.88% in Carding, 13.88% in Drawing, 13.88% in Roving, 22.22% in Ring Textile spinning, and 22.22% in Cone Winding. Educational status varied among participants, with 22.22% having primary school education, 25% having middle school education, 19.44% having high school education, and 33.33% being illiterate. Smoking status revealed that a large majority were non-smokers (94.44%), while a small percentage were smokers (5.55%). Notably, 93.33% of participants reported experiencing respiratory symptoms, leaving only 6.66% without such symptoms.
Investigation of indoor air quality in textile spinning mill
The investigation of indoor air quality was conducted in six sections of textile spinning mill such as cone winding, ring textile spinning, roving section, drawing section and blowing section. The descriptive statistics of PM2.5 & PM10 concentrations at various sections in textile spinning mill is shown in Table 2. The PM2.5 levels were highest in the Cone Winding section, with a mean of 104.96 µg/m3 and a maximum of 197.62 µg/m3, indicating substantial exposure to fine particulate matter. Ring Textile spinning and Roving sections also showed elevated PM2.5 levels, with means of 78.45 µg/m3 and 73.95 µg/m3, respectively. The Drawing, Carding, and Blowing sections had relatively lower mean PM2.5 levels, with blowing having the lowest at 58.3 µg/m3. High standard deviations, especially in Carding (39.06 µg/m3) and Cone Winding (26.91 µg/m3), suggested considerable variability in PM2.5 levels within these sections. The 24 h average PM2.5 concentrations in six distinct sections of textile spinning mill is shown in Figure 1.
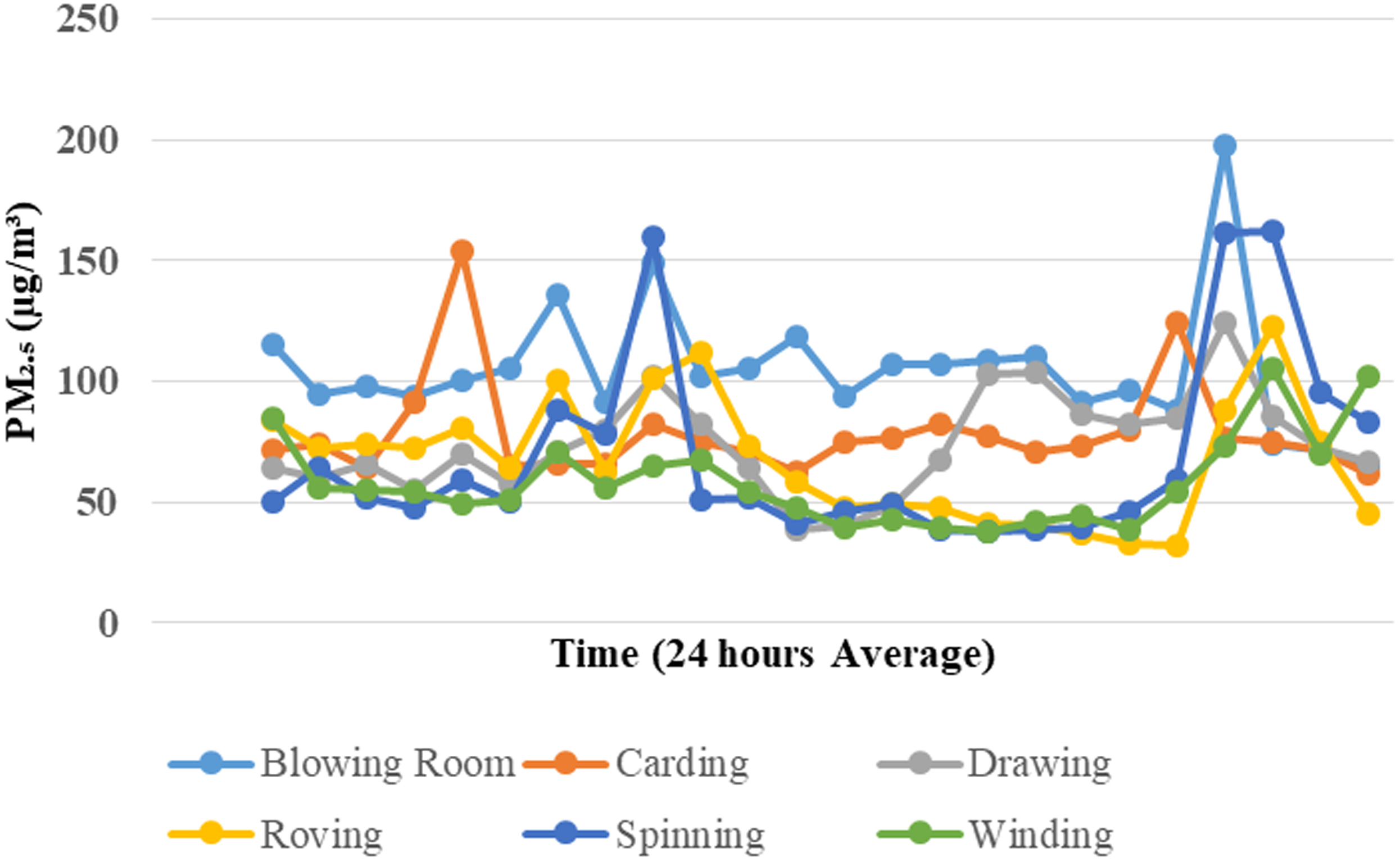
The 24 h average PM2.5 concentration in six distinct sections of textile spinning mill.
Descriptive statistics of PM2.5 & PM10 concentrations at various sections in textile spinning mill.
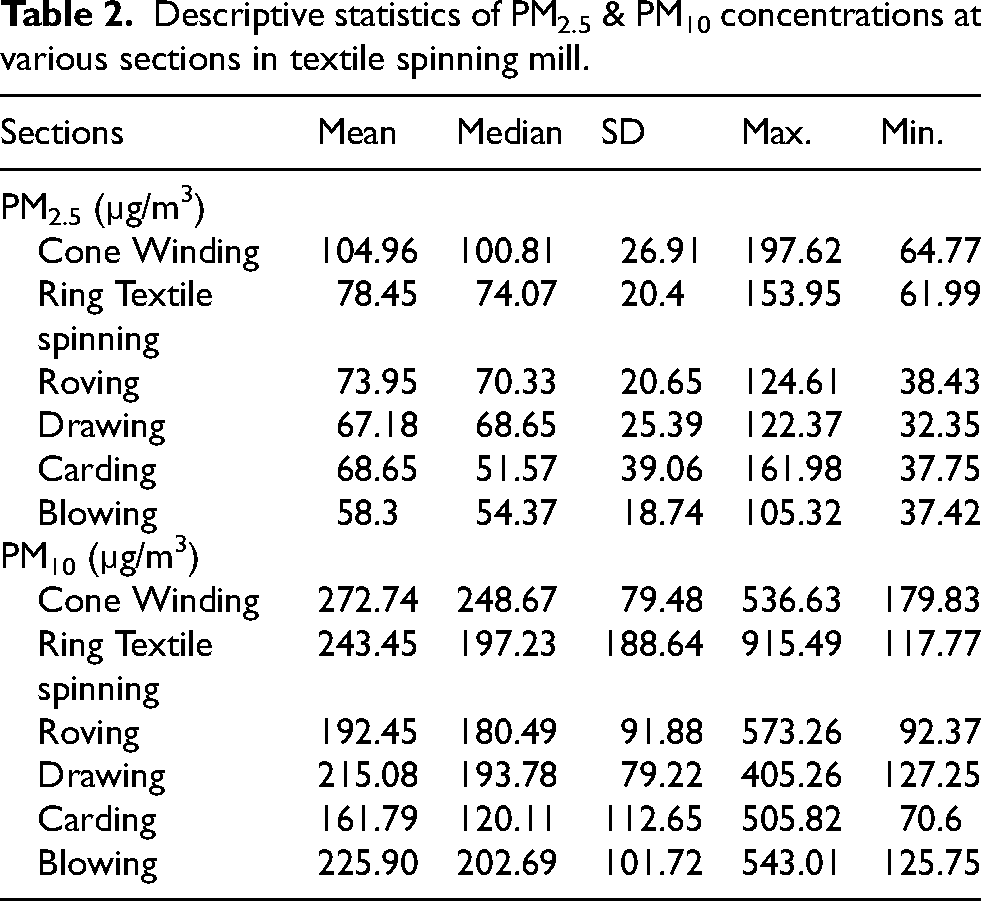
The IAQ results exhibited that, the concentration of PM10 levels were also notably high, particularly in the Cone Winding section, which had a mean of 272.74 µg/m3 and a maximum of 536.63 µg/m3. The Ring Textile spinning section exhibited a mean PM10 level of 243.45 µg/m3, with significant variability (SD = 188.64) and a maximum level reaching 915.49 µg/m3. The Roving and Drawing sections had mean PM10 levels of 192.45 µg/m3 and 215.08 µg/m3, respectively, while the Carding section had the lowest mean PM10 level at 161.79 µg/m3, though it showed high variability (SD = 112.65). The Blowing section also had a high mean PM10 level of 225.90 µg/m3. The 24 h average PM10 concentration in six distinct sections of textile spinning mill is shown in Figure 2. The analysis findings indicated that the 24 h average PM2.5 concentrations in textile spinning mill exceeding the quality standard (>35 µg/m3) were associated with a 2.128-fold increased risk of causing respiratory symptoms compared to levels below the standard (p = 0.032; 95% CI = 1.215–4.597; OR = 2.128). Similarly, the 24 h average PM10 concentrations surpassing the quality standard (>150 µg/m3) were associated with a 1.358-fold higher likelihood of resulting in respiratory symptoms compared to concentrations below the standard (p = 0.003; 95% CI = 1.847–3.012; OR = 1.249). The findings underscore the significant impact of particulate matter pollution on respiratory health, highlighting the importance of adhering to air quality standards to mitigate health risks in occupational settings.
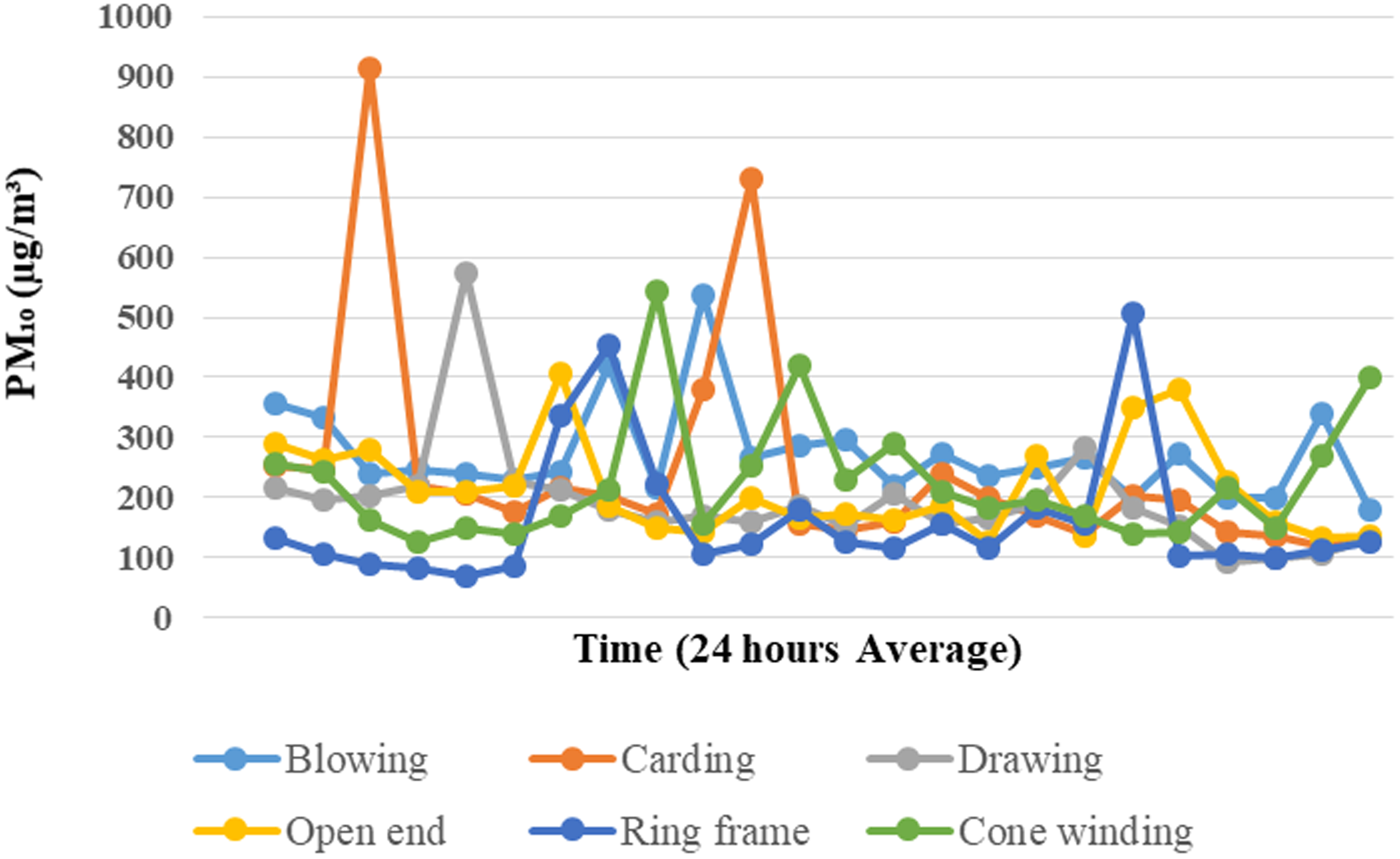
The 24 h average PM10 concentration in six distinct sections of textile spinning mill.
Prevalence of respiratory symptoms among textile spinning mill workers
The analysis of respiratory symptoms among textile spinning mill workers revealed notable findings. Among the workers surveyed, various symptoms were reported, including cough (11.76%), dry cough (12.94%), wheezing (11.76%), phlegm (14.71%), sneezing (17.65%), chest tightness (16.47%), and breathlessness (14.71%). Importantly, all of these symptoms showed statistically significant associations with the working environment, with p-values below 0.001. These results indicate a concerning prevalence of respiratory issues among textile spinning mill workers, potentially stemming from occupational hazards such as poor air quality, exposure to dust and fibers, and inadequate ventilation. 32 The comparison of prevalence of respiratory symptoms across different working sections among workers in textile spinning mill is shown in Figure 3.
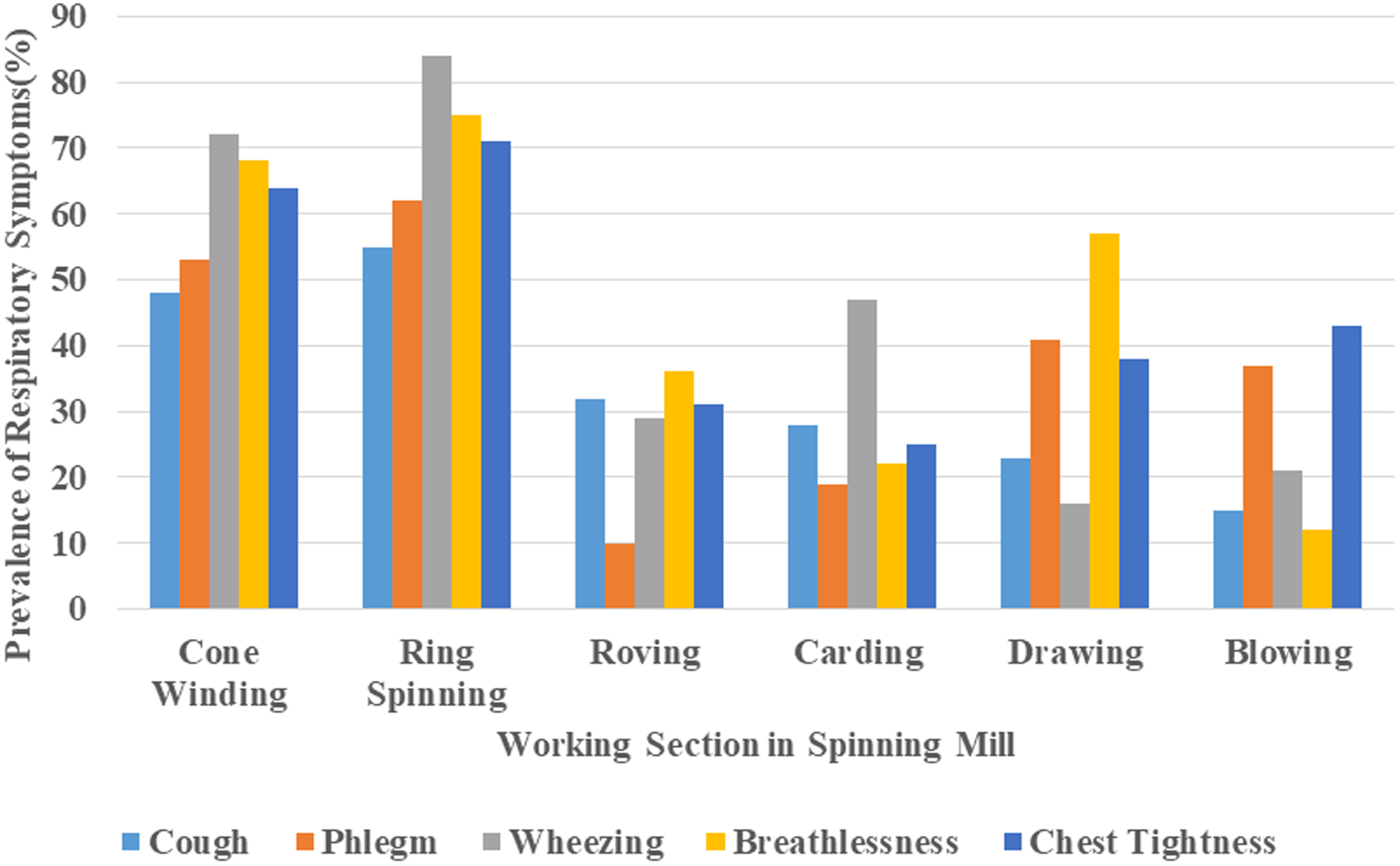
The comparison of prevalence of respiratory symptoms among workers in different sections in textile spinning mill.
Factors associated with respiratory symptoms among textile spinning mill workers
In this study, the logistic regression analysis found that age, working section, work experience, education and use of PPE were associated with prevalence of respiratory symptoms among textile spinning mill workers. The factors associated with respiratory symptoms among textile spinning mill workers is shown in Table 3. The findings of logistic regression analysis revealed that workers aged 41–50 years (OR: 2.34) and those over 50 years (OR: 5.48) had a greater frequency of experiencing respiratory symptoms compared to other age groups. Furthermore, individuals working in the cone winding (OR: 5.8) and ring textile spinning departments (OR: 7.8) showed higher odds of experiencing respiratory symptoms compared to those in other departments. The study revealed a higher frequency of respiratory symptoms and abnormal spirometry results among workers with over 15 years of experience (OR: 5.94), followed by those with 6–15 years of experience (OR: 3.48) when compared with workers having less than 5 years of experience. The workers who had no formal education (OR: 3.55, 95%CI; 2.47–5.47) are more likely to experiencing more respiratory symptoms than others. Furthermore, the workers who doesn’t use PPE (OR: 7.6, 95%CI; 3.78–12.58) had greater chances of affecting with respiratory symptoms.
Factors associated with respiratory symptoms among textile spinning mill workers.
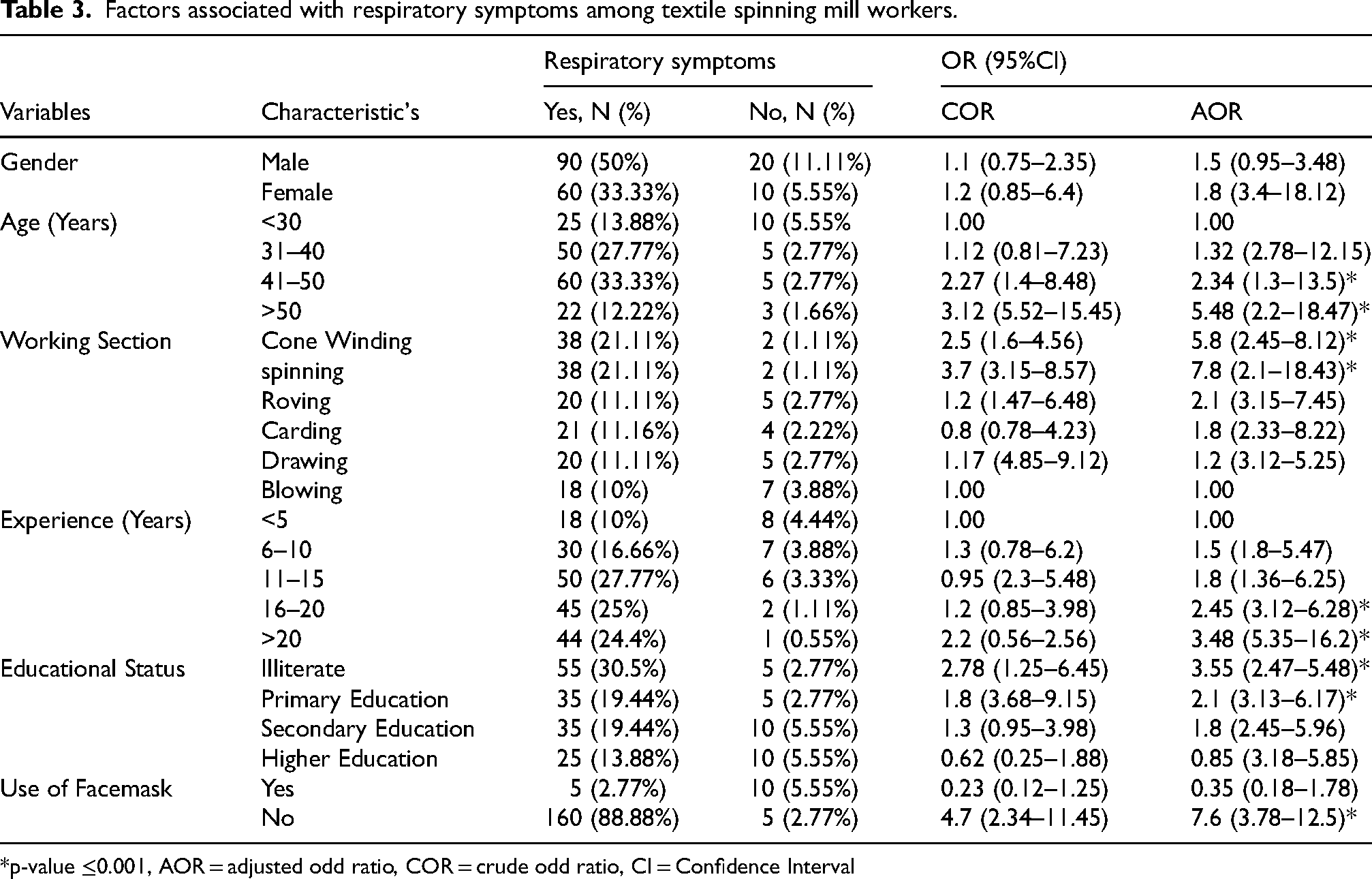
*p-value ≤0.001, AOR = adjusted odd ratio, COR = crude odd ratio, CI = Confidence Interval
Pulmonary function status among textile spinning mill workers
The mean value of FVC, FEV1, FEV1/FVC, and PEFR showed reduction among textile spinning mill workers compared to control groups was shown in shown in Table 4. The result analysis of association between respirable dust exposure and lung function among textile spinning mill workers revealed that a significant majority of workers (80.56%) were exposed to respirable dust levels exceeding 300 μg/m3. Only 19.44% of the workers had acceptable dust exposure levels below 300 μg/m3. This high level of dust exposure correlated with substantial respiratory impairment, as evidenced by lung function tests. Specifically, 83.33% of the workers had reduced lung function, with restrictive patterns observed in 53.89% and obstructive patterns in 29.44%. Further spirometry results showed that 78.89% of the workers had reduced FVC values, 84.44% had reduced FEV1 values, 86.11% had reduced FEV1/FVC ratios, and 82.22% had reduced PEFR values. The Changes in pulmonary function status across work experience and working department group is shown in Figures 4 and 5. The spirometry results indicated a concerning association between high levels of respirable dust exposure and impaired lung function among textile spinning mill workers. The prevalence of reduced lung function parameters, including FVC, FEV1, FEV1/FVC ratio, and PEFR, exhibited that chronic exposure to elevated dust levels was detrimental to respiratory health. 33 The high percentage of workers with restrictive lung function patterns indicates that the lung tissue itself may be affected, leading to decreased lung expansion. 34 Further, the presence of obstructive patterns suggests that the airways were also affected, likely due to inflammation and constriction caused by dust inhalation. 35
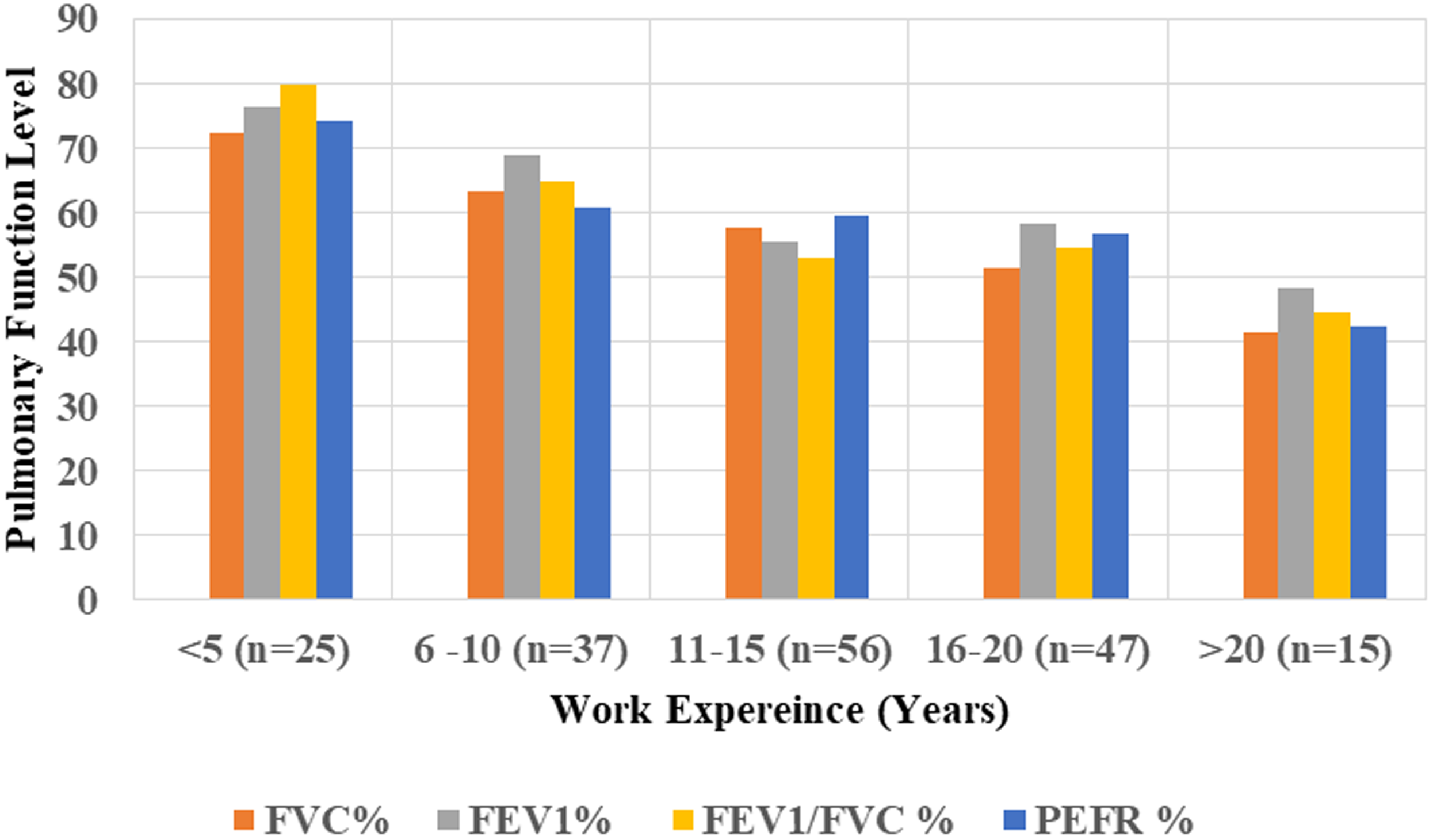
Changes in pulmonary function status across work experience groups in textile spinning mill.
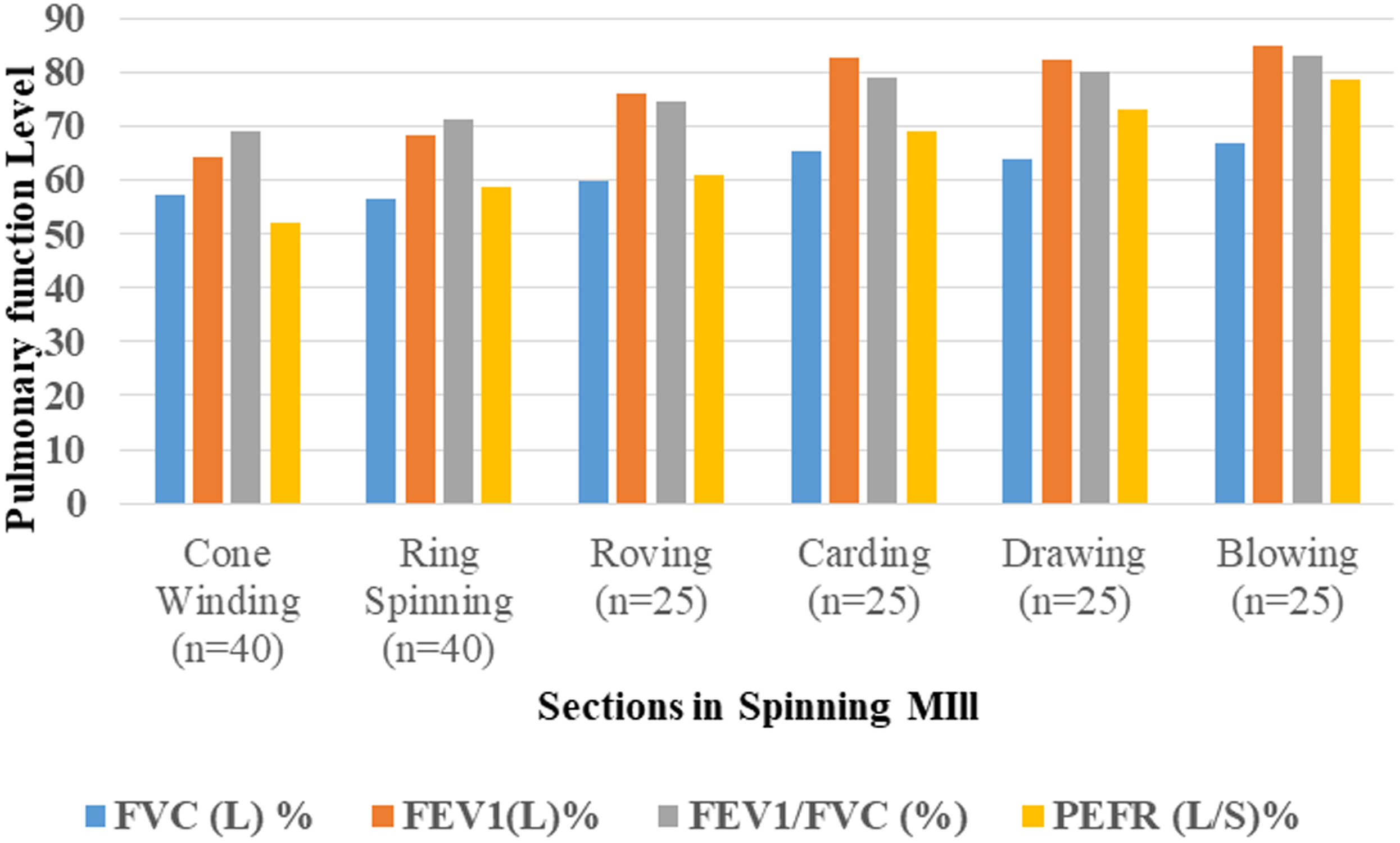
Changes in pulmonary function status among workers in different sections in textile spinning mill.
Pulmonary function among textile spinning mill workers and control groups.
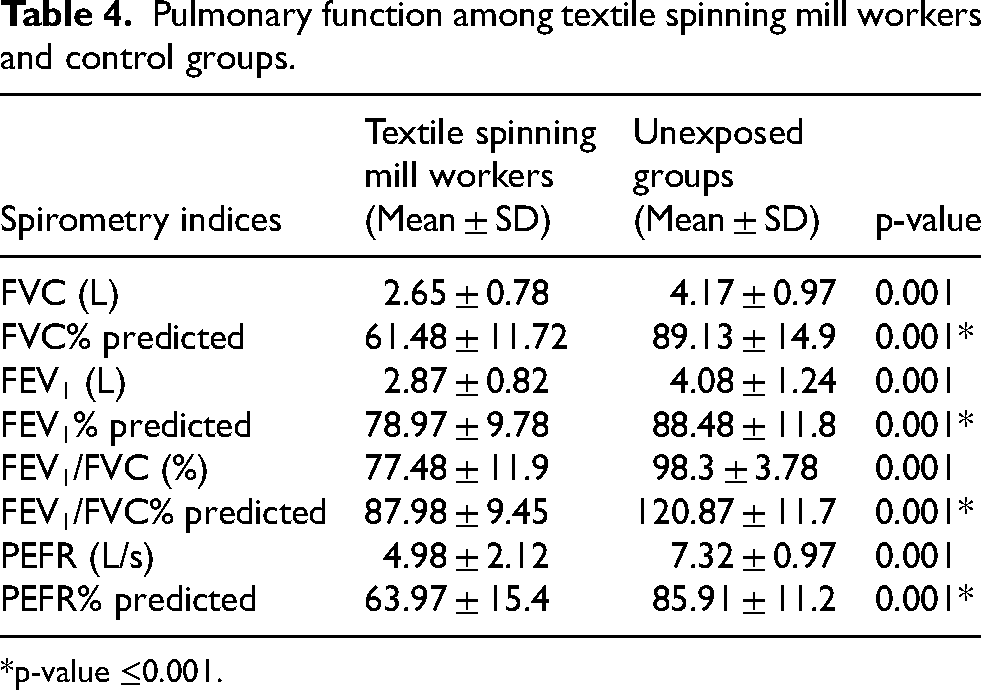
*p-value ≤0.001.
Factors associated with reduced lung function among textile spinning mill workers
The results of multivariable regression analysis showed that age, duration of employment, working department, educational level, presence of respiratory symptoms and increased dust exposure are potential risk factors associated with reduction in pulmonary function was shown in Table 5. From the results of regression analysis, the textile spinning mill workers those in the age group of 31–40 years (OR = 4.71, 95%CI; 1.52 −14.57), age groups of 41–50 years (OR = 5.08, 95%CI; 1.64–15.72), age groups of >50 years (OR = 5.12, 95%CI; 1.77–11.66), workers with work experience of 10–15 years (OR = 2.15, 95%CI; 1.62–7.40), service duration of 15–20 years (OR = 1.79, 95%CI; 1.54–5.88), work experience of greater than 20 years (OR = 2.83, 95%CI; 1.58–13.75), workers employed in ring textile spinning department (OR = 6.25, 95%CI; 2.69–9.11), those employed in cone winding department (OR = 8.28, 95%CI; 1.69 −23.11), workers with no formal education (OR = 2.12, 95%CI; 0.71–5.72), workers affected with respiratory symptoms (OR = 4.2, 95%CI; 0.45–9.45), with increased respirable dust exposure (OR = 11.43, 95%CI; 1.21–11.86) were significantly associated with reduction in the values of FVC than other groups and controls.
The results of multivariable regression analysis showed the factors associated with reduced lung function among textile spinning mill workers.
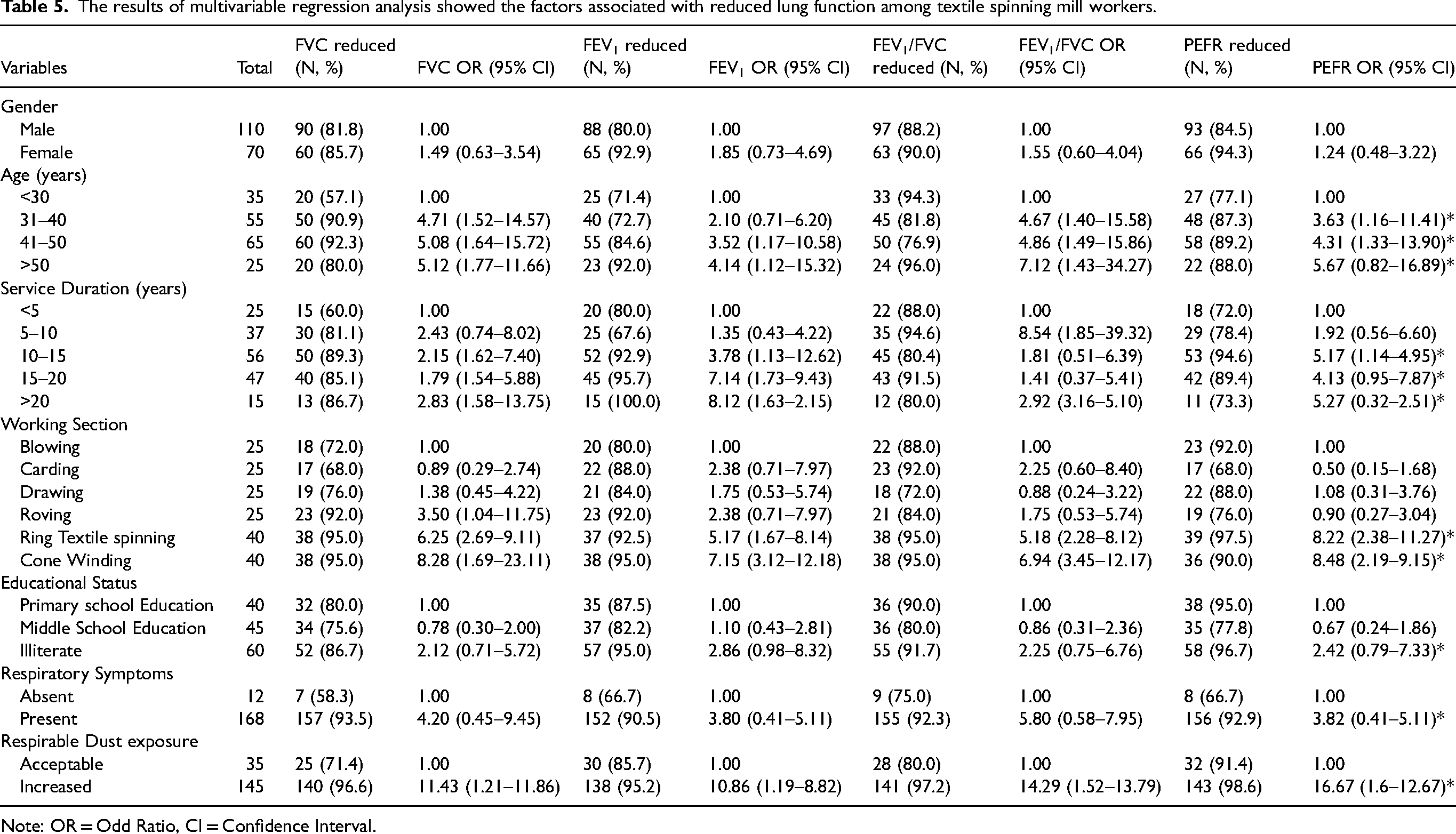
Note: OR = Odd Ratio, CI = Confidence Interval.
Similarly, the textile spinning mill workers those in the age group of 31–40 years (OR = 2.1, 95%CI; 0.71–6.2), age groups of 41–50 years (OR = 3.52, 95%CI; 1.17–10.58), age groups of >50 years (OR = 4.14, 95%CI; 1.12–15.32), workers with work experience of 10–15 years (OR = 3.78, 95%CI; 1.13–12.62), service duration of 15–20 years (OR = 7.14, 95%CI; 1.73–9.43), work experience of greater than 20 years (OR = 8.12, 95%CI; 1.63–2.15), workers employed in ring textile spinning department (OR = 5.17, 95%CI; 1.67–8.14), those employed in cone winding department (OR = 7.15, 95%CI; 3.12 −12.18), workers with no formal education (OR = 2.86, 95%CI; 0.98–8.32), workers affected with respiratory symptoms (OR = 3.9, 95%CI; 0.41–5.11), with increased respirable dust exposure (OR = 10.86, 95%CI; 1.19–8.82) were significantly associated with reduction in the values of FEV1 than other groups and controls.
Furthermore, the textile spinning mill workers those in the age group of 31–40 years (OR = 4.67, 95%CI; 1.4–15.58), age groups of 41–50 years (OR = 4.86, 95%CI; 1.49–15.86), age groups of >50 years (OR = 7.12, 95%CI; 1.43–34.27), workers with work experience of 10–15 years (OR = 1.81, 95%CI; 0.51–6.39), service duration of 15–20 years (OR = 1.41, 95%CI; 0.37–5.41), work experience of greater than 20 years (OR = 2.92, 95%CI; 3.16–5.1), workers employed in ring textile spinning department (OR = 5.18, 95%CI; 2.28–8.12), those employed in cone winding department (OR = 6.94, 95%CI; 3.45–12.17), workers with no formal education (OR = 2.25, 95%CI; 0.75–6.76), workers affected with respiratory symptoms (OR = 5.9, 95%CI; 0.58–7.95), with increased respirable dust exposure (OR = 14.29, 95%CI; 1.52–13.79) were significantly associated with reduction in the values of FEV1/FVC ratio than other groups and controls. Additionally, the textile spinning mill workers those in the age group of 31–40 years (OR = 3.63, 95%CI; 1.16–11.41), age groups of 41–50 years (OR = 4.31, 95%CI; 1.33–13.9), age groups of >50 years (OR = 5.67, 95%CI; 0.82–16.89), workers with work experience of 10–15 years (OR = 5.17, 95%CI; 1.14–4.95), service duration of 15–20 years (OR = 4.13, 95%CI; 0.95–7.87), work experience of greater than 20 years (OR = 5.27, 95%CI; 0.32–2.51), workers employed in ring textile spinning department (OR = 8.22, 95%CI; 2.38–11.27), those employed in cone winding department (OR = 8.48, 95%CI; 2.19 −9.15), workers with no formal education (OR = 2.42, 95%CI; 0.79–7.33), workers affected with respiratory symptoms (OR = 3.82, 95%CI; 0.41–5.11), with increased respirable dust exposure (OR = 16.67, 95%CI; 1.6–12.67) were significantly associated with reduction in the values of PEFR than other groups and controls.
Discussion
Socio-demographic characteristics and respiratory health risks
The socio-demographic profile of the workers in this study reveals several insights into the risk factors associated with respiratory health issues in textile spinning mill environments. The study population was predominantly male (61.1%), which reflects gender-based occupational segregation in the textile industry. This demographic trend suggests that interventions aimed at reducing occupational health risks should be sensitive to gender dynamics, possibly incorporating gender-specific health education and protective measures. The age distribution, with a significant proportion of workers aged between 31–50 years and a notable percentage (22.2%) over 50, suggests a workforce with a substantial exposure history to occupational hazards. The higher prevalence of respiratory symptoms among middle-aged and older workers could indicate cumulative exposure effects, with prolonged inhalation of textile dust and other airborne contaminants leading to the gradual development of respiratory conditions. 36 This is consistent with previous studies showing that chronic exposure to airborne dust in textile settings can result in significant respiratory morbidity, particularly in older workers with prolonged exposure histories.27,28
Furthermore, the high rate of illiteracy (33.33%) among workers suggests a correlation between educational level and health literacy, which could influence workers’ understanding and management of occupational risks. 37 Workers with lower levels of formal education may lack the knowledge necessary to recognize early symptoms of respiratory distress or the importance of using protective equipment effectively. 38 This finding emphasizes the need for tailored educational programs that address the specific knowledge gaps of less educated workers, using simple, accessible language and visuals to convey critical health and safety information. 39
Impact of indoor air quality on respiratory health
Indoor air quality (IAQ) measurements in the study revealed alarmingly high levels of particulate matter (PM2.5 and PM10) in specific sections of the textile spinning mill, particularly the Cone Winding and Ring Textile spinning sections. The PM2.5 and PM10 levels in these areas far exceeded the National Ambient Air Quality Standards (NAAQS), highlighting significant environmental health hazards. 40 The presence of high concentrations of fine particulates can be attributed to the mechanical processes of textile spinning and winding, which generate substantial amounts of airborne dust and fibers. 41 The adverse respiratory health effects associated with high levels of PM2.5 and PM10 are well documented.42,43 Fine particulate matter, particularly PM2.5, can penetrate deep into the lungs, causing inflammation and exacerbating respiratory conditions such as asthma, chronic bronchitis, and chronic obstructive pulmonary disease (COPD). 44 The study's finding of a strong association between poor IAQ and the prevalence of respiratory symptoms (such as sneezing, chest tightness, and breathlessness) underscores the direct impact of particulate matter on respiratory health. 45 This observation aligns with the pathophysiological mechanisms described in occupational respiratory medicine, where exposure to fine particulates in dust-laden environments leads to airway inflammation, oxidative stress, and impaired mucociliary clearance.46,47 Over time, these changes can result in chronic respiratory conditions, reduced lung function, and increased morbidity and mortality among exposed workers. The need for comprehensive dust control measures, such as enhanced ventilation, localized dust extraction systems, and regular air quality monitoring, is evident to mitigate these health risks effectively.48,49
Prevalence and predictors of respiratory symptoms
The study identified a disturbingly high prevalence of respiratory symptoms (93.33%) among textile spinning mill workers, suggesting widespread exposure to harmful environmental conditions. This prevalence was significantly higher which indicating that occupational factors play a pivotal role in the observed respiratory morbidity. 50 Workers with severe pre-existing respiratory diseases or those medically unfit for spirometry were excluded to ensure reliable pulmonary function measurements and to minimize confounding. However, this exclusion may have resulted in a “healthy worker effect,” where severely affected workers are more likely to leave employment, be reassigned, or be absent from work. As a result, the true burden of dust-related respiratory disease among textile workers may be higher than observed in this study. The most frequently reported symptoms—sneezing, chest tightness, and breathlessness—are consistent with both acute and chronic exposure to inhaled particulates and allergens.2,7,51 The analysis also revealed that certain worker characteristics, such as age, work section, and duration of exposure, are significant predictors of respiratory symptoms. 52 Older workers and those with longer exposure durations were more likely to report respiratory symptoms, which is consistent with the notion of dose-response relationships in occupational health. 53 Prolonged exposure to dust and other airborne contaminants is known to lead to cumulative respiratory damage, as evidenced by the higher symptom prevalence among these groups. 54 Additionally, workers in the Cone Winding and Ring Textile spinning sections reported a higher prevalence of respiratory symptoms compared to those in other sections. 5 This could be due to the higher levels of airborne dust and fibers in these sections, as suggested by the air quality measurements. The specific mechanical processes involved in these sections likely contribute to the generation of finer particulates, which are more harmful to respiratory health. 52 This finding highlights the need for targeted interventions in high-risk areas, such as engineering controls to reduce dust generation and enhanced protective measures for workers.
Association between educational level, PPE use, and respiratory symptoms
The study's findings on the association between educational level, PPE use, and respiratory symptoms provide crucial insights into occupational health practices. Workers with no formal education were significantly more likely to report respiratory symptoms, which suggests a lack of awareness and understanding of occupational health risks and the importance of PPE.2,55 This lack of awareness likely contributes to the lower rates of PPE use observed among less educated workers. The strong association between non-use of PPE and respiratory symptoms further underscores the importance of protective measures in preventing respiratory exposure to harmful dust. 56 Inadequate use of PPE, such as masks and respirators, can result in direct inhalation of dust and fibers, leading to respiratory symptoms and long-term lung damage. 57 This finding is consistent with existing literature, which indicates that proper use of PPE can significantly reduce exposure to airborne contaminants and improve respiratory outcomes.56,58 However, the study also suggests that merely providing PPE is insufficient. Training and education on the proper use and maintenance of PPE are essential to ensure its effectiveness. Workers must understand how to use PPE correctly, when to replace it, and how to maintain it to prevent respiratory exposure. This necessitates regular training sessions, clear instructions, and ongoing supervision to reinforce the importance of PPE in protecting respiratory health.
Pulmonary function and long-term health outcomes
The results of pulmonary function tests (PFTs) among textile spinning mill workers provide a clear indication of the long-term respiratory health effects of occupational dust exposure. The significant proportion of workers exhibiting restrictive and obstructive patterns in lung function is concerning, as these patterns are indicative of chronic respiratory conditions. 59 Restrictive lung patterns suggest reduced lung volumes, likely due to lung tissue damage or fibrosis, which can result from prolonged inhalation of fine particulates and fibers. 60 Obstructive patterns, characterized by reduced airflow and difficulty exhaling, suggest conditions such as chronic bronchitis or COPD. 17 These findings are particularly troubling given the relatively young age of many workers, indicating that significant respiratory impairment is occurring relatively early in their careers.27,28 This highlights the urgent need for early detection and intervention strategies, such as routine health screenings and lung function tests, to identify and manage respiratory conditions before they progress to more severe stages. Moreover, the presence of both restrictive and obstructive patterns in a single workforce suggests a combination of inflammatory and fibrotic processes, which could be exacerbated by continuous exposure to dust and other respiratory irritants.61,62 This underscores the importance of reducing exposure levels through engineering controls, improving workplace ventilation, and promoting the use of PPE. It also points to the need for comprehensive medical surveillance programs that include regular PFTs and other diagnostic tests to monitor workers’ respiratory health over time. Future research should focus on longitudinal studies to track the progression of respiratory symptoms and lung function over time, providing more robust evidence of the long-term effects of dust exposure. It would also be beneficial to investigate the effectiveness of different dust control measures and PPE types in reducing exposure and improving respiratory health outcomes among textile workers.
Limitations and strength of the study
This study has certain limitations that should be considered while interpreting the findings. First, the cross-sectional design limits the ability to establish a causal relationship between occupational dust exposure and respiratory health outcomes, as exposure and health parameters were assessed at a single point in time. Second, some information such as work history, duration of exposure, and respiratory symptoms was based on self-reported data, which may be subject to recall bias. Third, although major occupational exposure factors were considered, other potential confounding variables such as environmental exposure outside the workplace, individual susceptibility, and lifestyle factors may have influenced the results. Fourth, exposure measurements were conducted using area-based monitoring, and variations in individual worker exposure levels and day-to-day environmental conditions may have contributed to measurement variability. One limitation of this study is that bronchodilator reversibility testing was not performed as part of spirometry assessment. This was primarily due to logistical and resource constraints associated with field-based occupational health assessment. Future studies incorporating bronchodilator reversibility testing would provide more comprehensive evaluation of respiratory function and improve identification of occupational asthma. Despite this limitation, the present study has several important strengths. These include the use of standardized spirometry for objective lung function assessment, validated respiratory symptom questionnaires, and direct measurement of workplace dust exposure. The integration of environmental exposure assessment with clinical respiratory evaluation provides a comprehensive understanding of the relationship between occupational exposure and respiratory health. Additionally, this study contributes valuable regional data on textile workers in India, helping to address an important gap in occupational health research.
Conclusion
This study evaluated the quality of indoor air and its effects on the respiratory health of textile spinning mill workers in Tamil Nadu, India. The results showed that the level of particulate matter in the indoor air was high in major sections of production, which implies high levels of occupational exposure to dust. A significant percentage of workers were reporting respiratory symptoms and lowering pulmonary functioning was noted in the exposing workers. These findings indicate that indoor air quality and respiratory illnesses in textile spinning mill conditions are highly correlated, and the exposure to dust is one of the primary contributing factors. These results indicate the necessity to implement preventive and control measures to enhance the indoor Air Quality in textile spinning mills. To reduce the level of airborne particulate, effective ventilation systems, dust control measures, machinery regular maintenance and clean practices of the workspace should be implemented. Besides, proper respiratory protective equipment should be given to the workers and they should be trained on proper usage. Early detection and prevention of respiratory impairment is also recommended by regular medical surveillance and periodic spirometry testing. In general, engineering controls, worker protection, and constant monitoring are imperative to enhance the indoor air quality in order to minimize the occupational dust exposure and protect the respiratory health of textile spinning mill workers.
Footnotes
Ethical considerations
The research described here was approved by Kongu Engineering College Ethics Committee (KEC/R&D/EC/2022-23/003).
Consent to participate
All participants gave written informed consent and participation in the study was entirely voluntary.
Author contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Shankar Subramaniam, Abbas Ganesan, Chander Prakash and Naveenkumar Raju. The first draft of the manuscript was written by Abbas Ganesan and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Indian Council for Medical Research (5/8-4/30/ENV/2020-NCD-II) and Shankar Subramaniam, and Naveenkumar Raju has received the funding support.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data underlying this article will be shared on reasonable request to the corresponding author.