
Abstract
Background
Pregnancy induces spinal changes that are generally expected to resolve by the end of the puerperium. However, the mode of delivery may influence this recovery.
Purpose
This study aimed to assess pain-free active lumbar spine range of motion (ROM) in postpartum women following Cesarean birth (CB) or vaginal birth (VB), compared to women who had never been pregnant.
Methods
A cross-sectional analytical study included 66 women divided into three groups: Group A (n = 25, CB women), Group B (n = 16, VB women), and Group C (n = 25, controls). Lumbar ROM, including flexion, extension, bilateral side bending, and axial rotation, was measured using bubble inclinometers between the 6th and 12th postpartum weeks.
Results
The Kruskal-Wallis test showed significant differences were found among the groups in extension ROM (P = 0.002) and bilateral side bending ROM (P = 0.002 right, 0.004 left). Post-hoc analysis showed that CB women had significantly decreased extension ROM than controls (P = 0.001), and significantly decreased right and left side bending compared to both VB (P = 0.009, 0.013) and control groups (P = 0.010, 0.014). No significant differences were observed in flexion (P = 0.877) or axial rotation (P = 0.412 right, 0.753 left).
Conclusion
CB women exhibited persistent limitations in lumbar extension and side bending ROMs beyond the puerperium, possibly due to scar restrictions and core muscle weakness rather than pregnancy itself. VB women demonstrated spinal mobility more comparable to controls, suggesting VB may be more favorable for postpartum spinal recovery.
Introduction
Pregnancy or gestation can affect the maternal musculoskeletal system through its associated vascular, biomechanical, and hormonal adaptations. 1 As women progress from the first to the third trimester of pregnancy, some postural changes, such as increased lumbar lordosis, bilateral anterior pelvic tilt, sacral base angle, and a compensated posterior head position to maintain balance, are common. 2 Pregnant women may experience lower back discomfort, particularly during their third trimester. This discomfort can occur because of the enlarging uterus, which alters the lumbar spine biomechanics by increasing lumbar lordosis, which results in compensatory thoracic and pelvic adaptations.3,4
A Cesarean birth (CB) is a surgical operation that involves the delivery of one or more fetuses through both abdominal and uterine incisions. 5 Despite the national and international warnings, the Egyptian CB rate reached an alarming percentage of 72% in all births by the end of 2021, compared to the 21% worldwide CB rate of the same year.6,7 This type of birth and its related anesthesia may trigger different musculoskeletal dysfunctions during the postpartum period. For example, these dysfunctions may include but are not limited to abdominal muscle weakness, low back pain, and sacroiliac joint syndrome.8–12 Based on the previous CB-associated dysfunction, the lumbar spine biomechanics may be altered after CB. 13 Vaginal birth (VB) refers to the birth of a single fetus or, in some circumstances, a twin through the vagina (the normal birth canal). 14 VB is the more advantageous mode of birth because of the reduced morbidity and mortality rates compared to CB; however, the prevalence of sacroiliac dysfunctions was higher after VB than CB.15, 16 The WHO defines puerperium as the period that begins immediately after delivery of the newborn and extends up to 6 weeks postpartum, by which end most maternal adaptations to pregnancy return to the non-pregnant status.17,18
One of the axial skeleton's primary biomechanical functions is to allow the spine to move without restriction. 19 The lumbar spine's active range of motion (ROM) is one of the kinematic measurements for assessing the lumbar spine functions. 20 Kinematically, movements of the lumbar spine are flexion and extension (occurs through the sagittal plane), bilateral side bending (occurs through the coronal plane), and bilateral axial rotation (occurs through the transverse plane). 21 The normal lumbar spine's active ROM: for flexion is 50–70°, for extension is 10–30°, for side bending is 25–35°, and for axial rotation at the thoracolumbar junction is 20–40°. 22
Physical therapists for women's health are concerned with improving the quality of life for women throughout different stages of their lives, like during pregnancy, puerperium, and the delayed postpartum period (which can extend up to 24 weeks after delivery). 23 Although many studies evaluated lumbar spine adaptations during pregnancy (like the study of Daneau et al., 24 the study of Michnik et al., 25 and the study of Morino et al., 26 ), no studies assessed lumbar spine's active ROM in women after the end of the puerperium. So, this study was conducted to examine the pain-free lumbar spine's active ROMs after the end of puerperium among women who underwent CB or VB and compared it to the controls who had never experienced pregnancy. To our knowledge, this is the first study to investigate these variables.
The null hypothesis (H₀) stated that there is no significant difference in lumbar spine's ROMs among the three groups. The alternative hypothesis (H₁) stated that at least one group differs in the lumbar spine's ROMs.
Methods
Study design
A cross-sectional analytical study with retrospective categorization of exposure.
Settings
This research work was conducted at the Women's Health Teaching Hospital, South Valley University, Qena, Egypt. This work was performed between June 2021 and August 2023. Data about the candidate registry, like phone number, type of birth, and date of birth, was obtained from South Valley University Teaching Hospital's database. The personal data were taken from the candidates or assessed before the beginning of the study. These personal data included the name, height, body weight, BMI, previous history of specific low back pain, age, and parity (that describes the number of births of a 24-week or older newborn, regardless of being stillborn or alive 27 ). Candidates were contacted by phone. The candidates were asked to visit South Valley University Teaching Hospital to assess their lumbar spine active ROM. The index date of this study was 6–12 weeks postpartum for women of the CB and VB groups. This index date indicates the end of puerperium. Puerperium can be defined according to the World Health Organization (WHO) as the exclusive period that starts immediately following the birth of a newborn and lasts up to 42 days or 6 weeks postpartum. The underlying cause behind determining this index date was related to the return of most pregnancy-related physiological and anatomical changes to their pre-pregnancy status after the end of puerperium.17,18
Sample size calculation
Based on the obtained very large effect size (1.2) of CB on the lumbar extension ROM as calculated from our pilot study (the mean ± SD values of Post-cesarean lumbar extension ROM were 20° ± 6.54°, with 22 participants, and the mean ± SD values of the controls’ lumbar extension ROM were 26.82° ± 4.51°, with 22 participants). Using the G* power analysis, F-tests, with a large effect size of 0.4 for 3 groups, an alpha level of 0.05, and a power of 80%, we needed 66 participants.
Study candidates
66 women were enrolled and completed this study. Women were categorized into 3 groups: Group A: 25 mothers who experienced CB. Group B: 16 mothers who experienced only VB. The mothers of these 2 groups were primiparous (experienced only one birth) or multiparous (experienced more than one birth). Group C was the negative control group, which consisted of 25 females who did not experience pregnancy. Control candidates were restricted to nulliparous women to provide a baseline group without pregnancy-related musculoskeletal adaptations. Parous but non-postpartum women were not included, as prior pregnancies may leave persistent changes in abdominal musculature, lumbopelvic biomechanics, and fascial properties, even years after delivery. This approach ensured a more homogeneous reference group for valid comparison with postpartum women. Before measuring the outcome variables, all candidates were assessed for the severity of their postpartum low back pain (LBP); only women with mild and moderate severity nonspecific LBP on the visual analogue scale were included in the study. Nonspecific LBP refers to LBP that is not triggered due to a specific disease or disorder like an inflammatory disease, a fixed spinal deformity, infection, radicular syndromes, cauda equina syndrome, fractures, or tumors. 28 The classification of LBP severity was rated according to the VAS scoring system of Boonstra et al. 29 Our exclusion criteria included women who either complained of severe nonspecific LBP or those who complained of specific LBP, women who experienced VB with previous abdominal surgery, women older than 35 years, and women who did not continue all assessment procedures.
Bias reduction
More than one Researcher completed the measurements and data analysis. We kept a detailed personal record of every candidate throughout the steps of this research. We did not have any conflict of interest, we used a valid and reliable instrument, and we recruited the participants wisely. For example, we adjusted their age to range between 19 and 34 years because it is considered an effect modifier for different lumbar spine's active ROMs as understood from the study of Saidu et al. 30 Also, to minimize recall bias, information on the type and date of birth was extracted from the hospital registry and cross-verified with medical records. Whenever possible, reliance on maternal recall was avoided. Importantly, outcome variables (lumbar spine ROMs) were measured prospectively during clinical visits rather than through retrospective self-report.
Ethics statement
This study was approved by the Ethical Committee of the Faculty of Physical Therapy, South Valley University (Approval No: P.T - GYN-11/2024–556). The study protocol was registered on ClinicalTrials.gov (ID: NCT05538325). Before assessing our outcome variables, a written informed agreement form was obtained.
Variables of interest
In this research, the independent variables were CB and VB. The dependent variables were the pain-free active ROM of the lumbar spine: flexion, extension, bilateral side bending, and bilateral rotation. All the lumbar spine's active ROMs were measured in degrees from the starting position of a segment to its position at the end of its pain-free ROM.
Measurement of the dependent variables of interest
*Bubble Inclinometer: It was used to measure all lumbar spine's active ROMs for women in the three groups.
-Two bubble inclinometers (Baseline Bubble Inclinometer, model 12-1056, Fabrication Enterprises; White Plains, New York) were used to measure the angles of the lumbar spine's active ROMs.
- The bubble inclinometer is a highly reliable instrument for measuring the lumbar spine ROM in both healthy and low back pain subjects. The intraclass correlation coefficient (ICC) for within-day and between-day reliability was 0.770–0.982 and 0.835–0.977, respectively. 31 Also, it is a valid instrument for spinal ROM measurements, with a strong Pearson's correlation coefficient (r) of 0.72 to 0.84 when correlated to the electronic goniometer. 32
Assessment procedures for lumbar spine's active flexion and extension from the sagittal plane
-The 1st sacral vertebra's (S1) spinous process and the 12th thoracic vertebra's (T12) spinous process were used as reference points for measuring lumbar spine active ROMs: flexion and extension, as described by Magee et al. 33 ROM was measured using two inclinometers placed at T12 and S1 while the participant stood upright. For flexion, participants bent forward with knees extended; for extension, they bent backward. Isolated ROM was calculated by subtracting the S1 reading from the T12 reading, as described by Kolber et al. 34
Assessment procedures for lumbar spine's right and left active Side bending from the coronal plane
-Using the same landmarks and standing position, inclinometers were aligned in the frontal plane. Participants slid one hand down the corresponding leg side without trunk flexion or knee bend. Isolated ROM was calculated by subtracting the S1 reading from the T12 reading, as described by Sadeghi et al. 31 Both sides were tested.
Assessment procedures for lumbar spine's right and left active axial rotation from the transverse plane
− We used only T12 as a reference point for measuring the active ROM of right and left lumbar axial rotation. This point was solely used because the majority of lumbar rotation ROM comes from the thoracolumbar region, with only about 5° occurring purely at the lumbar spine, in the case of a fixed flexed pelvis on the femur, as illustrated by Neumann,. 35 Participants bent forward (nearly 90° hip flexion) with arms crossed, then rotated the trunk to each side without pelvic movement. ROM was recorded directly from T12.
Data collection
Data were screened for the normality assumption test using the Shapiro-Wilk test. It yielded a non-normal distribution in all variables except for age and BMI. Non-parametric analysis was carried out for the non-normally distributed variables, while parametric analysis was carried out for the normally distributed variables.
Statistical analysis
The SPSS Package program version 25 for Windows (SPSS, Inc., Chicago, IL) was used to complete the consecutive statistical procedures:
− − − − − The level of significance in all statistical analyses was 0.05 of probability (i.e., P ≤ 0.05).
Results
Demographic characteristics of the candidates
Based on the three groups in this study, Group A: Cesarean birth (CB), Group B: Vaginal birth (VB), and Group C: Nulliparous controls (never pregnant), the mean ± SD scores of ages measured in years for the three groups A, B, and C equaled 25.3 ± 4, 26.4 ± 2.8, and 25.0 ± 2.6, respectively. The mean ± SD scores of BMI measured in kg/m2 for the three groups A, B, and C equaled 24.7 ± 2.3, 24.4 ± 2.7, and 24.4 ± 3.9, respectively. The mean ± SD scores of parity (referring to the number of births for groups A and B were 2.1 ± 1.2, and 2.1 ± 1.2, respectively. The mean ± SD scores of PPD measured in weeks for the two groups A and B were 7.7 ± 1.7, and 8.6 ± 2.4, respectively (Table 1). The demographic characteristics showed non-significant differences among the three groups in age (P = 0.351) and BMI (P = 0.920) as determined by the one-way ANOVA test. Although the Kruskal-Wallis H test revealed significant differences in parity (P = 0.000) and PPD (P = 0.000) across the three groups, pairwise comparisons indicated non-significant differences between CB and VB women for either parity (P = 1.000) or PPD (P = 0.912).
Descriptive statistics of the demographic characteristics among candidates of the three groups.
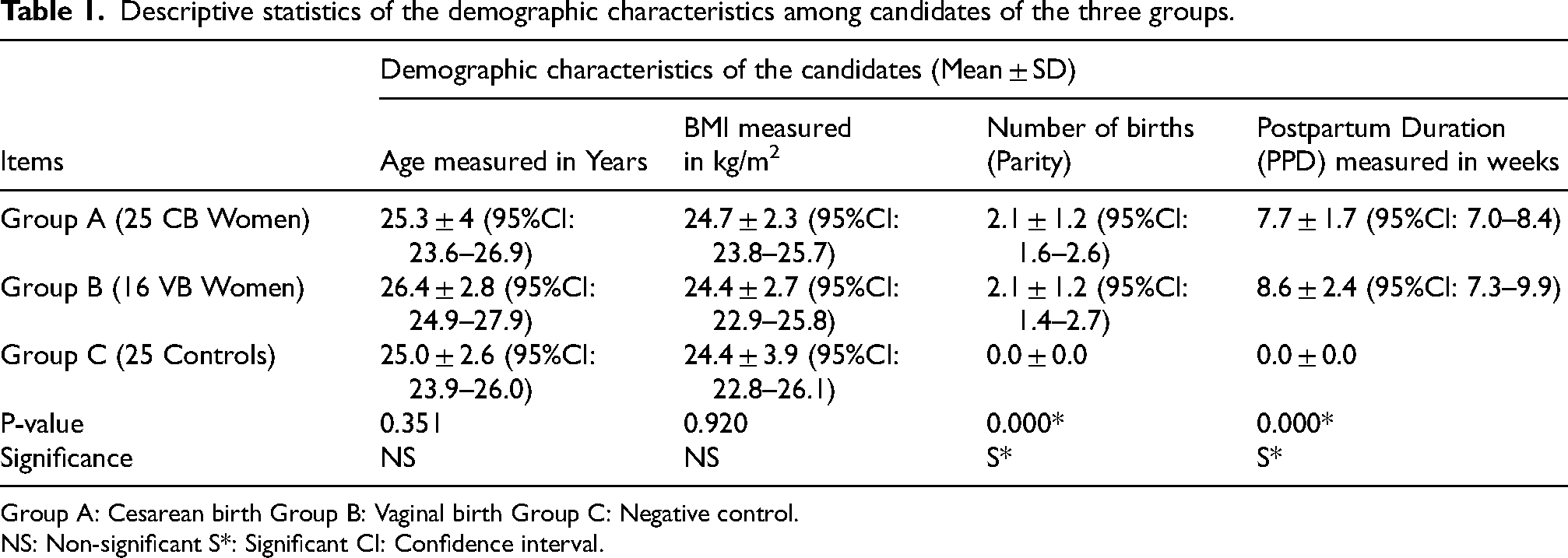
Group A: Cesarean birth Group B: Vaginal birth Group C: Negative control.
NS: Non-significant S*: Significant CI: Confidence interval.
The Kruskal-Wallis H test & Bonferroni correction for multiple tests (post-hoc test)
The Kruskal-Wallis H test for all lumbar spine's active ROMs
The mean ± SD values of lumbar flexion active ROM for groups A, B, and C equaled
54.6° ± 5.8 (95%CI: 52.2–57.0), 55.0° ± 4.5 (95%CI: 52.6–57.4), and 55.2° ± 6.0 (95%CI: 52.7–57.7), respectively. The mean ± SD values of lumbar extension active ROM for groups A, B, and C equaled 20.0° ± 6.6 (95%CI: 17.3–22.7), 23.8° ± 5.9 (95%CI: 20.6–26.9), and 26.6° ± 4.5 (95%CI: 24.7–28.5), respectively. The mean ± SD values of lumbar right side bending active ROM for groups A, B, and C equaled 16.0° ± 5.6 (95%CI: 13.7–18.3), 20.6° ± 4.4 (95%CI: 18.3–23.0), and 20.6° ± 6.0 (95%CI: 18.1–23.1), respectively. The mean ± SD values of lumbar left side bending active ROM for groups A, B, and C equaled 15.4° ± 5.4 (95%CI: 13.2–17.6), 20.3° ± 4.3 (95%CI: 18.0–22.6), and 20.0° ± 6.1 (95%CI: 17.5–22.5), respectively. The mean ± SD values of lumbar right axial rotation active ROM for groups A, B, and C equaled 17.6° ± 8.2 (95%CI: 14.2–21.0), 20.0° ± 4.5 (95%CI: 17.6–22.4), and 21.0° ± 7.8 (95%CI: 17.8–24.2), respectively. The mean ± SD values of lumbar left axial rotation active ROM for groups A, B, and C equaled 19.4° ± 7.7 (95%CI: 16.2–22.6), 19.4° ± 5.1 (95%CI: 16.6–22.1), and 21.6° ± 8.6 (95%CI: 18.0–25.2), respectively. The Kruskal-Wallis H test revealed significant differences among the three groups in lumbar extension (P = 0.002), lumbar right-side bending (P = 0.002), and lumbar left side bending (P = 0.004), although, it revealed non-significant differences among the three groups in lumbar flexion (P = 0.877), lumbar right axial rotation (P = 0.412), and lumbar left axial rotation (P = 0.753) (Table 2).
Kruskal-Wallis test of the lumbar spine's active ROMs among the 3 groups.

Group A: Cesarean birth Group B: Vaginal birth Group C: Negative control.
S*: Significant NS: Non-significant CI: Confidence interval.
-The Post-hoc power analysis using the G*Power, indicated 99% power for lumbar extension ROM (using an effect size f of 0.584, number of participants of 66, and number of groups 3, and an alpha level of 0.05). Also, it indicated 91% power for lumbar right side bending ROM (using an effect size f of 0.456, number of participants of 66, and number of groups 3, and an alpha level of 0.05). Additionally, it indicated 93.6% power for lumbar left side bending ROM (using an effect size f of 0.48, number of participants of 66, and number of groups 3, and an alpha level of 0.05). These power analyses indicate sufficient and high powers to detect differences in these lumbar ROMs among these three groups and decrease the liability of committing type II errors, meaning the null hypothesis is not rejected when, in reality, a significant difference does exist. This study sets an alpha level of 0.05, which means there is a 5% chance of committing a Type I error by rejecting a true null hypothesis. The study's critical value from the chi-squared table was 5.99. The calculated H value for lumbar extension, right, and left side bending were (H: 12.2, 12.1, and 11.2), respectively. As these H values of the Kruskal-Wallis test are greater than 5.99, we can trust in the statistical significance of these ROMs by rejecting the null hypothesis.
The post-hoc test (Bonferroni correction for multiple tests) for the variables showed statistically significant differences
− The post-hoc test revealed significant differences in parity (number of births) between groups A&C (MD = 2.1, P = 0.000), and B&C (MD = -2.1, P = 0.000). However, it revealed a non-significant difference between A&B (MD = 0.0, P = 1.000), which confirms comparable baseline characteristics of Parity between CB and VB women.
− The post-hoc test revealed significant differences in postpartum duration (PPD) between groups A&C (MD = 7.7, P = 0.000), and B&C (MD = 8.6, P = 0.000). However, it revealed a non-significant difference between A&B (MD = -0.9, P = 0.912), which confirms comparable baseline characteristics of PPD between CB and VB women.
− The post-hoc test revealed a significant difference in lumbar extension between groups A&C (MD = -6.6, P = 0.001). However, it revealed non-significant differences between B&C (MD = -2.8, P = 0.512), and A&B (MD = -3.8, P = 0.258) (Table 3). Despite the non-significant difference between group A (CB) and group B (VB), there was a moderate effect size of 0.6 using Cohen's d formula with a pooled SD of 6.34.
− The post-hoc test revealed significant differences in lumbar right side bending between groups A&C (MD = -3.4, P = 0.010), and A&B (MD = -2.4, P = 0.009). However, it revealed a non-significant difference between B&C (MD = -1.0, P = 1.000) (Table 3).
− The post-hoc test revealed significant differences in lumbar left side bending between groups A&C (MD = -2.2, P = 0.014), and A&B (MD = 0.0, P = 0.013). However, it revealed a non-significant difference between B&C (MD = -2.2, P = 1.000) (Table 3).
Discussion
Both pregnancy and childbirth make changes to the whole maternal musculoskeletal system, especially the lower back region.36,37 By the end of the 6th week of the postpartum period, most major changes return to the pre-pregnant condition 18 ; however, some lumbopelvic measures, including the lumbar spine's muscles, may continue changing even after the end of puerperium up to 3–6 months postpartum.38,39
The post-hoc test (Bonferroni correction for multiple tests) among the 3 groups for lumbar extension, right axial rotation, and left axial rotation.
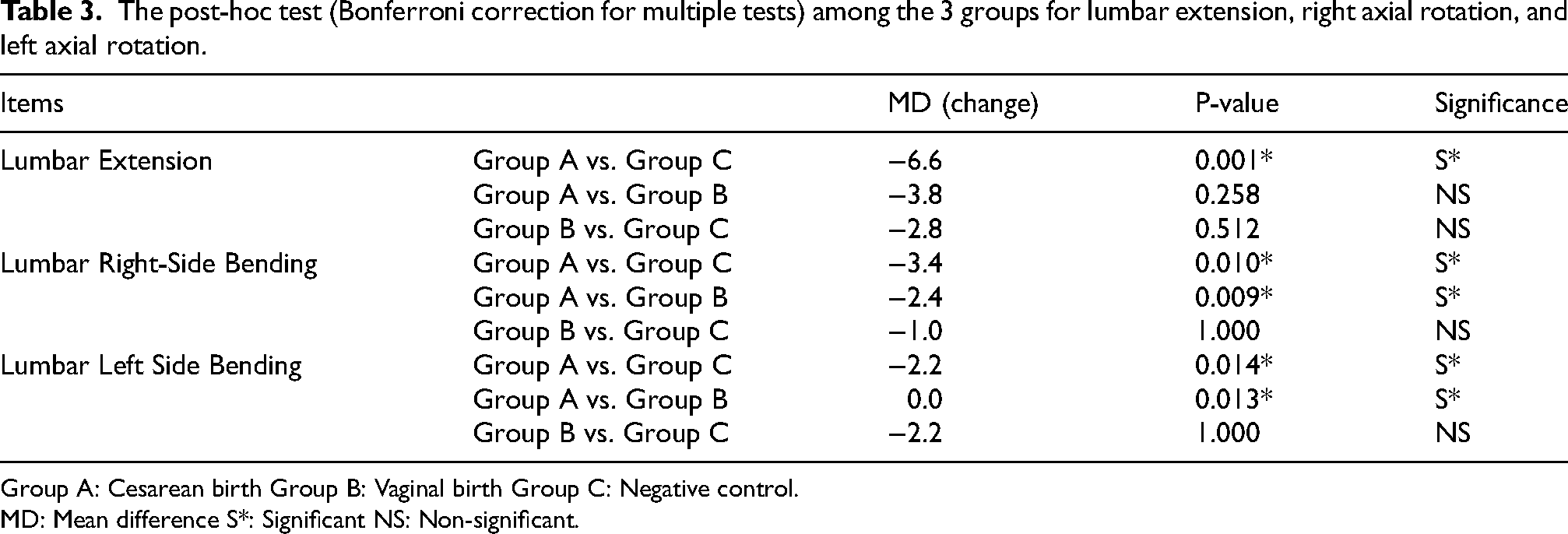
Group A: Cesarean birth Group B: Vaginal birth Group C: Negative control.
MD: Mean difference S*: Significant NS: Non-significant.
The present study revealed significant decreases in lumbar extension and bilateral side bending ROMs in women who experienced CB compared to the controls. Additionally, CB women showed significant decreases in bilateral side bending ROMs compared to VB women. The notable decrease in lumbar extension and bilateral side bending after CB may be attributed to the restrictive effects of the abdominal CB scar. This can be explained by the fact that extension and side bending occur in the sagittal and coronal planes, respectively, and both movements apply tensile forces on the scar, requiring it to be elastic for full ROM. However, the scar tissue of incised muscles and surrounding connective tissue undergoes a fibrotic, scar-mediated healing process after surgery, which impairs ROM restoration and complicates the reacquisition of normal biomechanical characteristics. 40 Additionally, core muscle weakness in the abdominal obliques following CB trauma may limit spinal mobility, as these muscles are primarily recruited during lumbar side bending.
Although this study found that CB women had lower lumbar extension ROM than VB women, the decrease was not statistically significant. The moderate effect size (Cohen's d = 0.6) suggests potential clinical relevance. This finding indicates that women who undergo CB may benefit from postpartum interventions aimed at improving lumbar extension mobility, enhancing core strength, and addressing scar tissue restrictions to help prevent long-term functional impairments. This non-significant decrease may be due to similar pregnancy-related postural adaptations in both groups, including ligamentous laxity, altered spinal alignment, and abdominal muscle weakening, all of which can affect spinal mobility. Additionally, unlike side bending, which heavily involves the abdominal obliques, lumbar extension primarily depends on the erector spinae, multifidus, and hip extensors (gluteus maximus and hamstrings). Since CB primarily affects the abdominal muscles rather than the back and hip extensors, its impact on lumbar extension may be less pronounced than on other movements. This study also found that VB women had lower lumbar extension ROM than the controls who had never experienced pregnancy. However, this decrease was not statistically significant. While pregnancy-related postural adaptations may slightly restrict lumbar extension, the additional restrictive effect of the CB incision, combined with these adaptations, may explain the greater reduction in lumbar extension ROM observed in CB women compared to the controls.
The results of this study revealed non-significant changes in lumbar flexion and bilateral axial rotation ROMs among the three groups. A possible explanation for these findings is, first, in postpartum women, the hip flexors may compensate for weak abdominal muscles, potentially making flexion less restricted. Second, lumbar flexion ROM does not require scar elasticity, as the movement direction involves scar compression rather than tension. Meanwhile, axial rotation, when measured at the thoracolumbar junction from a 90° flexed trunk position, does not place significant tension on the scar site.
The findings of this research regarding the marked decrease in lumbar active extension and side bending in women experiencing CB come in agreement with the research of Coulton et al., 41 which revealed a decreased lumbar extension and left side bending active ROM in a postpartum woman who gave birth by CB. On the other side, we found non-significant differences in all postpartum lumbar spine active ROMs of women who experienced VB when compared to those of the control group. This may disagree with the results of Corso et al., 42 who found restricted lumbar extension, side bending, and rotation ROMs in a woman who experienced VB.
This study has considerable strengths, such as: first, being the primary study that assessed the lumbar spine's active ROMs after CB and VB, and compared it to the controls who had never experienced pregnancy. Second, assessing multiple outcomes. Third, using reliable, valid, and modern instruments in the assessment. Fourth, this study compared women of the CB group to those of the VB group, which may rule out the confounding influence of pregnancy on the outcome variables in the case of comparing one of the two groups to the negative control group only. At the same time, we had some limitations. First, the main limitation of employing an analytical cross-sectional design with retrospective exposure classification rather than a prospective cohort is that it restricts the ability to establish temporal relationships between exposure and outcomes. In a prospective design, the same women could be assessed both before pregnancy and after completion of the puerperium following CB or VB, which would provide a more precise evaluation of whether kinematic lumbar measures return to the pre-pregnant status. In contrast, the retrospective approach relies on comparisons with a control group, which may introduce selection bias and limit causal inferences. Second, although sacroiliac dysfunctions may correlate to LBP and so on in the lumbar spine's active ROM, as understood from the study of Capobianco and Cher. 43 Evaluation for sacroiliac joints was neither included during participant recruitment. In addition, although women with specific LBP and those with moderate to severe nonspecific LBP were excluded, we did not quantify subclinical pain or apply standardized pain scoring tools at the time of lumbar ROM testing. This may have introduced unmeasured variability due to differences in individual pain thresholds or guarding behavior. Third, the study's findings may have limited generalizability due to the small overall sample size. The low number of participants in the VB group likely reflects the difficulty in recruiting women who had undergone VB in Egypt, given the substantial rise in CB rates. However, this limitation may reduce the generalizability of the results. Fourth, assessors were not blinded to group allocation, which may introduce potential measurement bias. Fifth, while we referenced literature supporting the reliability of the bubble inclinometer, we acknowledge that reliability data were not collected from the current sample.
The clinical value of this study may be clarified in its guidance to the Physical therapists who provide postpartum care to take into consideration that women who finished their puerperium after CB still have a marked decrease in lumbar extension and side bending active ROMs. These limited movements may be one of the risk factors for delayed postpartum LBP. Also, these results emphasize the potential benefits of VB in maintaining musculoskeletal health, reinforcing the importance of strategies that support and encourage safe VB whenever possible. Our findings complement those of the recent study of Ali et al. 44 , who reported that cesarean birth is associated with greater postpartum non-specific low back pain and reduced transversus abdominis strength compared to vaginal birth. In line with this, we observed that CB women exhibited persistent reductions in bilateral lumbar side-bending and extension ROM, whereas VB women regained ROM values comparable to controls by the end of the puerperium. We recommend further studies with a prospective design and a larger sample size be conducted. Such studies could examine the effects of interventions like abdominal Cesarean scar myofascial release and/or core muscle training on lumbar spine mobility. The use of objective assessment tools, including ultrasound imaging, electromyography (EMG), and fascial mobility evaluation, is also encouraged to better understand the biomechanical mechanisms involved. Additionally, studies comparing active and passive lumbar ROM in postpartum women are encouraged, as they may help identify contributing risk factors. We also recommend that future studies incorporate standardized pain scoring systems to further control for pain-related variability in lumbar mobility. Furthermore, future studies should consider including parous women who are not in the immediate postpartum period to allow for a more rigorous and comprehensive comparison.
Conclusion
CB women exhibited observed decreases in bilateral lumbar side bending ROM compared to both VB women and controls, as well as an observed decrease in lumbar extension ROM compared to controls only. This decline in active lumbar ROM may be attributed to core muscle weakness and/or the restrictive effects of the CB incision scar. By the end of the puerperium, only VB women regained lumbar ROMs comparable to those who never had experienced pregnancy, whereas CB women remained limited in specific ROMs, suggesting that delivery mode influences postpartum spinal mobility. Women's health physical therapists should consider these ROMs’ limitations in postpartum rehabilitation. Advanced core strengthening, particularly for the abdominal obliques, along with cautious manual scar release after six weeks post-CB, may help restore mobility. Future studies with larger sample sizes are needed to enhance the generalizability of these findings.
Footnotes
Acknowledgment
The Princess Nourah Bint Abdulrahman University Researchers’ Supporting Project number (PNURSP2025R117), Princess Nourah Bint Abdulrahman University, Riyadh, Saudi Arabia, supported this study. Best regards to all candidates who kindly completed this study.
Informed consent statement
Written informed consent was obtained from all subjects involved in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Princess Nourah Bint Abdulrahman University Researchers’ Supporting Project number (PNURSP2025R117), Princess Nourah Bint Abdulrahman University, Riyadh, Saudi Arabia, supported this study.
Conflict of interest
The authors confirm that they are free of conflicts of interest.
Data availability statement
The data from this study can be obtained upon request from the corresponding author. Due to ethical considerations, the data are not publicly accessible.
Institutional review board statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the Faculty of Physical Therapy, South Valley University (Approval No: P.T - GYN-112024–556).