
Abstract
The purpose of this review was to analyze fidelity features in parent-implemented interventions for young children with disabilities. The authors conducted a review of 24 studies published in nine peer-reviewed journals. Each identified article was scored on the following categories: the participant characteristics, settings, study design, independent variables, measurement of implementation and intervention fidelity, parent training components, dependent variables, social validity, overall outcomes, and study rigor. The results indicated that, although all studies described parent training components, few reported implementation fidelity. Across the studies trainers were most likely to use performance-based feedback and modeling to support parent implementation of the intervention. Although 20 studies used single-case design methodologies, only 2 studies met contemporary single-case research design standards. The authors provide an analysis of implications for future research related to supporting high-fidelity implementation of parent-implemented interventions.
The burgeoning field of implementation science is changing how we address the gap between science and practice and highlights the imperative role of fidelity. Implementation science is the scientific study of variables and conditions that impact the effectiveness and sustainability of evidence-based programs and practices (Fixsen, Blase, Duda, Naoom, & Van Dyke, 2010). Specifically, implementation science examines how interventions can be integrated into diverse practice settings with high fidelity and is concerned with two aspects of fidelity. First, implementation fidelity refers to the practices (i.e., training and coaching) used to support the implementation of the intervention. Second, intervention fidelity refers to the actual implementation of the intervention (i.e., use of newly learned strategies). Although these terms are often used interchangeably, clear distinctions between the two are necessary to identify, sustain, and scale-up evidence-based practices. For example, in the research on parent-implemented interventions, implementation practices lead to parent use of the intervention, and effective use of the intervention leads to positive child outcomes (see Figure 1). Fixsen and his colleagues argue that components of and variables affecting high-fidelity implementation are as important as the components of variables affecting the effectiveness of an intervention (Fixsen, Naoom, Blasé, Friedman, & Wallace, 2005). According to implementation science, high-fidelity implementation of effective training practices (implementation fidelity) yields high-fidelity implementation of evidence-based practices (intervention fidelity), which results in positive child outcomes. In fact, research has shown that low-fidelity implementation often yields ineffective outcomes (Strain & Bovey, 2011; Vernez, Karam, Mariano, & DeMartini, 2006). Thus, an analysis of the research on the effectiveness of parent-implemented interventions should include an analysis of child outcomes, parent-intervention fidelity, and the practices used to support parent high-fidelity implementation.
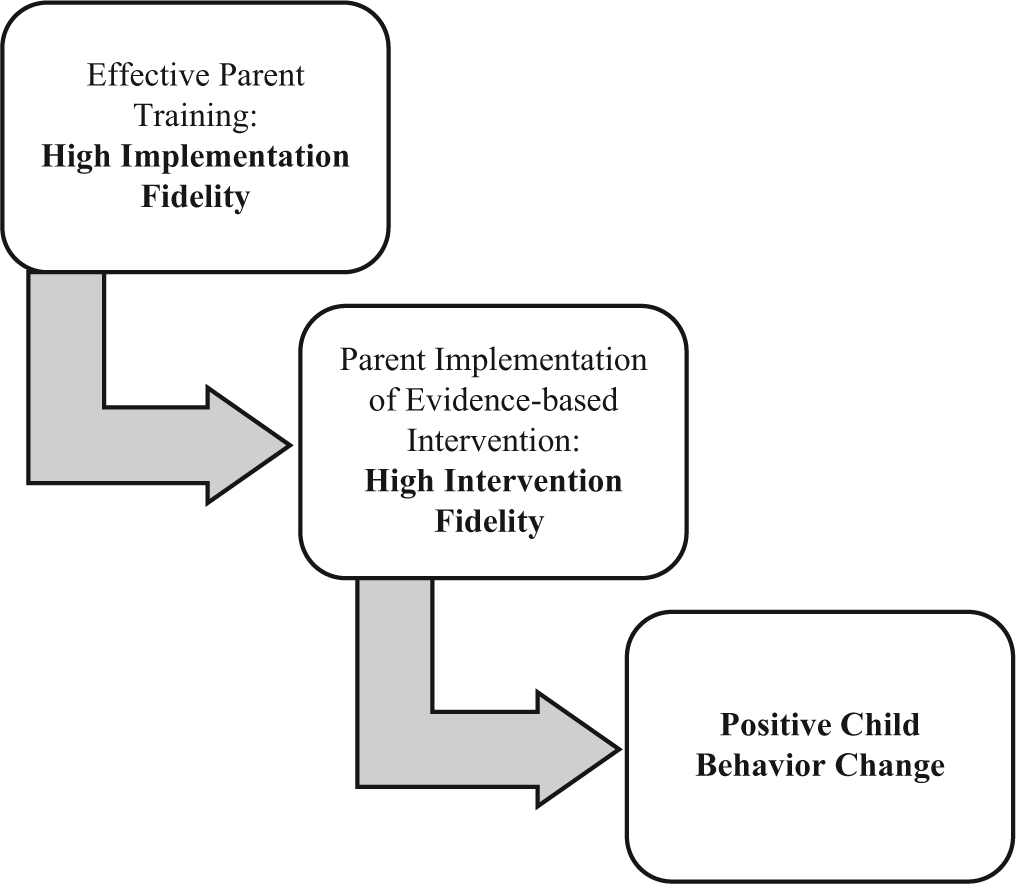
Relation Between Implementation Fidelity, Intervention Fidelity, and Child Outcomes for Parent-Implemented Interventions
Parent-implemented interventions are an essential component of quality early intervention/early childhood special education (EI/ECSE) programs for young children (National Research Council, 2001). Parent-implemented interventions are designed to enhance parents’ capacity to promote their children’s development and learning. The influence of parents on their child’s development is critical; parents are the most important facilitators of learning for their young children (Dunst, Trivette, & Hamby, 2008; Powell & Dunlap, 2010). Children develop within the context of their family; thus, teaching parents effective strategies to support their children’s development is both practical and essential. The effectiveness of parent-implemented interventions has been demonstrated for children with a range of disabilities for a variety of outcomes. For example, parent-implemented interventions have been effective for children with developmental disabilities (McConachie, Randle, Hammal, & Le Couteur, 2005) and for children with behavior disorders (e.g., Moes & Frea, 2002). Parent-implemented interventions are related to increases in communication skills (Gentry & Luiselli, 2008) and reductions in challenging behaviors (Duda, Clarke, Fox, & Dunlap, 2008).
However, when examined individually, the outcomes for parent-implemented interventions are mixed. Not all children or families respond positively to parent training programs (Lundahl, Risser, & Lovejoy, 2006; Roberts & Kaiser, 2011; Webster-Stratton & Hammond, 1997). For example, in their review of parent-implemented language interventions, Roberts and Kaiser (2011) documented a range of effect sizes for child language outcomes, and caution interpretations of their results due limited measurement of intervention or implementation fidelity. Lundahl et al. (2006) found parents experiencing multiple risk factors benefited more from individual than group trainings. In fact, several factors that might impact child outcomes have been identified across these reviews. These include parents’ use of the intervention strategies (i.e., intervention fidelity) and the training and support parents received (i.e., implementation fidelity). These factors are likely to mediate or moderate treatment outcomes (Beauchaine, Webster-Stratton, & Reid, 2005; Lundahl et al., 2006; Martinez & Forgatch, 2001).
Parent involvement in EI is directly related to its efficacy (Mahoney, 2009). Teaching parents to be responsive and supportive shapes their children’s development and has positive long-term outcomes (Dunst & Kassow, 2008; Powell & Dunlap, 2010; Sandall, Hemmeter, Smith, & McLean, 2005). Furthermore, teaching parents to teach their children new skills is associated with positive benefits for both the children and parents (Dunst et al., 2007). Thus, there is substantial research supporting parent-implemented intervention. However, the research on how to train parents is just emerging (Dunst & Trivette, 2012; Powell & Dunlap, 2010).
Although the efficacy of parent-implemented intervention has been examined across individual studies, no reviews to date have specifically focused on the intervention and implementation fidelity features of parent-implemented interventions for young children with disabilities. Previous reviews in this area (Harris, 1998; Probst, 2001) have lacked a systematic approach in assessing these fidelity features. As illustrated in Figure 1, both intervention fidelity and implementation fidelity of parent-implemented interventions will impact child outcomes. In fact, parents’ inconsistency and infrequency in using the intervention practice often explains the lack of effectiveness (Durlak, 2010). Relatedly, identifying effective practices for training parents and systems for measuring implementation fidelity has both practical (i.e., scaling up evidence-based practices) and research (i.e., identifying evidence-based practices) implications. The purpose of this literature review was to analyze implementation fidelity (i.e., parent training practices) and intervention fidelity (e.g., intervention strategies) within the literature on parent-implemented interventions. Methodological features and experimental rigor of the identified studies also were analyzed.
Method
Peer-reviewed parent training studies were identified through three steps. First, PsychINFO and ERIC databases were searched using the terms parent training or parent education or parent implementation and children with special needs or children with disabilities and intervention. Limits were set for peer-reviewed journal articles, those written in English, and those reporting studies involving human participants. Second, limits were set to include nine journals that focus on early childhood or general special education (see Table 1). We selected these nine journals to yield a sample of studies representative of the larger literature on parent-implemented intervention with young children with disabilities. Thus, we identified journals focused on ECSE and related areas with large readership and acceptable impact factors (i.e., range = 0.7-3.7). This yielded 113 studies. Third, both authors determined independently whether each of the 113 studies met the following inclusion criteria: (a) the purpose was focused on a parent-implemented intervention, (b) the intervention focused on improving child outcomes (e.g., language, play, reducing challenging behaviors), (c) the dependent variables included child behaviors, (d) participants included parents of children with disabilities and children ages 8 years or younger with disabilities, and (e) the study used an experimental design. The search results yielded 24 studies, and the authors had 100% agreement for study inclusion.
Number of Identified Articles From Selected Journals

After obtaining the full study report, we then independently extracted information regarding the following 32 variables from each study: the participant characteristics, settings, study design, independent variables, measurement of implementation and intervention fidelity, parent training components, dependent variables, social validity, overall outcomes, and study rigor (Gersten et al., 2005; What Works Clearinghouse [WWC] Single Case Research Design [SCRD] Standards, Kratochwill et al., 2010, 2013). These variables were selected to allow for a systematic analysis of implementation and intervention fidelity features. Each author independently coded all identified studies using a coding protocol and a data extraction spreadsheet designed for this review. The first author reviewed spreadsheets for consistency. Consensus identification was used for disagreements. Agreement was high; fewer than 10 disagreements occurred across studies and variables. Thus, overall agreement between the two authors was more than 95% across studies and variables.
Results
The 24 identified studies were published between 1972 and 2012. Additional details regarding the 24 studies are provided in subsequent sections. Each coded variable is described and summarized. One of the 24 studies focused on training personnel to coach parents and measured parent implementation of the intervention and child outcomes (Hester, Kaiser, Alpert, & Whiteman, 1996). The remaining 23 studies focused solely on parent-implemented interventions.
Participants
Parents
A total of 277 parents were included across these 24 studies (see Table 2). One-hundred and ninety-two mothers and 53 fathers were included across 23 studies; 1 study did not report the gender of parent participants (Yawkey, 1982). Twelve studies (50%) did not report parent ages. All of the 12 studies reporting parent ages included parents in their thirties. Two studies (8%) included parents younger than 21, and 6 studies (25%) included parents older than 40. Fifteen studies (63%) reported parent education levels. Ten of these 15 studies included parents with high school as their highest level of education and 11 included parents with some college. Ten studies reported parent socioeconomic status (SES). Seven of the 10 studies included families reporting low SES. Eleven studies (42%) reported parent race. Ten of these 11 primarily included white/Caucasian parents. One study took place in the Netherlands and included non-Western immigrant parents.
Parent Information
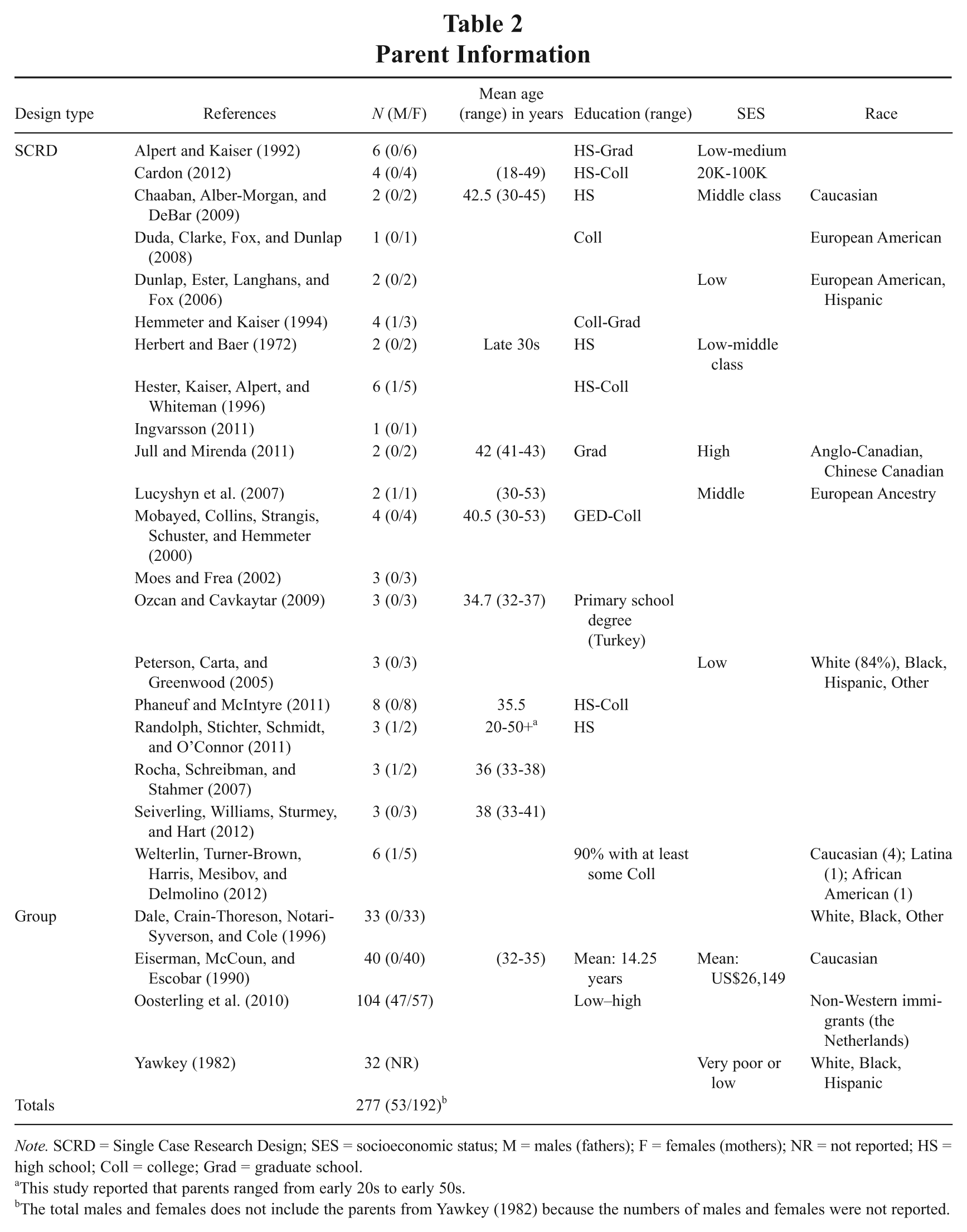
Note. SCRD = Single Case Research Design; SES = socioeconomic status; M = males (fathers); F = females (mothers); NR = not reported; HS = high school; Coll = college; Grad = graduate school.
This study reported that parents ranged from early 20s to early 50s.
The total males and females does not include the parents from Yawkey (1982) because the numbers of males and females were not reported.
Children
A total of 241 children were included across these 24 studies (see Table 3). The studies were coded for child age, disability category (i.e., Autism Spectrum Disorders [ASD], Developmental Delay, Speech/Language Delays, and Other), and the presence of challenging behaviors. The studies included children representing a wide range of ages and disabilities. The children ranged in age from 24 months to 8 years. Twenty-two (92%) included children between the ages of 3 and 5, 11 (46%) included children younger than 3, and 3 (13%) included children between 6 and 8 years old. Fifteen studies (63%) included children with an ASD. Four studies (17%) included children identified with developmental delays (excluding ASD and other developmental disorders). Ten studies (42%) included children with speech/language delays. Five studies (21%) included children with other disabilities. For example, Hemmeter and Kaiser (1994) included children with Down syndrome, cerebral palsy, and seizure disorders. Mobayed, Collins, Strangis, Schuster, and Hemmeter (2000) included a child with multiple genetic anomalies. The 20 SCRD studies were further coded for providing additional information regarding the children’s functional repertoires. Twelve of the 20 SCRD studies provided additional information (beyond standardized assessment) regarding the child participants functional repertoires’ related to the outcomes of the study. For example, Alpert and Kaiser (1992) provided information regarding children’s functional communication skills. Duda et al. (2008) and Dunlap, Ester, Langhans, and Fox (2006) provided information regarding the children’s challenging behavior and functional communication skills.
Child Information

Note. SCRD = Single Case Research Design; ASD = Autism Spectrum Disorder, S/L = speech and language, DD = developmental delay, O = other.
Range given when provided. Ages provided in months unless otherwise specified.
For SCRD studies, the authors also provided information regarding the child(ren)’s functional repertoire(s).
Setting
The primary parent training and intervention settings were identified across the 24 studies (see Table 4). One study did not report the parent training setting (Dale, Crain-Thoreson, Notari-Syverson, & Cole, 1996). In 14 (58%) of the 24 studies, parent training sessions were conducted only in the families’ homes. In 7 studies (29%) researchers conducted parent training only in clinics; in 2 studies researchers used both homes and clinics. In 18 (75%) of the 24 studies, the parents implemented the interventions only in homes. In 5 studies (21%) parents implemented the interventions only in clinics; in 1 study parents implemented the intervention in homes and clinics.
Intervention and Outcome Information Across Studies
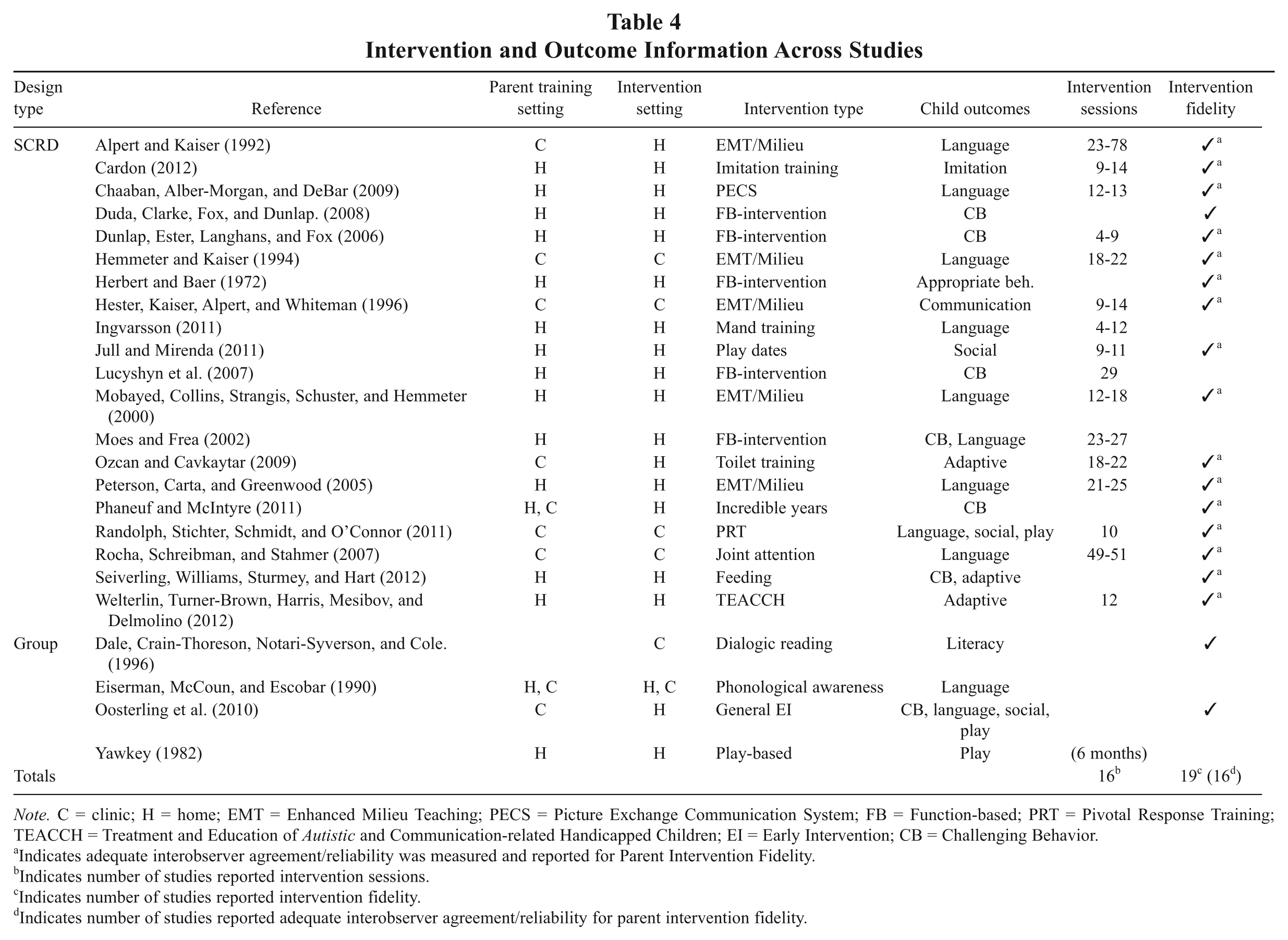
Note. C = clinic; H = home; EMT = Enhanced Milieu Teaching; PECS = Picture Exchange Communication System; FB = Function-based; PRT = Pivotal Response Training; TEACCH = Treatment and Education of Autistic and Communication-related Handicapped Children; EI = Early Intervention; CB = Challenging Behavior.
Indicates adequate interobserver agreement/reliability was measured and reported for Parent Intervention Fidelity.
Indicates number of studies reported intervention sessions.
Indicates number of studies reported intervention fidelity.
Indicates number of studies reported adequate interobserver agreement/reliability for parent intervention fidelity.
Intervention
Type
Sixteen different intervention types were included across these 24 studies (see Table 4). In 5 studies, the researchers examined parent-implemented milieu teaching, and in 5 others they examined functional assessment based interventions. The remaining intervention types were examined in 1 study each. For example, Chaaban, Alber-Morgan, and DeBar (2009) examined parent-implemented Picture Exchange Communication System (PECS) training. Phaneuf and McIntyre (2011) examined parent implementation of the Incredible Years curriculum. Seiverling, Williams, Sturmey, and Hart (2012) examined parent implementation of an escape-extinction based feeding intervention.
Child outcomes
Across the studies, researchers measured the following child outcomes: reducing challenging behaviors or improving language or communication, social, adaptive, literacy, play, or other skills (see Table 4). In 4 (17%) of the 24 studies, the researchers examined multiple types of child outcomes. Twelve studies (50%) examined interventions focused on improving child language development or communication skills. For example, Alpert and Kaiser (1992) and Hemmeter and Kaiser (1994) examined the effects of parent-implemented milieu teaching on child language. Seven studies (29%) examined interventions focused on reducing challenging behaviors. Duda and colleagues (2008) examined parent-implemented functional assessment based intervention focused on reducing the challenging behaviors of three siblings. Three studies each examined interventions focused on improving child social, adaptive, or play behaviors. For example, Randolph, Stichter, Schmidt, and O’Connor (2011) examined parent-implemented Pivotal Response Training on child language, social, and play behaviors. One study each examined interventions focused on improving child literacy, imitation, or appropriate behaviors.
Duration
This refers to the length of time researchers measured or reported parent use of the intervention and measured child outcomes. Researchers reported the number of intervention sessions in 16 (67%) of the 24 studies (see Table 4). The number of sessions ranged from 4 to 78 sessions. One study did not report the number of sessions, but reported the duration in months (i.e., 6 months; Yawkey, 1982).
Parent Training
Training practices
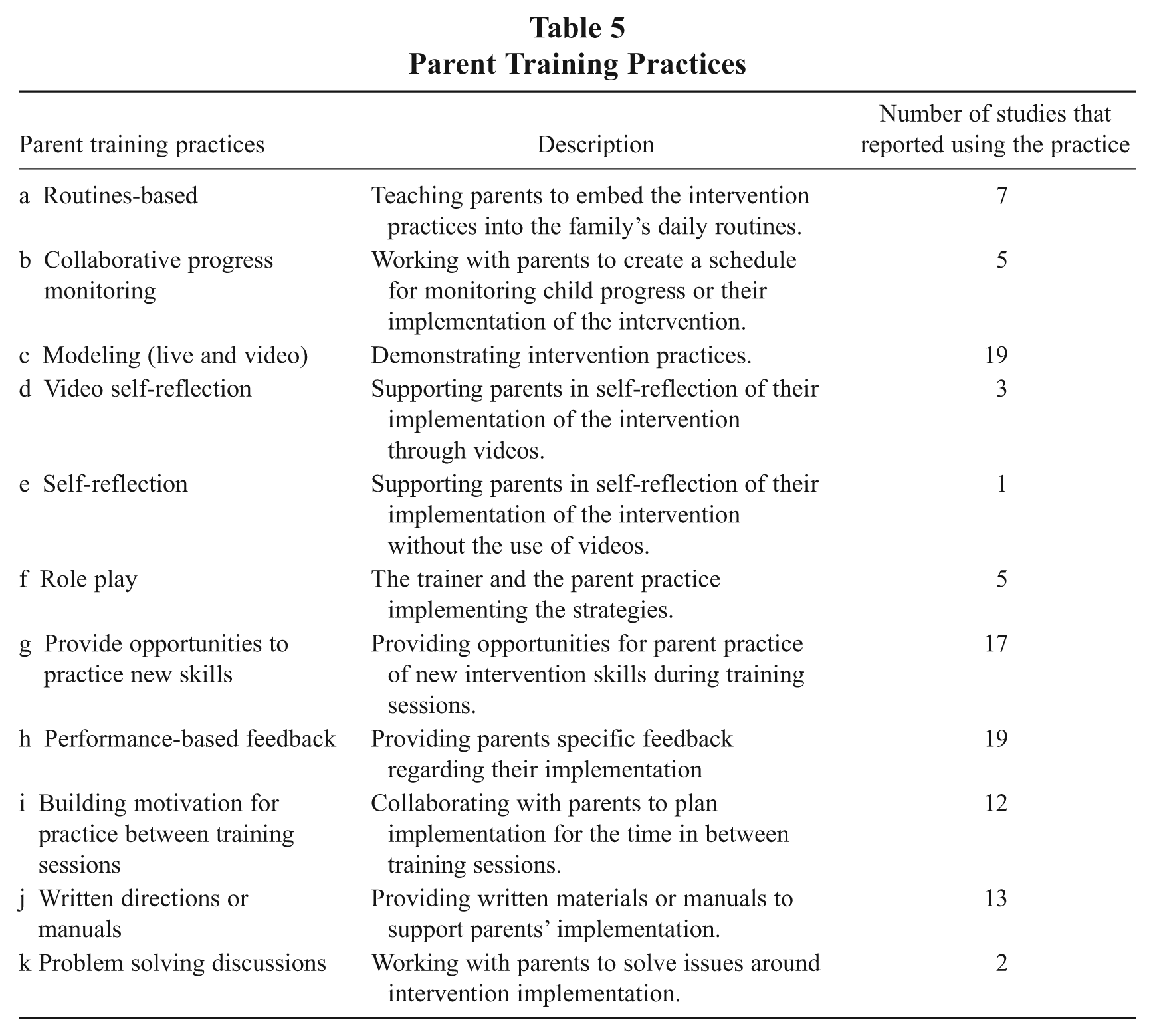
Researchers in the 24 studies used the follow practices to train parents: (a) a focus on routines, (b) collaborative progress monitoring, (c) live or video modeling, (d) video self-reflection, (e) self-reflection, (f) role-play, (g) opportunities to practice new skills, (h) performance-based feedback, (i) motivation for practice between sessions, (j) written directions or manual, and (k) problem solving discussions (see Tables 5 and 6). Nineteen (79%) of the 24 studies used live or video modeling, and 19 (79%) used performance-based feedback. For example, in Duda and colleagues (2008), trainers modeled and described the intervention procedures, provided positive feedback, and discussed the current session with the parent. Likewise, in Rocha, Schreibman, and Stahmer (2007), the trainers modeled joint attention techniques and then provided instruction and feedback while the parent practiced. Seventeen studies (71%) provided opportunities for parents to practice new skills. For example, in Phaneuf and McIntyre (2011) trainers provided parents with opportunities to practice positive interactions with their children and provided corrective feedback. Thirteen studies (54%) provided written directions or a manual to support parent implementation, and 12 (50%) supported parent practice between sessions. For example, in Jull and Mirenda (2011), trainers provided parents with a play date planning handout to help parents facilitate play dates with their children between sessions. In Alpert and Kaiser (1992), trainers taught mothers to use milieu teaching practices incidentally throughout their days and helped mothers identify natural opportunities. Eight studies (33%) embedded the intervention into the family’s daily routines. Five (21%) used collaborative progress monitoring or role-play to support parent implementation. Three (13%) used video self-reflection. Two (8%) used collaborative problem solving, and 1 (4%) encouraged parents to engage in self-reflection without videos. Most studies used a combination of practices: 23 (96%) of the 24 studies used two or more practices, 19 (79%) used three or more practices, and 18 (75%) used four or more practices.
Parent Training Practices
Parent Training Information

✓ = measured and reported.
Reported trainer education or experience.
a = routines based, b = progress monitoring, c = live or video modeling, d = video self-reflection, e = self-reflection, f = role-play, g = provided opportunities to practice new skills, h = performance-based feedback, i = motivation for practice between sessions, j = written directions or manual, k = problem solving discussions.
Equal numbers of intervention and parent follow-up sessions.
Interobserver agreement/reliability measured and reported for parent training implementation fidelity.
Experimentally examined the relation between training and parent implementation (n = 13).
Separate training and follow-up
The 24 studies were coded for including a separate parent training session prior to commencing the intervention and additional follow-up after the parent training sessions. Three studies (13%) conducted a single training session without follow-up training (i.e., Chaaban et al., 2009; Dale et al., 1996; Herbert & Baer, 1972). Most researchers across these studies provided follow-up coaching to support parent implementation (n = 21, 88%; see Table 6). Twelve of the 21 studies that included follow-up training conducted a separate training prior to follow-up. Across the studies, the follow-up training included the practices described in the previous section. For example, Lucyshyn and colleagues (2007) reported staggering the training and support across routines. They provided an initial training during the dinner time routine for two sessions, then provided ongoing modeling, coaching, practice, self-monitoring, and problem solving during subsequent dinner time routines. They repeated this level of training and support for the going-to-bed routine and community outings. Similarly, Moes and Frea (2002) taught mothers to implement Functional Communication Training (FCT) procedures using modeling and feedback during initial training sessions. Once mothers could use the FCT strategies independently (>80% intervention fidelity) the researchers faded supports, but continued to provide coaching (e.g., feedback, problem solving discussions, motivation to practice between sessions) to mothers on their use of FCT during daily routines.
Trainer education
Across this literature, there was a dearth of information on trainer qualifications or education (see Table 6). Only 2 (8%) of the 24 studies reported the trainer education or experience (i.e., Hester et al., 1996; Mobayed et al., 2000). Hester and colleagues (1996) and Mobayed and colleagues (2000) reported trainers’ education and experience teaching children with disabilities and working with parents.
Training duration
Fourteen studies (58%) reported the duration of the parent training. When reported, the duration was most frequently reported in number of sessions. The number of sessions ranged from 3 to 78 (see Table 6). For 6 studies (25%), the training duration was reported to be similar to the intervention duration. Thus, in these studies parent training/follow-up support was provided for the duration of the intervention.
Fidelity Measurement
Intervention fidelity
The focus across the identified studies was parent implementation of specific intervention procedures (i.e., intervention fidelity) and child outcomes were the primary dependent variables. Improvements in child outcomes were hypothesized to result from parents’ high-fidelity use of the intervention. Thus, intervention fidelity should be measured and reported across all studies. Researchers in 19 (79%) of the 24 studies reported intervention fidelity (see Table 4). Sixteen of these 19 also reported interobserver agreement (IOA) on intervention fidelity.
Generalization and maintenance of parent use of the intervention
The generalization and maintenance of parent use of the intervention procedures is essential to ensure the sustainability of the intervention. Parent generalization of the intervention procedures was measured in 11 (46%) of the 24 studies (see Table 6). Parent generalization of the intervention was measured across materials, settings, prompts, and routines. Five studies measured generalization across routines and 3 measured generalization across settings. For example, Hemmeter and Kaiser (1994) measured generalization of parent use of the milieu procedures from the clinic setting to their home environment. Nine (38%) of the 24 studies measured parent maintenance of the intervention procedures. The measurement of maintenance of parent use of the intervention ranged from 1 week (Cardon, 2012) to 7 years (Lucyshyn et al., 2007) after the study ended.
Implementation fidelity
In this literature, implementation fidelity refers to the practices used to train parents to use the intervention procedures. Measurement of implementation fidelity is essential to ensure that training procedures are carried out as planned and to inform evidence-based practices. Although all studies provided information regarding the implementation practices, only seven studies (29%) reported measuring implementation fidelity (see Table 6). Of these seven, only three reported IOA on implementation fidelity. For example, Dunlap et al. (2006) used a checklist to record implementation of the procedures and content of the parent training but did not report IOA on the use of the checklist. Mobayed and colleagues (2000) measured the researchers’ adherence to parent training procedures including providing parent feedback, and reported IOA on adherence to these parent training procedures.
Social Validity
The measurement of social validity is imperative to determine the feasibility and utility of the parent training and the social significance of the child outcomes. Researchers in 15 (63%) of the 24 studies measured social validity of the intervention procedures or outcomes or both. The procedures used to measure social validity varied across studies. For example, Alpert and Kaiser (1992) and Eiserman, McCoun, and Escobar (1990) measured parent satisfaction with the training procedures using a written rating scale or questionnaire. Duda and colleagues (2008) measured the acceptability, efficacy, and feasibility of the intervention by having three parents of preschool age children rate the child and parent behaviors, the intervention procedures, and their personal level of comfort with implementing the intervention via video segments of the participants.
Study Design and Rigor
Design
All studies in this review examined the effects of the parent-implemented intervention on child behaviors. Twenty (83%) of the 24 research studies utilized SCRD. Four (17%) used randomized controlled trial group designs (Dale et al., 1996; Eiserman et al., 1990; Oosterling et al., 2010; Yawkey, 1982). Although the identified studies focused on parent-implemented interventions, 13 (54%) of the 24 studies also examined experimentally the relation between training and parent implementation (see Table 6). For example, Alpert and Kaiser (1992) used a multiple baseline design to stagger implementation of the coaching across mothers. This allowed for an examination of the functional relation between coaching and parent implementation as well as between parent implementation and child language outcomes. The remaining 11 (46%) studies only examined experimentally the relation between parent-implemented interventions and child outcomes.
Application of the WWC SCRD standards
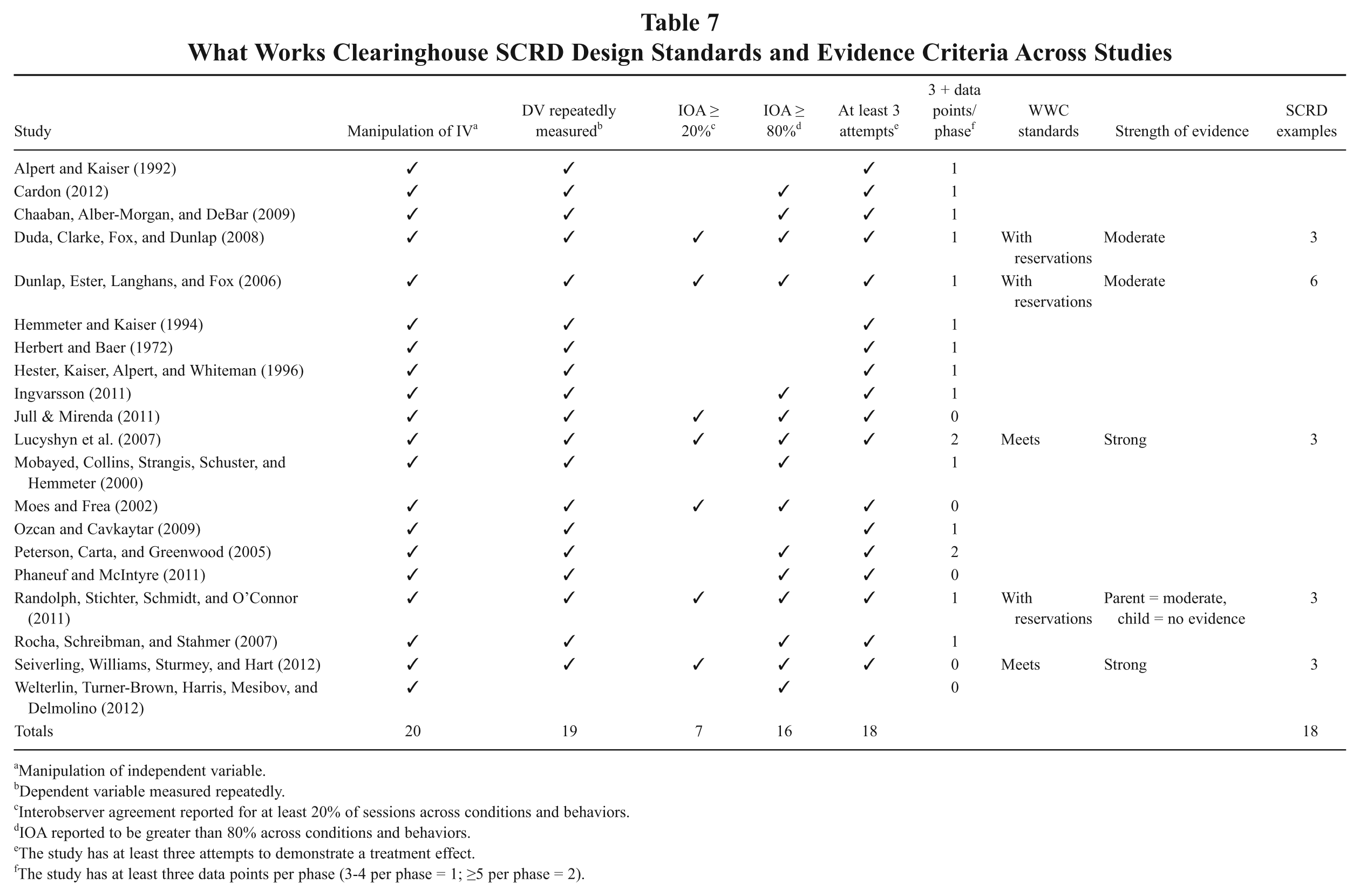
The WWC (Kratochwill et al., 2010, 2013) SCRD design standards and evidence criteria were used to evaluate whether the SCRD studies in this literature demonstrated sufficient rigor, evidence, and replication (see Table 7). Six design standards (Kratochwill et al., 2010, 2013) were used to evaluate each study. These were analyzed using standards designed and used in previous behavioral research (e.g., Maggin & Chafouleas, 2011; Maggin, Johnson, Chafouleas, Ruberto, & Berggren, 2012). The initial four standards were scored using a dichotomous scale (i.e., present, not present) at the study level and the final two design standards were coded at the case level using a dichotomous scale for the fifth standard and trichotomous scale for the sixth. The individual studies were ultimately classified as: (a) Meets Standards if they provided five or more data points per condition and met all other design standard criteria, (b) Meets Standards With Reservations if there were three or four data points per condition and they met all other criteria, and (c) Does Not Meet Standards if there were fewer than three data points per condition or the case failed to meet any other criteria. The strength (i.e., strong or moderate) of the evidence was analyzed for the studies meeting standards or meeting standards with reservations using predetermined evidence criteria based on the WWC standards (e.g., Maggin & Chafouleas, 2011). Only 2 of the 20 SCRD studies (Lucyshyn et al., 2007; Seiverling et al., 2012) were classified as Meets Standards. Both studies also provided strong evidence for a treatment effect. Three of the 20 SCRD studies were classified as Meets Standards With Reservations due to having fewer than five but more than three data points per condition. All 3 studies provided moderate evidence of a treatment effect for at least one outcome. The remaining 15 SCRD studies were classified as Does Not Meet Standards; thus, provided no evidence of a treatment effect. Two (10%) of the studies did not meet standards due to having fewer than three data points per phase and 13 (65%) did not meet standards due to inadequate measurement of IOA.
What Works Clearinghouse SCRD Design Standards and Evidence Criteria Across Studies
Manipulation of independent variable.
Dependent variable measured repeatedly.
Interobserver agreement reported for at least 20% of sessions across conditions and behaviors.
IOA reported to be greater than 80% across conditions and behaviors.
The study has at least three attempts to demonstrate a treatment effect.
The study has at least three data points per phase (3-4 per phase = 1; ≥5 per phase = 2).
Group study rigor
The study quality of the four group design studies included in this review was evaluated using standards derived from the quality indicators for group experimental research outlined by Gersten and colleagues (2005). Nine standards were created based on their quality indicators (see Table 8). These standards include (a) random assignment, (b) comparable groups, (c) adequate description of the intervention and comparison condition, (d) the use of multiple outcome measures, (e) reliability of outcome measures, (f) evidence of validity of outcome measures, (g) fidelity of intervention reported, (h) effect sizes reported or computable with information provided, and (i) attrition is reported and is lower than 30%. Only one study, Oosterling and colleagues (2010), met all nine standards. One study (Yawkey, 1982) only met three of the nine standards. All four studies used random assignment to groups, reported comparable groups, and used multiple outcome measures. Three studies adequately reported the independent variable, provided validity information for outcome measures, and provided effect sizes (Dale et al., 1996; Eiserman et al., 1990; Oosterling et al., 2010). Only two of the four studies reported intervention fidelity (Dale et al., 1996; Oosterling et al., 2010). Only Oosterling and colleagues (2010) provided adequate reliability measures and information regarding attrition.
Group Design Study Quality
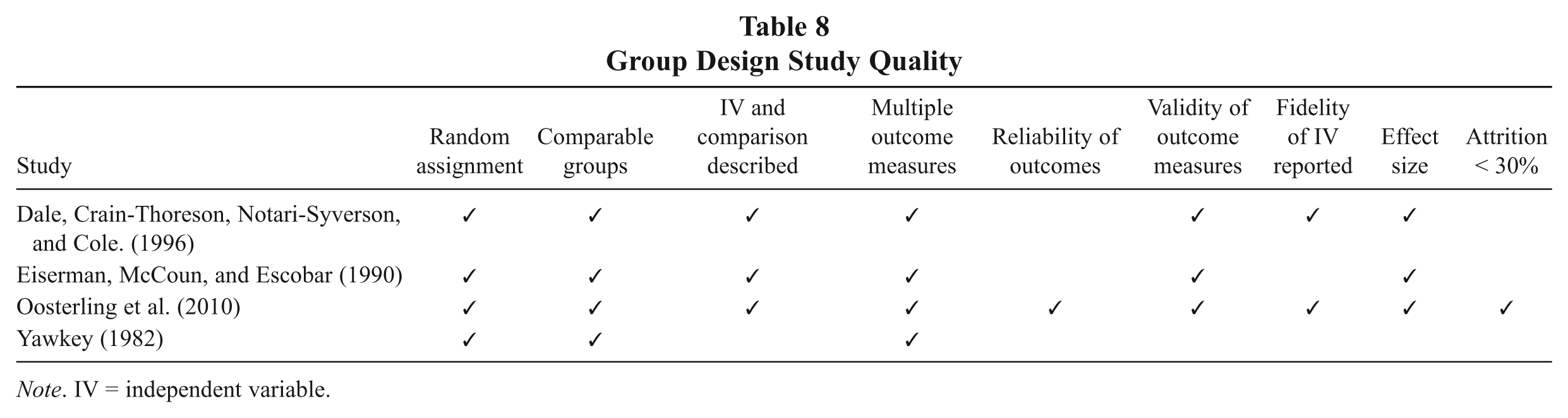
Note. IV = independent variable.
Overall Study Outcomes
The findings across all 24 studies indicated that parent-implemented interventions were effective. That is, researchers across all studies reported that parents implemented the intervention and child outcomes improved. In fact, when reported, parents implemented the intervention procedures with high fidelity. However, these results should be interpreted with caution given the lack of implementation fidelity and the minimal number of studies meeting contemporary design standards.
Discussion
State of Literature
The purpose of this review was to examine implementation and intervention fidelity features of parent-implemented intervention with young children with disabilities. Given the burgeoning field of implementation science and the unique triadic features of parent training as presented in Figure 1, a systematic analysis of parent training practices was warranted. Although multiple reviews on parent-implemented interventions for young children with disabilities have been conducted (e.g., function-based interventions, Conroy, Dunlap, Clarke, & Alter, 2005; interventions for children with autism, McConachie & Diggle, 2007; language interventions, Roberts & Kaiser, 2011), none have systematically examined implementation or intervention fidelity features. An examination of these fidelity features is critical to identify evidence-based parent-implemented interventions and effective parent training practices (Fixsen et al., 2005; Powell & Dunlap, 2010). This review identified several important strengths. For example, most studies reported intervention fidelity (79%) and provided follow-up training (88%) to support parent implementation of child-focused interventions. Furthermore, more than half (n = 13, 54%) examined experimentally the relation between parent training and parent implementation as well as parent implementation and child outcomes. However, only seven studies (29%) reported implementation fidelity and six (25%; 1 group and 5 SCRD) met contemporary research design standards. These and additional findings are discussed in the subsequent sections.
Measuring Intervention Fidelity
The measurement of intervention fidelity is imperative to ensure that the parents implemented the intervention as intended. Furthermore, quality fidelity measures should include evidence of reliability and validity (Odom, Boyd, Hall, & Hume, 2010). Nineteen (79%) of the 24 studies measured intervention fidelity and 16 (84%) of these reported IOA estimates for intervention fidelity. Thus, this is a strength within this sample of literature. However, fewer than half (n = 11, 46%) of the 24 studies measured parent generalization of the intervention procedures, and only 8 measured outcomes across daily routines. Few studies (n = 9, 38%) measured maintenance of parents’ use of the intervention procedures once the study ended. Thus, there was no assurance that parents sustained implementation, which might impact the children’s improvements on the target behaviors over time. This lack of maintenance has been noted in previous reviews of parent-implemented interventions (Roberts & Kaiser, 2011).
Measuring Implementation Fidelity
In this review, implementation fidelity referred to the measurement of the specific practices used to train parents across parent training sessions. Few studies (7 of 24, 29%) measured and reported implementation fidelity. This is not surprising given implementation science is a burgeoning field. Previous reviews of parent-implemented intervention have noted similar findings. For example, Roberts and Kaiser (2011) found only 9 of the 18 identified parent-implemented language intervention studies provided information regarding parent training. Implementation features (i.e., the practices used to train parents) were as crucial as the intervention features to establish evidence-based practices. In fact, substantive literature reviews have demonstrated that actual benefits materialize with effective interventions and effective implementation practices, but not without both (Fixsen, Blase, & Campbell, 2012). In addition, it makes practical sense to have a clear understanding of both evidence-based implementation practices and evidence-based intervention practices. This distinction between the two is rarely made in intervention research. As shown in Figure 1, both high-fidelity implementation of evidence-based parent training and high-fidelity implementation of evidence-based practices are required to have a positive impact on child outcomes. For example, although most studies in this review provided follow-up support, performance-based feedback, modeling, and opportunities for practice, only seven studies measured the implementation of these components. These might be essential components of parent training and have a positive impact on parent high-fidelity implementation. In addition, rigorous studies measuring and examining these components systematically, both separately and as part of a larger training package, are warranted. Relatedly, IOA estimates for implementation fidelity were underreported in this literature (only three of seven reported). These are not currently included in design standards for SCRD or group design studies. However, as implementation science becomes more widely regarded, one might assume that measurement of implementation components (including IOA) will be considered an essential design standard for identifying evidence-based practices.
Providing Follow-Up and Support
As described previously, follow-up support was provided in most of the studies in this review (n = 21, 88%). Moreover, across the studies, when measured, parents implemented the intervention with high fidelity. This finding is supported by the larger implementation science literature. In fact, substantive literature reviews have demonstrated that follow-up support is related to higher rates of fidelity and improved outcomes for children (Fixsen et al., 2005). Thus, this review aligns with the professional development research and suggests that follow-up training might be an essential aspect of parent interventions. However, as discussed previously, a major limitation of this review is the lack of measurement of implementation fidelity. Only 6 (29%) of the 21 studies providing follow-up support reported implementation fidelity of the specific follow-up coaching practices. The practices were coded based on the study authors’ reporting describing use of the practice regardless of the level of evidence provided. The level of evidence for the specific practices used varied across studies.
Effective Training Practices
Although researchers in all studies examined parent-implemented interventions, only 13 examined empirically the relation between the parent training and parent implementation of the intervention. Thus, 13 studies could conclude that their specific training practices were functionally related to high-fidelity parent implementation of the intervention. This should be interpreted with caution, however, given only 3 of these studies also reported implementation fidelity and IOA. Moreover, there are some notable consistencies across the studies. Performance-based feedback, modeling, and opportunities for practice emerged from this review as the most frequently used parent training practices. In fact, among the 13 studies that examined parent training empirically, 11 used modeling and feedback within the training and 10 provided opportunities for parents to practice the intervention during training sessions. This finding is similar to findings from recent reviews of parent-implemented interventions (Dunst & Trivette, 2012; Powell & Dunlap, 2010) and recommended practices in family coaching (McWilliam, 2010; Rush & Shelden, 2011) in which several promising practices have emerged, including performance-based feedback, modeling, and practice. These practices also have been included in effective coaching models for early childhood practitioners (Barton, Kinder, Casey, & Artman, 2011; Fox, Hemmeter, Snyder, Binder, & Clarke, 2011; Strain & Bovey, 2011). For example, several studies provided performance-based feedback verbally using positive and corrective comments based on specific examples of the parents’ behaviors during or after each session (e.g., Chaaban et al., 2009; Mobayed et al., 2000; Rocha et al., 2007). Other studies provided performance-based feedback using graphs displaying the frequency of use of the intervention strategies (Alpert & Kaiser, 1992), directive statements regarding how to implement the strategies (Moes & Frea, 2002), and written examples of correct and incorrect uses of the strategies (Hemmeter & Kaiser, 1994; Hester et al., 1996). The larger professional development literature supports the use of performance-based feedback as an effective practice for changing adult behaviors (Barton et al., 2011; Casey & McWilliam, 2011).
Study Rigor
Twenty (83%) of the 24 studies in this review used SCRD methodologies. The authors used the WWC standards to examine SCRD study rigor. Although 14 (65%) of the 20 SCRD studies were completed prior to the publication of the WWC SCRD Technical Documentation (Kratochwill et al., 2010), the standards align with the Horner et al. (2005) quality indicators and previously published guidelines for SCRD (e.g., Tawney & Gast, 1984). Only 1 of the 6 studies that were published after the WWC standards met those standards and 1 met with reservations. The WWC standards are more stringent than traditional convention regarding the number of data points per condition (i.e., WWC standards require at least five data points per condition). Thus, not surprisingly, only 2 studies had at least five data points across conditions and 13 had at least three or four. However, this was not the main reason for not meeting the WWC design standards. Of the 13 studies that had at least three or four data points per condition (and could meet standards with reservations), 10 had inadequate IOA measures. Thirteen studies did not report IOA for 20% of sessions across conditions, participants, and behaviors. Likewise, 4 reported IOA estimates lower than 80%. Only 2 SCRD studies (Dunlap et al., 2006; Randolph et al., 2011) that met the WWC standards (i.e., both met with reservations) also reported implementation fidelity. There are notable strengths within the rigor of this SCRD literature. For example, 15 (75%) of the studies included at least three data points per phase, 19 (95%) repeatedly measured the dependent variable, and 18 (90%) had at least three attempts to demonstrate a treatment effect.
The WWC recommends combining SCRD studies into a single summary rating once there are at least five studies that meet design standards or meet design standards with reservations across three different research teams with at least 20 examples (e.g., participants, behaviors, settings) across the studies. This literature meets the first two criteria; however, there were only 18 examples (i.e., participants, behaviors; see Table 7) across the five studies. This analysis should be interpreted with caution given these studies are just a sample of the literature.
Similarly, across the group studies, only 1 met all design standards, but all four studies used random assignment of participants to treatment groups. Furthermore, all four studies reported comparable groups and used multiple outcome measures. These are strengths of the group studies in this sample. Even so, only one study provided adequate reliability of outcome measures and information regarding attrition. The design standards used to evaluate these studies were published after three of the four studies. Thus, results should be interpreted with caution.
Additional Study Features
Trainer education
Trainer education and training specific to the intervention was reported inadequately across these studies. Only 2 studies (8%) reported trainer education or experience with family coaching and in EI/ECSE. Previous reviews have noted similar findings. For example, in their meta-analysis of parent-implemented language interventions, Roberts and Kaiser (2011) found a dearth of information regarding the personnel who trained parents. Information on how trainers were prepared to coach families was not provided in any of the 24 studies. Trainer experience and preparation are essential features and are imperative for ensuring high-fidelity implementation. The trainers (i.e., the implementation team) are accountable for full and effective use of the intervention (Fixsen et al., 2012), which might require different levels of training or education based on the specific intervention. Trainers’ expertise in the intervention topic and experience in coaching adults is an important consideration.
Social validity
Social validity was measured in more than half of the studies (n = 15, 63%). Although the studies measured different aspects of social validity, using different formats, when reported, social validity was positive. When measured, parents were found to be satisfied with the outcomes, training procedures, intervention, and goals of the intervention. This is a positive finding, because when parents are satisfied they are more likely to sustain implementation of the intervention (Strain, Barton, & Dunlap, 2012).
Natural settings
An encouraging finding in this review is the primary settings of the training and the interventions. Sixteen of the 24 studies (67%) conducted both the parent training and the intervention in natural settings—homes. However, only 8 (33%) of the 24 studies reported focusing on daily routines. This is significant because recommended family-centered practices focus on teaching parents to embed multiple learning opportunities during meaningful routines and activities (Jung, 2003; McWilliam, 2010). A family-centered approach means practitioners focus on increasing the quality of parent–child interactions within daily routines and activities, which is likely to enhance family quality of life (McWilliam, 2010).
Future Research
The results of this review highlighted several areas for future research. Perhaps most importantly, future research in parent-implemented interventions should include documentation and measurement (i.e., implementation fidelity) of the parent training and coaching practices. Systematic measurement of implementation fidelity is needed to identify effective practices for training parents to implement child-focused interventions. Based on generally accepted standards for fidelity (Horner et al., 2005), implementation fidelity measurement should be direct and continuous. In addition, future research should examine systematically the general coaching practices and specific forms of these practices. For example, future research might examine the specific characteristics of performance-based feedback that are related to its effectiveness in improving parent implementation (e.g., Does feedback need to include positive and corrective examples? Does feedback need to be delivered during or immediately after a practice session or at a later time? Do all parents respond to written or graphical feedback?). Future research also might consider adapting the framework of telemedicine practices in which implementation support can be communicated through handheld hardware devices such as cell phones, portable laptop computers/iPads, in the forms of emails, text messages, and video chats (Barton & Wolery, 2007; Bigelow, Carta, & Lefever, 2008; Harper, 2006).
As described previously, fewer than half of the studies measured generalization or maintenance of parent use of the intervention. This is consistent with previous reviews (Roberts & Kaiser, 2011). Thus, future research should examine strategies for fading supports to promote the sustainability of parent-implemented interventions across settings and routines. In fact, both generalization and maintenance of parents’ implementation of the intervention are essential for establishing evidence-based parent-intervention practices. The ongoing adoption and use of the intervention practices will have a direct impact on child outcomes. Relatedly, future studies should examine the duration of training that affects outcomes to determine what is cost-efficient while ensuring intervention sustainability.
Limitations
There are several limitations worth noting. First, the synthesis is not a comprehensive review of all parent interventions for children with disabilities. The specific journals identified were selected based on their foci, readership, and impact factors; additional studies might have been identified if other journals were included. However, the results from this review are supported by other reviews of parent-implemented interventions with young children (e.g., Meadan, Ostrosky, Zaghlawan, & Yu, 2009; Roberts & Kaiser, 2011). Meadan et al. (2009) and Roberts and Kaiser (2011) also noted a lack of measurement of implementation fidelity. Second, the large number of variables examined in this literature increases the probability of human error in data extraction. This was minimized because the two authors coded all studies independently and discussed disagreements. However, more stringent reliability calculations would increase confidence in the results. Third, applying contemporary research criteria to studies published more than two decades earlier is bound to indicate weakness, and might not indicate current strengths. Thus, the use of these standards should not discount the strengths in the parent-implemented intervention literature (e.g., use of natural settings, measurement of intervention fidelity). Finally, the search criteria used might have excluded studies that were not labeled explicitly as parent-implemented interventions.
Conclusion
Implementing evidence-based practices can be a complex undertaking and must include adequate resources and supports. Thus, “fidelity assessment is not just a nicety of experimental endeavors; it has a direct bearing on how well the components should be used in practice when specific outcomes are desired” (Wolery, 2011, p. 156). Unquestionably, we need to expand the parent-implemented intervention literature to examine fidelity features rigorously and systematically, including which training practices work for which parents under which conditions for which type of interventions or child outcomes. It might be that specific training practices are better suited for certain populations or intervention types. However, this was unclear based on the current literature. Furthermore, neither implementation nor intervention practices are likely to result in positive outcomes if they are not used as intended. Promising practices have emerged from both the early childhood professional development and parent training research, but the research and evidence on implementation fidelity features and their measurement pales in comparison with the research on effective intervention practices. The field needs to promote the measurement of implementation fidelity and intervention fidelity to ensure that we are identifying and effectively measuring those interventions and supports needed for implementation that are sustainable and doable at scale to have positive effects on all young children with disabilities and their families (Fixsen et al., 2012).
Footnotes
Authors’ Note:
Erin E. Barton, School of Education and Human Development, University of Colorado Denver; Angel Fettig, Department of Curriculum and Instruction, University of Massachusetts Boston. Erin E. Barton is now at Department of Special Education, Vanderbilt University.