
Abstract
Childhood abuse is an important risk factor for depression, anxiety disorders, and substance use later in life. One possible mechanism underlying this association could be deficits in cognitive processing of emotional information. This study tested the impact of distracting emotional information on working memory performance in 21 young women with a history of sexual and physical abuse during childhood/adolescence (mean age = 20.0), and compared their performance to 17 individuals reporting nonabuse-related childhood stress (mean age = 19.6) and a control group of 17 women without a history of childhood stress (mean age = 20.0). During the most difficult distractor condition, working memory accuracy for positive versus neutral incidental emotional stimuli was reduced in women reporting a history of abuse relative to both control groups (with and without nonabuse-related childhood stress). The current results reveal aberrant responses to positive stimuli and are consistent with the notion of persistent influence of childhood abuse on processes critical for emotional well-being and emotion control.
Traumatic events and experience of early stress (ES) during childhood or adolescence, such as parental loss, witnessing violence, or sexual or physical abuse have been linked to a variety of adverse health outcomes during the life span (McCrory, De Brito, & Viding, 2010). More specifically, these experiences have been shown to be an important risk factor for development of later psychopathology, such as depression, posttraumatic stress disorder, anxiety, and substance abuse (Coffino, 2009; J. G. Green et al., 2010; MacMillan et al., 2001). Importantly, childhood sexual abuse is particularly related to psychopathology even when other adversities and stressors are taken into consideration (Molnar, Buka, & Kessler, 2001). In order to develop interventions aimed at diminishing the adverse effects of such traumatic childhood stress later in life, it is crucial to gain insight into the underlying cognitive mechanisms linking early life stress to psychopathology.
Current research suggests two possible pathways for reduced health and quality of life in victims of childhood maltreatment. These pathways center on (1) reduced cognitive control and self-regulatory abilities and (2) dysfunctional emotion processing. Although limited, on one hand, previous work in individuals with experience of ES has documented impairments in cognitive control such as inhibition (Carrion, Garrett, Menon, Weems, & Reiss, 2008; De Bellis, Hooper, Spratt, & Woolley, 2009; Jovanovic et al., 2013; Lewis, Dozier, Ackerman, & Sepulveda-Kozakowski, 2007; Mueller et al., 2012), response shifting (Mueller et al., 2010), and working memory (Majer, Nater, Lin, Capuron, & Reeves, 2010). Due to the frequent co-occurrence of multiple stressors (J. G. Green et al., 2010), most of these previous studies have included individuals with different types of early life stress, such as neglect and maltreatment (Mueller et al., 2010), emotional abuse, sexual or physical abuse and/or neglect (Majer et al., 2010), and youth who experienced physical or sexual abuse, or witnessed violence (Carrion et al., 2008). By comparison, only a few of these studies have differentiated between types of stressors and have taken the severity of the ES experience into account (De Bellis et al., 2009; Majer et al., 2010). In contrast to the limited work on cognitive impairments in ES, much research has documented detrimental changes in processing emotions after emotional neglect and maltreatment (Maheu et al., 2010; Masten et al., 2008; Tottenham et al., 2010). For example, individuals with a history of maltreatment show abnormalities in emotional face recognition, especially in negatively valenced faces and exhibit a hyperresponsivity to both angry (Curtis & Cicchetti, 2011; Fries & Pollak, 2004) and fearful faces (Masten et al., 2008).
Even though both pathways, that is, reduced cognitive control and impaired emotion processing, are important to understand the relationship between ES and psychopathology, increasing efforts, which focus on the tight and dynamic interplay between emotion and cognitive control (Cromheeke & Mueller, 2013; Pessoa, 2009), suggest that these two pathways might not be independent. Dovetailing this interplay, a study that investigated the effects of reward on cognitive control reported improvements in inhibitory control with reward in healthy adolescents but not adolescents with a history of maltreatment and emotional neglect, which suggests stress-related deficits in the processing of positive information (Mueller et al., 2012). However, apart from studies examining information processing changes associated with reward (e.g., Guyer et al., 2006; Milner et al., 2011; Mueller et al., 2012), no study to our knowledge has investigated how other positive and negative emotional stimuli influence cognitive control processes in individuals reporting severe trauma such as physical and sexual abuse. However, cognitive research suggests a change in the processing of positive and negative child-related schemata in children at risk of physical abuse relative to low-risk children (Milner et al., 2011). Recent work demonstrated that the ability to update positive information in working memory was positively linked to life satisfaction and balanced affect (Pe, Koval, & Kuppens, 2013). Such findings might provide important clues to building resilience and establishing effective therapeutic interventions for survivors of abuse and ES (e.g., Fisher, Chamberlain, & Leve, 2009; Healey & Fisher, 2011; Pe et al., 2013). Since studies investigating emotion–cognition interactions in maltreatment are scarce, evidence in disorders for which individuals with experience of maltreatment have high propensity might provide helpful links.
In a meta-analysis on the emotional Stroop task, depressed individuals, relative to healthy comparisons, exhibited consistent attentional biases for both negative and positive stimuli albeit not as strong in the latter (Epp, Dobson, Dozois, & Frewen, 2012). In line with this view, remitted depressed individuals show differential neural responses during functional magnetic resonance imaging to positive (hypoactivation) and negative (hyperactivation) distracting emotion in the prefrontal cortex during a working memory task (Kerestes et al., 2012). In anxious individuals, less evidence is available but shows, for example, slowed updating of working memory during positive emotion in high anxious versus low anxious children (Visu-Petra, Tincas, Cheie, & Benga, 2010). These empirical data support suggestions of a link between cognitive control abilities such as working memory and emotion regulation and emotion control processes (Joormann & D’Avanzato, 2010; Joormann & Gotlib, 2008, 2010; Schmeichel & Demaree, 2010; Schmeichel, Volokhov, & Demaree, 2008), further underlining a tight interplay between affective and executive processes.
The current study sought to address how emotional stimuli interfere with cognitive control processes, such as working memory, in young women with a history of childhood sexual and physical abuse. To assess specificity of adverse childhood experience on emotion processing, a second group of young women who had experienced other childhood adversities were included in addition to a control group with no history of ES, given that different types of childhood stress have been found to result in distinct outcomes (Bruce, Fisher, Pears, & Levine, 2009; McCrory et al., 2010). Based on (1) findings in individuals with mood and anxiety disorders (Joormann & Gotlib, 2008; Stout, Shackman, & Larson, 2013), (2) a high vulnerability of sexually and physically abused individuals to develop such psychopathology (Chou, 2012; J. G. Green et al., 2010), and (3) the severity of childhood sexual/physical abuse relative to other adversities (Molnar et al., 2001), three main predictions were made. First, it was hypothesized that the abuse group would show impaired working memory performance during emotional distractors relative to (1) a neutral condition, (2) individuals reporting a history of nonabuse-related childhood stress, and (3) healthy comparisons in a visuospatial working memory task. Finally, we also predicted that both groups with a history of childhood stress would show higher rates of self-reported psychopathology than the control group.
Method
Participants
First-year university psychology students (n = 616) were asked to complete several screening questionnaires in exchange for course credit. For the present purposes, students were asked to indicate the number of stressors they had encountered during childhood and/or adolescence (0, 1, 2, or more). Due to ethical reasons, no questions were asked regarding the specificity of stressors at that moment. To recruit female participants with a history of physical/sexual abuse, we invited individuals who reported two or more early life stressors on the initial screening (n = 78) into the laboratory, of whom 40 voluntarily agreed to participate in the study and fill in additional questionnaires. All participants came from a homogenous background in Flanders and were of Caucasian ethnicity. To assess the nature of the stressors more specifically, upon visiting the laboratory participants completed the Stressful Life Events Screening Questionnaire (SLESQ; Goodman, Corcoran, Turner, Yuan, & Green, 1998), a 13-item self-report measure to determine exposure to 11 specific and 2 general categories of events (e.g., life-threatening accident, sexual, physical, or emotional abuse). For each category, participants were asked to indicate whether they had experienced such an event and, if they responded “yes,” to specify the event (e.g., age, frequency, duration). The SLESQ has a good test–retest reliability (median κ = .73) and adequate convergent validity (median κ = .64; Goodman et al., 1998). In the current sample, the internal consistency of the SLESQ was acceptable (α = .6). To assess sexual and physical abuse specifically, the questionnaire includes the following items: “1) At any time, has anyone (parent, other family member, romantic partner, stranger or someone else) ever physically forced you to have intercourse, or to have oral or anal sex against your wishes, or when you were helpless, such as being asleep or intoxicated? 2) Other than experiences mentioned in earlier questions, has anyone ever touched private parts of your body, made you touch their body, or tried to make you to have sex against your wishes? 3) When you were a child, did a parent, caregiver or other person ever slap you repeatedly, beat you, or otherwise attack or harm you?” For the abuse group, only female students who had reported either sexual abuse (n = 10), physical abuse (n = 4), or a combination of both (n = 7) were selected (Total N = 21, mean age [M age] = 20.0, standard deviation [SD] = 1.9). Students reporting other experiences of childhood stress, such as illness or accidents, were included in the nonabuse stress group (n = 17, M age = 19.6, SD = 1.1). The control group consisted of 17 female students (n = 17, M age = 20.2, SD = 1.7) who did not report any prior or current stressful life events in the SLESQ (details of experienced stressors in Table 1). All participants agreed to voluntarily take part in the experiment in exchange for course credits or monetary compensation. The study was approved by the ethical committee of the Faculty of Psychology and Educational Sciences at Ghent University.
Detailed Information on Reported Stressors as Assessed With the Stressful Life Events Screening Questionnaire (SLESQ) for the Control, Stress, and Abuse Group, Separately.

aExamples include a car accident, witnessing an explosion, suicide attempt of a parent or life-threatening illness of a parent.
To assess the presence of psychopathology, participants completed the Dutch version of the Adult Self-Report (ASR; Achenbach & Rescorla, 2003), a screening instrument measuring mental health problems (internalizing and externalizing), resulting in scores on both syndrome scales and Diagnostic and Statistical Manual of Mental Disorders scales. The ASR has a good reliability and content validity, and excellent internal consistency (α = .94; Evers, van Vliet-Mulder, & Groot, 2005; α = .95 in the current sample). T scores higher than 63 on the subscales Internalizing problems, Externalizing problems, and Total problems are considered clinical. Current levels of depression and anxiety were assessed with the Beck Depression Inventory (BDI; Beck, Erbaugh, Ward, Mock, & Mendelsohn, 1961) and State–Trait Anxiety Inventory (STAI; Spielberger, Gorsuch, & Lushene, 1970; Table 2). Both the BDI-II-NL and STAI-NL have good validity and excellent internal consistency (α = .88 and α = .9, respectively, Evers et al., 2005; in the current sample: α = .93 for BDI, α = .92 for STAI-State, α = .94 for STAI Trait). Since resilience has been shown to moderate the presence and severity of depression following childhood trauma (Wingo et al., 2010), we also included the Resilience Scale (RS-NL; Wagnild & Young, 1993), a 25-item questionnaire with good internal consistency (α = .85; in the current sample: α = .80), test–retest reliability (r = .9), and acceptable construct validity (Portzky, Wagnild, De Bacquer, & Audenaert, 2010).
Demographic Information and Mean Scores (SD) on the Measures of Anxiety (STAI), Depression (BDI), Total Psychopathology (ASR), Mean Number of Stressors, and Resilience Score.

Note. SD = standard deviation; STAI = State–Trait Anxiety Inventory; BDI = Beck Depression Inventory; ASR = Adult Self-Report.
a z scores are shown for BDI, STAI-state, and STAI-trait. b T scores are used.
Stimuli and Material
Images of 44 different actors (24 male and 20 female) were selected from the NimStim face stimulus database (Tottenham et al., 2009) and the Radboud Faces Database (Langner et al., 2010). Each actor posed three emotional expressions (neutral, happy, and angry) with closed mouth, resulting in a total of 132 faces. Only pictures with emotion ratings of 70% or higher (mean emotion rating: 94%) for all three emotions were selected (Langner et al., 2010; Tottenham et al., 2009). To avoid confounds based on external features, background and hair were removed, and images were gray scaled (256 gray levels) using Adobe Photoshop 5.0. The faces were displayed on a black background at 160 × 200 pixels, corresponding to approximately 4 × 5 cm. At the beginning of the experiment, 30 individuals (15 male and 15 female) were randomly chosen from the selection of 44 actors. Each actor only expressed one emotion throughout the task, resulting in 10 individuals per emotion (five male and five female). The task consisted of 120 trials divided into four blocks of 30 trials each. Within each block, every actor was shown once. After completing the task, participants were asked to fill in the questionnaires.
Procedure
The sequence of the Spatial Emotional Match To Sample (SEMTOS) task, modeled after a nonemotional variant of Awh, Jonides, and Reuter-Lorenz (1998), during a single trial was as follows (Figure 1): (a) A yellow fixation cross was shown at the beginning of the trial for 1 s, (b) the memory cue (a happy, angry, or neutral face) appeared for 400 ms in 1 of the 24 possible locations. The locations were equally spaced on an imaginary concentric circle with a radius of 250 pixels. To prevent verbal coding of locations, every possible location was located at least 10° clockwise or counterclockwise from the cardinal axes, (c) during a retention interval of 5,000 ms, a red or blue color probe was shown for 1,000 ms. Participants were asked to indicate the color of this stimulus by pressing the red or blue button (“w” or “x” on the keyboard, covered with red and blue stickers, respectively) with the left hand. The interval between the end of the memory cue and the appearance of the color probe varied randomly between 1,000 ms and 3,000 ms, (d) after the retention interval, the face was shown again for 1,500 ms. Participants had to indicate whether this memory probe had the same location as the memory cue that was shown at the beginning of the trial. They were instructed to press “=” for match trials and “≠” for miss trials (“:” and “=” on the keyboard, covered with stickers of = and ≠, respectively), using their right hand.
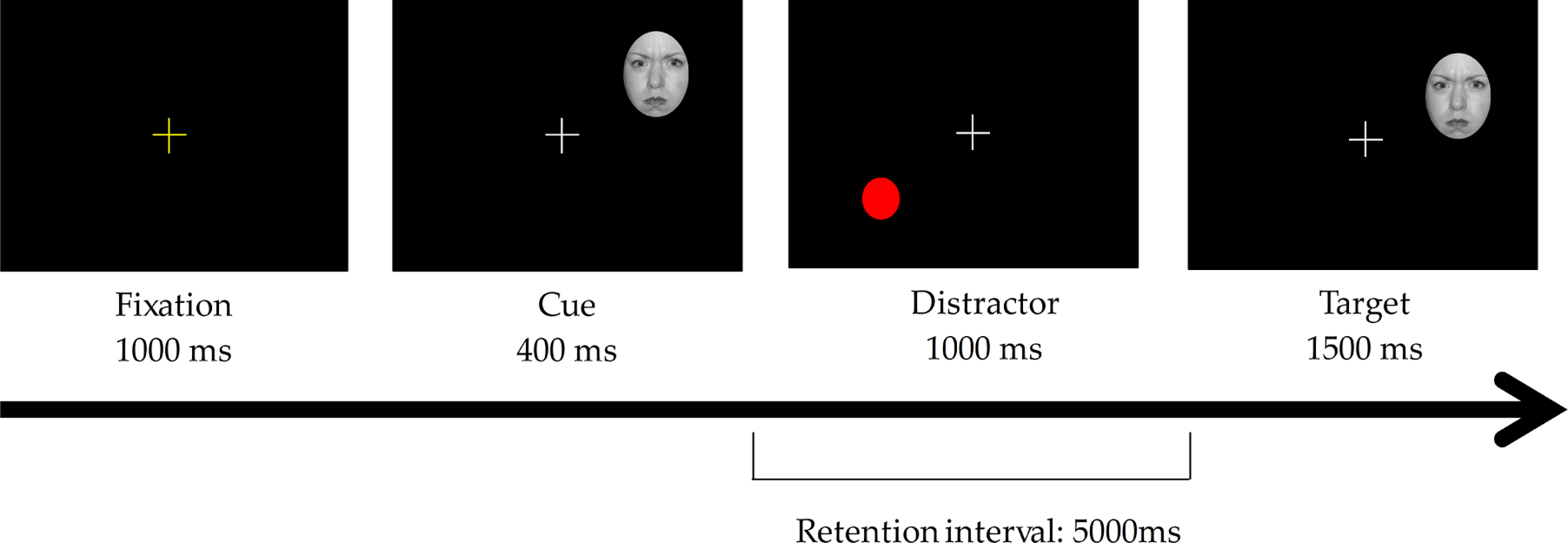
Overview of a typical trial in the SEMTOS task. SEMTOS = spatial emotional match to sample.
Before starting the experiment, both the memory and the color discrimination tasks were practiced separately first, and then together. Each practice block consisted of 10 trials. Participants only continued to the next block if they had an accuracy rate of at least 60%. They were asked to look at the fixation cross at the beginning of each trial, when the fixation cross turned yellow. For both the memory probe and the color probe, only responses within a response window of 2,000 ms were registered. Participants were instructed to respond as quickly as possible, but without compromising accuracy. They did not receive feedback about their performance on either task.
The location of the memory probes matched the memorized location on 40% of the trials (match trials). When the locations did not match (miss trials), the distance between the memory cue and probe was varied systematically between 15° (Miss1), 20° (Miss2), and 25° (Miss3) clockwise or counterclockwise on the imaginary concentric circle, respectively. The emotional expression and gender of the faces was counterbalanced across these conditions.
The distance between the memory cue and the color probe varied systematically. Color probes were shown either near (40° on the imaginary circle) or far (160° on the imaginary circle), and either clockwise or counterclockwise from the memorized location.
Statistical Analysis
A 4 × 3 × 3 repeated measures analysis of covariance (ANCOVA) on responses to the memory probe was conducted with Location (Match, Miss1, Miss2, Miss3) and Emotional expression (angry, happy, neutral) as within-subjects factors and Group (abuse, stress, and control group) as between-subjects factor. The ANCOVA was run twice, once for accuracy (% correct) and once for reaction times (in milliseconds). Significant interactions or main effects were followed up with pairwise comparisons, paired samples t-tests, or univariate analyses, as appropriate. Mean reaction times were based on correct trials. Reaction times of less than 100 ms were excluded as anticipatory responses. Additional correlational analyses (Pearson’s r) were carried out to investigate the association of the behavioral findings with results of mood state and psychopathology as well as individual factors of abuse (e.g., age of onset, duration, frequency of abuse). Measures of effect size are reported as Cohen’s d or partial η2 (as appropriate).
Results
Questionnaire Results
Table 1 shows details of the type and number of stressors reported by the control, stress, and abuse group. Groups differed significantly on the mean number of stressors with the abuse group reporting more stressors than the stress group, and both the abuse and stress group reporting more stressors than the control group (p < .001 for all pairwise comparisons, Bonferroni corrected). Table 2 shows the demographic and psychopathology indicators by the control, stress, and abuse group. Age or resilience scores did not differ between groups. However, significant group differences were found on trait levels of anxiety, state levels of anxiety, and symptoms of depression. Post hoc tests indicated that both the stress and the abuse group scored higher than controls on trait (p = .005 and p = .001, respectively) and state anxiety (p = .026 and p = .028, respectively). The abuse group also reported more symptoms of depression than controls (p < .001), while the difference between the stress and control group on this measure approached conventional levels of significance (p = .059). In terms of psychopathology, while none of the participants in the control group met clinical cutoff scores, 8 of the 17 women in the stress group and 8 of the 21 women in the abuse group scored within the clinical range on internalizing and externalizing scales, a difference that was significant, χ2(2, N = 54) = 111.06, p = .004. Participants also differed on the total psychopathology (ASR) scores, with women in the abuse and stress group scoring significantly higher than control women (p < .001 and p = .003, respectively). Given the group differences in levels of depression and anxiety, these variables were added as covariates in the subsequent analyses (but we do not discuss them, as they were not the focus of our hypotheses).
Accuracy
As expected, the three-way Location by Emotion by Group interaction was significant, F(12, 300) = 2.02, p = .023, partial η2 = .08. To follow-up this interaction, the analyses were rerun split at the level of Group (Figure 2, Table 3). Location significantly interacted with Emotion in the abuse, F(6, 108) = 2.32, p = .04, partial η2 = .11, and the stress group, F(6, 84) = 2.42, p = .03, partial η2 = .15. In the control group, however, this interaction was not significant.

(A) Accuracy scores (% correct) for the control (left panel), no-abuse stress group (middle panel), and abuse group (right panel) split by emotional valence and location. (B) Reaction times (ms) for the control (left panel), no-abuse stress group (middle panel), and abuse group (right panel), split by emotional valence and location of the stimuli. Full lines indicate match trials, dotted lines are Miss1 trials, dashed lines are Miss2 trials, and the combined dashed/dotted lines are Miss3 trials. Error bars denote standard error of the mean. Asterisk indicates significance, p < .05.
Mean (Standard Deviations) Reaction Times (in Milliseconds) and Accuracy (in % Correct) for the Control, Stress, and Abuse Group.

Note. RT = reaction time; Acc = accuracy.
The Emotion by Location interaction in the abuse group showed that in the most difficult distractor condition, the Miss1 trials, women with a history of abuse performed significantly worse for happy compared to neutral faces (p = .022; see Figure 2A). By comparison, an impact of affective valence was not present in Match trials or in easier to detect Miss2 or Miss3 trials. In the stress group, follow-up analyses for each location separately did not yield any significant main effects of emotion, although there was a slight trend in the Miss3 trials, F(2, 32) = 2.61, p = .09, partial η2 = .14. In addition, the main ANCOVA revealed a significant main effect of Location, F(3, 150) = 74.58, p < .001, partial η2 = .60, which indicated a higher accuracy for match trials and trials farthest from the target (Miss3) than for distractors closer to the target (Miss1 and Miss2 trials; all pairwise comparisons p < .001, Bonferroni corrected) regardless of Group.
To further assess the difference in responding to Miss1 happy faces in the abuse group, difference scores of emotional valence (neutral–happy) and (neutral–angry) were calculated (Figure 3). Confirming the findings from the main analysis, the (neutral–happy) accuracy difference score was significantly different from 0 in the abuse group, t(20) = 2.48, p = .022, d = 0.56, but not in the stress group or the control group. By comparison, the (neutral–angry) accuracy difference score in the Miss1 trials did not differ significantly from 0 in the abuse, stress or control group.
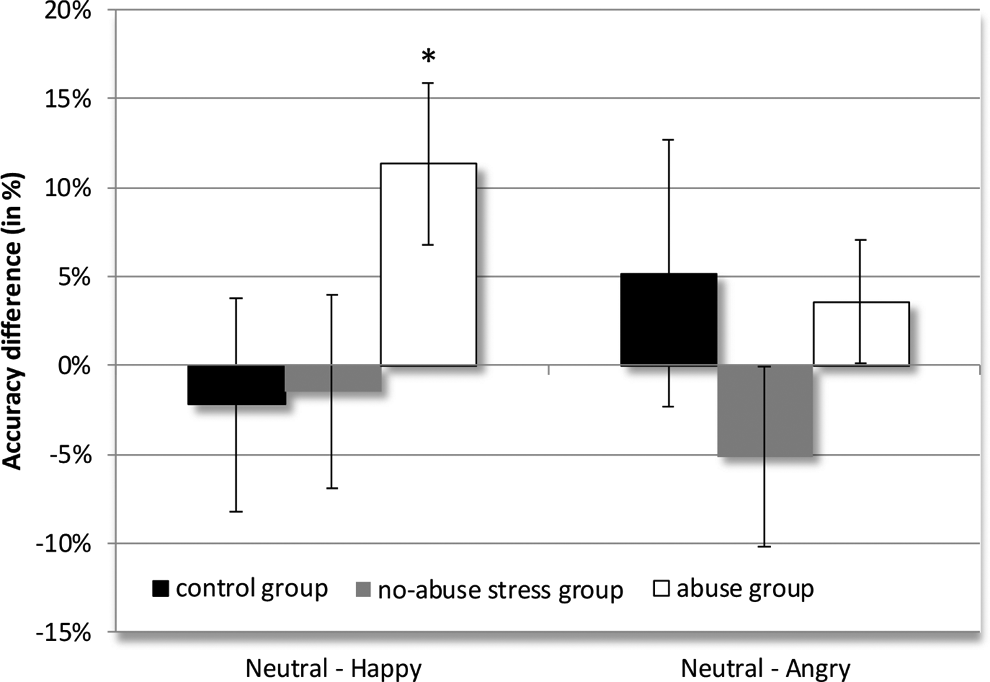
Accuracy difference scores (%) for the Miss1 condition in both the abuse and the control group. Positive scores indicate a higher accuracy for neutral faces compared to either happy (left panel) or angry (right panel) faces. The figure illustrates the decreased accuracy for happy compared to neutral faces (in the Miss1 condition) in the abuse group. Error bars denote standard error of the mean. Asterisk indicates significance, p < .05.
Reaction Time
Reaction time analysis only yielded a main effect of location, F(3, 147) = 16.17, p < .001, partial η2 = .25. Pairwise comparisons showed that participants were faster for match trials than for Miss1 (p < .001) and Miss2 (p < .001) trials. They were also faster for easier to perform Miss3 trials than for relatively more difficult Miss1 (p < .001) and Miss2 (p = .002) trials. The three-way interaction was not significant but approached conventional levels of significance, F(12, 294) = 1.60, p = .09, partial η2 = .06 (Figure 2B). No other main effects or interactions were significant (Table 3).
Exploratory Analyses of Abuse Type, Duration, Onset, and Psychopathology
Because total psychopathology scores were higher in the stress and abuse compared to the control group, we investigated whether the accuracy difference that was found between the happy and neutral faces in the Miss1 condition was due to behavior problems. The (neutral–happy) accuracy difference was not significantly correlated with the total psychopathology score (ASR) nor did it differ between participants who scored in the clinical or subclinical range and participants with scores in the normal range. When looking at the abuse, stress, and control groups separately, no significant correlations were found between the (neutral–happy) accuracy difference and the Total score, and Internalizing or Externalizing subscales in either group (all p > .05).
Additionally, we tested the association between the (neutral–happy) accuracy difference and details of the abuse, but no significant correlations were found with age of onset, duration, or frequency of abuse. We also explored whether adding age of onset, duration, and frequency of abuse as covariates had any impact on the three-way Location × Emotion × Group interaction in the abuse group. However, the three-way interaction was still significant, F(6, 90) = 2.21, p = .049, partial η2 = .13, suggesting little impact of abuse details on the main finding. Moreover, details of the abuse experience did not significantly interact with the factors Location and Emotion.
Discussion
The present study sought to provide evidence for the persistent influence of childhood maltreatment on neuropsychological functions later in life. To this goal, the influence of emotional distraction on working memory, a function implicated in emotion regulation and emotion control (Joormann & D’Avanzato, 2010; Joormann & Gotlib, 2008, 2010; Schmeichel & Demaree, 2010; Schmeichel et al., 2008), was assessed in female survivors of childhood trauma (physical and/or sexual abuse) or experience of nonabuse-related childhood stress. Two main findings pertinent to the study goal emerged. First, as hypothesized, affective valence interrupted effective working memory performance in female university students with a history of abuse. However, contrary to the hypotheses, this interruption only occurred for positive but not negative faces. Second, no interference effect was found for participants without a history of abuse or participants with nonabuse-related childhood stress.
While much previous research has documented perturbed processing of, and heightened sensitivity to, negative emotional faces in individuals with a history of abuse (Gibb, Schofield, & Coles, 2009; Masten et al., 2008; Tottenham et al., 2011), findings of effects of positive emotion on cognitive performance in this population are scarce. Indeed, the main finding of the current study demonstrated impaired working memory performance during positive faces in women with a history of abuse relative to women with nonabuse-related childhood stress or women without childhood stress. Such data suggest a detrimental impact of incidental (i.e., irrelevant) positive information on working memory accuracy. Of note, this detrimental impact was only apparent in the most difficult distractor condition (close proximity between target and distractor) but not in easier to perform distractor conditions. On the easier working memory conditions, all groups performed equally well and were insensitive to distracting affective information. Although two recent neurobiological studies failed to find differential amygdala activation for happy compared to neutral faces in relation to childhood trauma (Dannlowski et al., 2012; van Harmelen et al., 2013), these studies did not take the relationship between emotional valence and skills subserving emotion regulation into account. An interesting study by Tottenham et al. (2011) that examined the influence of amygdala activity for fearful compared to neutral faces during inhibitory control in previously institutionalized children did unfortunately not examine happy faces. However, parallel research in reward processing has documented reduced reward sensitivity in individuals with a history of abuse (Guyer et al., 2006), also failing to elevate inhibitory control performance (Mueller et al., 2012). Thus, a question for future work concerns the implications of reduced processing of positive emotion for cognitive and emotion control after ES.
Based on evidence in individuals with depression or anxiety (Epp et al., 2012; Kerestes et al., 2012; Levens & Gotlib, 2010; Visu-Petra et al., 2010) and research on emotion processing in ES (Maheu et al., 2010; Masten et al., 2008; Tottenham et al., 2011), we also expected to find an effect in negative faces. However, negative incidental emotion did not seem to impair working memory in any group. One interesting theoretical conjecture regarding the selective effect of positive stimuli could be linked to resilience. All participants in the current study were university students, thus potentially showing a selectivity bias of individuals being able to attend university despite the early trauma. Such a notion would be supported by the idea that positive emotions aid high-resilient individuals to recover from stress (Ong, Bergeman, Bisconti, & Wallace, 2006) and enhance coping resources (Tugade, Fredrickson, & Feldman Barrett, 2004). High resilience also moderates depression scores in maltreated individuals (Wingo et al., 2010) supported by psychophysiological data, which shows that hemispheric asymmetry in the electroencephalograph distinguished between resilient and nonresilient children (Curtis & Cicchetti, 2007). Thus, given that there were no significant differences between the three groups of the current study on measures of resilience, it is conceivable that a selective effect of positive emotion might be limited to high-resilient individuals relative to low-resilient individuals. However, as we had no a priori expectations with regard to this measure, current work in our laboratory is following up on this intriguing possibility.
An alternative explanation for the lack of a difference between angry and neutral faces might be differences in interpretation of neutral and negative faces in affected and comparison participants. Previous studies have found that neutral faces are not always perceived as emotionally neutral in individuals with, or at risk of, psychopathology. Masten et al. (2008) used a morphed facial identification task to examine processing of facial emotions in maltreated children. Compared to controls, maltreated children (with and without posttraumatic stress disorder) showed a heightened ability to identify fearful faces when they were morphed with neutral faces (50% neutral and 50% fearful). Additionally, depression-prone individuals misinterpret neutral faces as being sad more often than healthy controls (Leppanen, Milders, Bell, Terriere, & Hietanen, 2004). In the current study, participants in the abuse and stress group reported more depressive symptoms than healthy comparisons, which could suggest that a negative interpretation bias might increase elaboration of neutral faces and consequently improve working memory performance for neutral and negative faces together. More work on distinguishing between these possibilities is required.
As alluded to earlier, cognitive biases have been implicated in several psychopathological disorders, such as depression or anxiety disorders. For example, depression is associated with interpretation biases toward negative stimuli (Gotlib et al., 2004; Joormann & Gotlib, 2008; Levens & Gotlib, 2010), with an increased interest in therapies targeting such biases (Baert, De Raedt, Schacht, & Koster, 2010; Beard, Sawyer, & Hofmann, 2012; Britton et al., 2013; Schweizer & Dalgleish, 2011; Schweizer, Grahn, Hampshire, Mobbs, & Dalgleish, 2013). A recent study on the effect of emotional working memory training in a healthy population yielded promising results, since the training improved not only performance on the emotional working memory task but also on a transfer task measuring emotional regulation capacity (Schweizer et al., 2013). In addition, Pe, Koval, and Kuppens (2013) found that the ability to update positive material in working memory was related to well-being. Future research could examine the effectiveness of bias training when training either positive or negative information in individuals with a history of abuse.
Some limitations of the present study require discussion. One limitation certainly concerns the small sample size, even though a gradual effect of location distance on accuracy and sensitivity to incidental emotion suggests that the study group was sensitive to the task. However, due to the small sample size, the additional correlational analyses relating the (neutral–happy) accuracy difference in Miss1 trials to questionnaire results and details of abuse history should be considered exploratory. Second, while restricting the study to female participants might limit generalizability to men with a history of childhood abuse, it also constitutes a strength by excluding any possible confound of sex. A third limitation concerns the use of self-report measures. Even though the SLESQ is a well-validated instrument (Goodman et al., 1998; B. L. Green, Chung, Daroowalla, Kaltman, & DeBenedictis, 2006), we cannot exclude the possibility of recall bias. For the assessment of psychopathology, we also used a self-report measure, that is, the ASR (Achenbach & Rescorla, 2003), instead of a structured psychiatric interview. However, the emphasis of the current study was on the experience of abuse on cognitive mechanisms of emotional processing rather than clinical psychopathology. In addition, the ASR is a reliable and valid (Achenbach & Rescorla, 2003) instrument and is frequently used to assess psychopathology in young adults (Hack et al., 2004; Reef, Diamantopoulou, van Meurs, Verhulst, & van der Ende, 2010). Moreover, it detected significant differences between the two groups in experienced pathology on several scales of the ASR. Finally, because of time constraints and in order to avoid fatigue in participants, we decided to only use one positive and one negative emotional expression in the task. Even though sad faces are often used in depression research, we opted for angry faces given the heightened sensitivity of traumatized individuals to threatening information (Gibb et al., 2009; Johnson, Gibb, & McGeary, 2010; Pine et al., 2005; Pollak & Tolley-Schell, 2003). Future work could examine sensitivity to other emotional expressions.
Conclusion
The present study highlights interfering effects of positive emotion on working memory performance in women with a history of abuse relative to women with other childhood stressors or comparisons without a history of ES. These findings aim to increase awareness of history of abuse among female university students and the impact it might have on cognitive skills related to emotion control. Larger and more strongly powered studies are needed to replicate this finding to investigate how individual differences and abuse characteristics influence working memory impairment for positive information.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Ghent University (Multidisciplinary Research Partnership “The integrative neuroscience of behavioural control”).