
Abstract
Background
Chronic nonspecific low back pain (CNLBP) is linked to changes in trunk motor control, often presenting as increased movement regularity. Entropy-based metrics quantify such alterations in motor variability, yet evidence remains fragmented.
Objective
The present study aims to systematically review studies employing entropy measures to assess trunk movement regularity in individuals with and without CNLBP.
Methods
A comprehensive search was conducted across nine databases, including PubMed, Scopus, and Embase. Cross-sectional studies comparing CNLBP participants to healthy controls were included. Two independent reviewers handled study selection, data extraction, and risk of bias assessment.
Results
Five studies (n =222) met the inclusion criteria. Of the 222 participants in the pooled dataset, 42% were healthy controls and 58% had CNLBP, with an age range of 24.5 to 56.75 years. The weighted mean age across studies was approximately 43 years. Higher entropy (i.e., lower regularity) was observed in postural and gait tasks among CNLBP individuals. Conversely, reduced entropy (i.e., higher regularity) was noted in flexion-extension tasks, highlighting task-specific motor adaptations.
Conclusion
CNLBP is associated with task-dependent alterations in trunk movement regularity. Future research should standardize entropy computation and data collection protocols to enhance study comparability and clinical applicability.
Introduction
Chronic non-specific low back pain (CNLBP) is one of the most prevalent musculoskeletal disorders worldwide, leading to functional impairments, reduced quality of life, and a substantial socioeconomic burden. 1 CNLBP is associated with altered motor control in the kinematic chains, such as gait dysfunctions. 2 Moreover, changes in trunk coordination and erector spine activity have been reported as direct consequences of CNLBP. 3 Trunk neuromuscular adaptations influence the body's capacity to perform stable movements across various tasks, resulting in compensatory strategies and modified postural control. 4
The framework of nonlinear dynamics emphasizes the importance of the regularity or irregularity of temporal movements for functional network dynamics. 5 For example, to assess the dynamics of a biological system, the degree of uncertainty can be investigated by sample entropy (SampEn). 6 The amount of information required to describe the biological process correlates with this measure of complexity. 6
Different entropy calculations have demonstrated how constraints in the motor control network (e.g., CNLBP) impact motor coordination, offer explanations for the regularity of movement patterns, and have been used as a relevant index of complexity, 7 which traditional linear metrics fail to detect.8,9 Methodological advances, such as multiscale entropy (MSE), have become essential for quantifying the regularity of time series across different health conditions.
For example, increased regularity (lower entropy) in trunk kinematics has been observed in individuals with CNLBP, suggesting reduced motor control adaptability. Although interest in nonlinear dynamics has grown in recent decades, the specific relationship between chronic spinal pain states and entropy-based motor assessments remains conceptually and methodologically underexplored. Furthermore, the lack of methodological uniformity limits the ability to compare findings across studies and restricts the development of standardized clinical applications for entropy-based assessments in CNLBP.
The aim of this review is to examine the capability of entropy metrics to identify consistent group differences in trunk movement regularity between individuals with CNLBP and healthy controls. We hypothesize that CNLBP correlates with reduced entropy values, indicating more rigid and less adaptable motor behavior.
Materials and methods
Protocol and registration
This study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines. 10 Additionally, it was registered with the International Prospective Register of Systematic Reviews (PROSPERO) under registration number CRD42020187731. 11 A completed PRISMA 2020 checklist is provided as supplementary material.
Eligibility criteria
Observational and analytical cross-sectional studies that compare trunk kinematic regularity between individuals with CNLBP and healthy controls were included. We excluded systematic reviews, case reports, case series, and interventional studies. Only observational cross-sectional designs with group comparisons were included. Studies without a healthy control group were also excluded.
We included studies of adult participants (≥18 years), both with and without CNLBP lasting over 12 weeks. Eligible studies had to evaluate trunk kinematic variables using entropy-based techniques, with data collected during, before, or after performing motor tasks (e.g., sitting posture, gait, trunk flexion/extension). The included studies could apply any type of entropy measure of trunk movement regularity, such as sample entropy, to measure how predictable or irregular movement patterns are by analyzing repeated sequences in the data. A higher SampEn value indicates greater irregularity or complexity, suggesting that the time series is less predictable or more disordered. Conversely, a lower SampEn value suggests more regularity or predictability in the data. In simple terms, higher values mean more varied and unpredictable movements, while lower values indicate more repetitive and rigid movement patterns. The MSE examines movement complexity across different time scales, from quick adjustments to longer movement strategies. This method aims to quantify the predictability of patterns: a time series containing many repetitive patterns (i.e., one that is more predictable) would have relatively lower MSE, while a less predictable process would exhibit higher MSE and lower regularity. Recurrence Quantification Analysis (RQA) is a nonlinear method used to characterize the temporal structure of repeated movement patterns. Within the RQA framework, entropy quantifies the complexity of deterministic structures by assessing the distribution of recurrent patterns over time. Higher entropy values indicate more complex and heterogeneous recurrence structures, reflecting greater variability in movement organization, whereas lower entropy values indicate more regular and predictable patterns.
Sources and search strategy
A comprehensive electronic search was performed across various databases
Selection process
The files extracted from each database were imported into the Rayyan Systematic Review Platform (https://www.rayyan.ai/). The first step is removal of duplicate records. Subsequently, two independent blinded reviewers screened the titles and abstracts. The same reviewers assessed the full texts of potentially eligible studies when necessary. No disagreements occurred during the selection process, and therefore, adjudication by the third assessor was not necessary. The entire selection process was conducted between September and November 2024.
Data extraction and summary
Data extraction was conducted independently by two reviewers using Google Forms (electronic form). 13 The process was structured into multiple phases: 1) Study identification and characteristics, 2) Participant information, 3) Motor tasks and kinematic data, 4) Entropy technical parameters, and 5) Risk of bias assessment. The included studies were summarized based on key methodological variables and results. Data synthesis focused on 1) entropy-based movement regularity, 2) task-specific differences, 3) methodological consistency, and 4) influence of the risk of bias. The structure of the extracted data is available as supplementary material in Cochrane-compliant format, including the original table headers and details on the extraction protocol.
Critical appraisal tool for analytical cross-sectional studies
The methodological quality of the included research was evaluated utilizing the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Analytical Cross-Sectional Research. This method was chosen for its relevance to observational study designs and its thorough assessment of both internal and external validity. Specifically, it offers a systematic methodology appropriate for diverse samples, commonly encountered in clinical biomechanics.
Despite the existence of alternative instruments, such as the one evaluated by Ma et al. (2020), 14 the JBI checklist was considered more aligned with the study designs included in this review and has been widely used in systematic reviews within rehabilitation sciences. 15 Two independent reviewers applied the JBI critical appraisal tool, and discordances in the final analysis were resolved by consensus.
The checklist consists of eight key criteria, each addressing a potential source of bias: 1)Definition of inclusion criteria: determines whether the study specifies well-defined inclusion and exclusion criteria before participant recruitment. 2) Detailed description of study subjects and setting: ensures that the study provides sufficient details about the population, setting, and timeframe, allowing comparability with other studies; 3) valid and reliable exposure measurement, which evaluates whether the method used to measure exposure is appropriate, standardized, and comparable to a gold standard; 4) Use of objective and standardized criteria for condition measurement assesses whether the study employs established diagnostic criteria or validated definitions to classify participants; 5) Identification of confounding factors determines whether the study recognizes potential confounders that could influence the observed relationships; 6) Strategies to address confounding factors, examining whether the study implements matching, stratification, or multivariate analysis strategies to minimize confounding effects; 7) Valid and reliable outcome measurement, which ensures that outcome variables are measured using validated instruments or standardized assessment methods; and 8) Appropriate statistical analysis, which assesses whether the statistical methods used are suitable for the study design and correctly account for confounders. Each criterion is assessed as yes, no, unclear, or not applicable.
Rating the certainty of evidence with grading of recommendation, assessment, development and evaluation (GRADE)
We evaluated the certainty of evidence utilizing the Grading of Recommendations Assessment, Development and Evaluation (GRADE) tool for cross-sectional observational studies.16–18 Two reviewers did the GRADE assessment on their own, and any differences were talked about until everyone agreed on the same thing.
According to GRADE guidelines, cross-sectional observational studies were initially assigned a low certainty rating by default, with the possibility of subsequent downgrading or upgrading based on these criteria. Five domains were assessed: risk of bias, inconsistency, imprecision, indirectness, and publication bias. For each outcome across studies, the overall certainty of the evidence was rated as high, moderate, low, or very low.
A high level of certainty means that you can be very sure of the estimated effect, and more research is unlikely to change this estimate. Moderate certainty indicates that the existing evidence corroborates the conclusion, yet further studies may alter the confidence in the estimate. Low certainty means that the real effect could be very different from what was found because of problems with the methods or inconsistencies. Very low certainty means that there is not enough evidence to make reliable conclusions.
For outcomes derived from a singular cross-sectional study, we adhered to GRADE guidelines, recognizing that inconsistency remains assessable. In these instances, the initial certainty level was low due to the observational design, and it was typically reduced by one level because of unexplained inconsistency (which cannot be evaluated with a single study); this was followed by a reevaluation for imprecision related to sample size and variability of estimates. A single study could not formally evaluate publication bias. As a result, the results of a single study were usually rated as having very low certainty unless there were clear criteria for upgrading.
Results
Results of study searches and characteristics
Figure 1 presents a flow diagram summarizing the study selection process. Table 1 presents the included studies, study designs, and publication indicators. Table 2 shows the characteristics of the participants, motor tasks, trunk kinematics, and data collection measurements. Five cross-sectional studies met the inclusion criteria of,19–23 comprising 222 participants with and without CNLBP. The studies were published from 2017 24 to 2024. 25 Geographically, the studies were conducted across five countries (Japan, Iran, Portugal, Switzerland, and Finland) spanning two continents (Asia and Europe).

PRISMA flow diagram for the search and selection process. Abbreviation: PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Studies included in the present review and publication indicators.
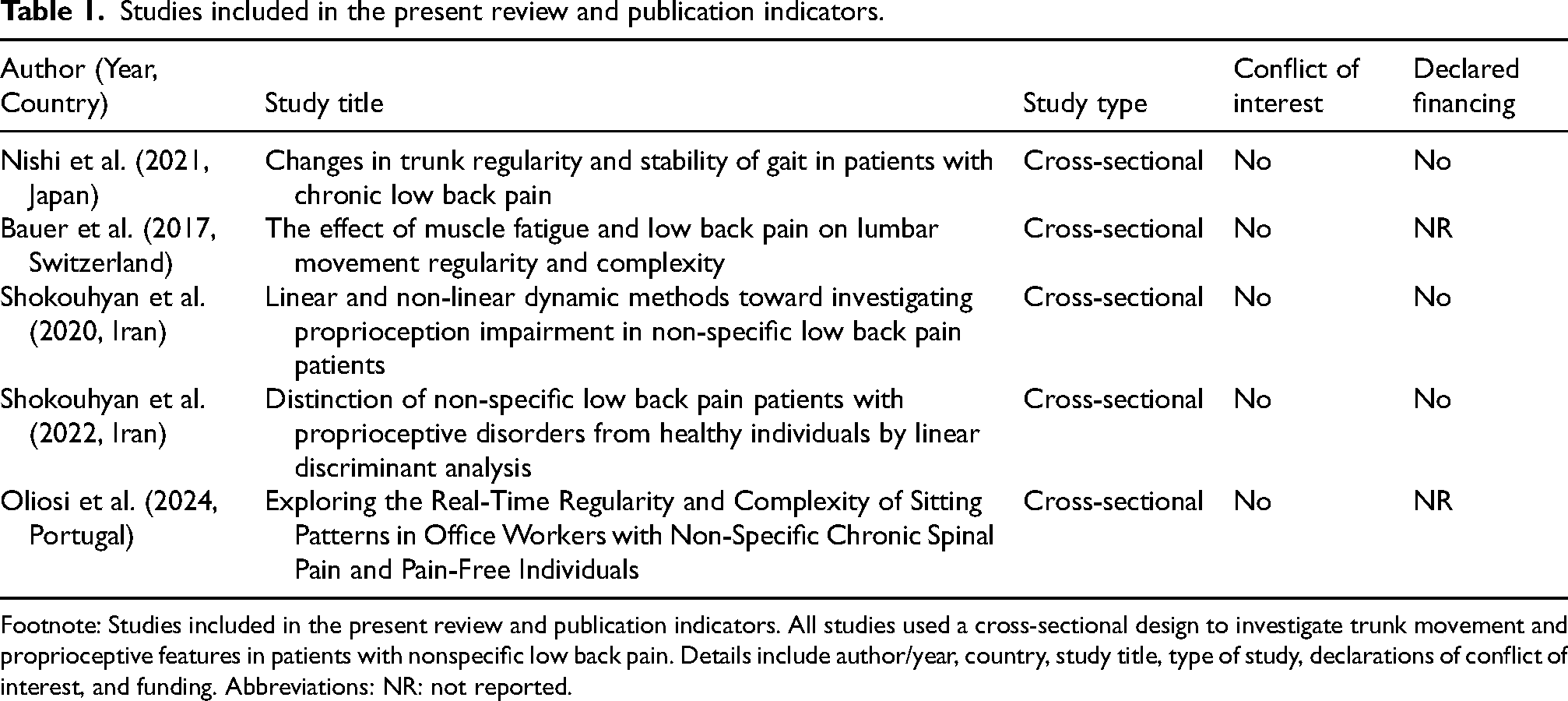
Footnote: Studies included in the present review and publication indicators. All studies used a cross-sectional design to investigate trunk movement and proprioceptive features in patients with nonspecific low back pain. Details include author/year, country, study title, type of study, declarations of conflict of interest, and funding. Abbreviations: NR: not reported.
Participant characteristics, outcome categories, motor tasks, and kinematic data collection across the included studies.
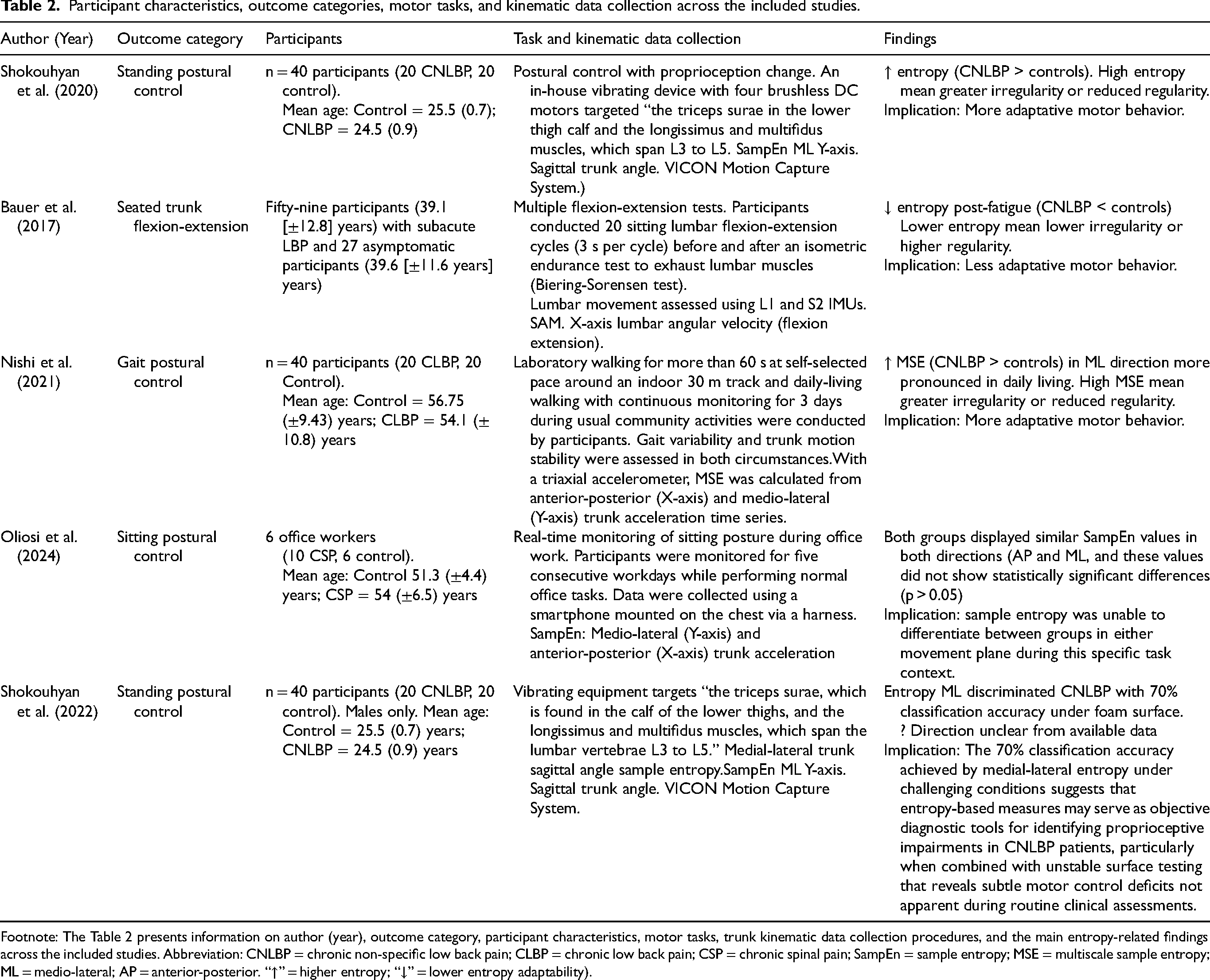
Footnote: The Table 2 presents information on author (year), outcome category, participant characteristics, motor tasks, trunk kinematic data collection procedures, and the main entropy-related findings across the included studies. Abbreviation: CNLBP = chronic non-specific low back pain; CLBP = chronic low back pain; CSP = chronic spinal pain; SampEn = sample entropy; MSE = multiscale sample entropy; ML = medio-lateral; AP = anterior-posterior. “↑” = higher entropy; “↓” = lower entropy adaptability).
Comparative summary of entropy analysis methods and findings across included studies.
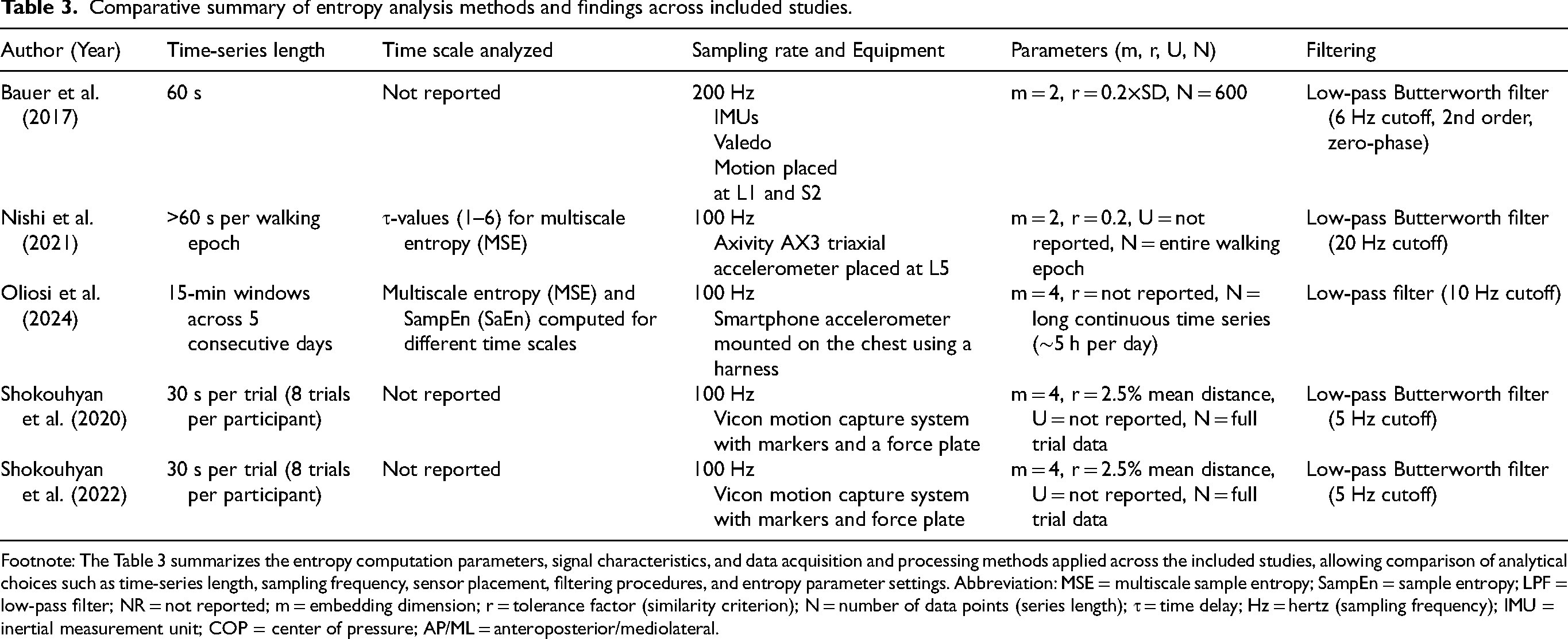
Footnote: The Table 3 summarizes the entropy computation parameters, signal characteristics, and data acquisition and processing methods applied across the included studies, allowing comparison of analytical choices such as time-series length, sampling frequency, sensor placement, filtering procedures, and entropy parameter settings. Abbreviation: MSE = multiscale sample entropy; SampEn = sample entropy; LPF = low-pass filter; NR = not reported; m = embedding dimension; r = tolerance factor (similarity criterion); N = number of data points (series length); τ = time delay; Hz = hertz (sampling frequency); IMU = inertial measurement unit; COP = center of pressure; AP/ML = anteroposterior/mediolateral.
Methodological quality assessment of included studies based on the JBI critical appraisal checklist.
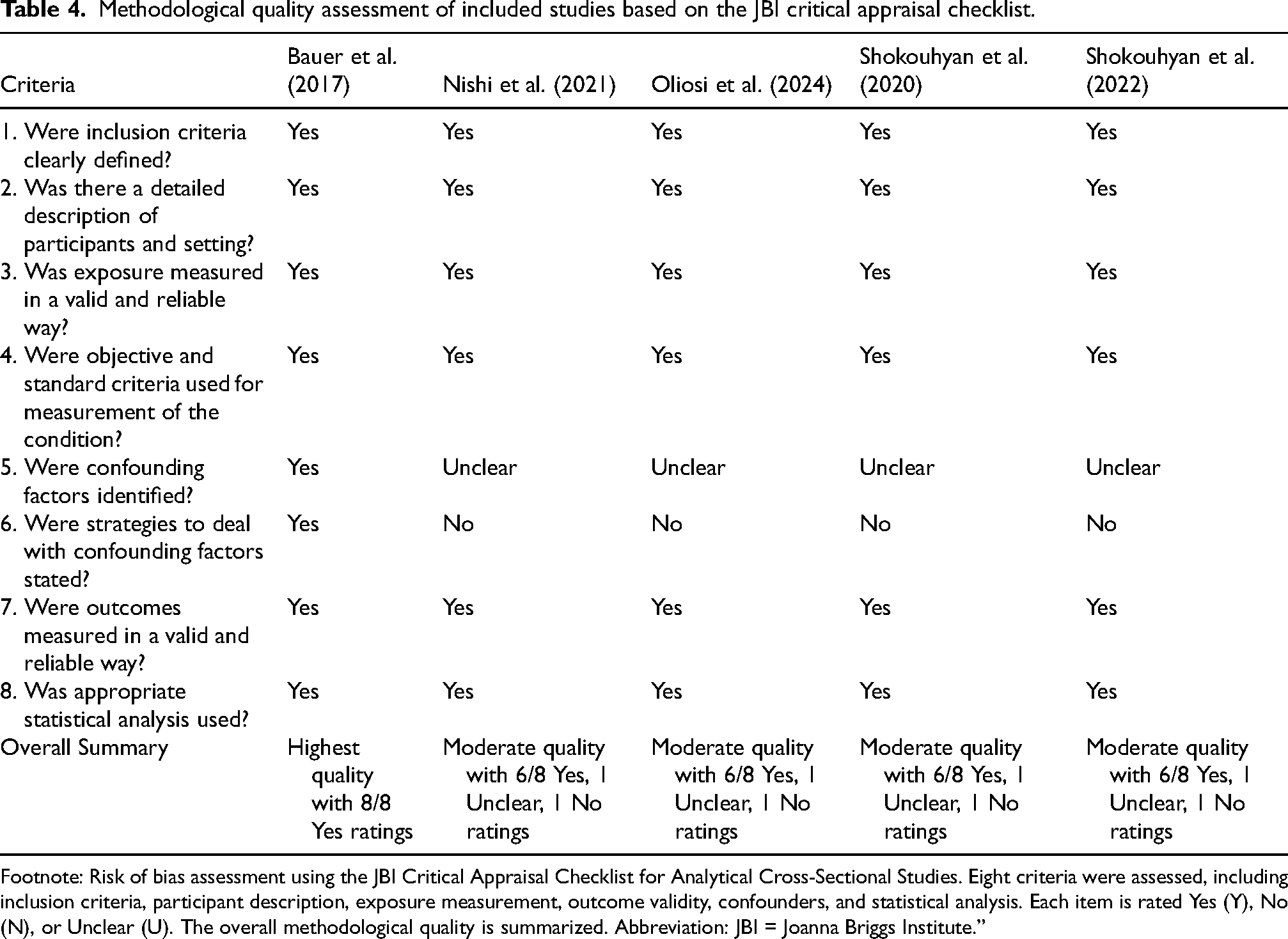
Footnote: Risk of bias assessment using the JBI Critical Appraisal Checklist for Analytical Cross-Sectional Studies. Eight criteria were assessed, including inclusion criteria, participant description, exposure measurement, outcome validity, confounders, and statistical analysis. Each item is rated Yes (Y), No (N), or Unclear (U). The overall methodological quality is summarized. Abbreviation: JBI = Joanna Briggs Institute.”
Summary of the certainty of evidence across outcomes according to the GRADE framework.
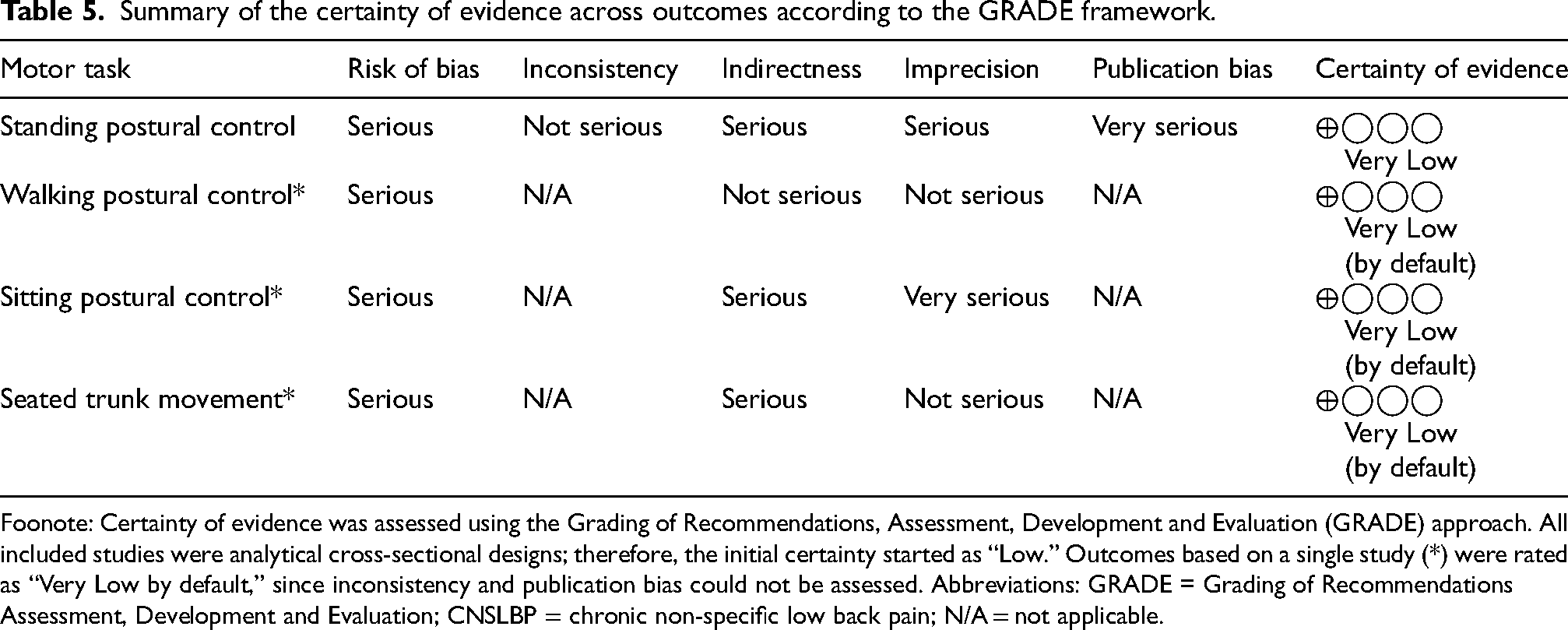
Foonote: Certainty of evidence was assessed using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach. All included studies were analytical cross-sectional designs; therefore, the initial certainty started as “Low.” Outcomes based on a single study (*) were rated as “Very Low by default,” since inconsistency and publication bias could not be assessed. Abbreviations: GRADE = Grading of Recommendations Assessment, Development and Evaluation; CNSLBP = chronic non-specific low back pain; N/A = not applicable.
Qualitative findings
Regarding participant characteristics, all studies included both CNLBP individuals and healthy control groups, ensuring appropriate group comparisons. The study sample sizes vary from 16 25 to 86 24 individuals. The mean age of participants, unifying the values of CNLBP and health controls per study, ranged from 24.522,23 to 56.75 26 years. Shokouhyan et al. (2020, 2022)22,23 assessed 40 male participants (20 CNLBP, 20 controls), with a mean age of 25.5 years in the control and 24.5 years in CNLBP individuals. Bauer et al. 2017 24 included 86 participants (59 CNLBP, 27 controls), with a mean age of 39.1 years in the control and 39.6 years in CNLBP individuals. Oliosi et al. (2024) 25 studied 16 office workers (10 with CNLBP, 6 controls), with mean ages of 50 years (controls) and 54.3 years (CNLBP group), 80% of whom were female. Nishi et al. 2021 26 included 40 participants (20 CNLBP, 20 controls), with mean ages of 55 years (controls) and 56.75 years (CNLBP group), with 40–45% female representation. Of the 222 participants in the pooled dataset, 42% were healthy controls and 58% had chronic or non-specific low back pain. With a range of 24.5 to 56.75 years, the weighted mean age across studies was roughly 43 years.
Considering the motor tasks and kinematic data collection, the included studies were categorized into four categories for interpretative synthesis. In the standing postural control outcome, Shokouhyan et al. (2022) 23 demonstrated that the linear discriminant analysis indicated that medio-lateral entropy was the optimal parameter for differentiating between the NSLBP and healthy groups, achieving classification percentages of 100% and 70%, respectively, while the foam surface combined with vibration provided the most favorable sensory condition. However, it does not say which group had higher entropy values; it only says that medio-lateral entropy was one of the best ways to tell the groups apart, with a 70% classification rate. However, Shokouhyan et al. (2020) 22 demonstrated that the entropy values were higher for the CNLBP group as compared to the healthy group across most of the trials (4.69 > 3.9), indicating decreased regularity under proprioceptive perturbations (more able to adapt to the environmental conditions).
Analyzing the walking postural control outcome, Nishi et al. (2021) 26 demonstrated that for MSE at τ ≥ 2 for medio-lateral, the CNLBP group had a higher MSE in daily life than in the laboratory settings. The health group did not have this pattern. Moreover, MSE at τ ≥ 4 in CNLBP patients was significantly higher compared to controls in the laboratory setting, and MSE at τ ≥ 2 in the CNLBP group was significantly higher than that of controls in the daily living context.
For the sitting postural control, 25 when compared to participants without pain, results show that those with CNLPB exhibited lower complexity and predictable trunk movements with increased regularity, even though the study did not find any significant differences in SampEn specifically.
Finally, the seated trunk movement outcome 24 showed that both groups displayed similar SampEn values in both directions with no statistically significant differences (p > 0.05), though CNLBP participants showed more complex and more predictable trunk movements compared to participants with pain-free CNLBP.
Motor tasks and kinematic data collection
Recent studies (2021–2024) have focused on ecological and task-specific motor assessments, such as trunk motion during office work 21 and walking in daily environments. 26 Olliosi et al. (2024), 25 using a smartphone-based method, recorded rotation vector, accelerometer, gyroscope, and magnetometer data. The device was harness-mounted on the chest and had sampling rates of 50 Hz for the magnetometer and 100 Hz for the majority of the sensors. For thorough multimodal data collection, additional electromyography (EMG) sensors and a smartwatch were employed. In the study of Nishi et al. (2021), 26 the L5 vertebra was equipped with a single tri-axial accelerometer that sampled at 100 Hz with a ± 8 g range. For three days, the device was worn constantly while going about daily tasks; it was only taken off to take a shower or go to sleep. Walking on a 30-meter indoor track for more than 60 s was part of the laboratory test.
Prior research (2017–2022) predominantly focused on laboratory-based tasks, including standing balance control under proprioceptive perturbation induced by vibrational stimuli and seated trunk flexion–extension movements. 24 Shokouhyan et al. (2020, 2022),22,23 with similar experimental setups used in both studies, employed force plates synchronized with a motion capture system at a sampling frequency of 100 Hz. Anatomical landmarks such as the C7, T12, lower sternum, clavicle, scapula, and bilateral PSIS and ASIS locations were marked with reflective markers. Both studies created specialized vibrating apparatus with four brushless DC motors, operating at a frequency of 70 Hz and an amplitude of roughly 0.5 mm, to modify proprioception at the soleus and lumbar muscles (longissimus and multifidus spanning L3-L5 vertebrae). The study of Bauer et al. (2017) 24 used an inertial measurement unit (IMU) system (recorded at 200 Hz and positioned at the first lumbar and second sacral vertebrae) that was all included in the tri-axial sensors. An 80 bpm metronome was used to guide the participants to controlled trunk flexion-extension movements while they were fastened with thigh belts.
Entropy-based metrics in the included studies
The methodological diversity observed in the computation of entropy-based metrics among the included studies reveals important differences in analytical design, data acquisition, and signal processing parameters.
The durations of time series varied significantly across studies, from brief 30-s trials per condition22,23 to 60-s recordings 24 and extended 15-min intervals collected over five consecutive workdays. 25 The sampling frequencies varied, ranging from 100 Hz in Shokouhyan et al. (2020; 2022)22,23 and Nishi et al. (2021) 26 to 200 Hz in Bauer et al. (2017), 24 which could have caused effects on entropy estimation that depend on resolution. Instrumentation and sensor placement differed among studies: Bauer et al. (2017) 24 situated inertial sensors between the second sacral and first lumbar vertebrae, Nishi et al. (2021) 22 affixed a tri-axial accelerometer at L5, and Oliosi et al. (2024) 25 positioned a smartphone-mounted IMU on the chest. This variability in anatomy and devices probably had an effect on the signal properties and the corresponding entropy values. The parameter settings differed. Bauer et al. (2017) 24 employed m = 2 and r = 0.2 × SD; the Shokouhyan studies22,23 utilized m = 4 and r = 2.5% of mean distance; and Oliosi et al. (2024) 25 applied m = 4. The use of low-pass Butterworth filters at 5 Hz (Shokouhyanet al., 2020; 2022),22,23 6 Hz (Bauer et al., 2017), 10 Hz 25 and 20 Hz 22 added to the heterogeneity. A detailed summary of entropy computation parameters, signal characteristics, and analytical variability across studies is presented in Table 3.”
Critical appraisal checklist for analytical cross-sectional studies
The JBI critical appraisal checklist assessment identified one high-quality study and four moderate-quality studies among the five analytical cross-sectional investigations. Bauer et al. (2017) 24 fully followed all eight JBI criteria, while Shokouhyan et al. (2022), 23 Nishi et al. (2021), 26 Oliosi et al. (2024), 25 and Shokouhyan et al. (2020) 22 each only met six criteria, with the same patterns of limitations.
The identification and management of confounding factors emerged as the principal weakness, with four studies inadequately addressing these criteria. Bauer et al. were the only ones who clearly named confounders when they said, “anthropometric factors such as age, gender, or body mass index (BMI), which can influence lumbar kinematics and the development of CNLBP, were controlled for in the study design,” and they used control strategies “for the effect of age, gender, and BMI.” This systematic limitation present in 80% of studies may undermine the validity of findings related to the relationships between movement variability and CNLBP, thereby constraining causal inference and generalizability across varied populations. The results of the methodological quality assessment using the JBI critical appraisal checklist are summarized in Table 4.
Assessment of certainty of evidence and reporting bias
The overall certainty of evidence across all four outcomes was assessed as low to very low. The evidence certainty for the standing postural control outcome22,23 was downgraded due to potential publication bias, given that both studies were conducted by the same research group, despite the results being internally consistent. The walking postural control outcome 26 exhibited a low risk of imprecision, bolstered by a sufficient sample size and clear analytical reporting. However, the overall level of certainty was deemed low because of the observational design. The seated trunk movement outcome 24 exhibited significant methodological rigor, characterized by comprehensive reporting, effective control of confounding variables, and accurate estimates, resulting in a moderate level of confidence within the observational evidence spectrum. The ecological sitting task 25 exhibited the lowest confidence, largely attributable to a limited sample size and unaccounted confounders. The primary factors limiting certainty across all outcomes were the risk of bias and publication overlap. Nonetheless, no significant issues were observed concerning consistency, as all studies aligned with similar directional effects, indicating greater entropy or variability in CNLBP participants relative to healthy controls under task-specific conditions. The certainty of evidence for each outcome, assessed using the GRADE approach, is summarized in Table 5.
Discussion
Findings from the five analytical cross-sectional studies highlight task-specific variations in movement regularity in CNLBP patients, reflecting a nuanced pattern that contradicts established beliefs about motor control adaptations. The present study suggests that individuals with CNLBP have elevated entropy values (indicating decreased regularity) in demanding postural contexts.
The present differing results align with contemporary motor control theories, suggesting that chronic pain conditions may lead to context-dependent adaptations. Decreased regularity in challenging balance tasks may signify compensatory strategies for increased movement adaptability, whereas reduced regularity in seated tasks may indicate protective stiffening behaviors or a maladaptive functional capacity. The evidence indicates that movement regularity in CNLBP is not consistently elevated or diminished; instead, it reflects a complex reorganization of motor control strategies that fluctuates based on task requirements, environmental limitations, and specific sensorimotor challenges encountered.
According to the mentioned contemporary motor control theories of motor control, in healthy biological systems, lower regularity (higher entropy) represents a structured and adaptable pattern, rather than random noise. When this structured regularity reduces, biomechanical patterns show decreased adaptability for motor tasks. Adaptability in healthy systems is maintained through the dynamic interactions among multiple subsystems, whereas aging and health conditions limit the system's capacity to respond to constraints and perturbations. Specific theoretical models demonstrate that musculoskeletal pain is associated with increased movement regularity (reduced entropy). According to the framework proposed by Stergiou et al. (2011), 27 this reduction in entropy is consistent with the loss of complexity hypothesis, which posits that decreased complexity leads to less efficient movement patterns. In this context, reduced entropy signifies a more rigid, less adaptive, and more predictable motor behavior. While optimal movement patterns require a balance of structured regularity and adaptability, chronic pain disrupts this balance. Hodges et al. (2011) 28 further support this view with the motor adaptation to pain model, suggesting that pain induces changes in motor behavior and reorganization to protect affected tissues, resulting in increased movement regularity and altered biomechanical patterns over time. Taken together, these theoretical frameworks support the findings of the present review. In CNLBP, decreased trunk movement entropy reflects higher movement regularity, potentially contributing to maladaptive adjustments due to diminished adaptability. Collectively, these results demonstrate that the influence of pain on movement complexity varies according to the specific motor task, highlighting the complex and multifactorial mechanisms underlying motor adaptations in CNSLBP.
For example, the context of the task affects entropy estimation because the level of environmental constraint affects how variable and adaptable movement patterns are. Laboratory studies usually have controlled conditions that limit motor variability, while ecological assessments show how movement changes and adapts in real life. Understanding this methodological difference is crucial for interpreting entropy results from various studies and enhancing the ecological validity of future research designs.
Entropy measures, such as SampEn (SampEn) and SampEn (MSE), are increasingly recognized as valuable tools in motor control research. Tang et al. (2025) 29 highlighted entropy as a critical parameter for quantifying movement adaptability through nonlinear time-series analyses. Further advancing the field, Yin et al. (2015) 30 introduced Multiscale Joint Permutation Entropy to assess temporal synchronization in movement patterns, thereby sheddings ligths on coordination impairments in individuals with CNLBP. However, significant methodological heterogeneity persists across studies employing entropy-based analyses, particularly regarding the selection of computation parameters such as embedding dimension (m), tolerance (r), number of scales, and sampling frequency. These variations critically affect entropy outcomes and hinder comparability across investigations. Recent evidence confirms that even minor differences in parameter settings or sampling rates can produce divergent entropy values, thus limiting reproducibility and clinical translation.31,32 Accordingly, the development and adoption of standardized protocols for data acquisition and entropy computation, along with transparent reporting of analytical parameters, are essential to enhance comparability and facilitate the clinical interpretation of entropy-based metrics in musculoskeletal research.
The key findings with potential clinical implications indicate that the task-dependent entropy alterations in CNLBP patients reveal clinically significant motor control adaptations that challenge traditional rehabilitation approaches. Higher entropy during challenging postural tasks suggests compensatory strategies where patients decrease movement regularity to maintain stability when proprioceptive systems are compromised, while reduced entropy during controlled tasks indicates protective stiffening behaviors that may limit functional recovery. These findings support individualized treatment approaches that consider task context, as interventions targeting movement variability should account for whether the goal is to enhance compensatory adaptability during challenging conditions or restore normal movement patterns during routine activities. The diagnostic potential of entropy measures, particularly the 70% classification accuracy achieved under challenging conditions, suggests clinical utility for objective assessment of proprioceptive impairments in CNLBP populations.
The evaluation using the JBI Critical Appraisal Checklist for Analytical Cross-Sectional Research indicated that 80% of studies inadequately identified and controlled confounding factors, which poses a significant limitation on the interpretation of movement variability findings in CNLBP. Bauer et al. (2017) 24 explicitly addressed confounders by stating, “Anthropometric factors such as age, gender, or body mass index (BMI), which can influence lumbar kinematics and the development of LBP, were controlled for in the study design,” and by implementing appropriate control strategies. The systematic weakness restricts the ability to draw causal inferences and may account for the contradictory findings observed in various postural tasks, as unmeasured variables like physical activity levels, occupational demands, and psychological factors could significantly affect movement patterns. The lack of confounder control limits the generalizability of findings across various populations and clinical contexts, which may hinder the application of these results in evidence-based clinical practice for managing chronic spinal pain. Significant deficiencies in sex representation and analysis compound the methodological limitations. Shokouhyan et al. (2022) 23 and Shokouhyan et al. (2020) 22 exclusively recruited male participants, stating that this choice was made for logistical reasons; therefore, investigating female participants and examining gender differences should be an important future direction. Bauer et al. (2017) 24 acknowledged sex as a confounding variable and controlled for the effect of age, gender, and BMI. In this line, the predominant exclusion of female participants and the absence of analysis concerning sex differences in most studies further restrict generalizability. Sex-based differences in motor control strategies may substantially influence the observed entropy and variability metrics, consequently limiting the clinical relevance of these findings to various CNLBP patient populations.
The certainty of evidence, assessed using the GRADE framework, was classified as low to very low across most outcomes. This primarily reflects the predominance of cross-sectional study designs, small sample sizes, and methodological variability in entropy computation parameters. Although these limitations do not invalidate the observed findings, they indicate that the true effect of movement regularity in CNLBP may differ from current estimates. This uncertainty restricts the prompt clinical application of entropy-based metrics, as variable analytical methodologies and insufficient sample sizes diminish confidence in their diagnostic and prognostic significance. To strengthen the evidence base, future research should prioritize larger and more diverse samples, multicenter collaborations to enhance reproducibility, and the establishment of standardized protocols for data acquisition and entropy computation. These advancements are essential for transforming entropy measures from promising research tools into reliable clinical indicators of motor adaptability and neuromuscular health.
This review has some limitations that must be acknowledged. The number of included studies was small, and methodological heterogeneity, particularly in task design, entropy parameters, and the number of studies per outcome reporting, precluded a formal meta-analysis. Additionally, the methodological heterogeneity and entropy values from various studies were examined qualitatively instead of being aggregated quantitatively to maintain consistency in comparison. Furthermore, the certainty of the evidence, as evaluated using the GRADE approach, ranged from low to very low across motor task categories. Such variation limits the strength of the inferences and highlights the need for future studies with standardized protocols and higher methodological rigor. The heterogeneity in study designs, entropy computation methods, and motor tasks was assessed in limited direct comparisons across studies. This review focused on identifying general trends rather than directly comparing absolute entropy values across studies to mitigate this limitation. Additionally, not all studies explicitly controlled potential confounding factors, such as pain intensity, physical activity level, previous treatments, and comorbidities. Since these factors can influence movement regularity, their lack of consideration may introduce variability in the reported findings. This limitation needs to be considered when interpreting the results. While CNLBP appears to play a central role in motor control alterations, uncontrolled variables such as activity level and comorbidities may also influence movement regularity patterns. Moreover, the recurrent exclusion of female participants or the lack of sex-specific analyses in the majority of studies limits the generalizability of findings across various populations.
From a scientific standpoint, nonlinear metrics are gaining recognition in movement research, particularly for assessing movement adaptability and motor control dysfunctions. While the findings of the current review reinforce the utility of entropy metrics in characterizing motor control in individuals with CNLBP, their clinical application still presents challenges. The absence of reference values and cutoff points to distinguish between healthy individuals and those with CNLBP hinders translation of these results into clinical practice. Future studies should explore the development of standardized guidelines for the clinical use of entropy as an objective biomarker of motor dysfunction, including consensus protocols for embedding dimensions (as studies varied from an embedded dimension of 4 to unspecified parameters), standardized time scale ranges for multiscale approaches, consistent sampling frequencies, and task-specific parameter optimization to ensure reproducibility across clinical settings. Reporting standards should require the disclosure of all computational parameters, including tolerance values, pattern lengths, time delays, and data preprocessing protocols such as filtering cutoff frequencies and minimum recording durations, to facilitate cross-study comparisons and clinical implementation.
This review demonstrates that movement regularity in CNLBP is task-dependent. During difficult postural and gait tasks, there were higher entropy values, but during controlled flexion-extension tasks, patients had lower entropy values than healthy controls. These findings underscore the relevance of entropy-based metrics for identifying motor control deficits and reinforce the importance of task-specific evaluation strategies in clinical settings. Importantly, such methods are compatible with kinematic data obtained from motion capture systems and could be feasibly extended to wearable technologies such as inertial measurement units, enhancing ecological validity and supporting future clinical integration of entropy measures beyond laboratory settings.
Although entropy-based measures demonstrate potential for assessing motor control in CNLBP, subsequent research should investigate their longitudinal stability, responsiveness to treatment effects, and correlation with patient-reported outcomes. Examining entropy alongside other neuromechanical markers may enhance our theoretical comprehension of movement adaptation and its impairment in CNLBP populations.
Conclusion
This review demonstrates that movement regularity in CNLBP is task-dependent, with higher entropy during challenging postural and gait tasks and reduced entropy during controlled flexion-extension tasks. These findings underscore the relevance of entropy-based metrics for identifying motor control deficits and support task-specific evaluation strategies in clinical settings. Entropy metrics may help find people with CNLBP who have less motor adaptability, which would make it easier to plan targeted treatments and group patients based on their neuromuscular control patterns. Future research should employ longitudinal designs to evaluate the prognostic value of entropy measurements and explore multimodal approaches combining entropy analysis with complementary technologies to enhance real-time assessment of motor control in naturalistic contexts.
Supplemental Material
sj-docx-1-bmr-10.1177_10538127251410296 - Supplemental material for Entropy metrics for analyzing trunk movement regularity in chronic non-specific low back pain: Insights from a systematic review
Supplemental material, sj-docx-1-bmr-10.1177_10538127251410296 for Entropy metrics for analyzing trunk movement regularity in chronic non-specific low back pain: Insights from a systematic review by Wagner Martins, Mariana Marcozze, Sergio Fonseca, Fabricio Magalhães, Elaine Cristina Leite Pereira, Mariana Aquino and Thales Souza in Journal of Back and Musculoskeletal Rehabilitation
Footnotes
ORCID iDs
Ethical approval
Not applicable. This study is a systematic review and did not involve research with human participants.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Author contributions
All authors contributed to the study conception, design, data extraction, analysis, and manuscript writing. All authors read and approved the final version.
Funding
This research resulted from the first author's postdoctoral project (Wagner Martins) and was funded by the Brazilian National Council for Scientific and Technological Development (CNPq).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
All data supporting this study's findings are publicly available in the included sources. Supplementary materials generated during this review are available upon request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.