
Abstract
Although there is ample evidence that endorsement of traditional masculinity ideology may negatively affect veteran men’s military to civilian transition, it remains unclear which specific facets of traditional masculinity are most likely to impede successful transition to civilian life. To better understand the association between traditional masculinity ideology and veteran transition, this study sought to examine the relationship between five facets of traditional masculinity ideology (restrictive emotionality, avoidance of femininity, toughness, dominance, and self-reliance) and four factors associated with difficult veteran transition (posttraumatic stress disorder [PTSD], depression, perceived social support, and alcohol-related problems) in (N = 289) veteran men. Results indicate that restrictive emotionality was the most significant contributing facet of traditional masculinity ideology to PTSD, depression, and perceived social support, whereas avoidance of femininity was the masculinity facet most significantly associated with alcohol-related problems. Theoretical and clinical implications are discussed.
For many service members, military to civilian transition is an arduous experience (Thompson et al., 2017). Approximately 25% of Canadian veterans (Dallaire & Wells, 2014) and 44% of American veterans (Segal & Segal, 2004) report their adjustment to civilian life as being difficult or challenging. These are worrisome statistics considering that veterans who experience difficulty during transition to civilian life are at greater risk of deleterious long-term psychosocial problems such as homelessness, addiction, unemployment, divorce, and suicidality (for a review, see Shields et al., 2016). There are several factors that may explain why some veterans find readjustment to civilian life challenging, whereas others make the transition with little or no difficulty. Among the most commonly cited factors associated with difficult transition to civilian life are social isolation and mental health difficulties—namely, posttraumatic stress disorder (PTSD), depression, and substance use disorder (for reviews, see Rose et al., 2018; Shields et al., 2016).
Frequently overlooked as a factor that may potentiate difficult military to civilian transition is the continued enactment or endorsement of traditionally masculine behaviors that are emphasized via military culture and training. In civilian life, these behaviors, which include but are not limited to marked stoicism, aggression, dominance, and rigid self-reliance, may be regarded by society as less adaptive (Brooks, 1990, 2001). Although men in in the military adhere to these culturally embedded masculinity norms in diverse ways and to variable degrees, such behaviors, or the belief that they symbolize the ideal representation of manhood (i.e., traditional masculinity ideology; Levant & Richmond, 2008), is, for many veteran men, a core feature of their military life and identity (Barrett, 1996). Although many men who elect to join the military identify with hypermasculine culture prior to entering the Armed Forces (Barrett, 1996; Brooks, 2001), others undergo a “secondary socialization” (Arkin & Dobrofsky, 1978, p. 159) via military training and culture, which promotes, tests, and celebrates hypermasculinity to prepare members of the military for combat (Fox & Pease, 2012). In many ways, the structure and values of the military—clearly defined hierarchy, prioritization of reason over emotion, and emphasis on strength over weakness—align with traditional masculinity ideals, such as toughness, dominance, and control (Chen & Dognin, 2017).
Although it may be the case that successful military missions necessitate the performance of traditional masculinity ideals, there is empirical evidence that these behaviors, or the belief that they define the optimal performance of manhood, can precipitate challenges that lead to a difficult military to civilian transition. Specifically, there is evidence that endorsement of traditional masculinity ideology in veteran men increases the risk of PTSD (e.g., Cox & O’Loughlin, 2017), depression (e.g., Jakupcak et al., 2014), lack of social support (e.g., Jakupcak et al., 2006), and substance abuse (e.g., Lorber & Garcia, 2010).
Although endorsement of traditional masculinity ideology has consistently been linked to psychosocial difficulties, it has been argued that viewing traditional masculinity as inherently problematic is overly simplistic, as masculinity ideals generally, and within military culture specifically, are complex, situational, and contextual (e.g., Green et al., 2010). For example, there is recent research suggesting that traditional masculinity can be seen alternately as a danger and as a resource for veteran men’s health and well-being (Caddick et al., 2015). Moreover, it is important to note that traditional masculinity ideology is not a “normative referent” for men, but rather a common constellation of standards and expectations for men in the Western world (Levant, 1996, p. 259). For these reasons, it has been suggested that traditional masculinity be conceptualized as a multidimensional construct (e.g., Higate, 2003), and one that is not assumed to be dichotomously either good or bad.
Military Transition Theory
Military transition theory (Castro & Kintzle, 2014) provides a framework through which the effect of traditional masculinity ideology on veteran transition can be understood. Within military transition theory, endorsement of traditional masculinity ideology may be considered a personal and cultural (i.e., military culture) factor that contributes to the foundation of the transition trajectory. According to the theory, personality and cultural factors may affect individual adjustment factors, such as a person’s coping styles, attitudes, and beliefs, which subsequently impact transition outcomes, including readjustment to family life, mental health, and social and community engagement. Below, we review how traditional masculinity ideology and veteran transition intersect with PTSD, depression, social support, and alcohol use, respectively.
Masculinity and PTSD
Members of the military are frequently exposed to traumatic events throughout the course of their military careers, such as being attacked or ambushed, involved in combat, accidental injury, or witnessing someone being badly injured or killed (Hoge et al., 2004). Although some service members recover from such trauma exposure, many continue to experience trauma-related symptoms (i.e., re-experiencing symptoms, avoidance symptoms, negative changes in cognitions and mood, and alterations in arousal or reactivity symptoms) far past the occurrence of the traumatic event, often meeting diagnostic criteria for PTSD (American Psychiatric Association, 2013).
Although there are several factors that may potentiate the development of PTSD following exposure to a traumatic event (for a review, see Schnurr et al., 2004), it has been suggested that endorsement of traditional masculinity ideology increases the risk of developing PTSD following exposure to a traumatic event predominantly through avoidance of behaviors associated with trauma recovery (Garcia et al., 2011). For example, the restrictive emotionality and self-reliance facets of traditional masculinity ideology may impede emotional processing of the traumatic experience by encouraging veterans to actively avoid discussing their experience, reactions, and the impact of the event with others, as doing so would be discordant with traditionally masculine ideals (i.e., may result in a lack of emotional control or convey that one is unable to manage his symptoms independently). As a result, important recovery resources, such as social support, are obfuscated, willingness to seek mental health care is reduced, or, in cases where help is sought, responsiveness to clinical interventions for PTSD that aim to interrupt avoidance of distressing trauma-related emotions, beliefs, and memories is impeded (Lorber & Garcia, 2010).
Although the relationship between traditional masculinity and PTSD is conceptually plausible, results of empirical studies examining this association in veteran men are mixed. Cox and O’Loughlin (2017) found that traditional masculinity ideology predicted PTSD, whereas Garcia et al. (2011) found that only a specific facet of traditional masculinity—self-reliance—predicted PTSD-related hyperarousal symptoms. Unexpectedly, Garcia et al. (2011) also found that the masculinity-congruent facet of success dedication may have a protective function against PTSD-related avoidance symptoms. Jakupcak et al. (2014) found a relationship between the emotional toughness facet of masculinity and PTSD. Still others (e.g., Jakupcak et al., 2006) have found a nonsignificant relationship between PTSD symptom severity and traditional masculinity. These varied empirical findings indicate the need for additional research on larger samples that involve more in-depth examination of the relationship between traditional masculinity ideology (and its individual facets) and PTSD.
Masculinity and Depression
There is emerging research indicating that pressure to conform to traditional masculinity ideals may contribute to men’s risk of developing depression. In civilian populations, the drive for achievement (i.e., dominance) has been linked with depression in men (Good & Wood, 1995), as has restrictive emotionality (Shepard, 2002). Specifically, it has been theorized that restrictive emotionality leads some men to suppress their emotional responding (Addis, 2008), a behavior associated with negative affect and increased psychological distress (Butler et al., 2003).
Given the cultural feminization of depression (for a review, see Kilmartin, 2005), men who actively avoid femininity may be dissuaded from disclosing their distress to others (O’Brien et al., 2005), thereby impeding their access to sources of social support and mental health services. This dynamic may be exacerbated in the context of military culture (Green et al., 2010), where distress is equated with weakness (Greene-Shortridge et al., 2007), and thus, actively denied. In veteran men specifically, a higher degree of the toughness facet of traditional masculinity ideology has been found to be associated with depression (Jakupcak et al., 2014). In addition, among civilians, the toughness facet of traditional masculinity ideology has been associated with a greater likelihood to take a wait-and-see approach to help-seeking for depression (O’Loughlin et al., 2011), potentially causing symptoms to intensify in the absence of treatment.
Masculinity and Social Support
Social support is considered a potent protective factor during military to civilian transition (Ahern et al., 2015), as veterans who receive sufficient social support from friends, family, or significant others are at lower risk of mental health problems (Pietrzak et al., 2010). However, studies have found that upward of 48% of veterans reported strained relationships with friends and family (Morin, 2011). Many indicated feelings of alienation from loved ones upon returning home (Ahern et al., 2015), as well as a sense of loss with respect to camaraderie and friendships formed during service (Blackburn, 2017).
Endorsement of traditional masculinity ideology may further impede veterans’ access to social support in the civilian world. In the general population, gendered behaviors have been shown to affect social support behaviors, such that femininity is traditionally aligned with seeking and receiving support, particularly emotional support, whereas traditional masculinity is associated with independence, competitiveness, and self-reliance (Reevy & Maslach, 2001). This may explain why men who more strongly endorse aspects of traditional masculinity typically report having significantly smaller social networks (Wohlgemuth & Betz, 1991) and less frequently seek assistance from their social support resources when dealing with challenges (Oliver et al., 1999). In the general population, an inverse relationship between traditional masculinity and perceived social support has been observed (Wester et al., 2007). In particular, the masculinity facet of restrictive emotionality has been shown to contribute to feelings of disconnection or isolation in familial and social relationships (Burns & Mahalik, 2011). In a sample of veteran men, the pressure to conform to traditional masculinity ideals was significantly and negatively associated with social support (Jakupcak et al., 2006).
Masculinity and Alcohol Abuse
It has been suggested that, in the military, alcohol use is an acceptable means of coping with distress, and that the pressure to conform to traditional masculinity ideals may contribute to the continuation of this behavior after leaving the military (Lorber & Garcia, 2010). Specifically, veteran men may opt to use alcohol to cope with transition difficulties, such as traumatic memories, isolation, anger, and psychological/physical injury (Ames et al., 2007), as doing so is more congruent with traditional masculinity ideals (e.g., stoicism) than is disclosing distress to friends, family, or mental health professionals (Lorber & Garcia, 2010). The association with pressures to conform to traditional masculinity ideals and the use of alcohol to cope with distress has been observed in the civilian population (Greene-Shortridge et al., 2007; Isenhart, 1993). Individual facets of traditional masculinity including toughness, avoidance of femininity (McCreary et al., 1999), and emotional control (Liu & Iwamoto, 2007) have been associated with heavy drinking. This may explain why veteran men are at twice the risk of substance use disorder compared with their female counterparts (Seal et al., 2009).
The Present Study
Although the relationship between traditional masculinity ideology and factors associated with difficult military to civilian transition has been recognized, it remains unclear which facets of traditional masculinity most strongly contribute to these risk factors. To better understand the association between traditional masculinity ideology and factors that potentiate difficult veteran transition, we examined the relationship between five facets of traditional masculinity ideology—restrictive emotionality, avoidance of femininity, toughness, dominance, and self-reliance—and four predictors of difficult veteran transition—PTSD, depression, perceived social support, and alcohol-related problems—within a population of veteran men who attended a program for veterans struggling with transition to civilian life. The above-listed facets of traditional masculinity ideology were selected due to their theoretical and empirical association with veteran transition.
Method
Participants and Procedures
Participants were (N = 289) Canadian veteran men who participated in a multimodal group therapy program designed to facilitate transition to civilian life. The program is open to all veterans who identify as struggling with transition to civilian life. Veterans are made aware of this program via word of mouth (e.g., health care providers, peers) and do not pay a fee to participate (all fees, including travel, room, and board, are covered by donations from the Canadian public and Veterans Affairs Canada). At the beginning of the program, participants are made aware of the option to voluntarily participate in the research component of the program. It is made clear to program attendees that their access to the program is not contingent upon their willingness to participate in the research, nor the administration or outcome of the assessments conducted. Those who consented to participate in the research component of the program completed a battery of questionnaires immediately prior to beginning the treatment. The university-affiliated ethics board approved data collection and study procedures and all research participants provided written informed consent.
Veterans ranged in age from 23 to 76 years (M = 46.72, SD = 10.78), 87.2% were Caucasian/White, 65.7% were married or partnered, 21.1% were divorced or separated, 75.8% had children, and 93.4% identified as heterosexual. Branches of service were 63.7% Army, 7.3% Navy, 9.7% Air Force, and 18.0% in “other” branches (e.g., multiple branches). On average, veterans in the current sample served in the armed forces for 18.3 years. Participants were most commonly ranked as corporals (24%) or sergeants (16%). Most frequently, participants served within the regular forces (64%), regular and reserve forces (20%), and reserve forces (12%).
Based on empirically derived clinical cut-off scores for the measures used to assess PTSD (Bovin et al., 2016), depression (Beck et al., 1996), and alcohol dependence (Allen et al., 1997), 75.1% of the participants had probable PTSD, 23.2% had probable moderate depression, 52.6% had probable severe depression, and 49.1% had probable alcohol dependence.
Measures
Male Role Norms Inventory–Short Form (MRNI-SF)
The MRNI-SF is a 21-item self-report measure of traditional masculinity ideology and beliefs pertaining to the importance of adherence to culturally defined standards for male behavior (Levant et al., 2013). Respondents indicate on a 1 (strongly disagree) to 7 (strongly agree) scale how much they believe men should adhere to traditional masculinity norms. A total score is derived by summing the item responses, with higher scores indicating greater endorsement of traditional masculinity ideology. The measure consists of seven subscales designed to assess traditional male role norms (i.e., facets of traditional masculine ideology). In this study, we used the (a) restrictive emotionality, (b) self-reliance through mechanical skills, (c) avoidance of femininity, (d) dominance, and (e) toughness subscales. In the present sample, internal consistency (i.e., coefficient α) for the total score was .93 and coefficient alphas for the subscales ranged from .78 to .93.
Posttraumatic Stress Disorder Check List-5 (PCL-5)
The PCL-5 is a 20-item self-report measure of the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) PTSD symptom severity (Weathers et al., 2013). Each PCL-5 item assesses one of the 20 PTSD symptoms. Respondents indicate on a 0 (not at all) to 4 (extremely) scale how much they have been bothered by each symptom over the past month. A total score is derived by summing item responses, with higher scores indicating greater PTSD symptom severity. Scores 33 or higher are considered clinically significant and are said to indicate probable PTSD (Bovin et al., 2016). In a recent review of self-report DSM-5 PTSD measures, the PCL was identified as a gold-standard measure regarding sensitivity, specificity, and diagnostic accuracy (Spoont et al., 2015). In the present sample, internal consistency (i.e., coefficient α) was .93.
Beck Depression Inventory-II (BDI-II)
The BDI-II is 21-item self-report measure designed to assess depression severity (Beck et al., 1996). Response options range from 0 to 3 and are summed to create a total score with a possible range of 0–63. A score of 0–13 is considered minimal range, 14–19 is mild, 20–28 is moderate, and 29–63 is severe. The BDI-II has been positively correlated with other measures of depression, such as the Hamilton Depression Rating Scale (r = 0.71) and has shown strong test–retest reliability (r = 0.93). Internal consistency in the present sample was α = .91.
Multidimensional Scale of Perceived Social Support (MSPSS)
The MSPSS is a 12-item measure designed to assess perceptions of social support adequacy from three sources: family, friends, and significant others (Zimet et al., 1988). Participants rate the adequacy of social support from the three sources from 0 (very strongly disagree) to 7 (very strongly agree), and responses are summed to create a total score with a possible range of 0–84. Higher scores represent a greater degree of perceived social support. The MSPSS has shown good reliability, factor validity, and construct validity. In the current sample, internal consistency was α = .91.
Alcohol Use Disorders Identification Test (AUDIT)
The AUDIT is a 10-item self-report questionnaire designed to screen for hazardous and harmful alcohol consumption (Saunders et al., 1993). The AUDIT assesses three domains of alcohol use: amount/frequency of drinking (i.e., alcohol consumption), alcohol dependence, and alcohol-related problems. In this study, we used the alcohol-related problems subscale because we were interested specifically in the negative effects of drinking rather than general alcohol use behaviors. Responses to each item range from 0 to 4, with a possible total alcohol-related problems subscale score of 0–16. A score of 4 or more on the “dependence” questions suggests the possibility of alcohol dependence. The AUDIT has shown satisfactory internal consistency and test–retest reliability (Bergman & Källmén, 2002). In the current sample, the internal consistency on the alcohol-related problems subscale was α = .67.
Data Analytic Strategy
To examine the relative contribution of facets of traditional masculinity ideology endorsement (i.e., restrictive emotionality, avoidance of femininity, self-reliance, toughness, and dominance) to predictors of difficult military to civilian transition (i.e., PTSD, depression, social support, and alcohol-related problems), a series of linear regression analyses were conducted. First, we ran four separate linear regression analyses, each predicting a factor associated with difficult veteran transition outcome. Predictor variables included in each model were those facets of traditional masculinity that had significant bivariate correlations with the outcome variable in the model. Second, consistent with methodological recommendations (Bursac et al., 2008; Tabachnick & Fidell, 2013), we used backward elimination and forward selection of predictor variables to create more parsimonious models. In backward elimination, all of the predictor variables were initially included. Then, according to the results of a Wald test, the nonsignificant variable with the least significant effect was removed from the model. This process was repeated until all predictor variables in the model had significant effects. In forward selection, we began with no predictor variables in the model. Predictor variables were then added, one at a time, and tested for fit using a chi-square statistic. Variables were added if inclusion significantly improved the model fit. This process was repeated until adding additional predictor variables did not improve the model fit. Finally, we conducted a manual variable selection in which we examined the effect sizes of variables and manually removed them from models. Results of the variable selection techniques were compared ensuring the results from the three processes converged. All statistical analyses were conducted using IBM SPSS Statistics version 25.
Results
Preliminary Analyses
Data from 289 participants were screened for missing responses. When minimal data were missing for an individual’s measure (i.e., less than 20% of items), item mean replacement was used. This approach has been shown to provide a strong representation of original data when both the number of items missing and the number of respondents with missing data were 20% or less (Downey & King, 1998). For cases that had significant missing data (e.g., >50%), the measure for the individual was eliminated from analyses. This resulted in slightly different sample sizes for each measure (n = 289 for the MRNI; n = 289 for the PCL-5; n = 260 for the BDI; n = 269 for the MSPSS; and n = 239 for the AUDIT). We then examined skewness and kurtosis via visual inspection of univariate histograms and skewness and kurtosis statistics. Moderate non-normality was observed on the PCL-5, the alcohol-related problems subscale of the AUDIT, and the self-reliance and dominance subscales of the MRNI. Following the recommendations of Tabachnick and Fidell (2013), we used square root transformations and conducted all analyses with transformed and untransformed data. There were minimal differences whether transformed or untransformed data were used; thus, we used untransformed data for ease of interpretation and comparison with other studies. On account of using five subscales from a single measure, a certain degree of multicollinearity was expected. Nonetheless, collinearity diagnostics were assessed. The variance inflation factor ranged from 1.66 to 1.95, well within the range of acceptable collinearity (i.e., 1–10; Yoo et al., 2014). Bivariate correlations and descriptive statistics for the primary study variables are presented in Table 1.
Bivariate Correlations and Descriptive Statistics for Primary Study Variables.
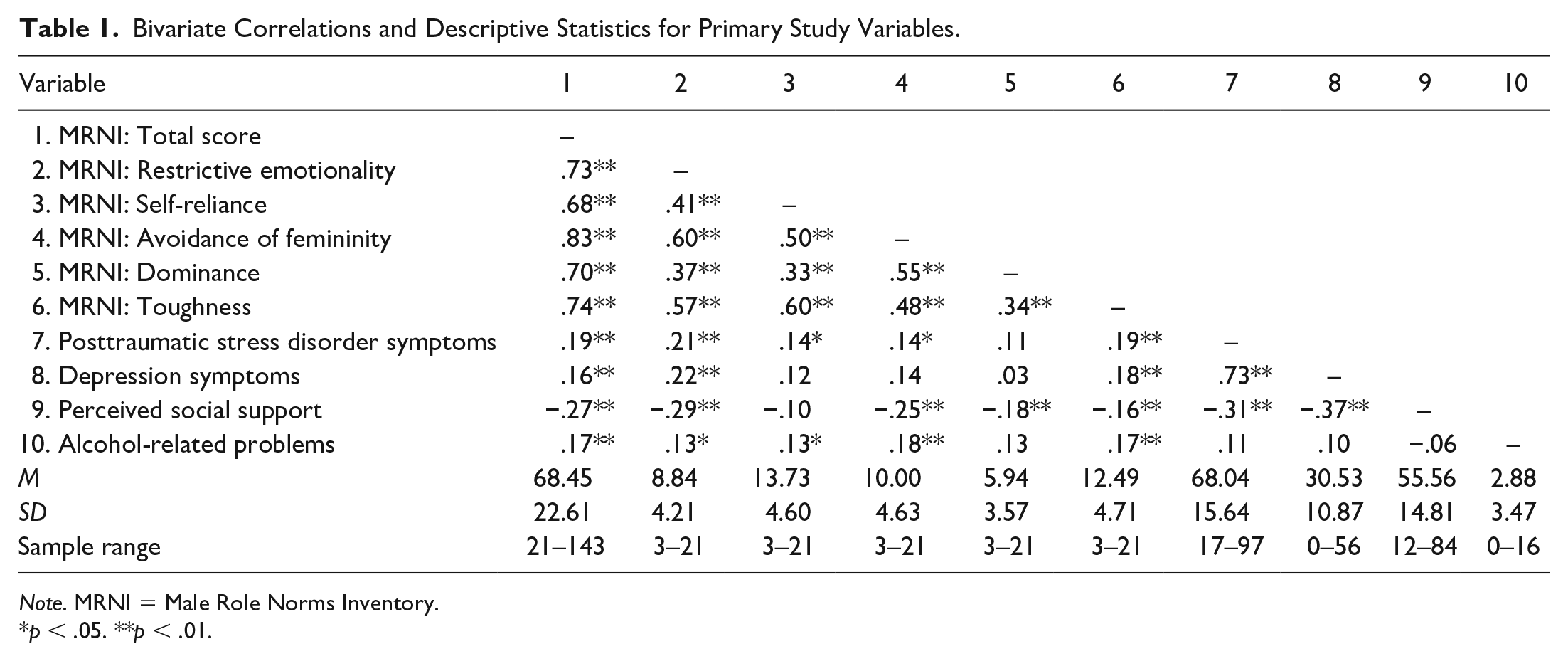
Note. MRNI = Male Role Norms Inventory.
p < .05. **p < .01.
Masculinity Ideology and PTSD
The facets of masculinity ideology that were significantly correlated with PTSD—restrictive emotionality, self-reliance, avoidance of femininity, and toughness—were entered into a linear regression analysis with PTSD as the criterion variable. While accounting for self-reliance, avoidance of femininity, and toughness, restrictive emotionality emerged as the only significant predictor of PTSD (see Table 2).
Masculinity Facets in Relation to Transition Outcomes.
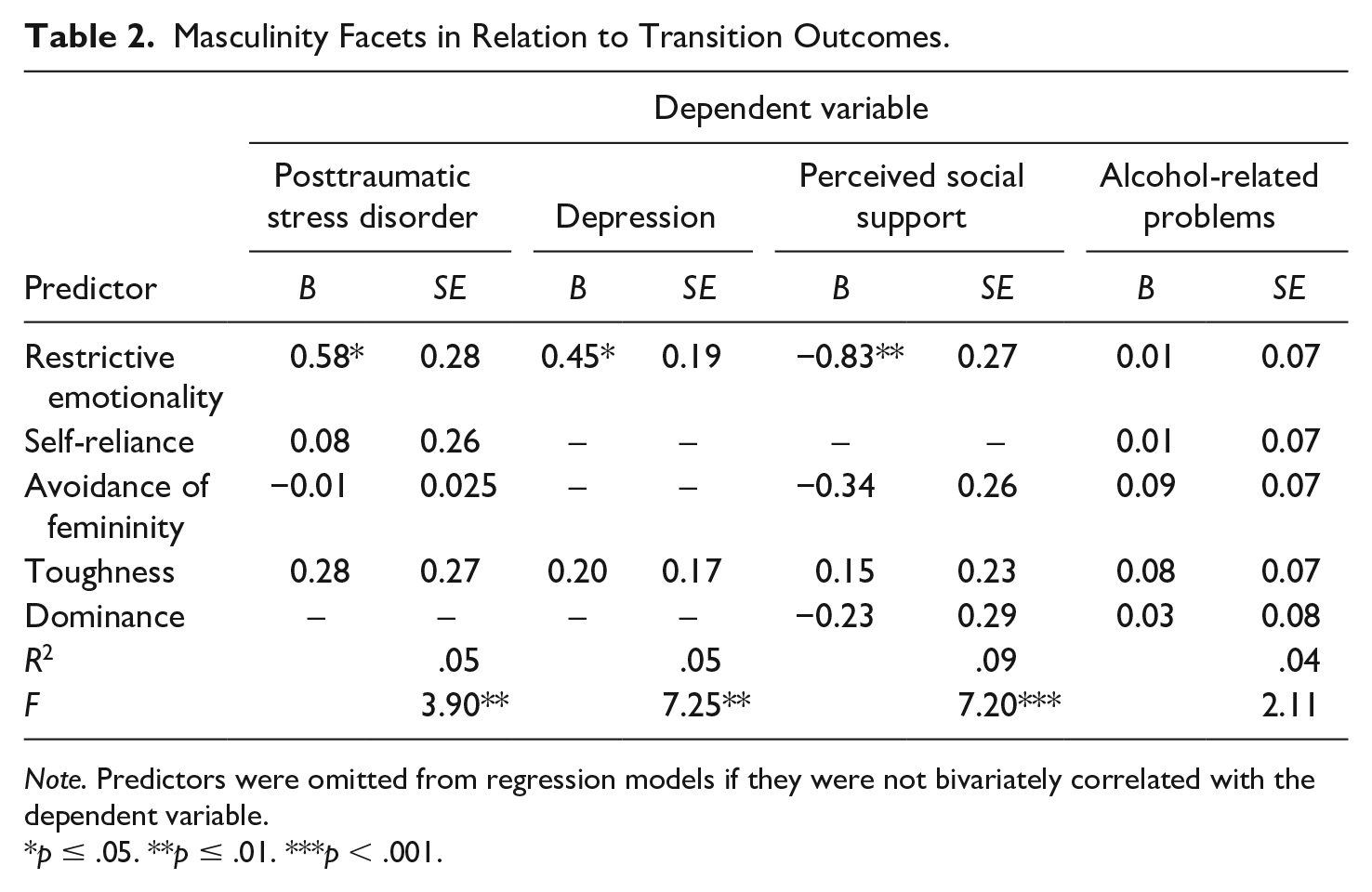
Note. Predictors were omitted from regression models if they were not bivariately correlated with the dependent variable.
p ≤ .05. **p ≤ .01. ***p < .001.
Next, we used backward elimination and forward selection to confirm that restrictive emotionality was the only significant predictor of PTSD. Both methods identified restrictive emotionality as the only significant predictor of PTSD; thus, it was the only predictor variable included in the second model. Restrictive emotionality was significantly associated with PTSD and accounted for 5% of the variance in PTSD scores (see Table 3).
Masculinity Facets in Relation to Transition Outcomes (Parsimonious Model).

Note. Only variables significant in the regression models were included.
p < .05. **p < .01. ***p < .001.
Masculinity Ideology and Depression
The facets of masculinity ideology that were significantly correlated with depression—restrictive emotionality and toughness—were entered into a linear regression equation with depression as the criterion variable. Results indicated that, while accounting for toughness, restrictive emotionality was the only significant predictor of depression (see Table 2).
Next, we used backward elimination and forward selection to confirm that restrictive emotionality was the only significant predictor of depression. Both methods identified restrictive emotionality as the only significant predictor of depression; thus, it was the only predictor variable included in the second model analyzed. Restrictive emotionality was significantly associated with depression and accounted for 5% of the variance in depression scores (see Table 3).
Masculinity Ideology and Perceived Social Support
The facets of masculinity ideology that were significantly correlated with perceived social support—restrictive emotionality, avoidance of femininity, dominance, and toughness—were entered into a linear regression analysis with perceived social support as the criterion variable. Results indicated that, while accounting for avoidance of femininity, dominance, and toughness, restrictive emotionality was the only significantly predictor of perceived social support (see Table 2).
Next, we used backward elimination and forward selection to confirm that restrictive emotionality was the only significant predictor of perceived social support. Both methods identified restrictive emotionality as the only significant predictor of perceived social support; thus, it was the only predictor variable included in the second model. Restrictive emotionality was significantly associated with perceived social support and accounted for 9% of the variance in perceived social support scores (see Table 3).
Masculinity Ideology and Alcohol-Related Problems
The facets of masculinity ideology that were significantly correlated with alcohol-related problems—restrictive emotionality, self-reliance, avoidance of femininity, and toughness—were entered into a linear regression analysis with alcohol-related problems as the criterion variable. Results indicated that, with all variables included in the model, none significantly predicted alcohol-related problems (see Table 2).
Next, we used backward elimination and forward selection to confirm that no facets of traditional masculinity significantly predicted alcohol-related problems. Both methods identified that avoidance of femininity was a significant predictor of alcohol-related problems; thus, we included it as a predictor variable in the second model. Avoidance of femininity was significantly associated with alcohol-related problems and accounted for 3% of the variance in alcohol-related problems scores (see Table 3).
Discussion
In this study, we evaluated the association between facets of traditional masculinity ideology and four predictors of difficult military to civilian transition—PTSD, depression, lack of perceived social support, and alcohol-related problems. Overall, findings are consistent with previous literature showing that continued endorsement of traditional masculinity ideology during civilian transition increases the risk of psychosocial difficulties during veteran transition (e.g., Cox & O’Loughlin, 2017; Jakupcak et al., 2014; Lorber & Garcia, 2010).
Examination of the relationship between individual facets of masculinity and indicators of difficult military to civilian transition revealed several significant correlations. However, when entered into linear regression models, wherein the effects of all predictor variables were taken into account in relation to one another, fewer facets of traditional masculinity appeared to significantly predict the outcome variables of interest. Restrictive emotionality was consistently the most significant predictor of the transition outcome variables examined, while avoidance of femininity (except in the case of alcohol-related problems), self-reliance, dominance, and toughness did not appear to significantly predict the outcome variables.
Restrictive Emotionality and Transition
With respect to PTSD, the significant contribution of restrictive emotionality to higher degrees of symptomatology is consistent with research and theory indicating that when intense affective states associated with trauma memories are actively avoided, processing of trauma-related emotions, beliefs, and memories—the cornerstone of gold-standard PTSD treatments such as exposure therapy (Rauch et al., 2012)—is unlikely to occur (Monson et al., 2004). As a result, symptoms may be exacerbated, or treatment efforts may be impeded.
We also observed a significant association between restrictive emotionality and depression in veteran men. This finding aligns with research indicating that suppression of affective states results in intensified negative affect and increased distress (i.e., an exacerbation of primary symptoms of depression; Butler et al., 2003). It has long been argued that men are under-represented in prevalence statistics concerning depression diagnosis due to their hesitancy toward seeking help (Kilmartin, 2005) or denying depression symptoms given their association with femininity (O’Brien et al., 2005). However, results of this study add another layer to the picture—that restrictive emotionality may account, at least in part, for a different presentation of depression in those who ascribe to traditional norms of masculinity. Whereas typical presentations of depression are characterized by an expression of sadness, in the presence of restrictive emotionality wherein negative affect is avoided or not identified, the experience of sadness may not be readily identifiable or reported. It may be that depression manifests in somatic symptoms, a phenomenon that has been linked to difficulty identifying and communicating emotional distress (e.g., Sayar et al., 2003). This may explain why somatic symptoms are observed more frequently in men with depression (Pollack, 1998).
With respect to perceived social support, the observation that restrictive emotionality contributed significantly to veteran men’s perceived lack of support from friends, family, or a significant other is consistent with previous research indicating that men who endorse traditional masculinity ideology have less available and smaller social networks (Wohlgemuth & Betz, 1991). Specifically, this result supports research indicating that restrictive emotionality impairs social interaction (e.g., Jansz, 2000) and that emotional sharing is an important element of building and maintaining close relationships (Derlega et al., 2008).
Taken together, and in light of research showing that military transition is significantly and negatively affected by PTSD, depression, and lack of social support (see Rose et al., 2018, for a review), the above results indicate that restrictive emotionality may be the facet of traditional masculinity ideology with the most detrimental effect on veteran men’s military to civilian transition. Put differently, suppression or lack of sharing affective states appears to put veteran men at risk of a difficult military transition trajectory and impaired psychosocial functioning.
Toughness, Avoidance of Femininity, and Self-Reliance
Although there is evidence in the extant literature that toughness, avoidance, and self-reliance consistently and significantly contribute to PTSD, depression, lack of social support, and alcohol dependence, we found little contribution, if any, of these masculinity facets to the outcome variables examined. An exception was in the case of alcohol-related problems for which avoidance of femininity was observed to be the only significant contributor (when accounting for the other facets of masculinity). One explanation for this finding is that men who more strongly endorse the “avoidance of femininity” facet of traditional masculinity were more likely to perceive disclosure of problems to others as a feminine trait and were fearful of their manliness being called into question if they shared their struggles. Subsequently, alcohol may be used as a maladaptive way to cope with their problems. Drawing from research showing an association between heavy alcohol consumption with unit cohesion among male soldiers (Du Preez et al., 2011), an alternative explanation for this finding may be that alcohol is utilized as a means for members of the armed forces to openly discuss their emotional experiences in a (military) culturally acceptable way.
With respect to the lack of observed relationship between self-reliance and perceived social support, one explanation is that masculinity is not in fact negatively associated with seeking support per se, so much as avoidance of specific types of support-seeking. For example, those who endorse traditional masculinity may avoid types of help that have been culturally feminized, such as disclosing emotions to friends, family, or a mental health professional, but are willing to seek more tangible forms of support (Reevy & Maslach, 2001). This may explain why restrictive emotionality appeared to contribute to lack of social support over and above self-reliance. Alternatively, it is possible that the self-reliance facet of masculinity was less apparent in the current sample, given recruitment was conducted through a veteran transition program, and thus consists of a sample of veteran men who agreed to seek help. This characteristic may not be representative of the majority of veteran men who strongly endorse traditional masculinity ideology.
Limitations
Limitations of this study include its cross-sectional design, which prevented us from examining the effect of traditional masculinity ideology on veteran transition longitudinally. In addition, our sample consisted predominantly of Caucasian, Canadian veteran men, and thus, was fairly homogeneous. It is important to recognize that the majority of the literature cited regarding masculinity in the military was written in the context of American military culture. Although we do not intend to imply American military values and culture are synonymous with that of the Canadian military, both organizations have been characterized as a hypermasculine (see Taber, 2018, for a review). In addition, all measures used were self-report measures which are prone to response bias. Moreover, as participants for this study were recruited from a veteran’s transition program, the sample may not be representative of a more typical presentation of veteran men who, due to their endorsement of traditional masculinity ideology, avoid seeking help (Lorber & Garcia, 2010).
Theoretical and Practical Implications
The results of this study show support for the military transition theory (Castro & Kintzle, 2014), such that traditional masculinity ideology, which was conceptualized as a personal and (military) cultural factor, proved to have an effect on outcomes associated with transition, specifically mental health and social engagement. Although the potential indirect effect of masculinity ideology on transition outcomes through coping strategies (or lack thereof) were not assessed in this study, it may be argued that some of the variables evaluated as outcome variables here (e.g., social support and alcohol use) could instead be conceived of as coping strategies. Future research would benefit from examining these variables as intermediary, or mediating, factors in the relationship between masculinity and veteran transition.
With respect to clinical implications, results of this study indicate it is paramount to address restrictive emotionality in programming aimed at preparing veteran men for, or assisting them with, transition to civilian life. Given the perceived association of emotional disclosure and emotional processing with femininity, mitigating the tendency to suppress emotions, restrict emotional disclosure, or detach emotionally from distressing situations, may prove difficult with veteran men who ascribe to traditional masculinity ideology. Clinicians may look to treatments recommended to address alexithymia, a construct similar to restrictive emotionality and also associated with masculinity (Levant et al., 2009). These treatments focus on introducing the person to the world of emotional experience, helping him develop an experiential language that allows for a more enriched narrative of one’s internal life (Ogrodniczuk et al., 2018). Others have suggested that the use of masculinity-congruent language such as “Real Men; Real Depression; “It takes courage to ask for help” (Rochlen et al., 2005) in promotional materials for programs designed for men with mental health difficulties may counter the cultural feminization and stigmatization of men seeking therapy. Finally, a recent qualitative study suggested that, in the context of group therapy, a shared endorsement of traditional masculinity ideology may operate to increase camaraderie among group members and result in their willingness to emotionally disclose to one another (Caddick et al., 2015). Thus, when it comes to mitigating the deleterious effects of restrictive emotionality on veteran men’s mental well-being, it may be that group therapy, as opposed to one-on-one therapy, is preferential for treatment of conditions that benefit from emotional processing, such as PTSD (Monson et al., 2009).
Future Directions
Taking into consideration that all military recruits, regardless of gender, undergo a “secondary socialization” (Arkin & Dobrofsky, 1978, p. 159) into military culture, it is possible that a difficult military to civilian transition is also potentiated among veteran women as a result of traditional masculinity ideology endorsement. This is an important consideration for future research concerning the impact of traditional masculinity of veteran health and well-being.
Footnotes
Acknowledgements
We wish to thank Leah Baugh, Myfanwy Bakker, and Katie McCloskey for assistance in data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Social Sciences and Humanities Research Council and the Veterans Transition Network.