
Abstract
There has been increasing acceptance of marijuana use in the United States in recent years, and rates among adolescents have risen. At the same time, marijuana use during adolescence has been linked to an array of health and social problems. Maltreated children are at risk for marijuana use, but the relationships among characteristics of maltreatment and marijuana use are unclear. In this article, we examine how the type and the extent of maltreatment are related to the level of adolescent marijuana use. Data analyses were conducted on a subsample of maltreated adolescents (n = 702) from the Longitudinal Studies of Child Abuse and Neglect project. Approximately half the sample had used marijuana, and maltreatment was associated with its use. Multivariate regression models showed that being male, extensive maltreatment, and peer marijuana use were associated with heavy use of marijuana. These findings suggest the importance of comprehensively assessing children’s maltreatment experiences and their peers’ drug use to help prevent or address possible marijuana use in these high-risk adolescents.
Although there is a recent trend toward legalization of marijuana use among adults that might imply little concern for marijuana use as a public health issue, marijuana has been linked to several adverse health outcomes (Hall, 2014; Volkow, Baler, Compton, & Weiss, 2014), including dependence (Swift, Coffey, Carlin, Degenhardt, & Patton, 2008), cognitive dysfunction (Meier et al., 2012), and impaired driving (Hartman & Huestis, 2013). Marijuana use has also been associated with mental health problems such as panic disorder (Zvolensky, Cougle, Johnson, Bonn-Miller & Bernstein, 2010), anxiety (Degenhardt et al., 2012; Kedzior & Laeber, 2014), and psychosis (Fergusson, Horwood, & Ridder, 2005).
Although marijuana use as compared to nonuse confers risk for various adverse outcomes in young adulthood (Ellickson, Martino, & Collins, 2004), it is especially problematic when use begins early in adolescence or is frequent (Brook, Lee, Brown, Finch, & Brook, 2011; Flory, Lynam, Milich, Leukefeld, & Clayton, 2004; Meier et al., 2012; Solowij et al., 2002; Windle & Wiesner, 2004). Adolescent marijuana users are at risk for academic difficulties (Lynskey & Hall, 2000), with users less likely than nonusers to complete high school or undertake postsecondary education, even after controlling for possible confounding variables (Homel, Thompson, & Leadbeater, 2014; Horwood et al., 2010; Palamar et al., 2014). Brain imaging studies have found structural abnormalities in gray matter density, volume, and shape of the nucleus accumbens and amygdala in 18- to 25-year-old marijuana users (Gilman et al., 2014). This finding is not unexpected given that the developing brain appears to be highly vulnerable to the effects of substance use and that the brain continues to develop into the mid-20s (Giedd, 2004). Other studies have reported a variety of neurocognitive problems among marijuana users (Hanson et al., 2010; Schweinsburg, Brown, & Tapert, 2008; Solowij et al., 2011). In the longer term, chronic heavier patterns of marijuana use predict risk for a number of psychosocial outcomes including diminished relationship quality (Brook, Pahl, & Cohen, 2008), greater need for economic assistance and occupational difficulties (Brook, Lee, Finch, Seltzer, & Brook, 2013; Fergusson & Boden, 2008; K. M. Green & Ensminger, 2006), and lower satisfaction with life (Schulenberg et al., 2005).
Despite the evidence regarding the effects of marijuana, recent national surveys have shown decreases in perceived risk concerning marijuana (Johnston, O’Malley, Bachman, Schulenberg, & Miech, 2014a), owing in part to the relaxation of state laws regarding the legality of marijuana use (Schuermeyer et al., 2014). In tandem with decreasing perceived risk, recent data show increased marijuana use by adolescents. By age 18, nearly half of American adolescents report having tried marijuana (Johnston, O’Malley, Bachman, Schulenberg, & Miech, 2014b). In 2013, 46% of high school seniors had smoked marijuana at some point, making it the most commonly used illicit drug among youth (Johnston et al., 2014a).
Among the research studies on risk and protective factors associated with marijuana use, several have focused on the impact of child maltreatment (CM), including physical and sexual abuse as well as neglect. Adults who retrospectively report having been maltreated as children are at elevated risk for drug involvement compared to individuals who have not reported maltreatment (J. G. Green et al., 2010; Kilpatrick et al., 2000; McLaughlin et al., 2010; Wu, Schairer, Dellor, & Grella, 2010). Moreover, prospective studies have found CM to be associated with drug use during adolescence (Horan & Widom, 2015; Oshri, Rogosuch, Burnette, & Ciccetti, 2011) and young adulthood (Lansford, Dodge, Pettit, & Bates, 2010; Lo & Cheng, 2007; Thornberry et al., 2014; Widom, Marmorsetin, & White, 2006). Wilson and Widom (2009) observed significant relationships between child abuse and neglect and subsequent illicit drug use in young adult women but not men. Maltreatment has been identified as a significant predictor of cannabis dependence (J. G. Green et al., 2010; Handley, Rogosch, Guild, & Cicchetti, 2015), even after adjustment for genetic vulnerability (Duncan et al., 2008).
CM is not, however, always associated with drug use, raising the question of what explains the variability in outcomes. First, the timing of maltreatment has been suggested to predict psychosocial and health outcomes. One study found that maltreatment during adolescence, as opposed to early childhood, was associated with substance use and other maladaptive behaviors (Thornberry, Ireland, & Smith, 2001). Oshri et al. (2011) reported that the severity of maltreatment in early childhood was related to adolescent marijuana abuse and dependence via poor adaptation in childhood and externalizing problems.
Dodge and colleagues (2009) described a dynamic cascade model of the development of early-onset drug use that supports the aggravating effect of early maltreatment. In contrast, other research has suggested that contemporaneous or recent maltreatment might be more predictive of substance use in adolescence and young adulthood. It has been suggested that adolescence is a period of heightened vulnerability to stress (Jankord et al., 2011; McCormick, Mathews, Thomas, & Waters, 2010), which might contribute to their risk-taking behavior (Steinberg, 2010). Persistent maltreatment that occurs during both childhood and adolescence might compound the risk for subsequent drug use (Ireland, Smith, & Thornberry, 2002).
Second, the type of maltreatment might also be a factor in the variation in drug use outcomes (Bailey & McCloskey, 2005; Moran, Vuchinich, & Hall, 2004). Neglect is the most common type of maltreatment reported to Child Protective Services (CPS). Of the 679,000 substantiated reports in 2013, 82% of the children were neglected, 18% were physically abused, 9% were sexually abused, and 9% were psychologically maltreated (U.S. Department of Health and Human Services, 2013). Just as different types of maltreatment have been associated with different child outcomes (Lau et al., 2005), physical abuse appears to be especially associated with drug use (Huang et al., 2011; Lo & Cheng, 2007; Wilson & Widom, 2009), but others found significant relationships with both physical and sexual abuse, but not neglect (Appleyard, Berlin, Rosanbalm, & Dodge, 2011). In contrast, Cheng and Lo (2010) found that sexual abuse, but not physical abuse or neglect, predicted cocaine, crack, and heroin use. In one of their studies, no relationship was found between childhood maltreatment and marijuana use after controlling for marijuana use prior to official CPS reports, parental closeness, and parent monitoring (Cheng & Lo, 2011). The influence of peers on adolescents’ drug use (Glaser, Shelton, & van den Bree, 2010; Monahan, Rhew, Hawkins, & Brown, 2014; Tucker, de la Haye, Kennedy, Green, & Pollard, 2014) requires taking this into account when examining the influence of CM on later drug use.
Despite strong support for the overall link between maltreatment and drug use, methodological limitations of previous research leave important gaps in our understanding of those characteristics of maltreatment that influence drug use. Research to date offers a mixed, uncertain picture of how characteristics of maltreatment influence adolescent drug use. Our goal in this multisite prospective study of children at risk of or reported for maltreatment was to examine whether the type, extent, and timing of their maltreatment experiences were associated with the level of their marijuana use during adolescence. To overcome some of the limitations of prior research, we utilized data from a large, multiwave and multisite prospective study of high-risk children.
The current study design affords the opportunity to fill important gaps in prior research on maltreatment and marijuana use. As indicated earlier, little research has focused on the relationship between maltreatment and marijuana use, and it has typically relied on retrospective recall in adults, failed to examine characteristics of maltreatment (e.g., Khoury, Tang, Bradley, Cubells, & Ressler, 2010), or examined outcomes in adulthood (Fergusson, Boden, & Horwood, 2008; Huang et al., 2011). In particular, prior research has rarely examined all types of maltreatment as predictors; in particular, the role of neglect has been neglected (e.g., Khoury et al., 2010). Several studies have examined the relationship between maltreatment and “substance use” as a more general class, without focusing on marijuana (Fergusson et al., 2008; Moran et al., 2004).
Method
Sample
The analytic sample was derived from the Longitudinal Studies of Child Abuse and Neglect (LONGSCAN), a consortium of five prospective studies of the antecedents and consequences of CM (Runyan et al., 1998). Although each subsample consisted of families at high risk for maltreatment as indicated by their potential or current involvement with CPS, they were deliberately varied to represent those at risk for maltreatment or already identified as maltreated. Participants were included in this sample if there were data from at least one interview indicating marijuana use or data at 18 that they had never used marijuana. Of the original LONGSCAN sample of 1,354 children, 1,041 (77%) met the inclusion criteria. Excluded participants were more likely to have been maltreated (73.5%) than those included (67.4%), χ2(1) = 4.10, p = .04. Excluded participants were more likely to be White (30.4%) and less likely to be Hispanic (16.0%) or Black (44.9%) compared to those included, 24.9%, 12.6%, and 55.8%, respectively, χ2(3) = 11.61, p = .009. LONGSCAN included children who had been maltreated as well as others who were not. Analyses were finally conducted on the maltreated subsample (n = 702).
Procedure
The consortium began common data collection when the children were 4–6 years old and gathered data from the caregivers and children every 2 years until 18 years of age (Runyan et al., 1998). CPS data were obtained by each site from the local or state agency at regular intervals. Each site employed procedures approved by its local institutional review board. Families were paid a nominal amount for their participation to compensate for their time and travel.
Measures
Maltreatment
A participant was defined as maltreated if the review of CPS data reports reviewed by the LONGSCAN project (Runyan et al., 1998) indicated one or more reports from birth to18 years of age. English, Bangdiwala, and Runyan (2005) describe in detail the identification of maltreatment from CPS records. In sum, trained observers at each site reviewed CPS records every 2 years and collected information about allegations of abuse and neglect. These allegations were categorized according to a modified version of the Maltreatment Classification Scheme (Barnett, Manly, & Cichetti, 1993). The decision to use allegations instead of substantiated reports was based on earlier research on LONGSCAN participants. Hussey et al. (2005) found that children with substantiated and unsubstantiated CPS reports had similar behavioral and developmental outcomes. Other researchers have also suggested that there is not a useful distinction between substantiated and unsubstantiated cases (Kohl, Jonson-Reid, & Drake, 2009).
Characteristics of maltreatment
Maltreatment experiences were further characterized for those in the maltreated subsample (n = 702; Table 1). The type of maltreatment was classified as physical abuse, sexual abuse, emotional maltreatment, or neglect (English, Graham, Litrownik, Everson, & Bangdiwala, 2005). Each type of maltreatment was coded dichotomously, and children could be classified as having experienced more than one type of maltreatment.
Bivariate Relationships Between Characteristics of Maltreatment and Level of Marijuana Use.

Note. n = 702. CM = child maltreatment; CPS = Child Protective Services.
aχ2 (3, k) of Marijuana Use (No/Some/Heavy) × Characteristic (k). bExtent defines limited as CPS reports in one developmental period and fewer than five reports. Extensive represents CPS reports in more than one developmental period and more than five reports.
The chronicity of maltreatment was defined by the number of developmental periods during which at least one report was made: 0–5, 6–11, and 12–18. The frequency of maltreatment was defined as either low (1–5 reports) or high (6 or more) between the ages of 0 and 18 years. Chronicity and frequency as well as timing of CPS reports were highly correlated, so we created a summary variable—extent of CM. Individuals with limited maltreatment (44%, n = 309) were defined as those who had CPS reports in only one developmental period and had low frequency of reports (mean = 2.0). Those who experienced extensive maltreatment (56%, n = 393) were maltreated in more than one developmental period (median = 2) or had high frequency of CPS reports (Mean = 7.2).
Peer marijuana Use
At ages 12, 14, and 16, participants were asked whether any of their friends used marijuana (n = 911). If at any interview participants indicated yes, they were counted as having had peer use (n = 437, 48%). If during at least two interviews participants indicated that their friends did not use marijuana (and never described their friends as using), they were counted as no peer use (n = 474, 52%).
Level of adolescent marijuana use
Participants were first classified as having used marijuana if use was reported at any of the age 12, 14, 16, and 18 interviews. Nonuse was defined by indicating at 18 that they had never used marijuana (never used marijuana). Adolescents who never indicated marijuana use and who did not complete the age 18 interview were considered to have missing data and were excluded. Those who reported marijuana use were further categorized by level of use. Heavy use was defined as reports in at least one interview of (1) use on more than 20 days in the last year or (2) use more than 10 times in the last month or (3) meeting criteria for substance dependence or abuse per the National Institute of Mental Health Diagnostic Interview Schedule for Children version IV at age 14 or 18.
Data Analyses
The goal of the present study was to understand the maltreatment characteristics that predicted the level of marijuana use during adolescence. A correlation matrix including the maltreatment variables as well as peer use (see Table 2) shows that the correlations were modest to moderate, ranging from −.09 to .48. Thus, multicollinearity was of minimal concern and allowed us to develop a model that included multiple dimensions of childhood maltreatment. Multinomial logistic regression analyses were conducted, with site and race/ethnicity as covariates. Site included the five research centers with Northwest as the reference. Race/ethnicity was coded in four categories (Black, Hispanic, Other, and White), with White as the reference group. Peer use was used as a covariate in some models with no peer use as the reference. In a preliminary analysis of the covariates as predictors of level of marijuana use, participant sex was found to be significantly related to the level of use and therefore was included in each model. Next, a model was developed that included all variables except peer use (Model 1) followed by a model that included peer use (Model 2).
Correlation Matrix of the Maltreatment and Peer Use Predictor Variables.
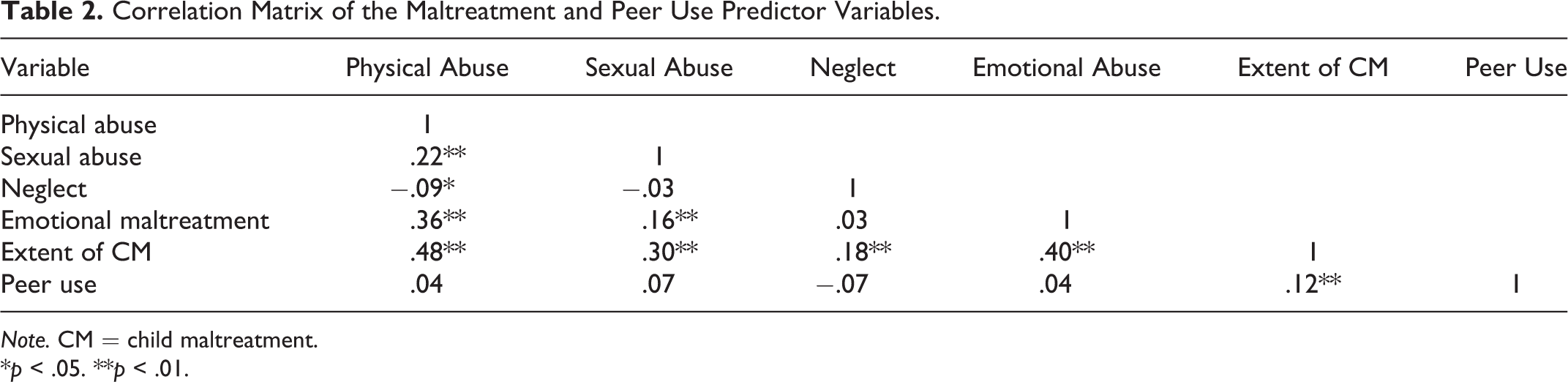
Note. CM = child maltreatment.
*p < .05. **p < .01.
Results
CM was associated with marijuana use. Specifically, a greater percentage of maltreated youth reported any marijuana use (53%) compared to those who had not been maltreated (36%, p = <.001). Maltreated youth were more likely to report both some use (31% vs. 22%) and heavy use (22% vs. 14%). Table 3 summarizes characteristics of the maltreated subsample (n = 702). Females were less likely than males to engage in heavy use (16% vs. 28%, p = .001). Marijuana use did not differ significantly according to race/ethnicity or study site.
Sample Characteristics by Level of Marijuana Use Among Maltreated Youth.
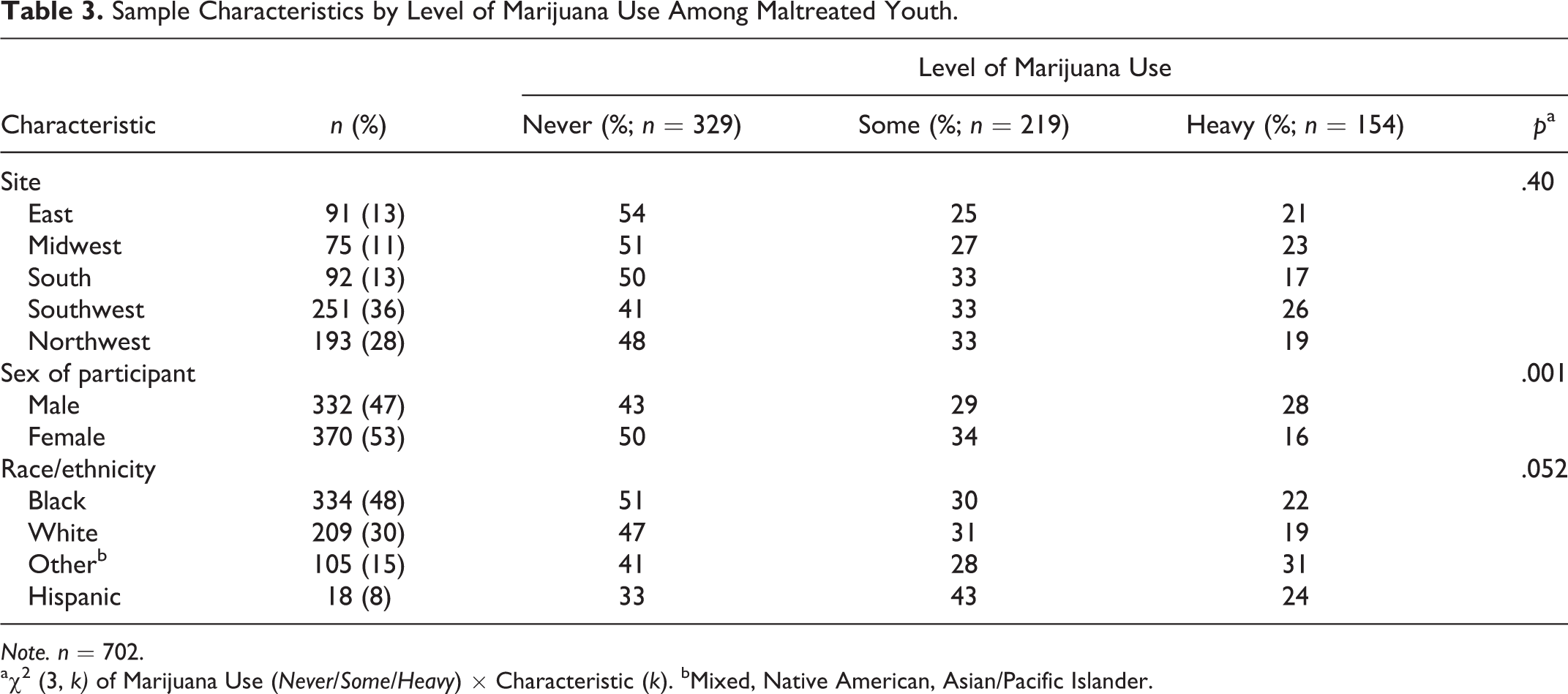
Note. n = 702.
aχ2 (3, k) of Marijuana Use (Never/Some/Heavy) × Characteristic (k). bMixed, Native American, Asian/Pacific Islander.
The bivariate relationships between maltreatment characteristics and marijuana use are shown in Table 1. Regarding maltreatment type, physical abuse was significantly associated with heavy use of marijuana and sexual abuse primarily with some use. More extensive CM was significantly associated with heavy use. Emotional maltreatment and neglect did not predict marijuana use. The tolerance ranged from .63 to .99 and the variance inflation factor (VIF) ranged from 1.01 to 1.44, indicating that multicollinearity among the maltreatment variables was of little concern.
All of the characteristics of maltreatment and covariates were jointly examined (Table 4). In Model 1, sexual abuse predicted some use of marijuana, and extensive CM was associated with heavy use. Females were more likely than males to be reported for sexual abuse (38% vs. 17%), χ2(1) = 40.35, p < .001, and they are more likely to have some use than heavy use. When peer use was added in the regression (Model 2), it is strongly predictive of marijuana use, and being male and having experienced extensive CM also are associated with heavy use of marijuana.
The Relationships Among Maltreatment Characteristics and Level of Adolescent Marijuana Use, Controlling for Site, Participant Sex, and Race/Ethnicity.
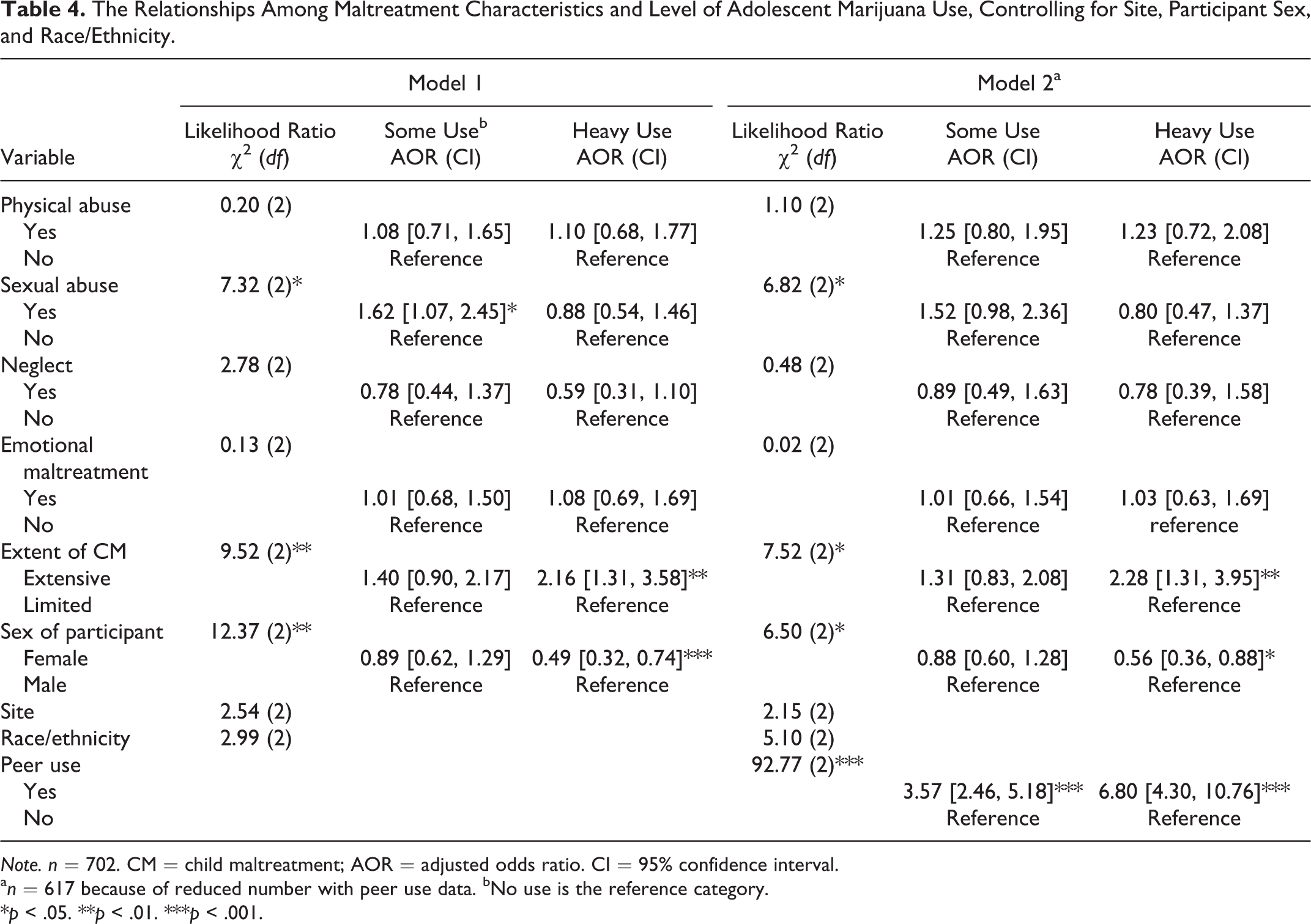
Note. n = 702. CM = child maltreatment; AOR = adjusted odds ratio. CI = 95% confidence interval.
a n = 617 because of reduced number with peer use data. bNo use is the reference category.
*p < .05. **p < .01. ***p < .001.
Discussion
This study adds important information to our understanding of the characteristics and predictors of marijuana use in vulnerable populations of children who are at risk or reported for maltreatment. Although not generalizable to the broader U.S. population of adolescents, these data are valuable because “at-risk and/or maltreated adolescents have an increased likelihood of using illicit drugs” (Braciszewski & Stout, 2012). As such, studying marijuana use within such high-risk populations has the potential to better elucidate the relative contributions of maltreatment and other risk factors such as peer use. As well, reported maltreatment is associated with a host of risk behaviors, and the pattern of predictors for each risk behavior is somewhat different (Courtney & Dworsky, 2006).
This study is consistent with earlier research and extends it by providing information about the effects of different characteristics of reported maltreatment and their relative influence in the context of peer use. Maltreatment was associated with marijuana use in bivariate models but did not retain significance in models that adjusted for peer marijuana use. In terms of type of maltreatment, sexual abuse predicted marijuana use. This finding is consistent with earlier research (Fergusson et al., 2008; Moran et al., 2004), which found that physical abuse and sexual abuse (and these combined) predicted substance abuse or dependence, although not specifically marijuana use. Physical abuse has also been found to predict earlier onset of substance use in young adolescents (Lansford et al., 2010). Those who experienced extensive maltreatment were more likely to report heavy use of marijuana. This finding is consistent with research suggesting the importance of both early (e.g., Dodge et al., 2009) and recent (i.e., adolescent) exposure to maltreatment (e.g., Thornberry et al., 2001). It appears likely that persistent exposure to maltreatment carries an especially high level of risk for adolescent substance use (Thornberry et al., 2014). Indeed, extensive CM was the one characteristic that significantly predicted adolescent marijuana use, after taking into account demographic variables and peer use.
Future research should focus on better understanding the mechanisms by which physical and sexual abuse influence youth adolescent risk-taking behaviors in general and marijuana use in particular. It is likely that adolescent (and earlier child) emotional functioning is a key contributor, as it has been shown to influence other effects of CM on risk behaviors (e.g., Oberlander et al., 2011; Thompson & Neilson, 2014). However, more detail is needed in terms of the specific pathways from particular characteristics of maltreatment, to particular deficits in emotional or psychological functioning, to risk for marijuana use. As well, it is likely that for many adolescents, marijuana use is only one of a cluster of risk behaviors that are part of a larger syndrome of risk taking (Monshouwer et al., 2012). From this perspective, peer use may have a more complex relationship with marijuana use than elucidated here (Monahan et al., 2014). Peer use appears to mitigate or possibly mediate the effects of reported maltreatment in these analyses. However, in terms of understanding this relationship, it is likely that maltreatment is one link in a chain that comprise a risk “caravan” for use of illicit drugs (Layne, Warren, Watson, & Shalev, 2007). The social development model described by Catalano, Kosterman, Hawkins, Newcomb, and Abbott (1996) incorporating the effects of empirical predictors, or risk factors, in the development of antisocial behavior may help illustrate the roles peers played in this study. The model also incorporates protective factors, for example, peers not using marijuana may moderate the effects of CM. This potential protective role was not evident in this study.
The results of the current study are largely consistent with several previous investigations showing an increased risk of problematic marijuana use among maltreated children as compared to their nonmaltreated counterparts (Duncan et al., 2008; Handley et al., 2015; Lo & Cheng, 2007; Oshri et al., 2011; Widom et al., 2006; Wright, Fagan, & Pinchevsky, 2013). This was true regardless of whether youth were sampled from the general population or identified from administrative records, and whether marijuana problems were operationalized utilizing a standardized instrument such as the Diagnostic Interview Schedule - Children (DISC) or a frequency measure such as in the current study. Findings regarding the dimensions of maltreatment that are related to marijuana use are mixed, with some studies observing a significant relationship with sexual abuse (Duncan et al., 2008) and others with physical abuse (Lo & Cheng, 2007). The current finding that maltreatment that occurred in multiple developmental periods is more strongly predictive of marijuana use than limited exposure to maltreatment supports prior research findings indicating that the severity or chronicity of maltreatment might have greater explanatory value rather than the type of maltreatment (Lo & Cheng, 2007; Oshri et al., 2011). The present study also highlights the utility of the ecological-transactional framework as a model for understanding the complex relationship between childhood maltreatment and substance use (Oshri et al., 2011), where the interaction between individual-level factors with characteristics of the broader environment can increase the risk of expression of various adverse outcomes of maltreatment. The current study revealed the importance of peer drug use on risk for marijuana use frequency and found that the prospective association between the extent of maltreatment and marijuana use was robust even after including peer drug use. This finding extends what was observed by Huang et al. (2011), where both maltreatment and peer drug use were significantly associated with drug-related problems. Future research is needed to attain an even more complete picture of the various mechanisms by which CM exerts its adverse effects. For example, Handley et al. (2015) observed that neighborhood disadvantage conferred risk for marijuana dependence symptoms more strongly for maltreated children than nonmaltreated children.
In interpreting these findings, there are several limitations that should be kept in mind. First, it is important to acknowledge that the assessment of maltreatment based on CPS reports has clear limitations including bias as to who gets reported and investigated. As well, the extent of maltreatment is important to consider, although the chronicity component used relatively broad developmental periods (0–5, 6–11, and 12–17). Despite the usefulness of these periods in prior LONGSCAN research (e.g., Flaherty et al., 2009; Thompson et al., 2012), future work should examine this in a more nuanced way (English et al., 2005). Similar refinements could be made in the measurement of other variables. For example, missing data on peer marijuana use were addressed by coding those with no peer use at at least 2 time points as “no peer use,” which was an imperfect, but necessary, compromise. Given the uncertain chronology of events, it was not possible to ascertain whether predictors directly triggered the use of marijuana or whether there were other intervening factors.
With these caveats, this study’s findings, especially given earlier research, strongly suggest that children exposed to physical and sexual abuse are at increased risk of marijuana use. Child-serving professionals should begin to integrate the findings from this and other studies into discussions about effective interventions to decrease the likelihood of vulnerable populations engaging in illicit drug use—in this case, marijuana. Prior research suggests the importance of primary prevention and early intervention. Adolescents who use substances have been found to increase their use during adolescence (Brown et al., 2008; Maggs & Schulenberg, 2005). This may be part of a risk taking or emotional coping approach common among adolescents with maltreatment experiences (Thompson et al., 2011). Alternatively, recent research with veterans has highlighted the possibility that use of marijuana may be a form of self-medication of some symptoms of post-traumatic stress disorder (Bonn-Miller, Vujanovic, & Drescher, 2011), and our findings are consistent with this possibility as well. In any case, earlier studies have found that maltreatment and other adverse childhood experiences increase the likelihood of future substance use well into adulthood (Aarons et al., 2008; Dube, Felitti, Dong, Giles, & Anda, 2003; Fergusson et al., 2008; Huang et al., 2011). Therefore, it is important to disrupt these potential trajectories at the earliest possible stage.
Since many adolescents who have experienced maltreatment and use substances are involved in the child welfare system, these findings have both policy and practice implications. The findings emphasize the importance of both comprehensive and accurate assessments including the extent of a child’s maltreatment as well as possible peer marijuana use. Such assessments are necessary to guide effective prevention and/or intervention for adolescents already using marijuana or considering its use. Maltreated males are at particularly high risk for heavy use of marijuana and likely require added support, interventions, and monitoring. There are also opportunities for screening and early intervention to detect and address marijuana use and related problems for maltreated adolescents in the child welfare system, particularly when there are such opportunities for children in Independent Living programs. Pediatric primary health care visits offer another opportunity where more frequent visits may be scheduled to support adolescents and to monitor their health risk behaviors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by grants from the Office of Child Abuse and Neglect, Administration on Children and Families, U.S. DHHS (Grants Nos. 90CA1401, 90CA156901, 90CA1681, and 90CA1749), and the National Institute on Drug Abuse (Grant no. 5R01DA031189-04).