
Abstract
This study investigated the relationships among dysfunctional career thoughts and career indecision with respect to symptoms of depression. Such information could be useful to counselors in identifying individuals at the outset of career counseling who may be experiencing emotional distress from life stressors in addition to career stress. One-hundred fifty-eight college students enrolled in a career development course completed measures of dysfunctional career thoughts, an occupational alternative question, and a measure of depression symptoms. Results indicated that dysfunctional career thoughts and occupational indecision were related to depression symptoms, with decision-making confusion being the best predictor. Implications of the findings for practice and research are discussed.
Clients enter career counseling with varying degrees of distress associated with their presenting career problem. Following intake procedures, they are often administered a screening questionnaire in order to assess readiness for career problem-solving and decision making (Sampson, Peterson, Reardon, & Lenz, 2000). In the practice of career counseling, client responses to routinely administered screening questionnaires can sometimes signal underlying mental health problems. For example, clients who are experiencing career decision-making difficulty often earn scores or endorse items that suggest possible mental health issues such as depression or anxiety (Saunders, Peterson, Sampson, & Reardon, 2000). Moreover, individuals with depression often report impairment in cognitive functions such as attention, memory, and decision-making ability (Woo & Keatinge, 2008). In addition, Beck (1976) noted that depressed individuals display a faulty cognitive pattern of analyzing environmental stimuli and selecting appropriate responses. For these reasons, the presence of mental health issues may well contribute to the presenting career problem, or even interfere with the process of career decision-making during counseling (Lenz, Peterson, Reardon, & Saunders, 2010; Zunker, 2008). Therefore, it is important for career counselors to be able to identify potential mental health issues at the outset of career counseling not only to provide the most effective career counseling services, but also to provide the client with appropriate mental health services and referrals (Zunker, 2006).
Under the Cognitive Information Processing (CIP) model (Peterson, Sampson & Reardon, 1991; Sampson, Reardon, Peterson, & Lenz, 2004), client readiness to make career decisions is assessed at the outset of the career counseling process so that practitioners may best adapt their interventions to the needs of the client. While there are a variety of measures that assess clients’ career-related difficulties (Gati et al., 2004), few specifically target negative thoughts related to career problem-solving and decision making. Thus, the focus of the present investigation is on the use of the Career Thoughts Inventory (CTI; Sampson, Peterson, Lenz, Reardon, & Saunders, 1996a), a measure of dysfunctional thoughts that may also serve as an indicator of potential mental health issues associated with presenting career problems. The CTI provides a total score along with scores for three subscales: (1) decision-making confusion (DMC), (2) commitment anxiety, and (3) external conflict. These four scores provide an indication of the extent to which clients endorse negative thoughts that may impair their ability to make effective career decisions. Because the total score of the CTI has been shown to correlate moderately with symptoms of depression (Dagenhart, 2005; Saunders et al., 2000), it may be a valuable tool for identifying potential mental health problems in addition to career-related maladaptive thought patterns. The Saunders et al. (2000) study additionally revealed that the CTI total score is also related to state and trait anxiety, locus of control, and career indecision, while the Dagenhart (2005) study found that the CTI total score was related to “Like” and “Dislike” response patterns to the Strong Interest Inventory. Thus, the CTI appears to be associated with a variety of important personality characteristics and behaviors that bear on the career decision-making process.
The state of career indecision may also contribute to both the career-related distress and the mental health issues reported by career counseling clientele. For example, in a study by Rottinghaus, Jenkins, and Jantzer (2009), participants who indicated they were decided on a career were significantly less depressed than those who were undecided. In practice, in addition to the CTI as an initial assessment, the Occupational Alternatives Question (OAQ; Slaney, 1980) appears often on career counseling intake forms. A client’s answer to the question, “What occupations are you considering and which is your first choice?” may also suggest the presence of mental health concerns. Related to this, Saunders et al. (2000) found a significant moderate correlation between the OAQ and depression. These findings suggest that clients who indicate higher levels of career indecision may also experience psychological distress associated with a presenting career problem.
While it is not common practice to assess concurrent mental health issues in career counseling, career problems are often inextricably related to mental health concerns (Betz & Corning, 1993; Blustein & Spengler, 1995; Herr, 1997; Krumboltz, 1993; Lenz et al., 2010; Swanson, 2002). Because the latter difficulties may interfere with career problem-solving and decision making, service professionals in the career counseling field would be remiss if they did not address both issues for the client in order to offer a more holistic range of services to effectively address a presenting career problem (Zunker, 2008). In identifying and addressing potential mental health concerns associated with a career problem, we propose that it may be possible to identify the existence of possible mental health issues that interfere with readiness for career problem-solving and decision making using common career-related measures. Through the identification of potential intervening mental health issues in career-related instruments, the use of more specific mental health assessments could then be explored with the client.
The purpose of the current study, therefore, was to investigate the relationships among measures of dysfunctional career thoughts, career indecision state, and symptoms of depression. Specifically, the question is raised, “Are there thresholds for scores on the CTI and the OAQ that suggest a level of emotional distress that should be addressed at the outset of career counseling?” Such information would be useful in settings such as career centers, counseling centers, employment centers, veteran’s hospitals, and any other venue that provides career counseling services. Being able to screen for the need to assess depression and other mental health problems will facilitate the provision of more comprehensive services to clientele who possess social and emotional concerns related to, or involved in, a presenting career problem.
We hypothesized that the total score and subscale scores of the CTI as well as the state of career indecision, as measured by the OAQ, will be positively related to the degree of depression symptoms measured by the Beck Depression Inventory-II (BDI-II). Because males and females may respond to environmental stress differently (Taylor et al., 2000) and may in turn differentially endorse depression symptoms, we also explored whether gender is a factor to consider in the relationship between negative career thoughts and career indecision with respect to depression.
Method
Participants
Participants were 158 undergraduate students enrolled in five sections of a 3-credit hour career development course in a large southeastern university. The sample was comprised of 91 males (57.6%) and 67 females (42.4%) with a mean age of 20.50 years (SD = 1.95). Regarding race and ethnicity, 61.6% were Caucasian, 23.9% African American, 10.1% Hispanic/Latino, 1.9% Native American, 1.3% Asian American, and < 1.2% indicating “other.” Year in school included 8.9% freshmen, 28.5% sophomores, 20.9% juniors, and 41.7% seniors.
Procedure
Participants were given a folder containing the battery of instruments by their course instructor during the first week of their regularly scheduled classes, and they were informed that they would have the option to participate in a research study that investigated the relationships between career decision making, career thoughts, and symptoms of depression. These folders were identified with unique numbers in order to maintain the anonymity of responses. Each folder contained the same battery of questionnaires, counterbalanced to control for order effects. Participants completed a basic demographic questionnaire, the CTI, the OAQ, and a modified version of the BDI-II.
Instruments
Demographic Questionnaire
Participants completed a form indicating their age, gender, ethnicity, year in school, current and prior work experience, and current involvement in campus activities/organizations. The OAQ was also included on this form.
CTI
The CTI is a theory-driven assessment that assesses dysfunctional thoughts related to career decision making (Sampson, Peterson, Lenz, Reardon, & Saunders, 1996b). The 48-item measure asks participants to rate the extent to which they agree or disagree with thoughts and emotions surrounding the career decision-making process according to a 4-point Likert-type scale where 1 = strongly disagree and 4 = strongly agree. Sample items are “I’ll never understand myself well enough to make a good career choice” and “I’m afraid I’m overlooking an occupation.” The CTI contains three subscales: decision-making confusion (DMC; 14 items), commitment anxiety (CA; 10 items), and external conflict (EC; 5 items) as well as a cumulative total score using all 48 items. The DMC scale reflects an “inability to initiate or sustain the decision-making process itself” (Sampson et al., 1996b, p. 28). The CA scale reflects an “inability to make a commitment to a specific career choice, accompanied by generalized anxiety about the outcome of the decision-making process,” with anxiety perpetuating the indecision (Sampson et al., 1996b, p. 28). The EC scale reflects the “inability to balance the importance of one’s own self-perceptions with the importance of input from significant others, resulting in a reluctance to assume responsibility for decision making” (Sampson et al., 1996b, p. 29). Higher scores indicate greater impairment in dysfunctional thoughts associated with the career decision-making process. Sampson et al. (1996b) reported internal consistency coefficients for the CTI subscales in a sample of college students as .82 for DMC, .79 for CA, and .74 for EC. Concurrent validity coefficients reported for the CTI total score for college norms include: My Vocational Situation–Identity, r = −.69; Career Decision Scale–Indecision, r = .70; Career Decision Profile–Decidedness, r = −.48; and NEO Personality Inventory–Revised (NEO-PI-R)–Depression, r = .51 (Sampson et al., 1996b). Four-week stability coefficients for high school and college students ranged from .74 to .82 (Sampson et al., 1996a). Participant αs in the current study were CTI total score = .96, DMC = .95, CA = .87, and EC = .75.
OAQ
The OAQ was used to measure students’ state of career indecision (Zener & Schnuelle, 1972; modified by Slaney, 1980). The OAQ is treated as a continuous and interval scale consisting of two questions: (1) “List all the occupations you are considering right now” and (2) “Which occupation is your first choice? If undecided, write ‘undecided’.” The OAQ is scored on a scale of 1 to 4 (1 = first choice listed with no alternatives, 2 = first choice listed with alternatives, 3 = no first choice listed/only alternatives, and 4 = neither a first choice nor alternatives are listed). Thus, the higher the OAQ score, the greater the degree of indecision. The test–retest reliability of a questionnaire that included the OAQ was reported to be .93 (Slaney, 1978). The OAQ has demonstrated concurrent validity with other measures of career indecision such as the Satisfaction with Career Scale, the Vocational Decision Making Difficulties Scale, and the Career Decision Scale (Slaney, 1980; Slaney, Stafford, & Russell, 1981).
BDI-II
The BDI-II is a 21-item self-report measure of depression symptom in adolescents and adults (Beck, Steer, & Brown, 1996a). It is a summated rating scale that asks participants to rate each item on a 4-point Guttman scale from 0 to 3, with higher scores indicating greater severity of symptoms of depression. The item content of the scale alludes to cognitive, emotional, and physical symptoms of depression (Beck & Steer, 1984; Moran & Lambert, 1983). For research purposes, Question #9, which concerns suicidal ideation and intent, was omitted from this scale as directed by the university institutional review board. Thus, the depression inventory included 20 total items. Beck, Steer, and Brown (1996b) reported a test–retest coefficient of .93 with outpatient college students, and Sprinkle et al. (2002) reported a .96 test–retest coefficient also with college students. An α coefficient of .91 was derived for the present participant sample using the 20-item scale.
Results
The correlation matrix, along with means and standard deviations of all variables, is presented in Table 1. With respect to zero-order correlations between dysfunctional career thoughts and depression symptoms, there was a moderate positive relationship between the CTI total score and the BDI-II (r = .42, p < .001). The relationship between the subscales of the CTI and the BDI-II were DMC (r = .51, p < .001), Commitment Anxiety (r = .40, p < .001, and External Conflict (r = .39, p < .001). Therefore, as predicted, all four measures of dysfunctional career thoughts were positively related to depressive symptoms. Further, a stepwise linear regression analysis, conducted to ascertain the best predictor of depression among the CTI subscales, revealed that when the DMC scale was entered first, only this variable captured a significant amount of variation in the model. Commitment Anxiety and External Conflict were nonsignificant predictors, once the variation attributed to DMC was partitioned (see Table 2). Therefore, because the DMC scale had the highest correlation with the BDI-II and captured the preponderance of variation in the prediction model, we concluded that the single best indicator of depressive symptoms using the CTI is the DMC scale.
Correlations Between Depression Symptoms, Career Thoughts, and Occupational Alternatives
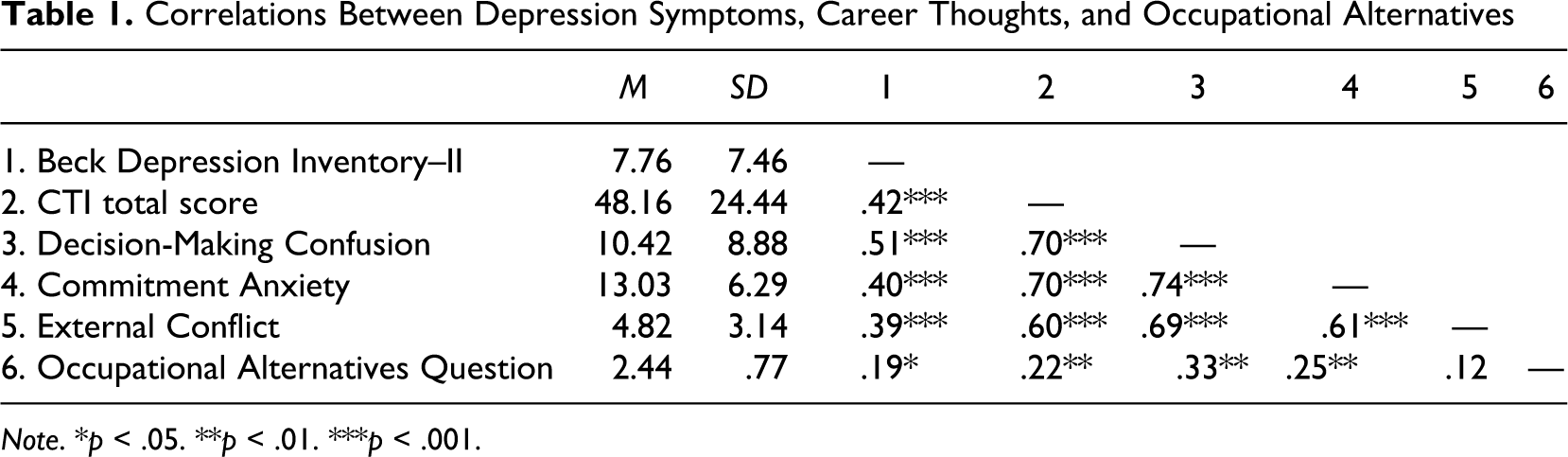
Note. *p < .05. **p < .01. ***p < .001.
Regression Analysis With CTI Subscales as Predictors of the BDI-II
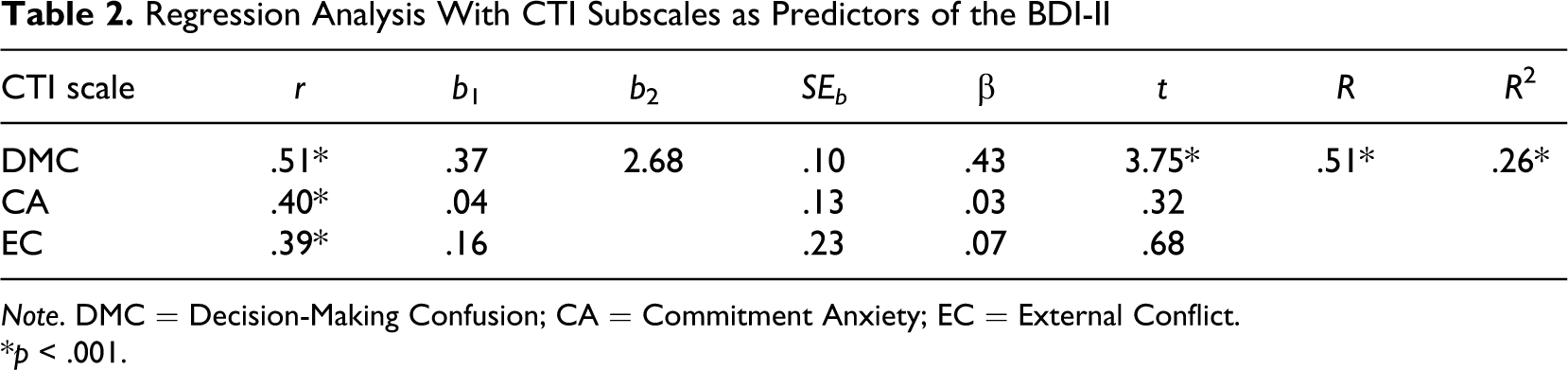
Note. DMC = Decision-Making Confusion; CA = Commitment Anxiety; EC = External Conflict.
*p < .001.
A correlational analysis revealed that there was also a significant (r = .19, p < .05) relationship between responses to the OAQ and depression symptoms. An analysis of variance (ANOVA) with the four levels of the OAQ as the independent variable and the BDI-II as the dependent variable failed to achieve significance, F(3, 154) = 2.103, p = .10. However, this result may be attributed to the unequal group sizes, in that 12 participants endorsed a “1” (decided), 79 a “2” (first choice, with alternatives), 52 a “3” (alternatives only), and the remaining 15 a “4” (undecided). For this reason, Groups 1 and 2 (those who had identified at least a first choice of an occupational alternative) and Groups 3 and 4 (those who were unable to identify a first choice or who were “undecided”) were combined to form two larger groups. A subsequent ANOVA with these two combined levels of the OAQ achieved statistical significance, F(1, 156) = 4.677, p < .05, Cohen’s d = .34. Therefore, the OAQ may serve as an indicator of mental health issues in that college students who have chosen an occupation or who have determined a first choice from a list of options demonstrated significantly less evidence of depression symptoms compared to college students who list only career options or record “undecided” (see Table 3).
ANOVA With Two Levels of OAQ and BDI-II as Dependent Variable
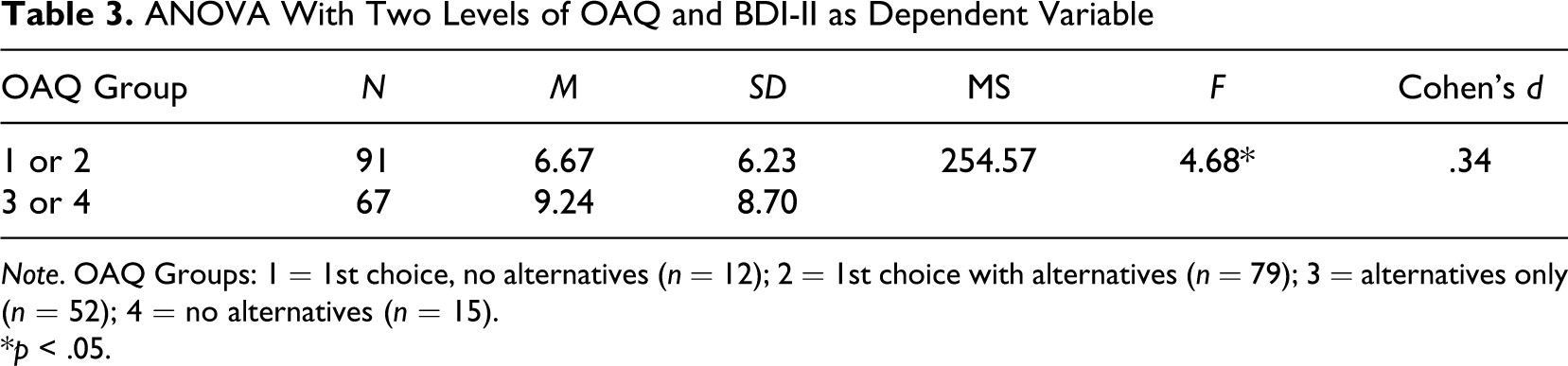
Note. OAQ Groups: 1 = 1st choice, no alternatives (n = 12); 2 = 1st choice with alternatives (n = 79); 3 = alternatives only (n = 52); 4 = no alternatives (n = 15).
*p < .05.
Finally, a series of one-way ANOVAs were conducted with gender as an independent variable and the BDI-II, CTI total score and subscales, and OAQ as dependent variables, respectively. Results indicated that there were significant differences between males and females for the CTI total score, F(1, 156) = 6.787, p < .05, and for the Commitment Anxiety subscale of the CTI, F(1, 156) = 4.953, p < .05. However, there were no significant differences (p > .05) between males and females regarding the DMC subscale of the CTI, the OAQ, or the BDI-II. Further, employing a hierarchical regression analysis, with gender as a second predictor of BDI-II scores, revealed that gender failed to capture significant (p < .05) increases in variation when either DMC or OAQ were entered first. Therefore, these findings suggest that both the DMC scale and the OAQ may be preferred as indicators of possible mental health issues associated with a presenting career problem, as any ostensible gender effects appear to be insignificant.
Discussion
The results of this study indicate that measures of career thoughts and career indecision, specifically all four dimensions of the CTI and the OAQ, were significantly related to symptoms of depression, while the DMC scale of the CTI and the OAQ appear to be the principal indicators of the presence of possible mental health issues that may be associated with a presenting career problem. Further, these scores do not appear to be influenced by gender.
These findings suggest an important perspective on the influence of depression on the process of career decision making itself. At this point, we find it helpful to draw on the cognitive information processing (CIP) paradigm and the Communication, Analysis, Synthesis, Valuing, and Execution (CASVE) decision cycle (Peterson et al., 1991; Peterson et al., 1996; Sampson et al., 2004) to illuminate the findings. Briefly describing the cycle, the Communication (C) phase entails becoming in touch with thoughts, feelings, and circumstances regarding the presenting career problem; the Analysis (A) phase alludes to forming a mental model of the problem as well as clarifying and developing self-knowledge and occupational knowledge; Synthesis (S) involves formulating viable career options; Valuing (V) entails prioritizing options and arriving at a first choice; and finally, the choice is implemented in the Execution (E) phase. In transposing the three factor scales on the CASVE cycle, the DMC scale is associated with the Communication, Analysis, and Synthesis phases of the CASVE Cycle, the EC scale is associated with the Valuing phase, and the CA scale is associated with the Execution phase. The results of this study indicate that depression is significantly associated with all phases of the decision cycle, suggesting the pervasiveness of this mood state. In addition, the findings underscore the importance of scores on the DMC scale, relative to others, in identifying potential mental health issues and addressing them at the beginning stages of the decision-making process. If this is so, the question now becomes, how might scores on the CTI and OAQ be used in the practice of career counseling?
Using a linear extrapolation of a linear regression formula (BDI-II = DMC (.424) + 3.335) conducted with scores on the DMC scale predicting scores on the BDI-II, college students who earn a T-score of 75 on the DMC scale predict a score of 16 on the BDI-II, a score indicating mild depression according to the BDI-II professional manual (Beck, Steer, & Brown, 1996b). In other words, individuals who obtain a score of this magnitude on the DMC provide evidence that they may well be experiencing emotional discomfort that is attributed to or associated with the presenting career problem. However, a T-score of 68 would take into account the lower bound level of the 95% confidence interval, to guard against the occurrence of false negatives. Thus, we recommend that a T-score of 68 or higher on the DMC scale of the CTI would indicate that further inquiry into the existence of possible mental issues is necessary. Furthermore, according to our findings, an accompanying score of 3 or 4 on the OAQ provides additional supportive evidence of possible mental health issues.
As in this study, the BDI-II could be used as a follow-up instrument to assess the extent of emotional discomfort associated with a presenting career problem in career or mental health centers. In addition, the Decision Space Worksheet (Peterson, Leasure, Carr, & Lenz, 2009–2010), a projective assessment, could be used to elicit elements in the social and emotional context out of which the presenting career problem arises. In career and mental health services where there is qualified professional assistance available, the use of a comprehensive personality measure such as the Minnesota Multiphasic Personality Inventory (MMPI)-2 [Hathaway & McKinley, 1942] or the Personality Assessment Inventory (PAI) [Morey, 1991] could provide an assessment of general personal and social adjustment (Lenz et al., 2010; Peterson & Githens, 1990). After obtaining scores on mental health assessments, a treatment plan or an individualized learning plan (ILP; Sampson et al., 2004) can be formulated with the client, taking into account possible referral for further clinical assessment or conjoint personal counseling. Finally, venturing into the realm of mental health issues has the potential to reveal severe or chronic pathological states or even the revelation of suicide ideation (e.g., Item #9 on the BDI-II), for which career counselors should be adequately prepared to manage.
However, the quest to incorporate mental health assessment and treatment into career counseling raises important organizational policy and procedural issues for a career or mental health service provider. A first issue alludes to the mission of the service provider with respect to addressing the needs of individuals who demonstrate mental health concerns along with their presenting career concerns. According to Betz and Corning (1993), Krumboltz (1993), and Zunker (2008), career and mental health concerns are intertwined, and therefore should be treated holistically and not treated as separate entities. A second issue concerns the level of expertise and qualifications of personnel to treat mental health aspects of the career problem. The ability to use interventions and counseling techniques appropriate for depression or anxiety such as cognitive behavioral therapy (CBT; Beck, 1976; Beck, Rush, Shaw, & Emery, 1979) or mindfulness-based interventions (Jacobs & Blustein, 2008; Kabat-Zinn, 2003) or even suicide prevention (Joiner, Van Orden, & Witte, 2009) would be in order. Third, there is the inevitable and realistic matter of financial resources to offer comprehensive career and mental health services that include purchasing, administering, and scoring mental health assessments in addition to providing the trained and certified staff and time to effectively address the mental health dimensions of a career problem (Reardon, 1996). In an era of static or declining resources to offer human services, these may become difficult issues to resolve. However, relying on referral sources to address mental health aspects of career problems also raises difficult issues such as availability, coordination with the career counseling process, and possible cost to the client. Nevertheless, if clients indicate through an intake interview and scores earned on routinely administered career instruments that mental health issues could be present which may limit their ability to solve career problems and to make appropriate decisions, we believe that addressing both the client’s mental health and career issues is an organizational, professional, and ethical responsibility.
Though the results of this study and prior authors (e.g., Lenz et al., 2010; Zunker, 2008) agree that career indecision and mental health issues are often entangled, the current study does not purport to provide a causal direction for this complex relationship. Rather, the purpose of this study was to offer clinicians an efficient manner in which comorbid mental health issues may be screened when assessing career indecision. Because this relationship is not yet fully understood, it is equally viable to state that mental health issues such as depression and anxiety may lead to career indecision and also that career indecision may lead to an individual’s feeling depressed and anxious. Future studies should attempt to shed some light on the causal nature of this relationship so that the etiology of career indecision and depression as they relate to each other may be better understood.
There are several limitations that should be addressed. In the current study, we selected the BDI-II as a general indicator of the domain of mental health, because depression has been shown to be negatively related to a client’s ability to navigate the career decision-making process (Saunders et al., 2000; Zunker, 2008). However, other mental health problems, such as anxiety and personality disorders, may likely interfere with career decision making and should therefore be investigated in future studies. Further, the present study used only the CTI and OAQ as potential indicators of accompanying mental health issues. Certainly, other instruments should be explored as predictors and potential mental health screeners. Finally, the present study was conducted with a college student sample, making the findings relevant for counselors working in collegiate settings. However, before the results of this study are generalized to other services and client populations, we recommend that similar research studies be conducted at the local site to confirm transferability.
In conclusion, we offer an alternative to either ignoring a mental health component of a presenting career problem or using subjective clinical judgment to make a determination of whether to move into the realm of mental health. While we have used instruments that are commonly used in career and mental health centers in this study, we encourage the exploration of other career and mental health instruments to ascertain the existence of mental health issues that are an important aspect of a presenting career problem.
Footnotes
Author’s Note
This article builds upon an article published in The Journal of Career Assessment in 2009 (Vol. 17, 3) titled “Relation of Depression and Affectivity to Career Decision Status and Self-Efficacy in College Students.”
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.