
Abstract
Women who experience childhood sexual victimization (CSV) report more problems with sexuality and with parenting during adulthood. Consequently, mothers with a CSV history may have particular difficulty with parent–child sexual communication. We examine this possibility in 184 diverse, low-income mother–adolescent daughter dyads. Mothers and daughters reported on the frequency, tone, and comfort of their sexual communication. Using dyadic approaches to analyses, we tested whether mothers’ and daughters’ reports, and their level of agreement, differ by maternal CSV history. In dyads with maternal CSV, daughters reported more frequent communication in which they felt less embarrassed, and they perceived their mothers as less embarrassed. Mothers with a CSV history were also more accurate in judging how their daughters feel during sexual communication. Although CSV is associated with many negative outcomes, our results suggest mothers with CSV may approach mother–daughter sexual communication in ways that could reduce sexual risk in offspring.
Approximately 19% of women experience some kind of sexual abuse or victimization by the age of 18 (Pereda, Guilera, Forns, & Gómez-Benito, 2009). Experiencing childhood sexual victimization (CSV) increases the likelihood for physical and mental health problems in adulthood (Fergusson, McLeod & Horwood, 2013), including differences in sexually related behaviors and beliefs (e.g., Lorenz & Meston, 2012). Given these differences, CSV history may impact how women navigate the sexual development of their children. Cavanaugh and Classen (2009) proposed a conceptual model delineating parent–child sexual communication (PCSC) as a primary pathway from parental CSV to offspring sexual risk. However, few studies have examined whether maternal CSV is related to differences in PCSC. Our study examined this question in a sample of 184 diverse, low-income mother–daughter dyads.
PCSC
Talking about sex is difficult in most families (Jerman & Constantine, 2010). As a result, numerous interventions have been developed to improve the frequency and quality of PCSC with the goal of reducing sexual risk (Santa Maria, Markham, Bluethmann, & Mullen, 2015). Although findings on PCSC and offspring sexual behavior have been somewhat mixed (see review, DiIorio, Pluhar, & Belcher, 2003), the majority of intervention studies indicate that more frequent and open parent–child communication is associated with later sexual initiation and more consistent condom use (for review, see Coakley et al., 2017). In these studies, the effectiveness of PCSC depends on the frequency, valence, and content of communication, as well as parent’s comfort and knowledge in these discussions.
Few studies have examined maternal CSV and PCSC, although there are reasons to expect these dyads may differ. In qualitative research, mothers with CSA report a desire to protect their children and a fear of being triggered by discussing sexuality, yet they also describe teaching their children about saying no to unwanted advances (Wright, Fopma-loy & Oberle, 2012). In empirical studies, women with a CSV history report more permissive or negative sexual attitudes (Randolph & Mosack, 2006), use more negative and fewer positive words when communicating about sex (e.g., Lorenz & Meston, 2012), and show attentional biases when processing sexually relevant information (Latack, Moyer, Simon, & Davila, 2017). Together, these findings indicate that mothers with CSV may differ in how they think and talk about sex, although the way these differences would impact PCSC is unclear (e.g., more or less frequent conversations). If sexual communication is less frequent or more negative in families in which a mother has a CSV history, this may be an important group to target in PCSC interventions.
One challenge to the study of PCSC is whose perspective is assessed. Agreement between parents and adolescents about the frequency or nature of sexual communication is generally low, with mothers tending to report more communication than daughters (e.g., Guilamo-Ramos, Jaccard, Dittus, & Collins, 2008), though adolescents’ reports are more strongly associated with sexual behavior (DiIorio et al., 2003). Parent–adolescent reporting discrepancies may be largest in higher risk families (Rote & Smetana, 2016). In addition, a mother or daughter’s comfort talking about sex could differ from how comfortable they appear to the other person. Both feeling uncomfortable and perceiving the other as uncomfortable could deter from conversations. For these reasons, it is important for studies of PCSC to include the perspective of both partners. Using dyadic data, the goal of this study was to examine whether aspects of PCSC differ when a mother has experienced CSV. Specifically, we test for differences in (1) the frequency and tone of sexual communication as reported by both members and (2) how comfortable mothers and daughters report being and how comfortable they view one another.
Method
Participants and Procedures
Study participants included 184 mother–adolescent daughter dyads residing in a midsized, economically depressed city in the Northeast United States. Families were participating in a National Institutes of Health funded, cross-sectional, mixed-methods study aimed at understanding the cultural and relational context of health disparities among adolescent girls. The study focused only on adolescent girls because they are disproportionately affected by reproductive health disparities. Adolescents were in 9th or 10th grade (M = 15.4 years old, SD = 1.05); mothers averaged 41.5 years old (SD = 8.03). Fifty-one percent were Latina, 27% African American, and 20% non-Hispanic White. Educationally, 22% of mothers did not finish high school (HS), 67% had a HS degree, and 11% had a bachelor’s degree. The biological father lived in the home in 36% of families. Families were recruited from schools, community social service agencies, YWCA, and local media outlets through distribution of flyers, advertisements, and referrals. Mothers and daughters separately participated in 2-hr interviews including measures completed using Audio Computer-Assisted Self-Interview in English (80%) or Spanish (20%). The University of Connecticut Institutional Review Board approved study procedures. Participants received 40 USD each.
Measures
Demographic
Mothers provided demographic information on race/ethnicity, family structure, immigration history, and financial resources. Although all families would be considered “low income” based on definitions by the National Center for Children in Poverty (see http://www.nccp.org/profiles/US_profile_6.html), a socioeconomic status (SES) risk composite (no HS degree, in public housing, receipt of free lunch) was computed to capture variations in economic disadvantage within this group.
Maternal history of CSV
After reporting on lifetime exposure to 10 potentially traumatizing events, mothers were directed to think back to their childhood before the age of 18, with cues given to remind them of those years (e.g., remember when you were in school). After this prompt, they answered “did anyone do something sexual to you against your will?” Although retrospective reports of abuse can be biased (e.g., mood effects on memory), this type of report has demonstrated reliability (Fergusson, Horwood, & Boden, 2011) and validity (Widom & Courtois, 1997).
Mother–daughter sexual communication
Mothers and adolescents answered parallel items about communication in seven areas (e.g., sex, substance use, schoolwork); responses to items on sex were used in this study. Participants rated “how frequently do you and your (mother/daughter) talk about sexual activity or sexually related topics (e.g., birth control)” on a 4-point Likert-type scale (never to very frequently). Those who reported any communication were asked about the tone on a 5-point scale (very negative to very positive) of these conversations. To assess discomfort, participants were asked “how embarrassed do/would you feel talking to your mother/daughter about sex” and “how embarrassed do you think your mother/daughter feels/would feel” in these conversations using a 5-point scale (not at all to very much).
Adolescent sexual behavior
Adolescents answered 11 items about sexual activity. The current study used whether or not they had had sexual intercourse (yes/no) as a covariate since this may impact parent–adolescent communication about sex.
Data Analytic Plan
Using SPSS 20, t tests were used to test for CSV group differences in communication frequency, tone, and embarrassment (self-report and perceived in other). Repeated measures analyses of covariance (ANCOVAs) were used to test whether dyads with and without maternal CSV differed in mother versus daughter reports on communication variables. A statistically significant interaction between CSV and reporter indicates group differences in agreement by CSV history.
Results
Preliminary analyses examined the group differences in demographic factors associated with CSV. CSV was not significantly related to race/ethnicity, presence of biological father in the home, or the SES risk composite. These demographic factors were also unrelated to communication variables. Communication variables were associated with teen sexual behavior, but the percent of girls reporting they were sexual active did not differ significantly by maternal CSV history, 32% in CSA group, 25% in the non-CSA group, χ2(1, n = 184) = 1.03, p = .31.
Mean scores for communication frequency, tone, self-reported embarrassment, and perceived embarrassment of partner by CSV history are presented in Table 1. Results from repeated measures ANCOVA for each of these variables are presented in Table 2. For frequency, there was a significant reporter by CSV interaction, meaning agreement on the frequency of communication differed by CSV history. As reported in Table 1, daughters of mothers with CSV reported significantly more frequent communication than other girls, although mothers’ reports did not differ. As a result of this difference, mothers with CSV showed more agreement with their daughters on reported frequency, whereas mothers without CSV overestimated how frequently they talked about sex relative to their daughters’ reports. For communication tone (i.e., how positive communication is), there was only a main effect of reporter, with daughters viewing conversations as more negative than their mothers did.
Group Differences in Sexual Communication Frequency, Valence, and Comfort in Families With and Without a Maternal CSV History.
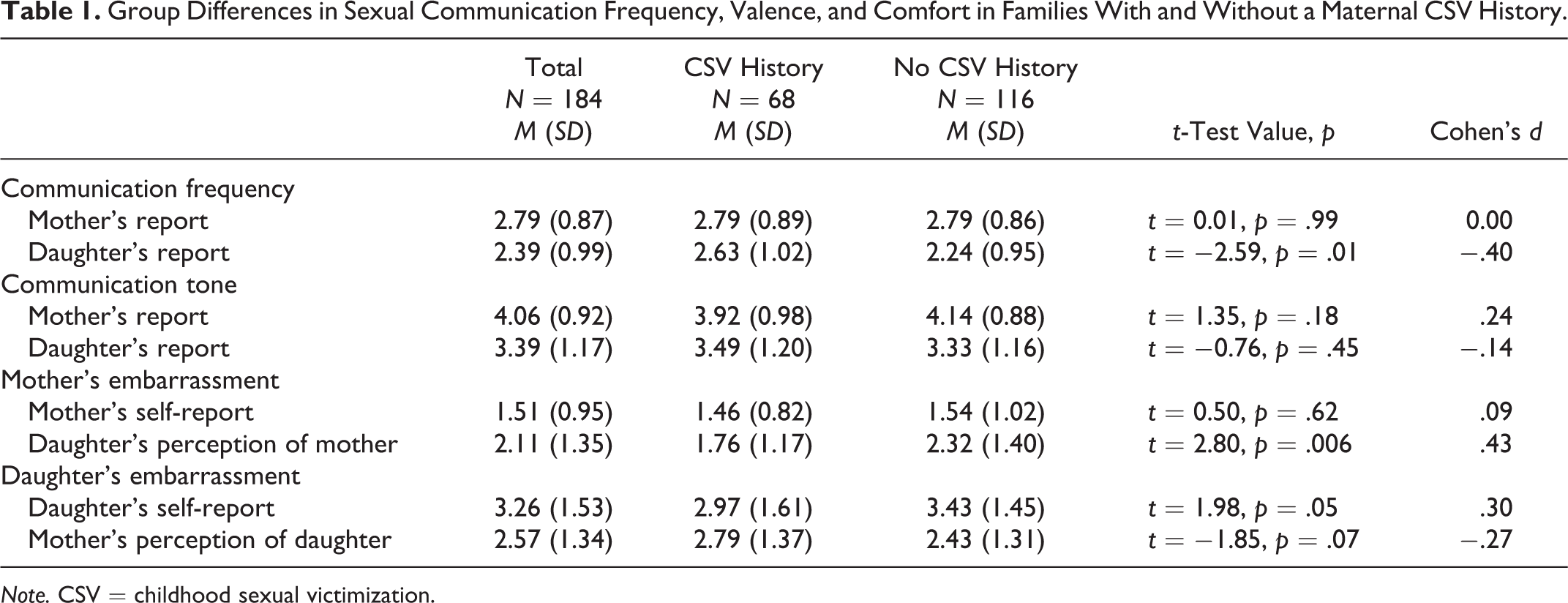
Note. CSV = childhood sexual victimization.
Results From Repeated Measures Analysis of Covariance Testing Differences in Mother and Daughter Reports of Communication Domains by CSV History.
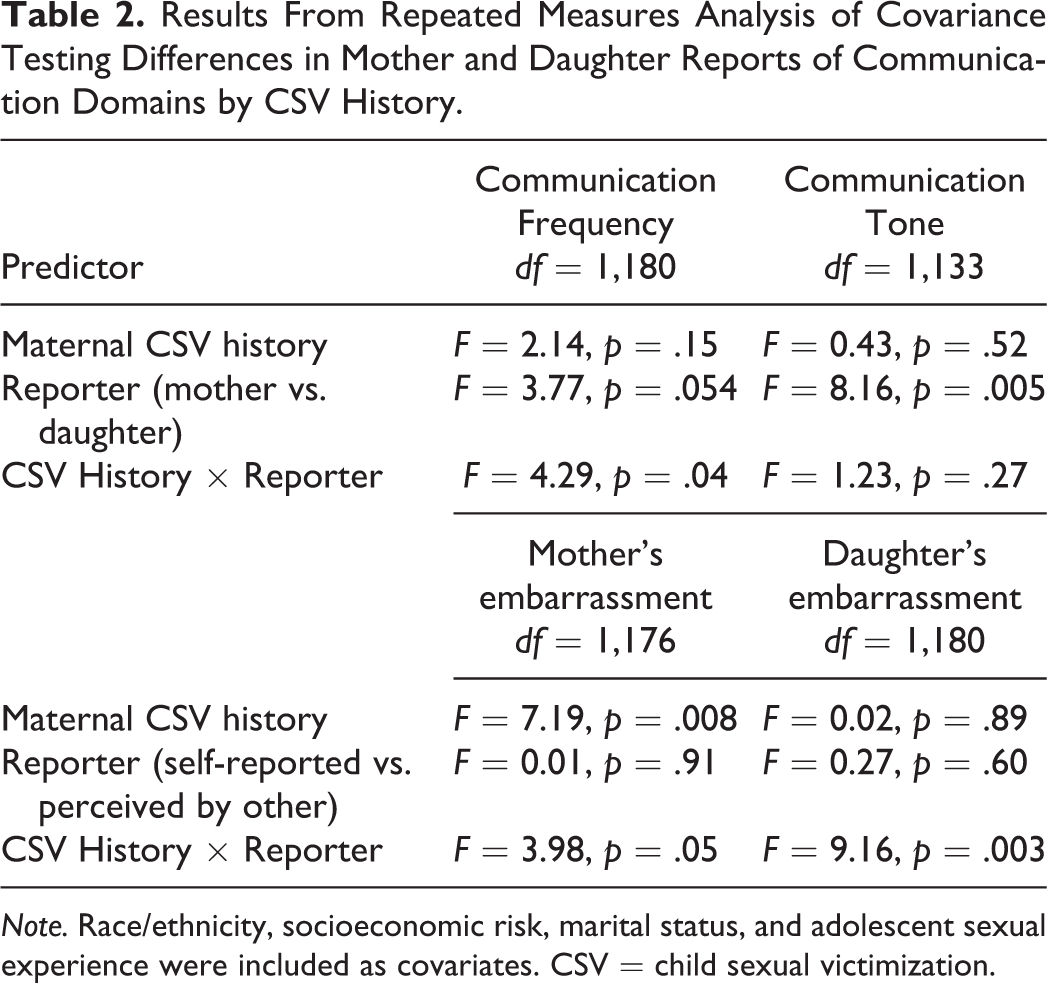
Note. Race/ethnicity, socioeconomic risk, marital status, and adolescent sexual experience were included as covariates. CSV = child sexual victimization.
There were also CSV group differences in felt and perceived discomfort talking about sex. Families with a history of maternal CSV endorsed less maternal embarrassment. When the reporter was considered, mothers with a CSV history were perceived as less embarrassed by their daughters. For adolescent embarrassment, daughters with maternal CSV reported less embarrassment (see Table 1), and their mothers were more accurate judges of how they felt. In contrast, mothers without a CSV history underestimated how embarrassed their daughters felt. Figure 1 illustrates the difference scores in mother and daughter reports by CSV group.

Mean difference scores between mothers and daughters’ reports on communication frequency, communication tone, and mothers and daughters’ discomfort. Difference scores reflect the difference between reporter scores (e.g., mother report minus daughter report of frequency).
Discussion
Maternal CSV was associated with differences in PCSC as reported by mothers and adolescents. Adolescents whose mothers experienced CSV reported talking with their mothers more frequently than peers, and these dyads showed more agreement in their reports. Other studies (Guilamo-Ramos et al., 2008) have found that mothers overestimate how much they talk about sex relative to daughters’ reports; our findings suggest this bias may be less evident when a mother has experienced CSV. Interestingly, group differences were significant from the adolescents’ perspective, suggesting these daughters may attend to or remember conversations more or have a broader range of what they consider sexual topics. There were no differences in tone (i.e., how positive communication felt) by CSV history.
There were also CSV group differences in how comfortable mothers and daughters felt discussing sex and in how they judged the other’s comfort level. Although mothers did not differ in self-reported embarrassment, mothers without CSV were viewed as more embarrassed by their daughters. These mothers may be exhibiting discomfort without realizing it, which could influence how likely a child is to initiate conversations. Alternatively, daughters may attribute limited communication to maternal embarrassment. In terms of adolescent discomfort, daughters generally reported feeling more embarrassed than their mothers assumed they felt, but this discrepancy again differed by maternal CSV. Daughters of mothers with CSV history were less embarrassed, and their mothers were better judges of how embarrassed their daughters felt. One possibility is that experiencing CSV increases a mother’s recognition or empathy for how uncomfortable it can be for adolescents to talk about sexual topics with a parent.
In sum, our results suggest that mothers with a CSV history may approach PCSC in ways that could make discussions more effective: They talk more frequently, seem more comfortable, and may have better recognition of how their daughter is feeling. Although CSV is associated with a range of negative outcomes, some mothers with this history may view openness in managing their daughter’s sexuality as a way of reducing the likelihood that she will also experience adverse sexual events (Wright et al., 2012).
Results should be interpreted in light of study limitations including the cross-sectional design, limited information on the content of communication, and a relatively small sample. Further, the measurement of CSV was not behaviorally based, which could have lowered endorsement. This measure also does not capture heterogeneity in CSV; research on how characteristics such as revictimization and level of recovery impact PCSC is needed. Finally, this study should be replicated with sons to examine how CSV history impacts mother–son conversations. Despite these limitations, this study adds to the literature on PCSC by using a dyadic approach in a community sample to examine communication among low-income, diverse adolescents, who disproportionately experience negative sexual health outcomes. Our findings raise the possibility that mothers who experienced CSV try to communicate about sex in ways that decrease sexual risk in their own daughters. Family-based interventions could harness the strengths (frequency and comfort) of CSA dyads in PCSC to help other families. More broadly, interventions that incorporate family members and consider potential intergenerational effects on adolescent sexual health may result in the best outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was conducted with support from National Institute of Health-National Institute of Child Health and Human Development (R21HDO65185).