
Abstract
Background
Accurate hand anthropometry underpins ergonomics, product design, medical applications, and occupational safety. Direct caliper-based measurement (DM) is labor-intensive and operator-dependent, whereas two-dimensional flatbed scanning (SC) has been advanced as a faster alternative, with validity for small anatomical landmarks remaining uncertain.
Objective
The objective of this study was to quantify between-method agreement and time efficiency of two-dimensional flatbed scanning (SC) relative to direct caliper measurement (DM).
Methods
In this study, 56 hand dimensions (36 lengths, 20 breadths) were obtained from 40 Thai adults (20 males, 20 females) by DM and SC. Between-method agreement were evaluated using mean absolute error (MAE), technical error of measurement (TEM), relative TEM (%TEM), and the coefficient of reliability (R). Time efficiency was quantified from average technician time and participant handling time.
Results
Pre-specified acceptability criteria (MAE ≤ 1 mm; TEM ≤ 2 cm; %TEM ≤ 1.5%; R ≥ 0.80) were satisfied by 42 of 56 dimensions (75%). Lengths and general breadths showed high agreement with the reference and strong repeatability (%TEM < 1.5%; R > 0.95), whereas small features—particularly finger-joint breadths < 25 mm—exhibited larger errors (%TEM 2.25–4.90%) and lower reliability (R < 0.80). Technician time was reduced from 30.85 to 14.10 min with SC, and participant handling was minimized (∼2.10 min).
Conclusion
Overall, SC can be adopted as a rapid, low-burden method for most hand dimensions, while refined protocols (e.g., increased image resolution, controlled hand pressure and posture, or equipment calibration) are indicated for sub-25-mm landmarks to ensure precision and strengthen population-specific anthropometric databases.
Keywords
Introduction
Anthropometric research provides essential data for the design of diverse products and services, spanning consumer accessories, workplace ergonomics, medical devices, and specialized systems such as aerospace and military platforms.1,2 Among anthropometric measures, hand dimensions are particularly critical because they directly influence design efficiency, user comfort, and operational safety. 3 Incorporating population-specific hand data reduces musculoskeletal strain and accidents associated with poor fit, and also supports forensic applications—e.g., analyses of ethnic and sex differences for identification.2,4,5 High-precision hand data are further required in medicine and medical device design (e.g., prosthetics, orthoses, surgical planning), safety-critical equipment and PPE, robotics and human–machine interfaces (e.g., data gloves, exoskeletons, control panels), and the fashion/luxury sector (e.g., rings, watches, specialized gloves), where millimeter-level deviations can affect outcomes and user satisfaction.
Standardized protocols such as ISO 7250–1:2017 define fundamental human body measurements and landmarks to support ergonomic design; within this framework, 11 hand-related dimensions (e.g., hand length, palm breadth, finger lengths) are specified. 6 For specialized applications, however, this baseline is insufficient. Expanded protocols now incorporate up to 86 hand variables to describe detailed morphology. 7 The reliability and repeatability of measurement systems remain essential, particularly in large-scale surveys where physiological variation, posture, landmark identification, instrument alignment, and inter-observer differences can degrade consistency.1,8–10 To support international comparability, a precision threshold of <1 mm has been recommended. 11
Multiple measurement approaches have been developed and are commonly categorized as one-dimensional (1D), two-dimensional (2D), and three-dimensional (3D). Traditional 1D methods using calipers and tape measures are simple and affordable but limited by operator variability and the lack of permanent digital records1,4,6,7,12 They are also labor-intensive, time-consuming, and prone to operator error.1,3,10,13 Imaging-based techniques include 2D photography and flatbed scanning, which enable faster acquisition and storage1,4,8,9,14–18 and 3D methods such as stereophotogrammetry and structured-light scanning, which provide volumetric data with greater precision.1,3,4,14,15 These techniques may nevertheless be affected by lighting, viewing angles, or cost constraints.12,15 Each method entails trade-offs in accuracy, efficiency, cost, and susceptibility to environmental or procedural errors. Of these, 2D flatbed scanning offers a practical balance for hand anthropometry because it is lower in cost, more widely accessible, and operationally simpler than 3D scanning systems, while still allowing permanent image capture and rapid extraction of planar dimensions. However, this practical advantage involves trade-offs: unlike 3D systems, flatbed scanning cannot adequately capture depth, curvature, or volumetric surface morphology. Previous studies have shown that 3D image analysis provides more comprehensive geometric and volumetric data with high agreement to direct measurement, but requires higher equipment cost and technical complexity, whereas 2D approaches are more efficient but limited to planar features. 15 Accordingly, the present study evaluated 2D flatbed scanning as a pragmatic alternative for planar hand measurements rather than as a replacement for higher-fidelity 3D scanning in applications requiring full three-dimensional characterization. Comparative evaluations of direct, 2D, and 3D methods are increasingly reported,1,4,15,19 yet practical reliability evidence remains limited. This study addresses that gap by assessing 2D flatbed scanning for hand anthropometry, testing whether scanner-based measurements can achieve agreement comparable to manual methods while reducing data-collection time. The analysis focuses on 56 hand dimensions, selected from the expanded set of 86 variables described in 7 that are measurable by both direct and scanner-based approaches.
Materials and methods
Scope of the study
Although ISO 7250-1:2017 specifies 11 fundamental hand dimensions, 6 subsequent reviews have expanded this set to 86 measurable variables categorized into five groups 7 : 37 length, 22 width and hand span, 13 depth, 11 circumference, and 3 diameter dimensions. However, because a flatbed scanner captures only two-dimensional information, it cannot record depth, circumference, or diameter measures. Consequently, only 56 dimensions—comprising 36 lengths and 20 widths—were selected for analysis, as these can be reliably obtained using both direct manual methods and 2D scanning. Figure 1 illustrates the dimensions included in this study, while Table 1 provides their detailed definitions.
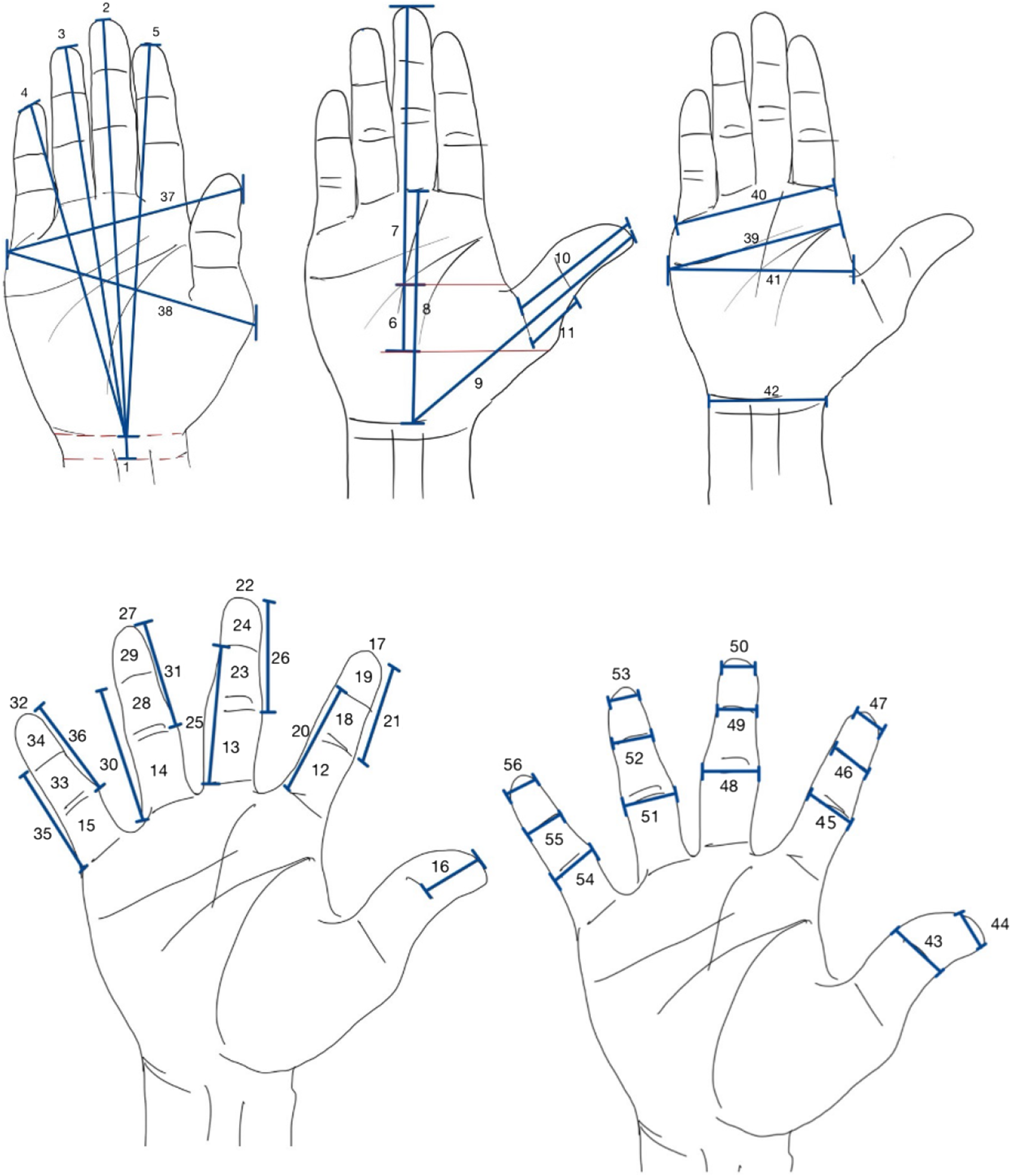
56-Dimension hand.
Definition of hand measurement (5,6,17,22–32).
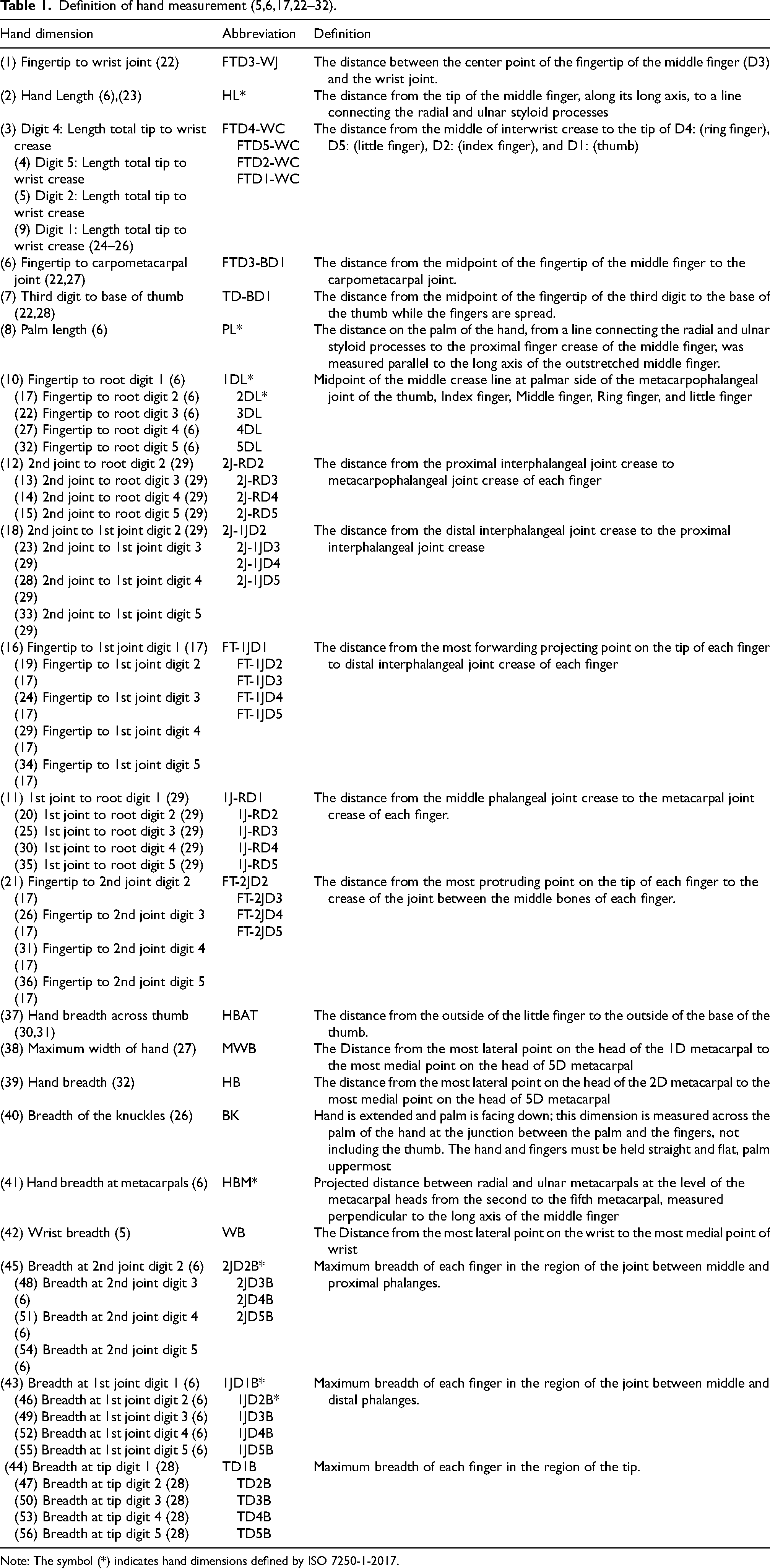
Note: The symbol (*) indicates hand dimensions defined by ISO 7250-1-2017.
The sample consisted of 40 Thai working-age individuals (20 males and 20 females) from southern Thailand, with a mean age of 36.36 ± 9.94 years. All participants were free from physical abnormalities or disabilities.4,20 Data collection focused exclusively on the dominant hand and was conducted between July and September 2024 by an occupational safety and health (OSH) academic with prior experience in hand measurement. To facilitate a smooth data collection process, the investigator fostered a supportive and friendly environment during participant interactions. All participants provided informed, voluntary consent to participate in the study. 21 The experimental protocol was approved by the Office of Human Research Ethics, Prince of Songkla University (No. PSU-HREC-2024-005-1-3).
The sample size of 40 participants was determined based on established anthropometric validation protocols. According to ISO 20685-1, 22 a minimum of 40 subjects is recommended to ensure sufficient sensitivity in detecting mean differences between measurement methods with approximately 95% confidence. This approach is commonly adopted in anthropometric and measurement reliability studies, where validation metrics such as TEM, %TEM, and reliability coefficients are prioritized over hypothesis-driven power calculations. In addition, previous studies in similar contexts have employed sample sizes ranging from 10 to 37 participants4,15,19,21,23–26 and have been considered adequate for evaluating measurement error and reliability. Therefore, the sample size used in this study is considered sufficient for assessing measurement agreement and reliability between methods. Moreover, the observed variability and agreement indicators in this study (e.g., MAE, %TEM, and R) further support that the sample size was sufficient to detect practically meaningful differences between methods.
Hand measurement techniques and data collection
The experimental procedure for obtaining measurements was divided into three stages:
Preparation stage
Preparation began with recording each participant's height and weight. All hand accessories were then removed, and participants received standardized instructions on the measurement procedure, including safety guidelines such as the option to pause or notify the researcher in case of discomfort. These steps ensured participants were adequately prepared for measurement. Next, 32 anatomical landmarks were marked on the dominant hand, as illustrated in Figure 2. These landmarks established the measurement boundaries and provided consistent reference points for positioning measuring devices across both methods, thereby enhancing the reliability and accuracy of the measurements. The measurements were taken in three standardized hand postures, as defined by ISO 7250-1:2017 and the guidelines reported in reference. 6

Landmarks identified and Hand posture: (a) posture 1: Finger Spread Position; (b) Posture 2: Fingers Closed Position; (c) Posture 3: Fingers Closed with Thumb Released Position.
Posture 1: Finger spread position
The participant raises the forearm horizontally with the palm facing downward. The hand was laid flat, and all five fingers were spread apart. This position is illustrated in Figure 2(a).6,19
Posture 2: fingers closed position
With the forearm raised and palm facing downward, the hand was placed flat on the surface, all fingers held closely together, and the thumb aligned with the side of the index finger (Figure 2(b)).
Posture 3: fingers closed with thumb released position
This posture is similar to Posture 2, but with the thumb extended outward from the hand, as shown in Figure 2(c).
The relevant anatomical landmarks, including the styloid process, are shown in Figure 1. Detailed descriptions and instruments for all 56 dimensions assessed in this study are presented in Table 1. Most definitions were adapted from previous studies,5,6,17,27–37 whereas those marked with an asterisk (*) were taken directly from ISO 7250-1:2017.
Several dimensions required special attention to ensure measurement accuracy. For example, for hand length (Dimension 2 – Hand Length), proper alignment of the wrist, fingertips, and forearm in a straight line was maintained. For hand breadth across the thumb (Dimension 37), participants were instructed to press the tip of the thumb firmly against the index finger to ensure consistency. For palm breadth excluding the thumb (Dimensions 39–41), participants kept the four fingers tightly together while extending the thumb outward and applying slight tension to stabilize hand shape. To minimize errors during large-scale data collection, visual diagrams indicating precise measurement locations were used in place of dimension names or abbreviations on the recording forms. This approach reduced the likelihood of misinterpretation and enhanced consistency across repeated measurements. In this study, all dimensions presented in Table 1 were measured with manual instruments and validated against measurements derived from 2D flatbed scanning.
Direct hand measurements were conducted using manual instruments, as illustrated in Figure 3, following the methods outlined in ISO 7250-1:2017. To standardize procedures, this study established specific protocols for the placement of instruments, identification of landmarks, and recording of measurements.
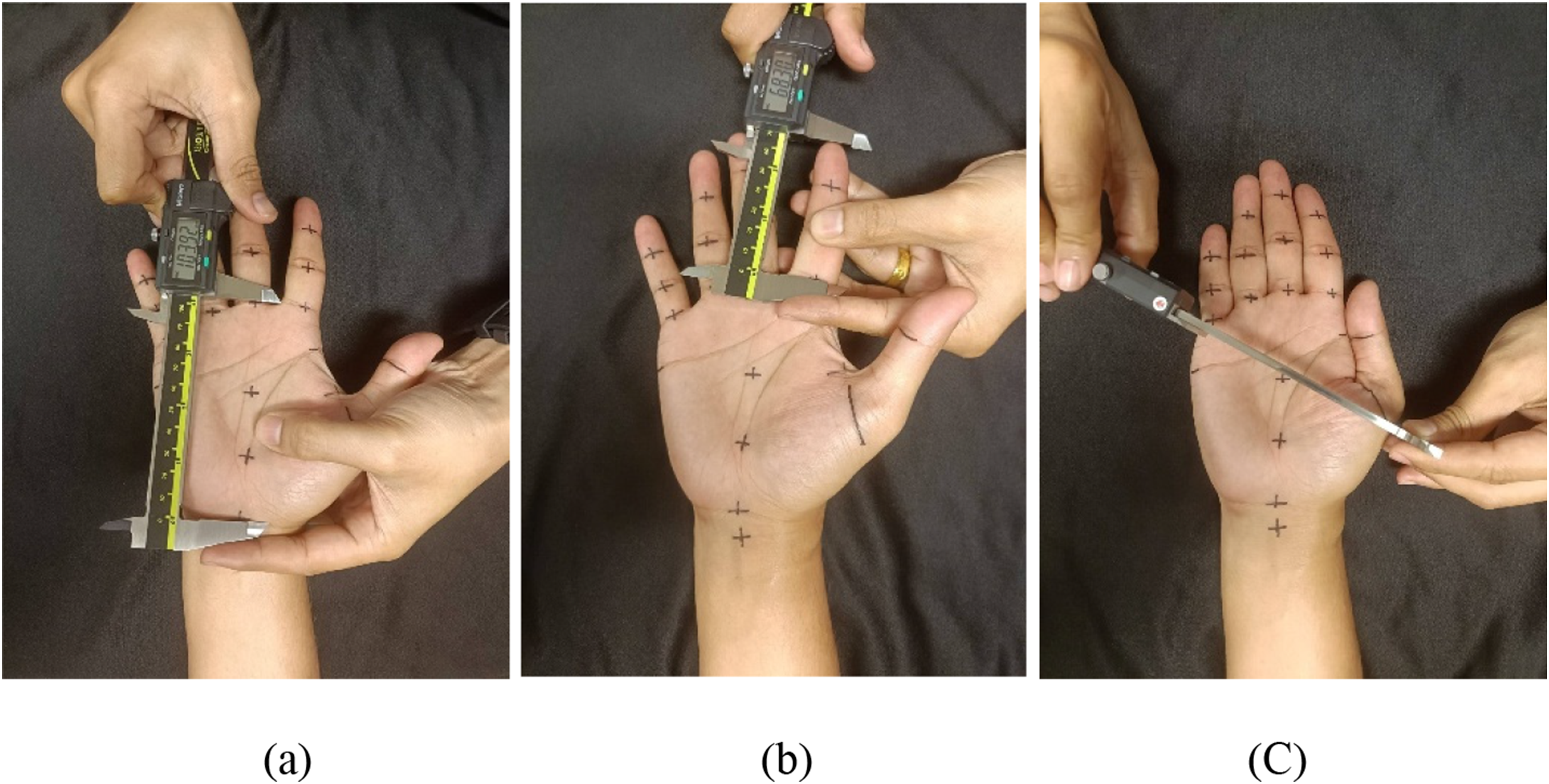
Traditional hand measurement by digimatic calipers: (a) example of measuring palm length (dimension 8); (b) example of measuring fingertip to root of digit 2 (dimension 17); and (c) example of measuring maximum width of hand (dimension 38).
To ensure precision, two digital calipers were used:
12-inch Digital Caliper (Digimatic Caliper, Code: 500-193-30, Model: 12 in): Used for dimensions 1, 2, 3, 4, 5, 6, 7, and 9. This device, compliant with ISO 13385-1, had a resolution of 0.01 mm and a measurement uncertainty of ±0.016 mm. 6-inch Digital Caliper (Digimatic Caliper, Code: 500-196-30, Model: 6 in): Used for all other dimensions and calibrated according to JIS B 7507:1993 and DIN 862:1988. This device shared the same resolution and uncertainty as the 12-inch caliper. Width measurements were similarly obtained using the 6-inch caliper, except for dimensions 37 and 38, which required the larger caliper due to a broader measurement range.
Although some experts recommend a maximum permissible error of 2 mm, 8 the calipers used in this study had a resolution of 0.01 mm and a precision uncertainty of ±0.016 mm, making the adoption of a 2 mm threshold unnecessary. To maintain consistency, the same set of instruments was used throughout the study. This approach minimized variability introduced by switching tools and enhanced the overall validity and reproducibility of the collected data. Each dimension was initially recorded once using predefined measurement procedures. When a measurement appeared inconsistent with the expected range for that dimension, it was not immediately repeated. Instead, all dimensions were first completed, and the identified dimensions were subsequently re-measured, with the average value used for analysis.
Repeated measurements were not systematically performed for all dimensions due to both practical and methodological considerations. In particular, direct hand anthropometric measurements are susceptible to soft tissue deformation, especially in regions with compliant tissues (e.g., fingertips and soft tissue pads). Repeated contact or pressure from measuring instruments may alter tissue shape and thickness, potentially introducing additional variability rather than improving measurement accuracy.
To minimize such effects, measurements were performed using standardized techniques with controlled pressure, and repetition was applied selectively only when necessary to ensure data quality. However, these strategies may reduce, but not completely eliminate, measurement error.
In all three postures, to achieve accurate measurements, the hand and wrist must be positioned in a straight line, with the fingertips and wrist lying flat and aligned on the scanner glass. Participants were instructed to place their hands gently on the scanner without applying pressure, ensuring that the hand remained flat and slightly tensed to preserve its natural shape. Additionally, real-time monitoring of the scanned images from all three postures was performed to detect excessive pressure, which could cause the fingers to flatten or distort. If such signs were observed, participants were advised to adjust their hand posture and repeat the scanning procedure.
The scanning method involved two main tools: (1) a 2D scanner with an anthropometric tape measure and (2) image processing software for dimension analysis.
1) A 2D Scanner with an Anthropometric Tape Measure
An Epson Perfection V850 Pro flatbed scanner was used to capture high-resolution images of the participants’ hands. This scanner supports resolutions up to 6400 dpi and operates at 4800 × 9600 dpi for both reflective and contact sheet scanning, ensuring excellent image clarity and detail.
To establish a measurement reference during scanning, a Rosscraft anthropometric tape measure—compliant with JIS B 7512 standards—was affixed to the hand placement area on the scanner, as shown in Figure 4. With a resolution of 0.07 mm, the tape measure was aligned in both horizontal and vertical orientations to provide accurate scale references within the scanned image.
2) Image Processing Software
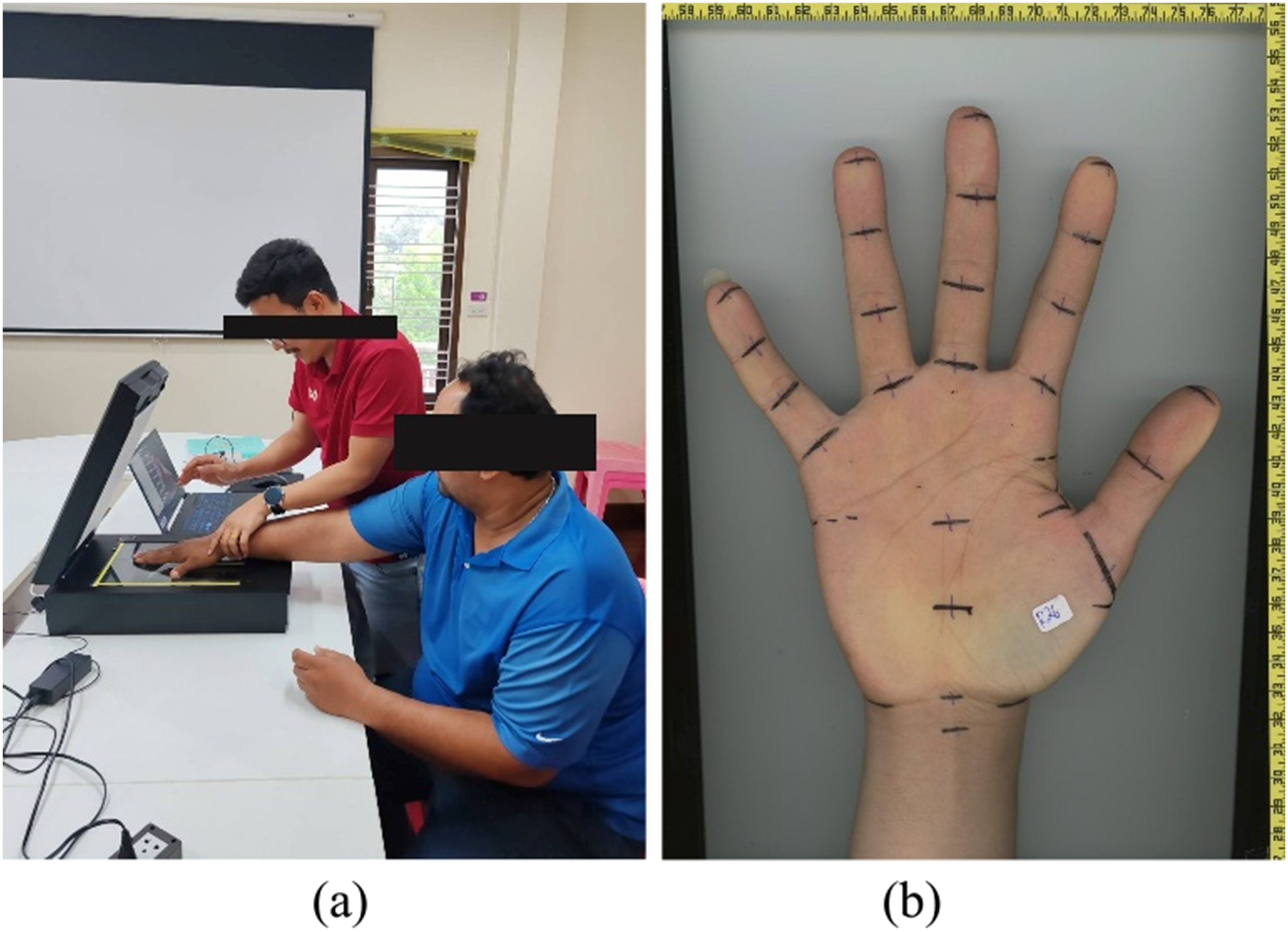
Hand measurement using a scanner and tape measure: (a) measurement using a hand scanner; and (b) scanned image showing the hand with tape markers as reference points.
ImageJ—a widely used software tool for image-based anthropometry—was employed for measurement analysis.4,38–40 The software's precise measurement functions allowed accurate assessment of 56 hand dimensions without the use of image enhancement techniques. Scanned hand images were saved in JPEG format at 600 dpi to preserve image quality. The “Set Scale” function in ImageJ was used to convert pixel measurements to real-world dimensions. This involved drawing a reference line along the tape measure in the scanned image and assigning it the corresponding length in centimeters, thereby calibrating the image to ensure accurate measurement conversion.
After processing, all measurements in centimeters were converted to millimeters using Microsoft Excel to standardize the dataset for subsequent statistical analysis. This approach ensured precision, consistency, and reproducibility throughout the measurement process, thereby reinforcing the reliability and validity of the data for further comparison and interpretation.
The precision of the measurement methods in this study was evaluated using four key indicators: Mean Absolute Error (MAE), Technical Error of Measurement (TEM), Relative Technical Error of Measurement (%TEM), and Coefficient of Reliability (R).4,9,11,21,23–26,41–44
For each hand dimension, all four key indicators were calculated using the following equations. From this point onward, D refers to values obtained from direct measurements, whereas S denotes values obtained from 2D flatbed scanning.
Mean absolute error (MAE)
The Mean Absolute Error (MAE) represents the average absolute difference between D and S. It is calculated by dividing the sum of absolute differences by the number of participants (n), as shown in Eq. (1).
The allowable difference between values obtained using the ISO 7250-1 method and alternative techniques should not exceed 1 mm for hand dimensions. 6
The Technical Error of Measurement (TEM) is a widely recognized indicator of measurement accuracy.4,9,11,21,23,24,41,42 Accurate estimation of TEM is critical for ensuring both the accuracy and reproducibility of anthropometric studies, as studies lacking TEM calculations often report significant errors.
25
TEM is calculated using Eq. (2).
Acceptable TEM values may vary depending on the evaluator's level of expertise,4,25,41,43 but a value below 2 cm is generally considered acceptable.
26
For further comparison, TEM can be expressed as a percentage relative to the mean measurement (%TEM):
A %TEM value exceeding 1.5% is regarded as unacceptable for most anthropometric measurements, while a threshold of ≤7.5% is accepted for subcutaneous fat assessments. 44
The coefficient of reliability (R) assesses the consistency and dependability of repeated measurements, reflecting the reproducibility of the measurement process.11,24 It is calculated using Eq. 4: < 0: No reliability 0–0.2: Slight reliability 0.2–0.4: Fair reliability 0.4–0.6: Moderate reliability 0.6–0.8: Substantial reliability 0.8–1.0: Almost perfect reliability.
Measurement analysis
A total of 56 hand dimensions—36 length-related and 20 width-related—were obtained from 40 working-age participants (20 males and 20 females). Measurements are presented separately for males and females in Tables 2 and 3. Dimensions 1–36 correspond to length, dimensions 37–42 to general breadth, and dimensions 43–56 to finger joint breadth.
Descriptive statistics of the measurement analysis (Male).

Descriptive statistics of the measurement analysis (Male).
Note: Direct measurements (D); scanner-based (S). Only a subset of data is shown; additional data points are omitted for brevity.
Descriptive statistics of the measurement analysis (Female).
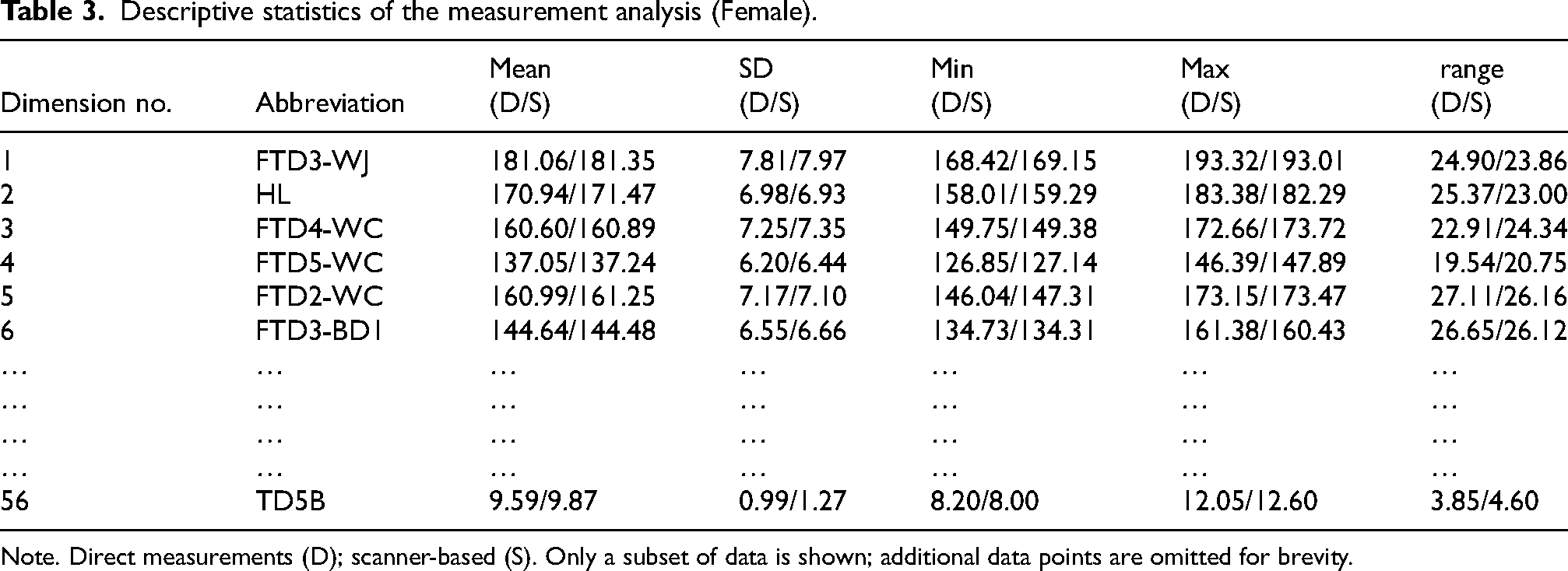
Note. Direct measurements (D); scanner-based (S). Only a subset of data is shown; additional data points are omitted for brevity.
Using direct measurements (D) as the reference standard, the accuracy, precision, and reliability of scanner-based (S) measurements were assessed. All key indicators (MAE, TEM, %TEM, and R) are summarized in Table 4. Results indicated that 42 of 56 dimensions—including hand length, finger length, and general hand breadth—met all criteria. The MAE ranged from 0.26–0.72 mm in males and 0.22–0.97 mm in females, all within the ISO 7250-1 tolerance of 1 mm. TEM values were consistently below 1 mm, further supporting the reliability of the scanner-based measurements. However, %TEM analysis highlighted limitations: while hand length, finger length, and general hand breadth remained below 1.5%, finger joint breadth dimensions exhibited elevated errors—ranging from 2.25–3.51% in males and 3.00–4.90% in females. These results indicate that smaller dimensions are more susceptible to measurement inaccuracies, even when absolute TEM values are comparable to those of larger dimensions. For instance, dimensions 22 (3DL) and 44 (TD1B) showed similar TEM values (0.43 mm and 0.56 mm, respectively), yet dimension 44 exceeded the %TEM limit due to its smaller mean size. This pattern was consistently observed across both sexes.
Measurement analysis (n = 40; F: 20, M: 20).
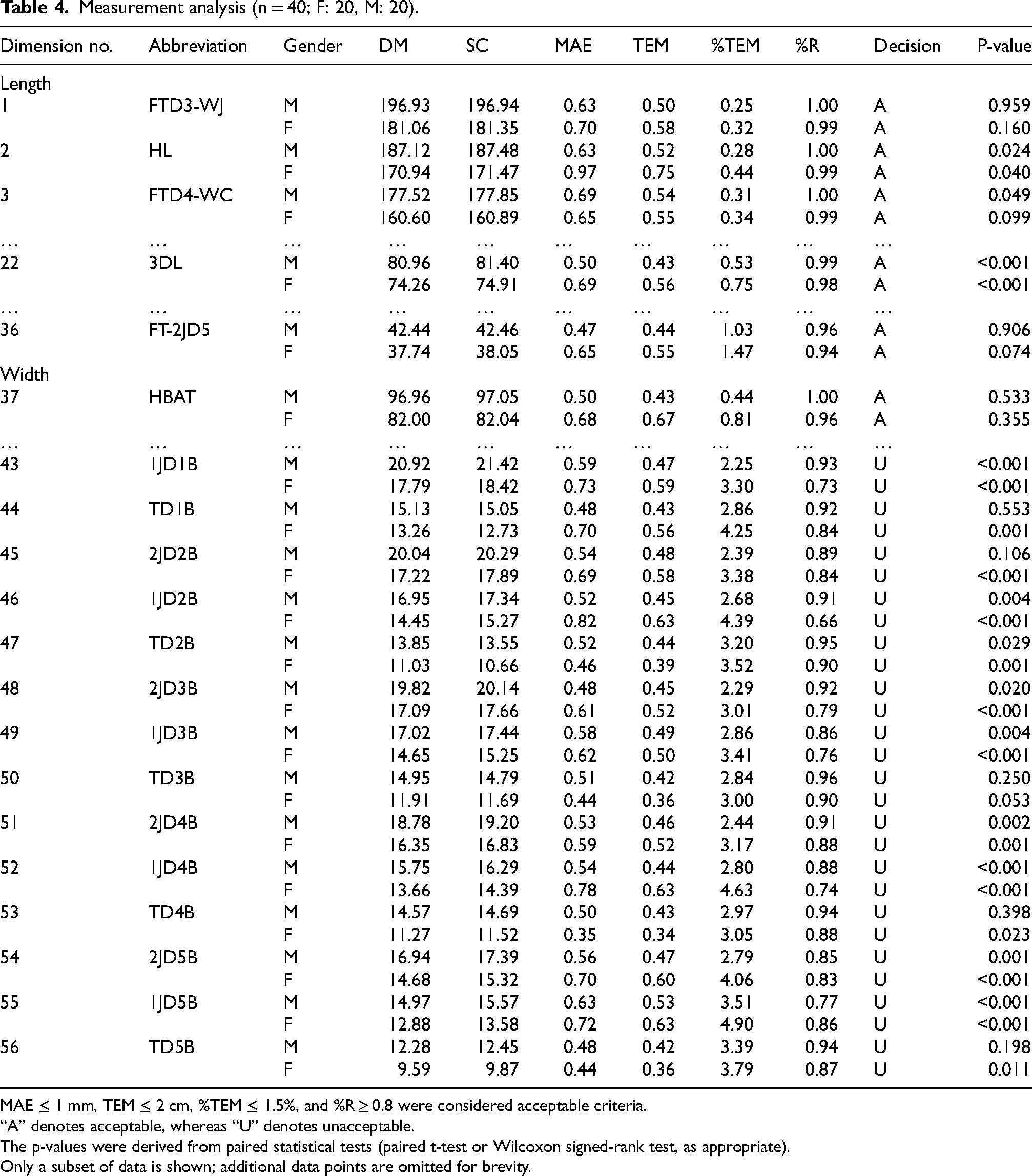
MAE ≤ 1 mm, TEM ≤ 2 cm, %TEM ≤ 1.5%, and %R ≥ 0.8 were considered acceptable criteria.
“A” denotes acceptable, whereas “U” denotes unacceptable.
The p-values were derived from paired statistical tests (paired t-test or Wilcoxon signed-rank test, as appropriate).
Only a subset of data is shown; additional data points are omitted for brevity.
Time analysis.

Reliability analysis revealed high R values (>0.95) for hand length and general breadth dimensions, demonstrating strong agreement between D and S. Conversely, finger joint breadths and dimensions below 25 mm again showed weaker correlations (R < 0.80), reflecting greater variability in these smaller-scale features. These discrepancies are likely attributable to technical challenges in S, including difficulty in defining anatomical landmarks and boundaries in complex, small regions, in contrast to the clearer landmarks used in hand length measurements.
As illustrated in Figure 5, most length dimensions achieved %TEM values below 1.5%, whereas finger joint breadth and other small-scale dimensions frequently exceeded this threshold. Notably, all dimensions smaller than 25 mm recorded elevated %TEM values and were disproportionately classified as “unacceptable” compared to dimensions larger than 50 mm. This finding underscores a fundamental limitation of S: although it performs reliably for larger hand dimensions, methodological refinements are required to improve its accuracy in capturing fine-scale anatomical features, particularly around finger joints.
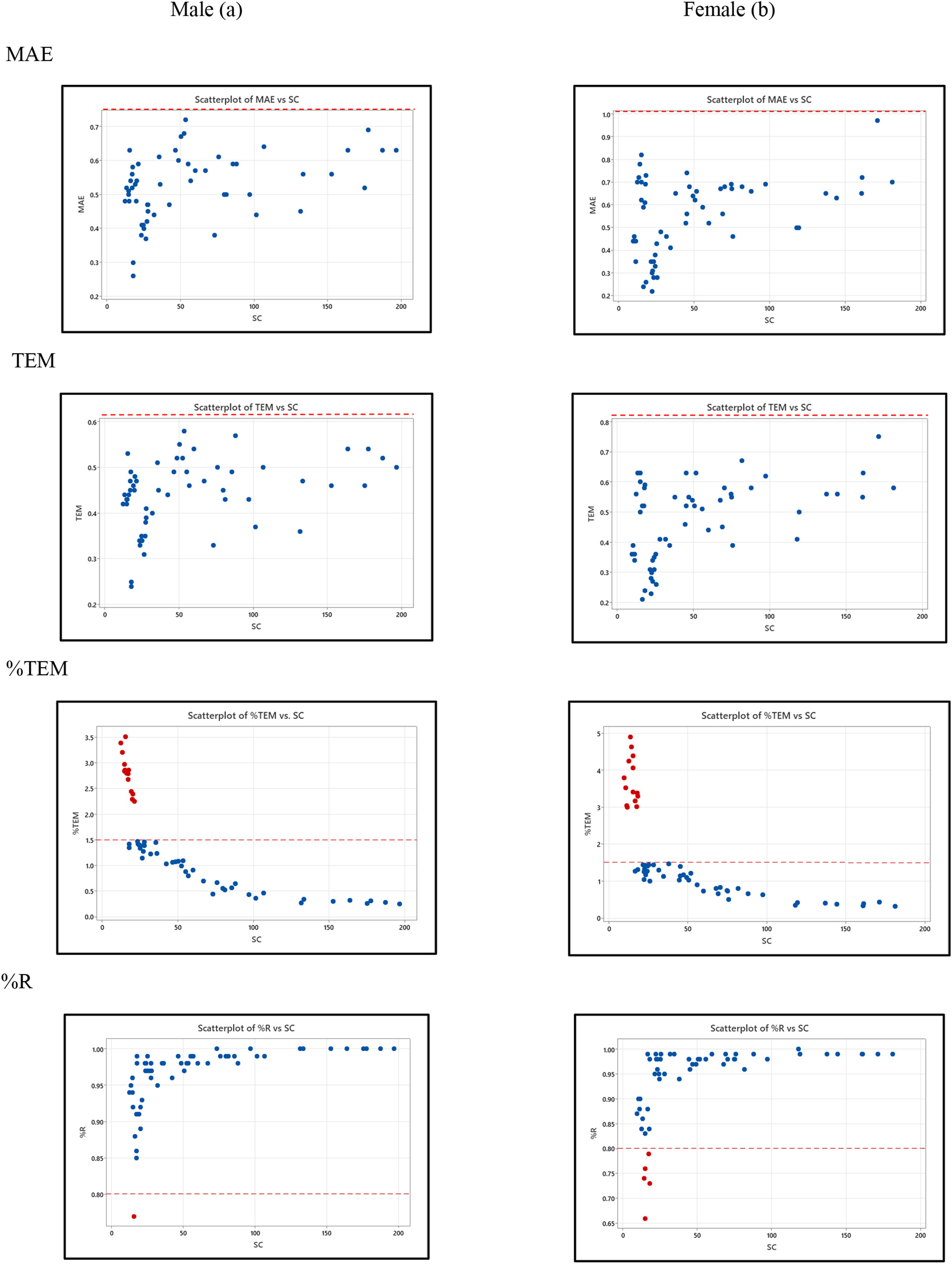
Distribution of hand dimension data over all 56 dimensions, categorized by gender: male (a) and female (b), for the 40 participants
Table 5 presents the time comparison between the direct measurement and scanner-based methods. Time comparisons between the two methods underscore the advantages of using the scanner. While direct measurement required 25.00–38.00 min per participant (mean = 30.85, SD = 3.10), the scanner-based method reduced the total time to 8.41–15.62 min for measurers (mean = 12.00, SD = 2.50) and only 1.15–3.23 min for participants (mean = 2.10, SD = 0.59). Although the latter involved additional image-processing time for measurers, the substantial reduction in participant involvement greatly enhances its practicality for large-scale anthropometric studies.
On average, the scanner shortened overall data collection to 14.10 min per participant—less than half the time required by the direct measurement—while participant burden was reduced from 30.85 min to just 2.10 min. These results highlight the scanner's potential in capturing larger hand dimensions, though further refinement is needed to improve the accuracy of small anatomical features, particularly finger joint breadths.
Discussion
In addition to accuracy and reliability, practical considerations such as cost, accessibility, and operational complexity play a critical role in selecting appropriate anthropometric measurement methods. Direct measurement methods are widely regarded as a reference standard due to their high accuracy and ability to identify anatomical landmarks through palpation; however, they are time-consuming and operator-dependent. Two-dimensional (2D) flatbed scanning offers a cost-effective and efficient alternative, enabling rapid data acquisition, reduced participant burden, and digital data storage, although it is limited in capturing complex anatomical features and three-dimensional morphology. In contrast, three-dimensional (3D) scanning technologies provide comprehensive geometric and volumetric data with high fidelity and strong agreement with direct measurement, but are associated with high equipment and software costs, technical complexity, and sensitivity to subject movement during acquisition. 45 Therefore, the choice of method should be guided by the intended application, required level of precision, and available resources. In this context, 2D scanning represents a practical compromise between accuracy and feasibility for large-scale anthropometric studies.
While the time-efficiency advantage of 2D flatbed scanning is clear, the discrepancies relative to ISO 7250-1:2017–compliant direct measurement warrant examination. Between-method differences vary across dimensions—typically larger for fine landmarks—reflecting uncertainty contributed by both methods. These discrepancies arise from factors associated with the measurer, the participant, and the measurement process; some are intrinsic, whereas others are amenable to control. By identifying their sources and implementing targeted measures (e.g., posture/pressure standardization, landmarking templates, device calibration, and higher-resolution or improved edge-detection settings), between-method agreement can be improved.
Sources of Measurement Errors and Control Measures of 2D Scanning
Measurement errors in 2D Scanning heavily depend on image quality and the precision of image processing software. When these factors are not properly configured or controlled, deviations may occur. Error mitigation in the scanner-based measurement therefore focuses on standardizing hand posture and minimizing pressure on the scanner surface. In this study, scanner calibration was not an issue because a pre-calibrated anthropometric reference tape was affixed to the scanning surface, and high-resolution scanning prevented image distortion, ensuring that discrepancies between scanned and actual dimensions were not due to image quality.
Based on a review of previous studies, commonly used scanning resolutions for hand anthropometry range from approximately 300 to 400 dpi. For example, prior studies have employed flatbed scanners such as the CanoScan LiDE 100 at 400 dpi, 46 the Epson Perfection V370 at 300 dpi, 38 and the CanoScan LiDE 110 at 300 dpi. 19
To minimize potential measurement error associated with insufficient image resolution, the present study employed a higher scanning resolution of 600 dpi. This setting was selected as a practical upper limit based on available equipment and was considered sufficient to improve boundary definition and measurement precision under the study conditions. During method development, higher resolution settings were also explored; however, increasing resolution beyond this level substantially increased scanning and processing time, which may introduce participant burden and reduce practical feasibility. Therefore, a trade-off between image quality and operational efficiency was considered.
Although a formal sensitivity analysis across multiple resolution levels was not conducted, all images were acquired and processed under standardized resolution and workflow conditions to ensure measurement consistency and reproducibility. Future studies should systematically evaluate the effects of different image resolutions and processing parameters to quantify their influence on measurement accuracy and reliability, particularly for fine-scale dimensions.
For small-scale dimensions (<25 mm), which showed reduced reliability, no dedicated corrective protocol was formally developed or experimentally validated. Nevertheless, the observed discrepancies can be explained by method-specific measurement characteristics. Prior to data collection, preliminary training with experienced anthropometrists and standardized measurement procedures were implemented to minimize measurement variability; however, no specific refined protocol targeting small-scale dimensions was developed.
In direct measurement, excessive pressure may compress soft tissue—particularly in regions lacking underlying bony support (e.g., fingertip areas)—leading to underestimation of true dimensions. This effect may be more pronounced in individuals with softer tissue characteristics.11,35,47 In contrast, scanner-based measurements rely on boundary detection of the outermost visible contour, which may result in slightly larger recorded values.
Despite attempts to minimize these sources of error during data collection, no formal validation was conducted to determine whether such adjustments could consistently improve reliability coefficients (R) to acceptable levels (i.e., R ≥ 0.80) for dimensions below 25 mm. When evaluated against these predefined acceptance criteria, these dimensions remained below acceptable reliability thresholds.
Therefore, these findings highlight the need for caution when interpreting small-scale measurements and support the continued use of direct measurement as the reference method for such dimensions. Under the current measurement conditions, scanner-based methods cannot reliably substitute direct measurement for fine-scale anatomical dimensions. Future studies should systematically evaluate refined protocols—such as controlled pressure application, positioning aids, and enhanced image analysis techniques—to improve measurement reliability in fine-scale anatomical features.
Posture-Induced Errors
Posture strongly affects the scanner-based measurement accuracy, particularly for hand length measured from the middle fingertip to the wrist. If the wrist is not placed flat on the glass, slight lifting or inward tilting shortens the recorded length. Twisting the wrist toward the thumb or little finger further distorts alignment, resulting in underestimated values. Similar findings have been reported in earlier studies1,15 which showed that bent fingers, uneven hand placement, or rotation during measurement produced curvature in the fingers and joints, leading to shortened lengths. Although repeated measurements in this study helped detect posture instability, these results highlight the need for strict posture control to reduce error. Uneven pressure when using calipers or tapes was also identified as a related error source.
Hand Pressure on the Scanner Surface
Another critical factor is the degree of hand pressure applied by participants. Excessive pressure compresses soft tissue, particularly in the fingers, producing visibly flattened and paler images due to tissue displacement. This compression artificially inflates finger breadth measurements, yielding wider dimensions than actual values. In contrast, minimal pressure produces dimensions more consistent with true anthropometric measurements.
Measuring Thumb Width
Unlike the direct measurement, where the thumb can be adjusted to achieve proper alignment, the scanner-based measurement does not allow repositioning during scanning. Consequently, the base of the thumb often tilts inward rather than lying flat, resulting in incomplete scans and measurement errors. This limitation was especially evident in width-related dimensions and is consistent with previous findings, 19 which reported posture-induced thumb rotation as a common source of inaccuracy.
Although no formal corrective protocol was implemented, postural and procedural guidance—such as standardized hand placement and visual checks—were applied during data collection to reduce thumb misalignment. In addition, all scanned images were systematically reviewed after acquisition across all hand positions to identify potential misalignment or incomplete contour capture. However, no hardware modifications or algorithmic corrections were applied, and this limitation could not be completely eliminated due to inherent constraints of the 2D scanning geometry and viewing angle. Consequently, thumb-related width dimensions remain susceptible to measurement error, and direct measurement is recommended as the reference method for these dimensions.
Practical Guidelines for Hand Measurement
Even with strict adherence to ISO 7250-1:2017 procedures, direct measurement remains susceptible to within-method variability and procedural limitations. The practice guidelines below are distilled from our experimental findings and are intended to mitigate controllable sources of discrepancy and improve between-method agreement.
1) Landmaking
Errors also arise from difficulties in identifying anatomical landmarks, which can bias measurers’ judgment and increase variability, particularly with traditional methods. Although scanning techniques rely on boundary detection, they too are affected by imprecise landmarking. Consistent with previous studies,26,48–51 this study confirms that accurate landmarking is essential for reliability. Among the 32 hand landmarks assessed, creases and bony protrusions were relatively easy to identify and supported accurate hand length measurement, while less visible bone joints required palpation and greater measurer expertise. For example, dimensions 6 and 7 involved locating the carpometacarpal joint and thumb base, and errors were common in width dimensions due to soft tissue and skin creases. Dimension 41 (palm width at the base of the thumb) was affected by tissue softness and required proper thumb positioning, whereas Dimension 42 (wrist width) was complicated by poorly defined wrist creases, requiring bone palpation. Overall, landmarks associated with creases were more reliable, whereas joint-related points and width dimensions were prone to greater variability due to skin elasticity, underscoring the need for specialized techniques.
2) Force Control
One major source of errors in width-related dimensions arises from inconsistencies in the force applied by measurers when using traditional instruments. Variations in the pressure exerted during device handling can lead to systematic discrepancies, as shown in Table 4 For example, for dimension 46 (breadth of the first knuckle of the index finger, 1JD2B), the direct measurement method produced an average of 16.95 mm for males, whereas the scanner-based measurement averaged 17.34 mm, yielding a difference of 0.39 mm. Among females, the discrepancy was larger, with averages of 14.45 mm and 15.27 mm, respectively (Δ = 0.82 mm). Similar trends were observed across dimensions 43–56, where the direct measurements consistently underestimated values compared with the scanner-based measurements.
The results indicated that the scanner-based measurements are generally larger than those obtained via the direct measurement, with more pronounced discrepancies in females. The primary explanation lies in the variability of applied force, particularly when measuring finger breadth. Softer tissue composition, such as subcutaneous fat layers, makes it challenging to maintain consistent pressure during the direct measurement, especially in females, whose hands tend to be softer than those of males. This tissue compressibility introduces variation in the direct measurement, whereas the scanner-based measurement, which captures image boundaries rather than relying on physical contact, avoids this source of discrepancy.
The findings of this study align with the research by Ulijaszek & Kerr (1999), 9 which examined measurement errors in anthropometry and nutritional assessments across various populations, including children, athletes, and older adults. Their study found that measurement errors commonly result from inconsistent pressure application when using calipers to measure subcutaneous fat thickness or from inaccurate identification of anatomical landmarks. It emphasizes the importance of standardizing measurement techniques and ensuring precise placement to reduce errors in anthropometric assessments.
Additionally, research by Oliveira et al., 21 investigated the technical measurement errors (TEM) among novice anthropologists in the Exercise and Physiology Laboratory (Labofise) at a Brazilian university. The study focused on three trainee anthropologists measuring nine subcutaneous fat sites according to International Society for the Advancement in Kinanthropometry (ISAK) standards. Most intra-measurer TEM values were within acceptable limits, except for subscapular skinfold measurements by the third measurer and thigh skinfold measurements by the second measurer, which exceeded the acceptable range. These errors were attributed to a lack of expertise in identifying the correct measurement points, insufficient tool handling precision, and inaccurate readings. These findings are consistent with studies.12,21,52
To reduce force-related variability, this study adopted a “light-touch” technique when using the direct measurement to measure finger breadth. While this approach helped minimize the compression effect, the scanner-based measurements still consistently exceeded their counterpart values. This discrepancy highlights an inherent limitation of the direct measurement: even with repeated trials and standardized protocols, variations caused by tissue softness and measurer-applied force cannot be fully eliminated.
Conclusions
The study conducted hand anthropometric measurements of working-age Thais using an indirect measurement method with a 2D hand scanner and compared the results with direct measurement methods. To evaluate the effectiveness of these methods in terms of time, precision, and reliability across 56 hand dimensions, key statistical indices TEM (Technical Error of Measurement), %TEM, and R (%R)—were calculated based on data from the study. These indices are widely used in research to assess interobserver reliability. The analysis found that the indirect measurement method (using a 2D scanner) could reliably replace the direct method in 42 out of 56 dimensions. This finding contributes to the development of an anthropometric database, supporting the creation of a national anthropometric database. In addition to reliability, the results demonstrated that the scanner-based method required less measurement time compared with the direct method, consistent with findings from previous studies. This advantage highlights its potential for large-scale anthropometric research and ergonomic applications by reducing participant burden and improving study feasibility. While various sources of measurement error were identified as both controllable and uncontrollable, one of the most critical factors ensuring accuracy is the reliability of measurement equipment. In this study, all measurement tools underwent calibration to ensure precision. Therefore, potential errors attributed to equipment inconsistencies were minimized, ensuring that measurement inaccuracies were primarily due to human and procedural factors rather than equipment limitations.
Limitations and directions for future studies
This study acknowledges several limitations that may influence the interpretation and application of its findings. First, although 3D scanning is widely recognized for its superior accuracy, its high cost and limited accessibility led this study to adopt 2D scanning (SC) as a practical alternative to direct measurement (DM). However, SC has inherent constraints, particularly in capturing depth-related anatomical features and complex surface geometries.
Second, intra-observer variability was not formally assessed. Although measurement procedures were standardized and operators received prior training, repeated measurements by the same operator were not conducted. This was partly due to practical constraints in data collection, as participation was voluntary and some participants were only available for a single measurement session, limiting the ability to perform repeated measurements under consistent conditions. In addition, this reflects the scope of the present study, which focused on comparing agreement between measurement methods rather than decomposing measurement system error.
Third, a formal Measurement System Analysis (MSA) was not performed to systematically identify and quantify sources of measurement error within the overall measurement process. In addition, inter-observer reliability was not evaluated, as measurements were conducted by a single operator to minimize inter-operator variability.
Future research should incorporate repeated measurements, intra- and inter-observer variability assessment, and structured MSA approaches to better distinguish operator-related variability from method-specific error and to further strengthen the reliability of anthropometric measurement systems. For applications involving multiple technicians, structured training, standardized protocols, and continuous monitoring of landmark identification, measurement technique, and potential systematic bias between operators are recommended to ensure consistency and scalability. In addition, further methodological refinement of scanner-based techniques is recommended to improve their applicability for fine-scale anatomical dimensions.
Footnotes
Acknowledgments
The authors sincerely appreciate the guidance and support from professors, colleagues, and staff at the School of Engineering, Prince of Songkla University. Special thanks are extended to the study participants and ergonomics experts for their valuable contributions, which greatly enhanced the study.
Ethical statement
The experimental protocol was approved by the Office of Human Research Ethics, Prince of Songkla University (No. PSU-HREC-2024-005-1-3).
Informed consent
All subjects signed consent forms in accordance with ethical approval.
Funding
This work was supported by the Prince of Songkla University Development Fund.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.