
Abstract
The call for family-centered therapeutic services, especially for families of young children, has come from governmental organizations, professional associations, practitioners, and families. Play therapists and family therapists are prime candidates to provide such services, but professional research and literature suggest that practitioners within these fields tend to exclude members of the family system. This had led some to propose filial therapy, an outgrowth of child-centered play therapy, as a means of meaningfully integrating parents and children in treatment. However, play therapists may have difficultly conceptualizing from a family systems lens, while family therapists may struggle to see the theoretical compatibility of filial therapy with their systemic views. This article demonstrates the conceptual overlap between filial therapy and the major family therapy models with the goal of encouraging play therapists and family therapists to answer the call to provide family-centered services.
The Call for Family-Based Services for Families With Young Children
Over recent years, there has been a resounding call for those in the helping professions to provide family-based services for families with young children. This call has come from governmental organizations, such as the U.S. Public Health Service (2000), who published a national action agenda underscoring the importance of researching, developing, and utilizing evidence-based, family-centered treatment in addressing the mental health of children. A similar call for involving families in therapeutic services is evident in the ethical codes of major professional associations (American Association for Marriage and Family Therapy [AAMFT], 2001, 6.8; American Counseling Association [ACA], 2005, A.1.d.; American Psychological Association [APA], 2010, 10.02; National Association of Social Workers [NASW], 2008, preamble) and in the APA’s (2005) policy statement on evidence-based practice.
Across helping professions, practitioners have emphasized the need for and the importance of family-centered assessment and treatment (Perry, 2007; Pritchett et al., 2010; Reeves & Anthony, 2009; Reinherz, Giaconia, Paradis, Novero, & Kerrigan, 2008; Tomlin & Viehweg, 2003; Wallander, Dekker, & Koot, 2006). Research buttresses the importance of family-centered treatment in that caregiver involvement in the mental health treatment of children is associated with better outcomes (Bratton, Ray, Rhine, & Jones, 2005; Richards, Bowers, Lazicki, Krall, & Jacobs, 2008).
Finally, families themselves seem to be actively seeking such services. Research conducted by Sax (2007) reveals that parents of children with mental health concerns desire family-centered systems of care that provide effective helping strategies, entail meaningful parental involvement, and enhance support among parents. However, as Perry (2007) has noted, there is a lack of systematic treatment methods that comprehensively address the diverse treatment needs of families with young children. The call from organizations, professionals, and families regarding the need for family-based services is clear, but an answer seems to be lacking.
A Problem in Common: Either/Or
Play therapists and family therapists in particular appear to be prime candidates for providing such services given that they have frequent contact with families of young children. Research indicates that play therapists often encounter family issues (Kranz, Kottman, & Lund, 1998; Ryan, Gomory, & Lacasse, 2002; Tsai & Ray, 2011), and family therapists often encounter families who are experiencing issues with their young children (Doherty & Simmons, 1996; Hines, 1996). In addition, surveys of play therapists (Haslam & Harris, 2011; Phillips & Landreth, 1998) and family therapists (Sori & Sprenkle, 2004) indicate that practitioners within these fields believe in the importance of providing services that meaningfully involve family members.
Integration of Family Therapy Approaches and Child–Parent Relationship Therapy (CPRT)
However, play therapists and family therapists have typically concentrated their efforts on either the child or parental subsystems, leaving untapped potential that is available within the family system as a whole. Numerous family therapists have identified and spoken to the lack of inclusion of children in family therapy (Botkin, 2000; Green, 1994; Johnson & Thomas, 1999; Korner & Brown, 1990; Miller & McLeod, 2001; Raimondi & Walters, 2004; Sori & Sprenkle, 2004; Zilbach, 1986, 1989). This issue within family therapy is surprising, given that many of the most influential family therapists, such as Ackerman (1970), Satir (1983), Whitaker (Keith & Whitaker, 1981), Minuchin (1974), and Haley (Montalvo & Haley 1973), advocated for the inclusion of children in their approaches. Play therapists have noted similar issues regarding the lack of practitioners working conjointly with family members (Gil, 1994; Haslam & Harris, 2011).
A Solution in Common: Both/And
Family therapy and play therapy share a problem in common, and where one is strong in terms of involving certain members of the family the other is weak. This had led several authors to propose that filial therapy, with its direct involvement of caregivers and children in treatment, is a solution that family therapists and play therapists can have in common in order to impact the family system (Gil, 1994; Guerney & Guerney, 1987; Hutton, 2004; Johnson, 1995; Johnson, Bruhn, Winek, Krepps, & Wiley, 1999; Kellam, 2001). Filial therapy, first introduced by Bernard Guerney (1964), is an approach in which parents of young children are trained to be “therapeutic agents” through learning how to apply basic child-centered play therapy skills in conducting play sessions with their children (p. 304).
Despite filial therapy being an outgrowth of child-centered play therapy (Axline, 1947; Landreth, 2002) and person-centered theory, proponents have provided theoretical arguments that explain how filial therapy satisfies the unique dimensions of both play therapy and family therapy (Hutton, 2004; Johnson, 1995; Johnson et al., 1999; Kellam, 2001). For instance, Johnson et al. (1999) provided six different arguments for filial therapy that coincide with traditional family therapy principles: 1) Filial therapy requires family involvement; 2) Filial therapy takes the focus off the child as the IP [identified patient]; 3) Filial therapy often leads to the parents’ seeing their role in the problem; 4) Filial therapy enhances parental leadership, strengthening the generational boundary between parents and children; 5) Filial therapy increases differentiated relating and reduces polarizations between parents and children; 6) Filial therapy highlights unhelpful systemic sequences. (pp. 172–173)
As illustrated through the theoretical arguments of its proponents and its growing research base, filial therapy appears to provide a treatment context that brings about change within children and parents, between children and parents, and between the relationships of others in the family system. The rationale within these conceptual arguments and the research should encourage play therapists and family therapists to consider how filial therapy might promote the best interests of the families with whom they work.
Two relevant issues, however, come to the forefront that may impede the ability for play therapists and family therapists to integrate a filial therapy approach into their therapeutic repertoire. For play therapists primarily trained to conceptualize within a framework of the individual, the challenge in realizing the full potential of filial therapy may be limited by their ability to find a means for framing the systemic implications of the approach. Without a systemic framework, play therapists may have greater difficulty in conceptualizing and working with families and their unique dynamics.
For family therapists primarily trained to conceptualize within a framework of the system, the challenge in realizing the full potential of filial therapy may be limited by their ability to see the compatibility of the components of an approach that is still largely explained through the language of child-centered play therapy. Without an understanding of the conceptual compatibility between family therapy and the components of filial therapy, family therapists may struggle to see how a consistent integration is possible.
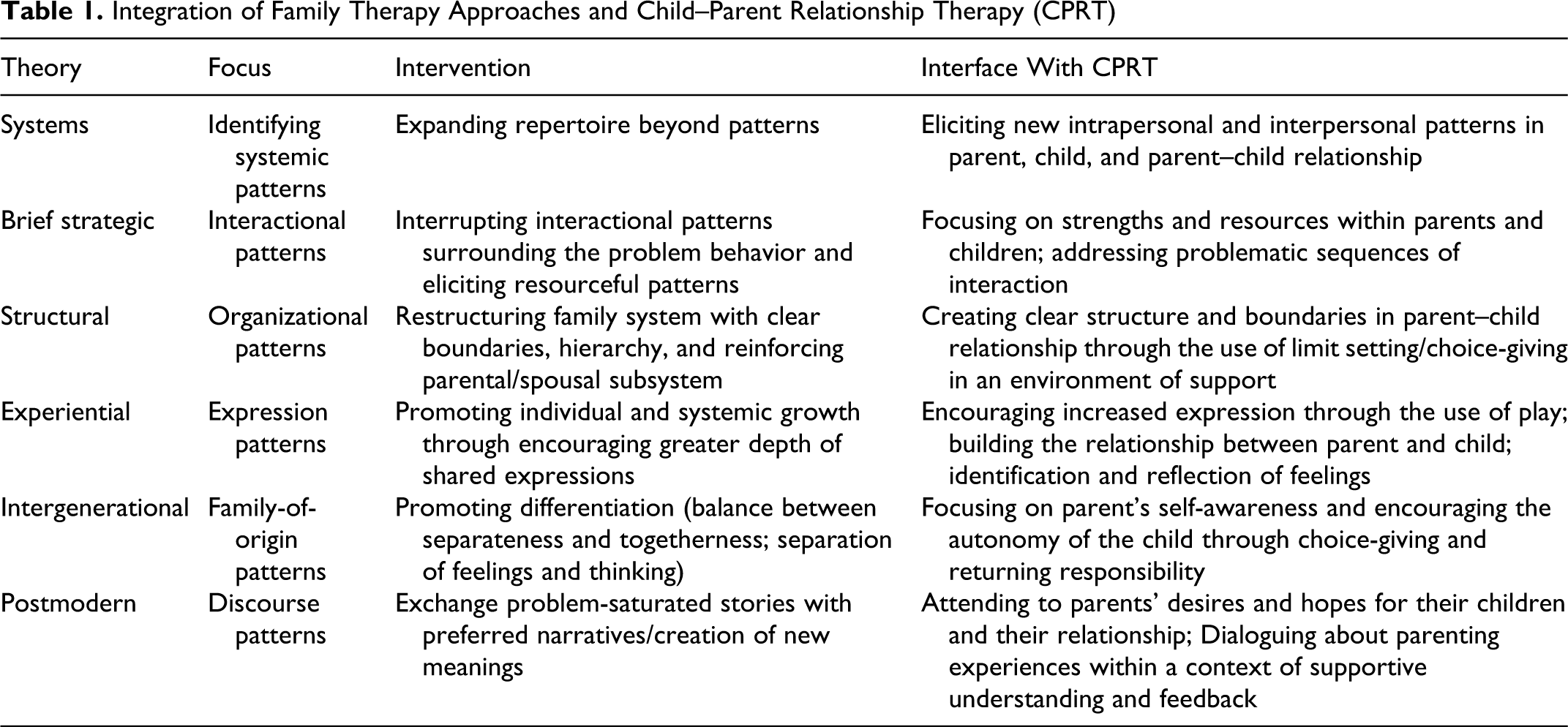
In light of the potential epistemological issues that exist in the utilization of filial therapy for play therapists and family therapists alike, I present a popular model of filial therapy known as child–parent relationship therapy (CPRT; Landreth & Bratton, 2006) and discuss its components within the lens of several categories of approaches to family therapy: brief-strategic, structural, experiential, integernerational, and postmodern. I will also incorporate research from the field of filial therapy that are suggestive of changes in the family system and that appear to align with the goals of these family therapy approaches. Although this is by no means an exhaustive coverage of either CPRT or family therapy, the following presentation provides play therapists with the opportunity to consider filial therapy through family systems frameworks. In addition, family therapists have the opportunity to consider how the components of filial therapy might merge with familiar concepts from the major approaches to family therapy.
CPRT Within the Lens of Family Therapy
CPRT is a popular 10-session filial therapy model presented by Landreth and Bratton (2006). Landreth and Bratton provided the following definition of their approach: Filial therapy is defined as a unique approach used by professionals trained in play therapy to train parents to be therapeutic agents with their own children through a format of didactic instruction, demonstration play sessions, required at-home laboratory play sessions, and supervision in a supportive atmosphere. Parents are taught basic child-centered play therapy principles and skills including reflective listening, recognizing and responding to children’s feelings, therapeutic limit setting, building children’s self-esteem, and structuring required weekly play sessions with their child using a special kit of selected toys. Parents learn how to create a nonjudgmental, understanding, and accepting environment that enhances the parent-child relationship, thus facilitating personal growth and change for the child and parent. (p. 11)
CPRT and Brief-Strategic Family Therapy
The first category of family therapy approaches, brief-strategic family therapies, are ones that share in common an emphasis on actively interrupting the interactional patterns surrounding the family’s problems in attempts to (1) help get them unstuck and (2) to allow the family to utilize its own resourcefulness in addressing its concerns. The family therapy approaches that share these principles are Mental Research Institute (MRI) brief therapy (Fisch, Weakland, & Segal, 1982; Watzlawick, Weakland, & Fisch, 1974), Milan systemic family therapy (Boscolo, Cechin, Hoffman, & Penn, 1987), strategic family therapy (Haley, 1976), and solution-focused therapy (de Shazer, 1985, 1988). Although the approaches utilize different theoretical language and techniques, they have similar values in seeking to initiate small, direct changes within interactive sequences. Whereas the MRI, Milan, and strategic approaches tend to focus on the problem-maintaining sequences of interaction, the solution-focused approach focuses on resourceful sequences of interaction. Put simply, these approaches want to help families “do something different” when they become entrenched in unhelpful patterns of relating and exchange these modes of relating for “doing what works” (de Shazer & Berg, 1995, pp. 250–251).
Filial therapy models, such as CPRT, also share a trust in the resourcefulness of the family and the importance of finding ways to interrupt problematic interactions. By its very nature, filial therapy affirms that “parents have within them the psychological and emotional wherewithal to make a major contribution to the positive development of their children” (Guerney, 2000, p. 7). Guerney (2000) identified that a major task of filial therapy is “to identify and utilize strengths and build on them in therapy” (p. 12). Through CPRT, therapists consistently encourage parents to “focus on the donut, not the hole” (Landreth & Bratton, 2006, p. 131), to see and affirm the strengths in their children, to have a future focus, and to see their own growth through positive supervisory feedback regarding their play sessions. All these contribute to cultivating resourceful interactions within the family. As in the brief-strategic family therapy approaches, there is a similar emphasis in CPRT on initiating small changes within the family’s interactions. For instance, parents only do one weekly 30-min play session, limiting the utilization of the skills that they learn for these times in order for parents to experience success in applying new skills (Landreth & Bratton, 2006, p. 26). In addition, parents have short, experiential homework exercises where they practice the specific skill of CPRT for that week. Experiencing these incremental positive shifts in behavior within the context of the parent–child relationship facilitates resourceful sequences of interaction.
Despite its heavy emphasis on building upon the strengths of the parent–child relationship, CPRT also provides the opportunity to focus on the problematic patterns within the family. For instance, in session 9, time is set aside for the parents and therapists to address any problematic interactions that they are still experiencing with their children (Landreth & Bratton, 2006). This allows parents and therapists to determine how they may generalize the skills they learned in CPRT to interrupt these problematic patterns. By seeking to interrupt these problematic interactional patterns and eliciting resourceful interactional patterns, CPRT mirrors the basic thrust of brief-strategic family therapy.
One extensive qualitative research study on filial therapy by Winek et al. (2003) offers support for this notion that filial therapy highlights problem-maintaining sequences of interaction between parents and children and generates resourceful sequences of interaction. They identified behaviors on the part of children and parents that both facilitated and inhibited progress. For example, for one of the inhibitive behaviors, they identified that parent’s “directiveness,” such as “making controlling statements,” detracted from play sessions as did children’s “being oppositional” (Winek et al., 2003, p. 99). Taken together, it is probable that these inhibitive behaviors interact with one another, so that as the parent is more directive, the child is more oppositional, and as the child is more oppositional, the parent is more directive. For one of the facilitative behaviors, they identified “encouraging” in parents and “following rules” in children as behavioral categories that contributed to positive play sessions. It is reasonable to assume that these problematic and resourceful interactions within play sessions reflect possible interactions that occur outside of play sessions. This research highlights how filial therapy may provide a means to assess and intervene within these interactive sequences.
CPRT and Structural Family Therapy
Another major family therapy approach, structural family therapy (Minuchin, 1974; Minuchin & Fishman, 1981), emphasizes the role of the organization of the family. Within this approach, healthy family systems that promote the growth of its members have the following elements: a generational hierarchy, a coalition between parents, and clear boundaries (Gehart & Tuttle, 2003, p. 36). The parental unit, as a unit of significant influence in the family, should “provide leadership for growth and development of the child” (Hanna, 2007, p. 10). In addition, healthy families have flexible boundaries between its members that are neither too diffuse, fostering enmeshment, nor too rigid, creating distance. Thus, a major task of structural family therapy is to use a family’s interactions to assess their structure and to “strengthen and clarify structure and boundaries” as needed (Gehart & Tuttle, 2003, p. 27).
Because of its roots in child-centered play therapy, filial therapy has to challenge misconceptions that it proposes that the family’s world should revolve around the child (Kellam, 2001). What may come as a surprise to many is that filial therapy actually incorporates “a heavy component of behavioral approaches” that encourage parents to assume the role of providing structure for their children (Guerney, 2000, p. 10). For instance, in CPRT, parents learn to utilize choice-giving with children. In this technique, parents are encouraged to present choices to their children that provide opportunities for the child to make decisions while ensuring that parents still maintain control of what constitutes acceptable choices. In addition to choice-giving, parents learn the skill of limit-setting. With limit-setting, parents learn how to respond to problem behavior by acknowledging the child’s wishes, communicating clear and consistent limits, and targeting alternatives for the child to choose. During play sessions, parents “let the child lead” (Landreth & Bratton, 2006, p. 203) while maintaining basic control of the structure of sessions. Through weekly discussions and videotaped play sessions, CPRT provides therapists with the opportunity to see and use the interactions between parents and children as a means to assess their family structure and encourage parents to utilize their skills to build relationships with their children that promote a more optimal family structure (Kellam, 2001). These structuring skills allow for the developmentally appropriate participation of children while maintaining parental hierarchy. In addition, these practices reinforce clear structure and boundaries in the family system, which contribute to an environment of consistency and safety for family members. Clear structure helps families avoid the lenient interactions characteristic of family boundaries that are too diffuse and the authoritarian interactions characteristic of family boundaries that are too rigid.
In her qualitative study of the systemic changes of using the CPRT approach, Wickstrom (2009) identified several changes reported by parents that are suggestive of adjustments in family organization and structure. For instance, parents in this study indicated experiencing the following gains: improved marital relationships and coparenting, increased sense of shared power, increased awareness of their level of influence in their relationships with their children, and creating developmentally appropriate equality with children. Bavin-Hoffman et al. (1996) also found in their qualitative study of 20 married couples who participated in CPRT that participants reported improved partner communication and increased unity within the marriage. In an ethnographic study of the process and effects of CPRT, Lahti (1992) too reported the finding of improved marital relationships and increased communication. Winek et al. (2003) found that some of the behaviors of parents that facilitated play sessions were when they set limits, redirected children toward appropriate behaviors, and joined in the fantasy play led by their children. Parents tended to inhibit play sessions when they were too directive, threatening, or did not enforce limits. These findings demonstrate how filial therapy can assist families in establishing appropriate parent–child hierarchies, foster the development of parental coalitions, and facilitate clear boundaries that allow for developmentally appropriate interaction between parents and children.
CPRT and Experiential Family Therapy
The experiential family therapy approaches of Carl Whitaker and Virginia Satir both share an emphasis on facilitating growth within the family through creating shared experiences of expression (Gehart & Tuttle, 2003; Satir, 1983; Whitaker & Bumberry, 1988). Experiential family therapists use themselves to model and facilitate this depth of communication between family members (Gehart & Tuttle, 2003; Hanna, 2007; Satir, 1983; Whitaker & Bumberry, 1988). Hanna (2007) stated, “Experiential family therapists focus on subjective needs of the individual in the family and facilitate family interactions that address the individuality and self-esteem of each member” (p. 17). There is a strong emphasis within experiential family therapy on individuation within a context of belonging in the family (Whitaker & Bumberry, 1988). Whitaker and Bumberry (1988) argued, “the central issue is to focus on expanding the significance of experience and broadening the horizons of life . . . If we can aid in the expansion of the symbolic world of the families we see, they can live richer lives” (p. 75). In order to facilitate this symbolic expression and understanding within families, Keith and Whitaker (1981) actually contended for the inclusion of play within family therapy.
In identifying the features of the CPRT approach, Landreth and Bratton (2006) highlighted the central importance that the use of play has in creating a means for symbolic expression between parents and children. Through play, the authors noted that families have a “communication medium” that provides an opportunity for the expression of “feelings, needs, wants, wishes, fantasies, experiences, and thoughts” (p. 16). Learning and utilizing the foundational CPRT skills of identifying feelings, reflective responding, and esteem building only further enhances the depth and breadth of expression between parents and children. Parents learn to “be with” their children, implicitly communicating the messages “I am here,” “I hear you,” “I understand,” and “I care” (Landreth & Bratton, 2006, p. 84). The group process component of CPRT allows parents to also have the opportunity to express themselves within a supportive context created through the modeling of the therapists. CPRT’s emphasis on building the relationship between the parent and the child ensures that there is a sense of belonging that is pivotal for individuation to occur.
The research appears to support the notion that CPRT leads to new and beneficial expressions between parents and children. For instance, multiple research studies involving CPRT have demonstrated that filial therapy leads to increases in parents’ acceptance of their children (Bratton & Landreth, 1995; Chau & Landreth, 1997; Costas & Landreth, 1999; Harris & Landreth, 1997; Kale & Landreth, 1999; Landreth & Lobaugh, 1998; Lee & Landreth, 2003; Tew, Landreth, Joiner, & Solt, 2002; Yuen, Landreth, & Baggerly, 2002). In addition, multiple studies have demonstrated that participation in CPRT increases parents’ empathic behaviors toward their children (Bratton & Landreth, 1995; Carnes-Holt, 2010; Chau & Landreth, 1997; Costas & Landreth, 1999; Ferrell, 2004; Glover & Landreth, 2000; Harris & Landreth, 1997; Jang, 2000; Kidron, 2004; Lee & Landreth, 2003; Smith & Landreth, 2003; Yuen et al. 2002) . Winek et al. (2003) found that parents facilitated play sessions by demonstrating behaviors of acceptance and encouragement, and children facilitated play sessions by expressing emotions. In addition, these researchers found that initiating affection and feelings of connection between parents and children facilitated play sessions. CPRT-trained parents, through qualitative studies, have consistently reported an increased awareness of the feelings or needs of their children (Edwards et al., 2007; Foley et al. 2006; Kinsworthy & Garza, 2010; Lahti, 1992; Solis et al. 2004; Wickstrom, 2009). Taken as a whole, these findings from research suggest that filial therapy helps to initiate interactions involving emotional expression in the parent–child relationship.
CPRT and Intergenerational Family Therapy
The intergenerational family therapy approaches, such as Bowen’s family systems theory (Bowen, 1985; Papero, 1990), “conceptualize families and their problems in terms of psychological dynamics passed from generation to generation” (Hanna, 2007, p. 14). In order to prevent unhealthy family dynamics from inhibiting the functioning of its members, intergenerational family therapists seek to help family members grow in their insight regarding the patterns within their family of origin and promote each member’s level of differentiation. Differentiated individuals have the ability to understand the separation between their feelings and thinking and “clearly distinguish self from others” (Gehart & Tuttle, 2003, p. 152). Through being able to manage their thoughts and emotions and maintaining a sense of self, intergenerational family therapists believe that family members can achieve relationships that support a healthy balance of togetherness and individuality (Gehart & Tuttle, 2003).
Filial therapists acknowledge the intergenerational nature of family dynamics. For instance, Guerney (2000) noted, “Parents frequently discover personal emotional baggage in trying to relate to their children as prescribed in the play sessions” (p. 8). Landreth and Bratton (2006) echoed this notion in describing how filial therapy “often reminds parents of emotional wounds and issues with their own parents that have been pushed aside over the years” (p. 18). Through the filial therapy process, parents have the opportunity to gain insight into these “personal issues that interfere with their relating to their children as change agents” and this “processing of personal issues facilitates…inner growth” (p. 18). In CPRT, therapists and parents process the following rule: “Be a thermostat, not a thermometer in your child’s life” (Landreth & Bratton, 2006, p. 134). Parents are encouraged to “respond rather than react” and recognize that their “child’s feelings are not [their] feelings” (Landreth & Bratton, 2006, p. 134). This principle in itself supports the differentiation of both parents and their children as they learn to distinguish their thoughts and feelings and maintain a healthy degree of self-other distinction. In addition, through the utilization of the skills of returning responsibility, choice-giving, and limit-setting, Landreth and Bratton (2006) highlighted how parents can provide opportunities to “encourage their child’s self-direction, self-responsibility, and self-reliance” (p. 12).
Several researchers have found that CPRT-trained parents have reported feeling less responsible for or controlling of the behavior of their children (Kinsworthy & Garza, 2010; Lahti, 1992; Wickstrom, 2009). In addition, Wickstrom (2009) found that parents reported decreased reactivity and rescuing behaviors. Winek et al. (2003) identified that parents’ self-awareness regarding how their thoughts and feelings influence their behaviors facilitated play sessions. In addition, children who demonstrated self-reliance and problem-solving behavior, as well as the ability to calm themselves, facilitated play sessions. Beckloff (1997) discovered that parents trained in CPRT made statistically significant gains in recognizing and accepting the independence of their children who were diagnosed with developmental disorders. Multiple research studies have indicated that CPRT often lowers parent–child relationship stress (Bratton & Landreth, 1995; Ceballos & Bratton, 2010; Chau & Landreth, 1997; Costas & Landreth, 1999; Kale & Landreth, 1999; Kidron, 2004; Landreth & Lobaugh, 1998; Lee & Landreth, 2003; Sheely & Bratton, 2010; Tew et al., 2002; Yuen et al., 2002). These research findings demonstrate how filial therapy might promote a healthy sense of individual identity for both parents and children, an increased awareness of family-of-origin issues, and opportunities for the development of self-awareness.
CPRT and Postmodern Family Therapy
The postmodern family therapy approaches, such as narrative therapy (White & Epston, 1990) and collaborative therapy (Anderson, 1997; Anderson & Gehart, 2007; Hoffman, 1993), emphasize how language significantly influences how people experience reality and their problems. Within these postmodern approaches, narratives or conversations provide a way for people to construct multiple meanings from their life experiences. Despite the possibility for generating multiple meanings, individuals tend to have “problem-saturated narratives” that preclude talking about concerns in other ways (Gehart & Tuttle, 2003, p. 214). Postmodern family therapists, because of their belief that problems are a reflection of language, believe that “people are separate from their problems” and “the person is not the problem” (Gehart & Tuttle, 2003, p. 215). Through conversations, postmodern family therapists aim to co-generate new meanings with family members that promote their “preferred narratives” and the construction of new possibilities.
Through the group-processing component of CPRT, parents have the opportunity to share their problem-saturated narratives within the context of a supportive group environment. Landreth and Bratton (2006) noted, “It is common that the discussion of relationship skills elicits parents’ current and/or long-standing intense feelings and reactions about their children. Parents need time to process these feelings” (p. 49). At the same time, CPRT also emphasizes that “the problem is not the problem,” and therapists are encouraged to “keep the focus on the relationship” between parents and children rather than spending time focusing on the problems that parents talk about (Landreth & Bratton, 2006, p. 201). This intentional redirection of the conversations away from problems and toward the possibilities of the parent–child relationship represents an opportunity for new meaning making, perceptions, and experiences of reality to occur. For instance, in the first session, parents are asked what they would like their children, when they are adults, to remember most about their relationship with them. In addition to exercises like these, Landreth and Bratton (2006) encourage therapists to close filial sessions with a motivational poem, book, or story, which stimulate renewed meaning for parents. Because play is a means of communication and parents are verbally active in the way they track, reflect, and respond to their children, the play sessions can also be seen as a means for creating new conversations and narratives between parents and children.
The qualitative studies of filial therapy by Winek et al. (2003) and Wickstrom (2009) offer evidence that parents leave filial therapy with new meanings about their family issues and relationships and new ways of communicating with one another. For instance, Wickstrom (2009) found that filial therapy challenged parents’ “dominant discourses”: “that prizes quick results over the process of relational change” (p. 204), “regarding the polarization of gender roles” (p. 202), and “regarding their expectations for themselves as parents” (p. 204). Winek et al. (2003) identified that parent’s “narrating,” “verbally reflecting the child’s behavior or feeling in the moment,” helped in facilitating play sessions with their children, which gives credence to the idea that play sessions within themselves provide new means for communication between parents and children (p. 97). In addition, one of the most common findings in qualitative studies regarding changes in the parent–child relationship is improved parent–child communication (Bavin-Hoffman et al., 1996; Garza et al., 2009; Lahti, 1992; Solis et al., 2004; West, 2010).
Summary and Conclusion
Despite the conceptual congruence and therapeutic rationale for working with the entire family system, play therapists and family therapists share a common problem in their propensities to focus on certain subsystems of the family. Each field faces pragmatic difficulties in finding consistent means to incorporate family members. As a result, practitioners often divide the family system or exclude members altogether from treatment, diminishing therapeutic potential.
In filial therapy, play therapists and family therapists have a common solution that allows them to incorporate adults and children in efficacious treatment. Guerney (2000) referred to filial therapy as a “remarkably robust approach” (p. 13), and the validity of this perspective is evident in examining its numerous components and its range of application. As demonstrated through the lens of family therapy, filial therapy provides a way to assess and intervene dynamically within family interactions. In examining filial therapy through systems frameworks, therapists trained predominantly in play therapy can find a helpful means for conceptualizing the systemic nature of their work. For practitioners primarily trained in family therapy, the systemic relevance of the filial approach might come as a surprise, given the theoretical framework from which the approach stems. Filial therapy honors the importance of the child subsystem, the parent subsystem, and the overall family system while providing the developmentally appropriate means to address these populations. Through the utilization of play in the context of working with children and discourse in the context of working with adults, filial therapy creates a relevant context for therapeutic interaction with the family system as a whole. See the possibilities.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.