
Abstract
Background
The growth of the food sector associated with inadequate ergonomic conditions and occupational risks has contributed to the increase in musculoskeletal disorders among workers.
Objective
The aim of this study was to describe working conditions and the occurrence of work-related musculoskeletal disorders among professionals working at a university restaurant.
Methods
This is a cross-sectional study with a convenience sample of university restaurant workers over 18 years of age. Those who refused to respond or did not complete the questionnaires were excluded as well as those who had worked at the company for less than 3 months. The Questionário Saúde e Trabalho em Atividades de Serviço (QSATS), the Nordic Musculoskeletal Questionnaire (NMQ), and the International Physical Activity Questionnaire (IPAQ) were used. Numerical data are expressed as mean ± standard deviation, while categorical variables are presented as both relative and absolute frequencies.
Results
Forty-seven workers (36.83 ± 12.53 years) participated in the study, of whom 40.43% were men and 59.57% were women. Out of all participants, 57.44% reported work-related symptoms. Workers reported frequent demands at work, such as repetitive and detailed gestures, prolonged standing or moving, and intense physical efforts, and most reported that their work never required them to sit for prolonged periods. The most prevalent musculoskeletal symptoms occurred on the wrists/hands, lower back, shoulders, and upper back.
Conclusions
Working conditions may contribute to the occurrence of musculoskeletal symptoms and work-related musculoskeletal disorders (WMSDs) in professionals working at a university restaurant, highlighting the need for ergonomic interventions to prevent these disorders.
Keywords
Introduction
In recent years, the food industry has grown significantly, leading to an increased demand for workers. This growth
In the food sector, factors such as posture, physical effort, repetitiveness, long working hours, and workplace organization are known to contribute to the development of these disorders
Kitchen workers are highly vulnerable to WMSDs due to inadequate working conditions, long working hours, and intense time pressure to complete tasks within strict deadlines. 6 Sticca et al. 7 identified injuries affecting the limbs, spine, and hearing, associating these exposures with impairments in physical and mental health. These findings highlight that, beyond musculoskeletal impacts, occupational exposures can result in broader health consequences. In this context, occupational health plays a crucial role in identifying and managing risks that can be physical, chemical, biological, ergonomic, and psychosocial.4,8
Physical risks include environmental factors such as excessive heat or noise. Chemical risks involve accidental or chronic exposure to harmful substances. Psychosocial risks affect the physical, mental, and social health of workers and are often related to adverse working conditions, resulting in increased stress levels.4,9 Given the multifactorial nature of these risks, it is essential to implement ergonomic interventions in work environments to prevent or reduce WMSDs by adapting workplaces to the individual needs of each professional. 10
Ergonomics emerged in 1949, focusing on the human–machine relationship, and over time expanded its scope to include physical and cognitive demands, aiming to promote harmony between work systems and workers’ well-being.
11
One of the main ergonomic interventions in the workplace is Ergonomic Work Analysis, which assesses the physical and psychophysiological impacts of workers’ activities and consists of five phases: demand analysis, task analysis, activity analysis, diagnosis, and recommendations.
12
Each phase focuses on distinct aspects of the work environment. The intervention begins with demand analysis, which involves identifying ergonomic problems encountered in daily work
Several factors can directly affect the health of food sector workers, increasing the risk of WMSDs. This reinforces the importance of ergonomic interventions in these environments. However, despite the recognized relevance of ergonomics in the food sector, evidence focusing on university restaurant workers remains limited. Thus, the present study aimed to describe working conditions and the occurrence of WMSDs among professionals working in a university restaurant.
Methods
This cross-sectional study was approved by the Research Ethics Committee, CAAE No. 75553517.1.0000.0102, under Opinion No. 2.327.563. Questionnaires were distributed to staff working in university restaurants at a public university campus in southern Brazil. A convenience sampling method was used. Prior to participation, all participants signed an Informed Consent Form (ICF).
Questionnaires were administered on the campuses of a public university in southern Brazil, specifically in areas where meals were served. Workers who voluntarily agreed to participate were directed to designated locations in small groups, accompanied by a supervisor, such as a nutritionist or department head. The questionnaires were explained to participants, and staff members were available to provide clarification when needed.
Regarding inclusion criteria, participants were required to be employees of university restaurants on the selected campuses, regardless of race or ethnicity, of either sex, and aged 18 years or older. Participants were excluded if they refused to complete the questionnaires, did not complete them in full, and/or had been employed at the institution for less than three months.
Restaurant workers included in the study performed duties related to kitchen work, tray service (pantry activities), food service, and cleaning activities. Their tasks included food preparation and pre-preparation; washing and cutting food; operating ovens and buffet stations; dishwashing and tray handling; organization of the work environment, stockrooms, and cold storage areas; food distribution and service; customer service; cleaning of dining areas; and manual handling and transport of loads. Some participants also reported support and team coordination roles, performing multiple tasks throughout the work shift. In this study, the term “restaurant workers” refers to all employees involved in food preparation, tray service, food distribution, customer service, cleaning, and support or coordination activities within university restaurant operations.
The following questionnaires were applied: the Questionário Saúde e Trabalho em Atividades de Serviço (QSATS), an updated version of the Health and Work Survey in Service (INSATS), 2007 version; the Nordic Musculoskeletal Questionnaire (NMQ, 2002); and the International Physical Activity Questionnaire (IPAQ, 2001).
The QSATS is a self-administered questionnaire that allows for the assessment of workers and their work environment. In addition to considering health–disease conditions, this questionnaire addresses factors potentially harmful to workers’ health through qualitative and quantitative data. Its structure includes five domains: personal and professional characteristics; work organization; working conditions; family life; and health. 13 For the purposes of this study, selected domains were adapted to focus on personal and professional characteristics, work organization, working conditions, and health.
Personal characteristics included questions on age, gender, level of education, and length of employment in the field. Professional characteristics addressed employment status (regular employee, contractor, or civil servant), work schedule and shift, pre-established weekly working hours, and average weekly working hours. 13 Sample characterization included quantitative data (mean and standard deviation) and qualitative data (percentages).
The “My Health” domain required employees to indicate the intensity of symptoms listed in a table, using the response options “does not present,” “occasionally,” and “frequently,” and to report whether the symptoms were caused or aggravated by work. Data interpretation involved counting the number of work-related symptoms reported by each employee, dividing this value by the total number of participants, and expressing the result as a percentage.
The “Working Conditions” domain assesses postural and physical effort demands associated with work activities, using the response options “always,” “sometimes,” “rarely,” or “never”. 13 For each of the six assessed conditions, the frequency of responses for each option was calculated and expressed as a percentage.
The domain related to work pace and intensity presents several situations involving the work environment, with three response options: “it does not bother me,” “it bothers me a little,” and “it bothers me a lot”. 13 Results were obtained by calculating the percentage distribution of responses across the available options.
The NMQ is used to assess musculoskeletal symptoms. Although the questionnaire does not provide a clinical diagnosis, it enables the identification of musculoskeletal complaints, serving as an important screening tool for the work environment. Results were analyzed by dividing the number of positive responses in each body region by the total number of participants and expressing the values as percentages. 14
The IPAQ aims to assess physical activity levels, classifying individuals as vigorously active, moderately active, or insufficiently active. The short version of the questionnaire was used in this study. It consists of eight questions related to physical activities performed in daily life. Results were analyzed based on activity duration (minutes), weekly frequency, and MET intensity. MET-minutes per week were calculated and presented in tabular form. 15
Results
All 53 workers were considered eligible and agreed to participate in the study. However, six participants did not fully complete the questionnaires and were excluded, resulting in a final sample of 47 participants (Figure 1). Of these, 59.57% were female and 40.43% were male, with a mean age of 36.83 ± 12.53 years. The predominant level of education was high school (55.32%), followed by elementary school (25.53%) and undergraduate education (12.77%). Most participants (80.85%) were regular employees, while 10.64% were contractors with fixed-term agreements.
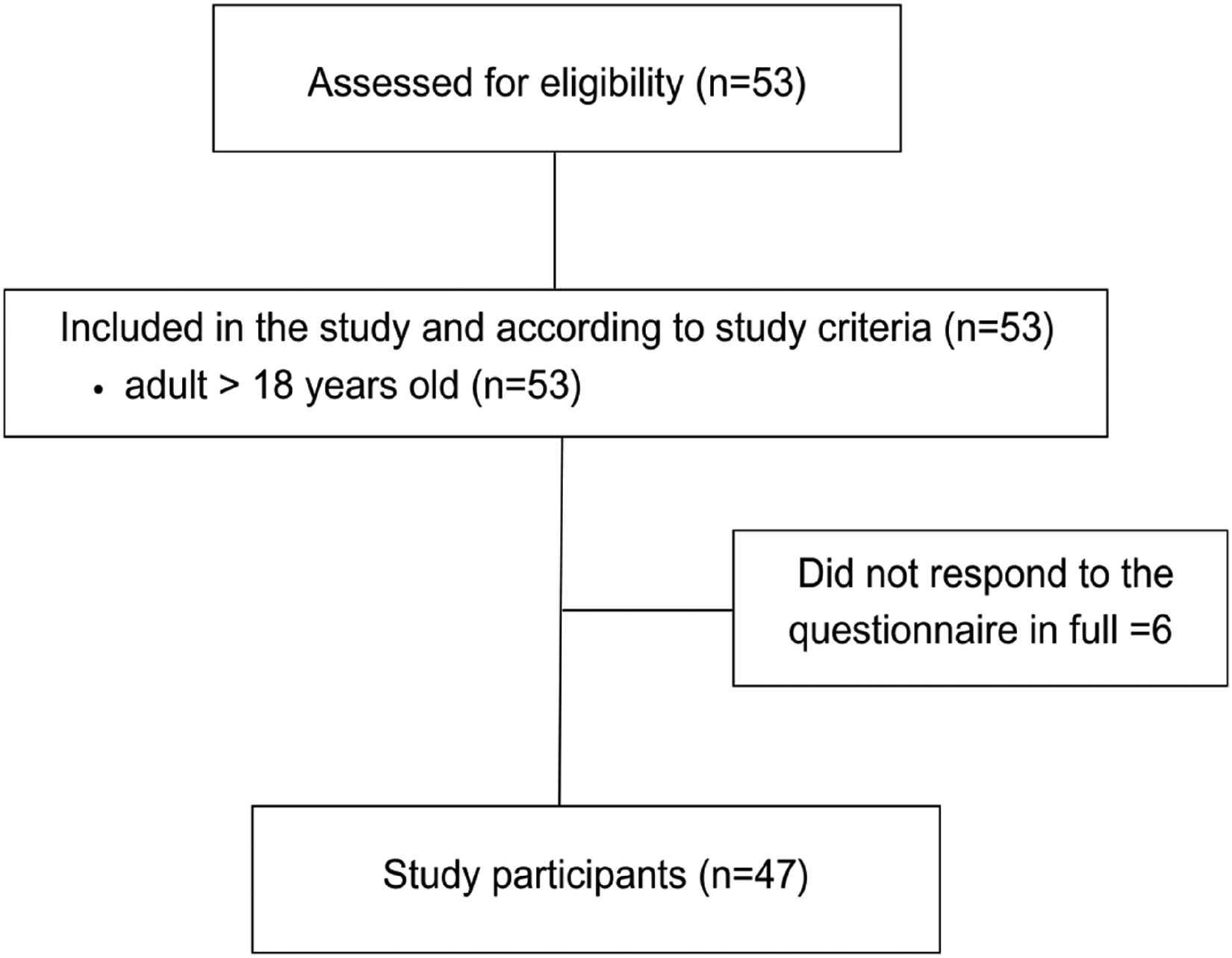
Fluxogram – participants. n = number of participants. Source: The Authors (2024).
Working hours were predominantly fixed (97.87%). Three work shifts were identified: 70.21% of the sample worked the daytime shift, followed by mixed shifts (25.53%) and the night shift (2.13%). Most employees (93.62%) worked on regular business days, whereas 6.38% followed alternative work schedules. The mean weekly workload was 42.64 ± 12.51 h, while the mean official working hours were 41.45 ± 4.51 h.
Another variable used to characterize the sample was the length of employment in the current job. Due to the wide variability in responses, employment duration was categorized into time ranges. Overall, 42.55% of workers had between three and eleven months of job tenure, 46.81% had between one and ten years of work experience, and 8.51% had between eleven and thirty-five years of employment, as shown in Table 1.
Sample characterization.
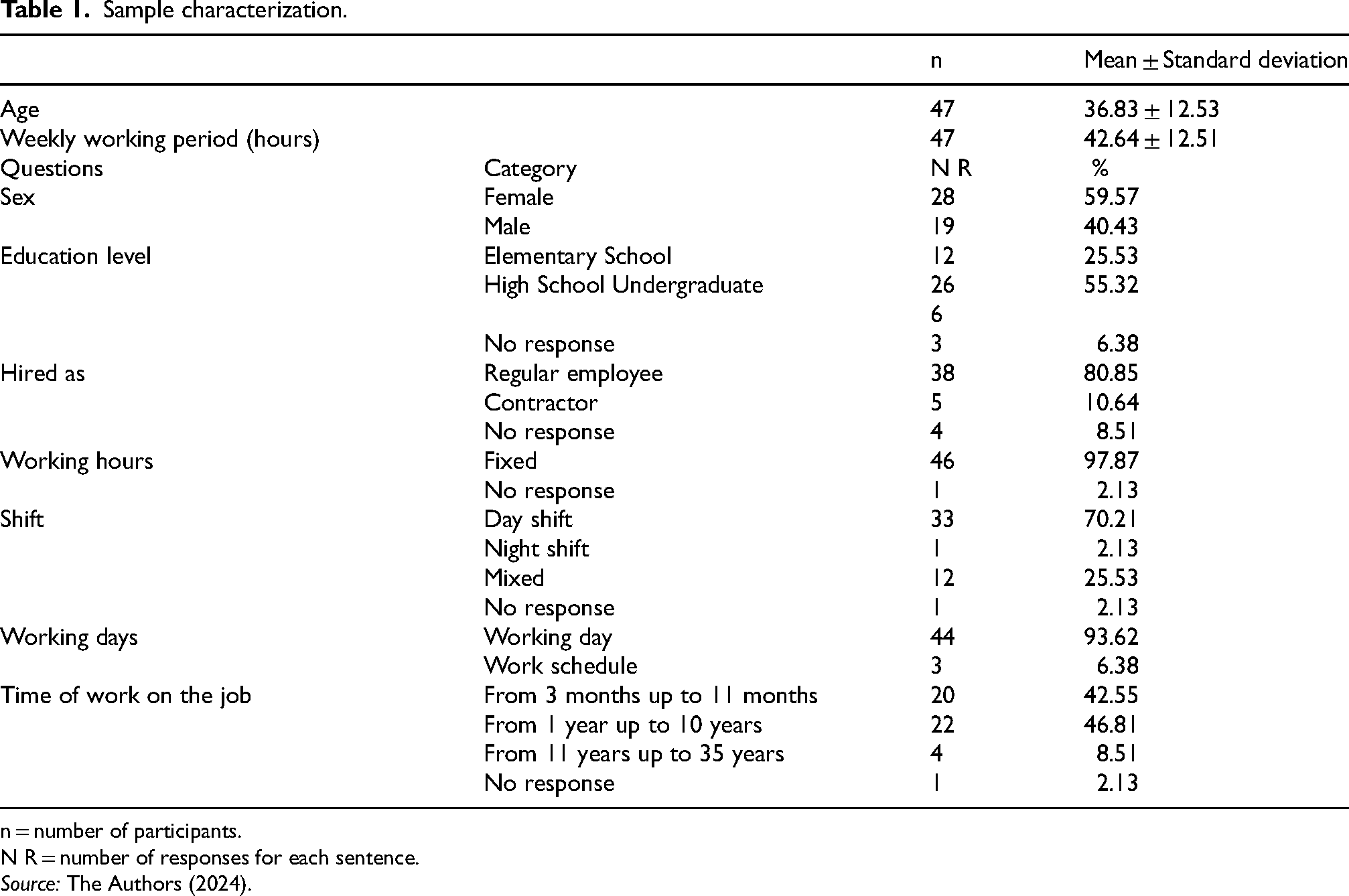
n = number of participants.
N R = number of responses for each sentence.
Source: The Authors (2024).
Responses from the “my health” section of the QSATS were used to classify participants into three subgroups. Workers reporting three or more work-related symptoms accounted for 40.42% (n = 19) of the sample, those reporting one or two symptoms represented 17.02% (n = 8), and those reporting no work-related symptoms comprised 42.55% (n = 20). The most frequently reported work-related symptoms were back pain (44.68%, n = 21), muscle and joint problems (34.04%, n = 16), discouragement (29.79%, n = 14), anxiety and/or irritability (29.79%, n = 14), and injuries (27.66%, n = 13), as presented in Table 2.
My health.
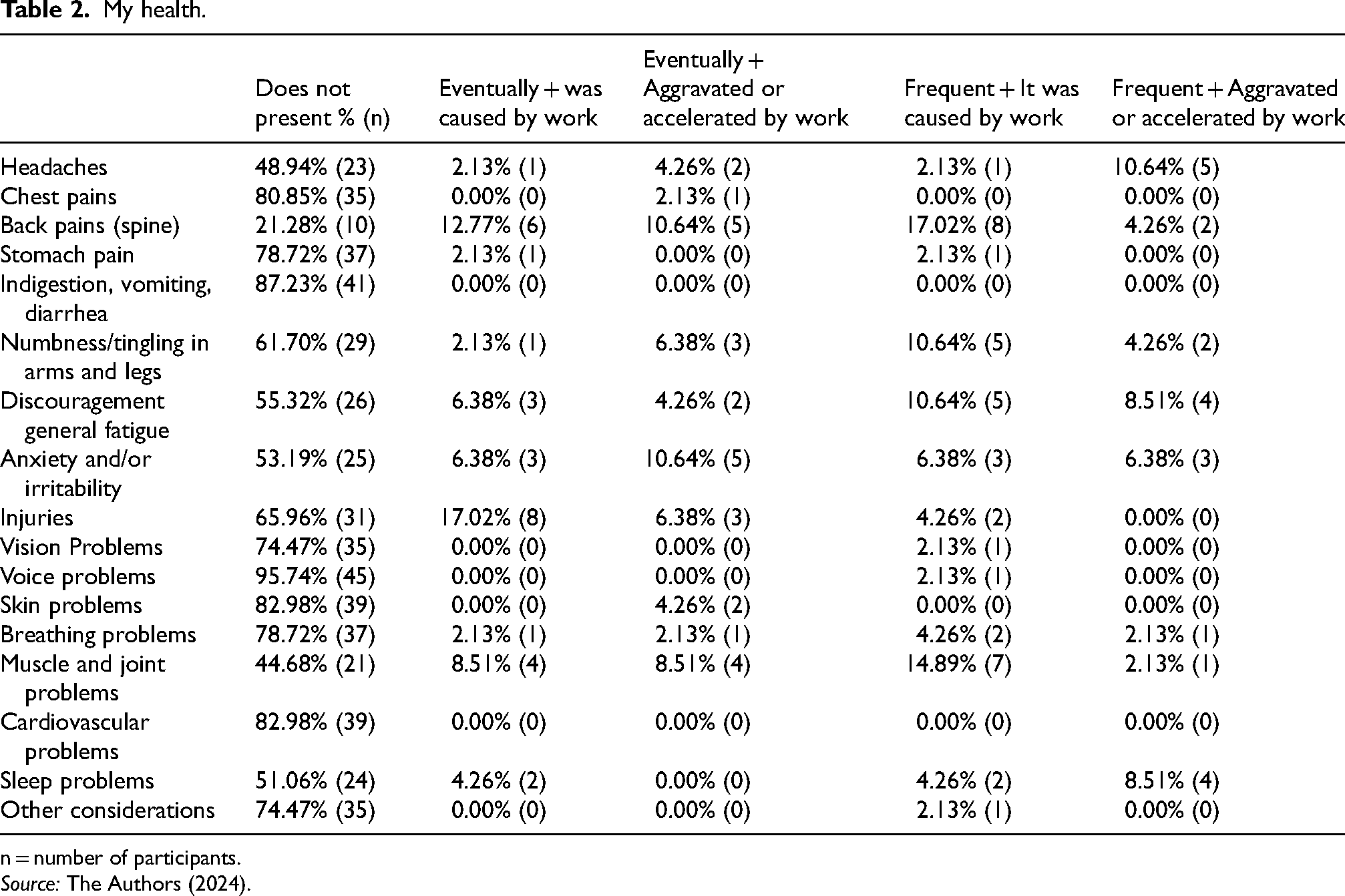
n = number of participants.
Source: The Authors (2024).
Regarding the facilities domain of the QSATS, most respondents considered the facilities to be adequate. A higher proportion of negative responses was observed only for the adequacy of spaces for breaks, snacks, or rest (28% of responses). Detailed results for this domain are provided in Appendix 3. In the working conditions domain, 80.85% (n = 38) of workers reported that their work “always” required repetitive and meticulous movements, 82.97% (n = 39) reported prolonged standing in the same position, and 74.46% (n = 35) reported frequent movement. Intense physical effort was reported as “always” required by 59.57% (n = 28) of participants. In addition, 63.82% (n = 30) indicated that their work “never” required sitting for prolonged periods. These results are detailed in Table 3.
Work conditions results.
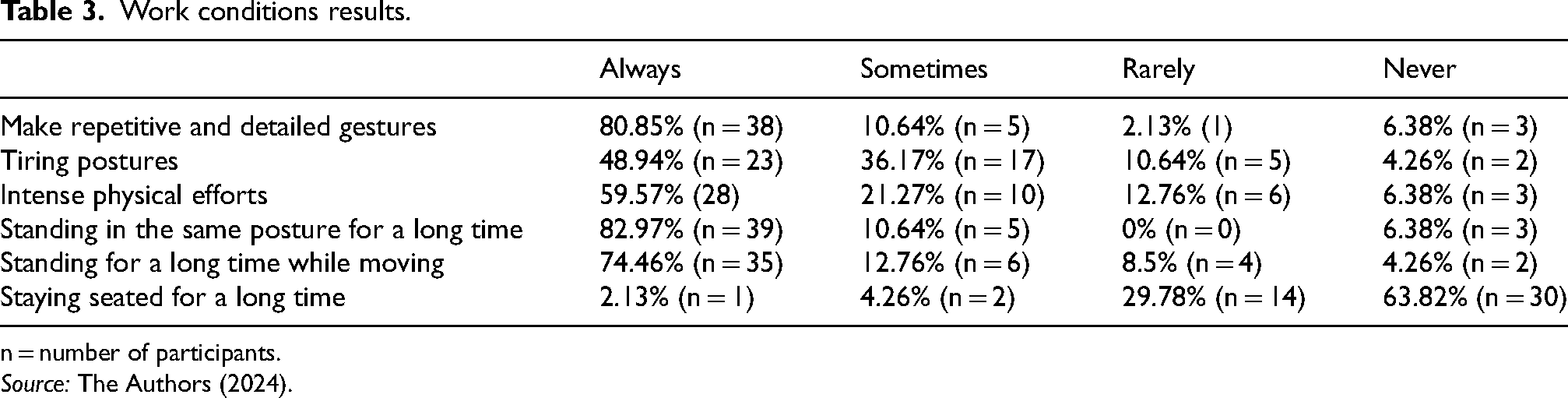
n = number of participants.
Source: The Authors (2024).
With respect to work pace and intensity, 68.20% of respondents reported that acting according to the demands or needs of the public, clients, or users was not a concern. Furthermore, 44.40% indicated that going beyond normal working hours did not bother them, while 46.70% reported discomfort with depending on the work of colleagues.
According to the QSATS results, the prevalence of musculoskeletal symptoms in the previous 12 months was highest in the wrists/hands (68.08%), followed by the lower back (57.44%), shoulders (57.44%), and upper back (48.93%). In the seven days preceding the assessment, the most prevalent symptoms were reported in the lower back (36.17%), followed by the upper back and wrists/hands (both 36.17%) and shoulders (13.00%). Table 4 presents detailed results for all body regions, limitations in daily activities, and consultations with health professionals.
NMQ results.
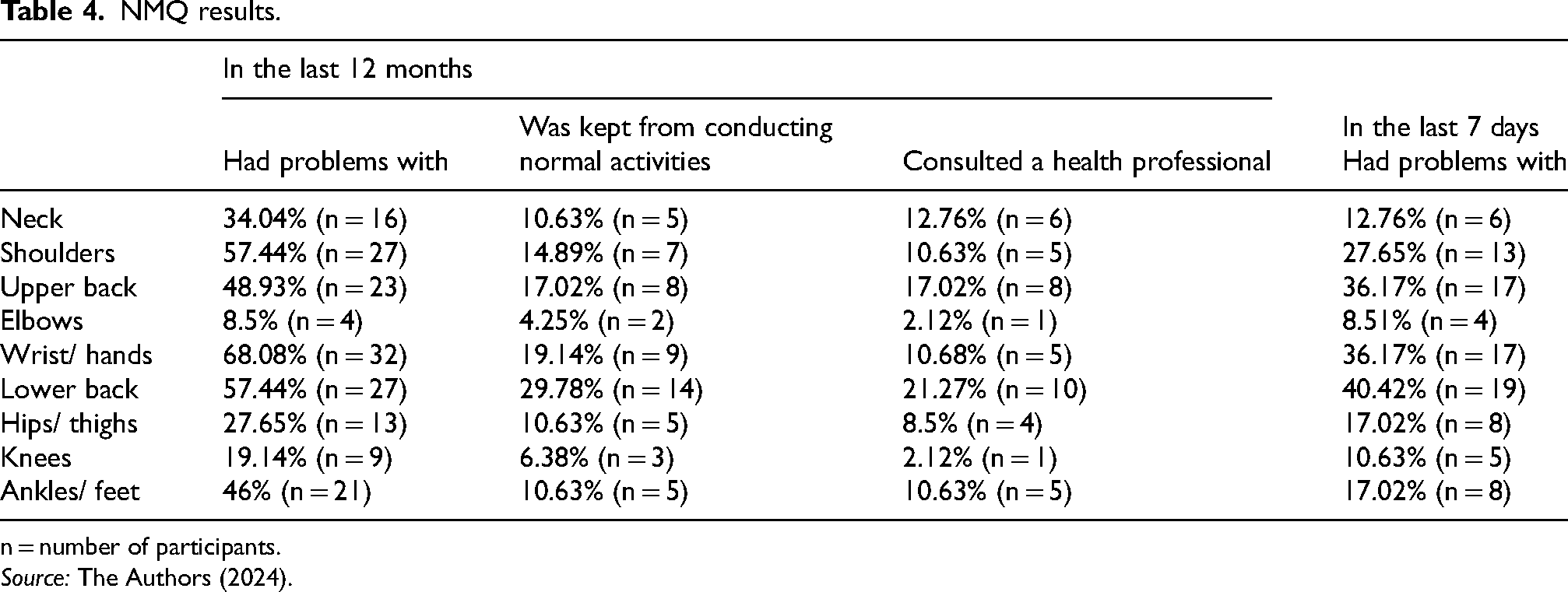
n = number of participants.
Source: The Authors (2024).
Regarding the level of physical activity assessed by the IPAQ, among the 47 respondents, 27.65% (n = 13) were classified as insufficiently active, 27.65% (n = 13) as moderately active, and 44.68% (n = 21) as vigorously active, as shown in Table 5.
Physical activity levels.
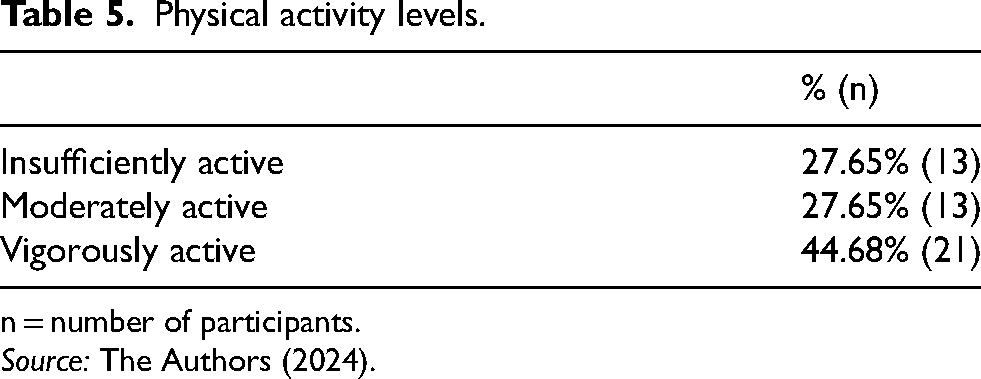
n = number of participants.
Source: The Authors (2024).
Discussion
The health of restaurant workers remains underexplored in the scientific literature, particularly regarding ergonomic aspects. Although instruments such as the QSATS and the NMQ have demonstrated good applicability for qualitative and quantitative assessments of occupational health, their use among university restaurant workers remains limited. LIMA et al. 16 highlight the need for further investigations in this professional group to support the development of effective workplace health promotion actions.
In this study, university restaurant workers were defined as professionals involved in meal preparation, distribution, service, cleaning, and organizational support. Ergonomics, as both a scientific discipline and an applied practice, seeks to adapt tasks, workstations, and work environments to promote health, safety, and well-being while improving system performance.17,18 Interventions such as task reorganization, scheduled breaks, workstation adjustments, and posture training are recognized strategies for reducing exposure to WMSDs.
The sociodemographic profile observed was consistent with that reported by LIMA et al., 16 particularly regarding the predominance of female workers, mean age, and educational level. This study extends this characterization by including employment status, weekly workload, and length of service, allowing for a more comprehensive analysis of occupational exposure and cumulative workload.
More than half of the participants reported a negative impact of work on their lives, mainly due to musculoskeletal symptoms such as back pain, fatigue, tingling, and joint or muscle discomfort. The absence of work leave despite the presence of symptoms may indicate the normalization of pain as part of the work routine, a phenomenon also observed in other occupational contexts. Comparable findings were described by Akbar et al., 19 who identified a considerable prevalence of WMSDs among workers exposed to repetitive tasks, inadequate postures, and long working hours.
A systematic review of the catering industry 20 revealed wide variability in the prevalence of WMSDs (3%–86%), depending on job role and type of establishment, mainly associated with inadequate postures, repetitive movements, excessive physical effort, long working hours, and insufficient breaks. Likewise, studies involving dairy diversification workers 21 showed that high physical workload, inadequate postures, and task unpredictability were associated with a greater occurrence of musculoskeletal pain.
In the present study, workers reported performing multiple tasks simultaneously during the same shift, such as cutting, cooking, washing, and serving food, characterizing work overload. This multifunctionality, combined with prolonged standing and constant movement, reflects an intense work pace with limited opportunities for rest, an organizational pattern associated with increased occupational health risks. 22 Similar conditions have been observed among public school teachers 23 and higher education faculty members, 24 who are exposed to long working hours, reduced breaks, and high psychosocial workload.
Data from the “My Health” section of the QSATS indicated continuous exposure to biomechanical risk factors, including forced postures, repetitive movements, prolonged standing, and constant walking, which are widely recognized determinants of WMSDs among food service workers.25,26,27 The post-pandemic context may have intensified these risks, as studies involving workers in higher education institutions have reported increased burnout, fatigue, anxiety, and depression associated with work overload and organizational changes. 28
Data from the NMQ revealed a high prevalence of spinal symptoms, particularly in the thoracic (48.93%) and lumbar (57.44%) regions, exceeding values reported in population-based studies. 29 This pattern was also observed by Iqbal et al., 30 who identified high physical strain and an increased risk of musculoskeletal pain among chefs and food service workers.
The high prevalence of WMSDs among food service workers is consistent across different countries and study designs.31,32 A meta-analysis reported comparable rates across European countries, reinforcing the vulnerability of workers exposed to high physical demands. 31 In addition, prolonged standing, multifunctionality, and repetitive upper limb movements were significantly associated with WMSDs among kitchen workers. 33 These findings are corroborated by studies of kitchen workers in Canada, which reported a prevalence of musculoskeletal discomfort of 98.1%, particularly in the lower back, feet, shoulders, and neck. 32
Evidence from other professions, such as dentists, also indicates a high prevalence of WMSDs (68%–100%), mainly affecting the lower back, shoulders, and neck, 34 suggesting that inadequate postures and high physical demands are common risk factors across different occupations.
Although the literature indicates that adequate levels of physical activity are associated with a lower prevalence of musculoskeletal symptoms,35,36 this protective effect may not apply to physically demanding occupations. In the present study, despite 72.33% of participants being classified as moderately or vigorously active, the high prevalence of symptoms persisted, possibly due to the predominance of occupational physical activity over preventive or compensatory exercise. 37 Even with adherence to World Health Organization recommendations, 38 these findings suggest that physical activity alone is insufficient to prevent WMSDs under unfavorable ergonomic conditions. This reinforces the importance of workplace-based interventions, such as active breaks, exercise programs, and ergonomic adjustments.39,40,41
Study limitations include the use of a convenience sample, which may limit representativeness and generalizability, and the absence of individual factors such as body mass index, prior history of musculoskeletal disorders, and medication use. Additionally, the descriptive nature of the analysis precludes causal inferences. Given the small sample size and the exploratory objective of the study, inferential analyses were intentionally not performed, as they could lead to spurious associations and overinterpretation of the findings. Nevertheless, this study provides a detailed characterization of working conditions and symptom patterns, thus contributing relevant evidence to inform future research and intervention strategies. Future studies should prioritize probabilistic sampling and control for potential confounding factors to strengthen the robustness of the results.
Conclusion
Work negatively impacted more than half of the participants, who presented symptoms that may have developed or been aggravated by work activities, indicating that these symptoms may be associated with work task performance.
The workers included in this study exhibited a higher prevalence of WMSDs compared to that reported in studies involving the adult Brazilian population, particularly affecting the upper limbs and trunk, and were exposed to multiple risk factors for WMSDs associated with their working conditions. These findings highlight the need for effective ergonomic planning and targeted interventions to prevent WMSDs among this population and similar occupational groups, including improvements in work organization, reduction of workload related to excessive force, repetitive movements, and prolonged standing (orthostatism), as well as the implementation of appropriate work–rest cycles.
The need for additional research focusing on workers in this sector is reinforced, given the limited body of literature that adequately addresses the unique characteristics of restaurant environments and the occupations within them.
Footnotes
Acknowledgements
The authors would like to thank the workers who agreed to participate in the study.
Ethical approval
This cross-sectional study was approved by the Research Ethics Committee of the Federal University of Paraná, CAAE No. 75553517.1.0000.0102, under Opinion No. 2,327,563.
Informed consent
Prior to participation, all participants signed an Informed Consent Form.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.