
Abstract
Victimization is common inside prisons and much remains unknown about the predictors of violence against incarcerated women. A sample of 564 incarcerated women was used to examine the link between in-prison victimization, childhood (physical, sexual, and emotional) harm, and mental illness. Nearly half or more of women reported childhood harm and over one-quarter experienced in-prison victimization. Childhood harm fell into four latent classes and low sexual abuse and high abuse classes predicted resident-on-resident sexual victimization, as did single types of childhood harm. Current depressive symptoms and perceptions of overcrowding predicted physical and sexual victimization perpetrated by residents and correctional staff.
Introduction
Victimization and violence are terms that are often used to describe the prison experience. Violence against women while they are incarcerated has been increasingly documented by human rights groups (Amnesty International, 2011; Human Rights Watch, 1996) and within the scientific literature (Wolff, 2018). This evidence is clear: Victimization is a frequent and varied part of the prison experience for women, and it takes a toll on their emotional and physical wellness (Wolff & Shi, 2010). What remains less clear is what predicts victimization inside prison. Specifically, what makes a particular woman a target for harm? In the criminal justice literature, theories of importation (risks are carried into the prison by the individual) and deprivation (risks are created by the harshness of the prison) have been used to answer the question: Why are incarcerated women a target for harm? (Lahm, 2015). These theoretical explanations have focused attention on the resident's age, race, ethnicity, and criminal history (importation) and prison conditions, such as overcrowding, security level, programming, demeanor of staff (deprivation) (see Steiner et al., 2017). This literature presumes, without justification, that risks for victimization are different for incarcerated and nonincarcerated women simply because these women are located in different settings. This article questions the bifurcation of risk modeling of victimization of women by setting.
Victimization of women living in the community has been studied extensively. This expansive literature addresses the question of why a particular woman is targeted for harm. According to this literature, the only covariates that have consistently predicted victimization of women are witnessing parental abuse as a child for physical victimization (Hotaling & Sugarman, 1986) and childhood sexual abuse for sexual victimization (Koss & Dinero, 1989). Data from the Centers for Disease Control and Prevention–Kaiser adverse childhood experience (ACE) study have more recently revealed a solid and strong association between ACEs (inclusive of directly experiencing childhood violence, abuse, neglect, or family dysfunction, or witnessing violence in the home or community) and sexual victimization in adulthood (Ports et al., 2016).
A number of theoretical explanations have evolved over time to explain victimization of women (see Etherington and Baker, 2017). Vulnerability, according to von Hentig’s (1948) typology of victims, is a major risk factor for victimization. He identified traits of vulnerability to include female, young or old age, mental illness, cognitive impairment, and depressive symptoms. Yet, more recently, with contributions from the disciplines of biology and neuroscience, a life-course, ecobiodevelopmental (EBD) explanation of revictimization has advanced. This explanation emphasizes changes in the brain and adaptive learning that often are consequences of childhood abuse (American Academy of Pediatrics, 2012). In similarity with the importation and vulnerability explanations, the life-course EBD model suggests that the effects of stressful and traumatizing experiences in childhood are transmitted across time through changes in brain architecture and stress responsivity in ways that elevate vulnerability risks for a host of adverse outcomes in adulthood, including revictimization.
In this article, we test the different explanations for victimization using self-report data drawn from a single women's prison. To predict in-prison victimization, we first use traditional importation/deprivation covariates, then add traditional vulnerability covariates—mental illness and depressive symptoms, followed by childhood physical, sexual, and emotional harm covariates. Our aim is to identify robust predictors that make theoretical sense and that have instrumental utility to prevent violence against incarcerated women.
Literature Review
During incarceration, women may experience physical and sexual harm (Centers for Disease Control and Prevention, 2002) that is perpetrated by other incarcerated women (referred to as “residents”) or correctional staff. Physical violence, compared to sexual violence, is most commonly reported by incarcerated women during their confinement. Based on self-report surveys administered in the United States and other countries, six-month prevalence estimates for physical violence against incarcerated women by other residents range from 6% (Wooldredge & Steiner, 2014) to ∼21% (Caravaca-Sánchez & Wolff, 2016; Lahm, 2015; Wolff et al., 2007). Rates for physical violence perpetrated by correctional staff are slightly lower, varying from 8% (Wolff et al., 2007) to 17% (Caravaca-Sánchez & Wolff, 2016). When rates of physical violence against incarcerated women are combined for both perpetrator types, roughly one in four incarcerated women report experiencing some form of physical violence during a six-month period (Caravaca-Sánchez & Wolff, 2016; Wolff et al., 2007).
Relative to physical violence, sexual violence against incarcerated women has been studied more extensively but also with greater methodological variability. Some studies have focused on either unwanted sexual contact or sexual assault (Blackburn et al., 2008; Butler et al., 2002; Hensley et al., 2003; Lahm, 2015; Struckman-Johnson & Struckman-Johnson, 2006; Walsh et al., 2012), while others separately probed sexually abusive conduct and nonconsensual sexual assault (Caravaca-Sánchez & Wolff, 2016; Wolff et al., 2006). Most have used a single general question, rather than a series of specific questions (see Wolff, Shi, & Backman, 2008a, Wolff, Shi, & Blitz, 2008b). While all the peer-reviewed studies of sexual violence against incarcerated women have relied on self-report data, different survey modes have been used varying from computer-administered (Wolff et al., 2009) to mail (Struckman-Johnson & Struckman-Johnson, 2006). And, lastly, most of these studies used an unspecified time period (“since admission”) (Blackburn et al., 2008; Butler et al., 2002; Hensley et al., 2003; Struckman-Johnson & Struckman-Johnson, 2006; Walsh et al., 2012), with only a few using a defined six-month time period (Caravaca-Sánchez & Wolff, 2016; Lahm, 2015; Wolff et al., 2009). Not surprisingly, given this variation in methods, the estimated prevalence rates for sexual violence against incarcerated women across these eight published studies vary widely from 2% (Butler et al., 2002) to 24% (Walsh et al., 2012; Wolff et al., 2009), with a weighted average of 17%. In the two studies that estimated prevalence rates by the perpetrator, rates were higher for resident-on-resident sexual violence (ranging from 7.5% to 20.8%) than staff-on-resident sexual violence (ranging from 5.8% to 7.3%), with higher rates estimated for the United States (Wolff et al., 2006) than for Spain (Caravaca-Sánchez & Wolff, 2016).
More is known about the types and rates of violence against incarcerated women than is known about the factors that heighten their risk of physical or sexual harm while confined in prison. This lack of information hinders efforts to keep women safe during their confinement. Increasingly, researchers have attempted to identify characteristics of residents, both male and female, that elevate their risk of in-prison harm. In a synthetic review of 16 studies published on in-prison victimization between 1980 and 2014, Steiner et al. (2017) identified three sets of predictor variables used in prison violence studies. They are background characteristics about the individual (28 in total including age, gender, race, ethnicity, physical size, education, mental illness, type of offense, and security risk), routines of the individual inside prison (10 in total including housed in general population, work assignment, perceived safety of prison, and time served), and prison-level characteristics (eight in total including age of the resident population, crowding, and architectural design). Literature reviews such as these are useful because they show consistency and inconsistency in model specification, estimation technique, and sample size. They also reveal how often studies blend samples of male and female residents together and control for their differences by a single binary gender variable, which assumes that processes and predictors underpinning violence against incarcerated men and women are comparable. Moreover, in these blended samples, female representation is a very small percentage of the larger sample because of the disproportionate representation of males in the correctional system, giving greater weight to the male experience in the estimation process (Wood, 2013; Wood & Buttaro, 2013; Wooldredge & Steiner, 2012, 2013, 2014).
Only four published studies have estimated the risk factors associated with violence against incarcerated women without the inclusion of incarcerated men (Aizpurua et al., 2021; Caravaca-Sánchez & Wolff, 2016; Lahm, 2015; Wolff et al., 2007). The study by Lahm (2015), using data from a single women's prison, predicted four types of victimization—physical, sexual, property, and verbal—using traditional importation and deprivation covariates. Of the 14 covariates tested, only age, education, and disciplinary tickets significantly predicted victimization. The other three studies focused on characteristics of the individual that are known from the broader community-based literature to increase vulnerability to harm, particularly mental illness and childhood exposure to harm.
Research has consistently found that people with mental illnesses, compared to their general population counterparts without mental illnesses, are more likely to experience victimization (Maniglio, 2009; Teplin et al., 2005). Mental illness may increase the likelihood of victimization if symptoms of mental illness weaken women in ways that make them easy targets for harm. Hans von Hentig (1948), in his classic typology of victimization, identified emotional and mental disability as a trait of vulnerability, noting that psychiatric or cognitive impairment may increase susceptibility to deception and manipulation. He also noted that “depressed” people may not be sufficiently “vigilant” and as such may be more “susceptive to manipulation.” Being less vigilant due to symptoms of depression, such as feelings of helplessness, hopelessness, and sadness, or symptoms of disordered thinking associated with symptoms of serious mental illness may elevate risks of victimization inside prison. Several studies of in-prison victimization have found a positive association between mental illness and sexual victimization (Blitz et al., 2008; Caravaca-Sánchez & Wolff, 2016; Wood, 2013; Wood & Buttaro, 2013) and physical victimization (Wolff et al., 2009).
Similarly, a wealth of research on childhood exposure to harm has found a positive association between childhood abuse and victimization in adulthood (Cannon et al., 2010; Ports et al., 2016; Widom et al., 2008). According to the life-course, EBD model of risk transmission, early experiences of abuse shape neurological and psychological development in ways that increase vulnerability to future harm. Adaptive changes within the brain weaken the person's ability to recognize and guard against harm (American Academy of Pediatrics, 2012). In addition, over time, traumatically stressed individuals often adopt and adhere to a triad of cognitions that reinforce their individual worthlessness and inadequacy, that the world is dangerous and people are untrustworthy, and that the future is bleak and hopeless (Substance Abuse and Mental Health Services Administration, 2014). The brains and belief systems of children who are harmed often nurture vulnerability as they mature, which heightens their susceptibility to victimization later in life.
Research conducted by Ports et al. (2016) found that the risk of adulthood sexual victimization increases with the cumulative ACE score. While each type of ACE was found to be significantly associated with adult sexual victimization, the strongest of these predictors was childhood sexual abuse. In a review of over 30 sexual victimization studies examining the connection between sexual victimization in childhood and adulthood, only two failed to find a significant connection (Classen et al., 2005). Using a prospective study design, Widom et al. (2008) found associations between a higher lifetime risk of revictimization and all forms of childhood harm (physical abuse, sexual abuse, and neglect).
Consistent with expectations, Wolff et al.(2007) found that incarcerated women who were sexually victimized prior to the age of 18 years were two times more likely to report resident-on-resident sexually abusive conduct and any type of sexual victimization (perpetrated by another resident or staff) during the past six months. Childhood sexual abuse was also significantly associated with in-prison sexual victimization against female residents in Spain (Caravaca-Sánchez & Wolff, 2016). Neither of these studies, however, examined associations among other types of childhood harm and sexual victimization during incarceration, nor did they examine associations with physical violence. Prior treatment for a mental illness was not found to significantly predict in-prison sexual victimization in either study.
The study by Aizpurua et al. (2021) advanced this literature by using a person-centered approach to capture the interdependence among types of childhood harm exposure. A latent class analysis (LCA) identifies clustering (or “classes”) among types of harm, and these classes of harm can then be used to predict outcomes, such as victimization. After constructing classes of harm and controlling for demographic and sentence-related variables, Spanish female residents categorized in the high harm with moderate household dysfunction class had higher odds of in-prison physical and emotional harm (not sexual harm) relative to the low harm class. More specifically, females in the high harm group were 3.8 times more likely to have experienced in-prison emotional harm and 5.3 times more likely to have experienced physical harm.
Much remains unknown about the predictors of violence against incarcerated women. What is known is often clouded by variation in the definition of in-prison sexual and physical violence (the dependent variables), the specification of the model (the covariates), and the specification of the childhood abuse variable (single typology [binary variable] vs. interdependent typology [latent class variables]). In this article, we add to the knowledge base by testing specifications of the regression model that are informed by different theoretical explanations of physical and sexual victimization—importation/deprivation, vulnerability, and life-course—in an effort to better understand the predictors of in-prison victimization of women. This article uses self-report data from the only women's prison in a state prison system and estimates a series of logistic regression models that vary only by the inclusion and specification of particular predictor variables. In this way, we control for the noise in the literature associated with the inconsistent definitions of in-prison violence and the exclusion of types of childhood harm in the regression models. We first estimate a model including race, ethnicity, age, education, offense type (importation theory), time served, number of visits, and perception of prison overcrowding (deprivation theory). History of mental illness and current depressive symptoms are added next to test vulnerability, followed by the addition of childhood physical, sexual, and emotional harm to test the life-course explanation of victimization.
Current Study
The current study uses a person-centered approach, based on the interrelations among child harm, to address methodological limitations of previous research. While research suggests that men and women have unique patterns of childhood harm (Wolff et al., 2020), very few studies have been conducted with incarcerated women specifically. This is an important limitation because such analyses could inform program planning and development that address the unique treatment needs of incarcerated women. In this article, we assess the heterogeneity of childhood harm among incarcerated women using LCA. Two hypotheses are tested: (1) More severe childhood harm classes (life-course EBD explanation) and current depressive symptoms (vulnerability explanation) will be significantly associated with in-prison violence, and (2) Childhood sexual harm will significantly predict in-prison sexual victimization. These hypotheses are consistent with the literature on victim vulnerability and the intertemporal transmission of victimization over the life cycle, and identify personal factors that can be easily identified for protective classification and treatment intervention during incarceration.
Methods
Participants
The sample of eligible participants includes all residents housed at the women's facility except those who were younger than 18 years or in administrative custody, in detention, on death row, or otherwise too sick to participate in the survey. Overall, ∼90% of residents were eligible to participate. A total of 564 eligible incarcerated women participated in the study (response rate of 55.0%). They were recruited from a single female prison in New Jersey with three levels of security: high, medium, and low. The sample ranged in age from 18 to 67 years (M = 35.55 years; SD = 9.33 years), with 63.3% of the sample being between the ages of 30 and 50 years. Residents self-identified as White (31.6%), Black (49.6%), and other (18.8%).
Procedure
The survey, administered by audio-computer-assisted self-interviewing (CASI), was conducted in English and Spanish in June 2005. The English version of the survey took respondents ∼60 min to complete, whereas the Spanish version took an additional 30 min. Face-to-face interviews were conducted in cases when participants either had restricted movement or computer anxiety (n = 18). The recruitment protocol, consent, procedures, and consent form were approved by the appropriate university and correctional agency research review boards and committees.
Measures
In-Prison Victimization (Outcome)
Four measures of in-prison victimization were assessed based on the type of violence (physical vs. sexual) and the perpetrator of such violence (resident vs. staff member). Physical violence by another resident was present when the respondent answered affirmatively to any of six questions examining whether, during the past six months, another resident had ever “slapped, hit, kicked, or bit you,” “choked or attempted to drown you,” “hit you with some object with the intent to harm,” “beat you up,” “threatened or harmed you with a knife or shank,” or “been physically assaulted by an inmate.” Physical violence by prison staff occurred when residents indicated having experienced any of those six incidents within the past six months perpetrated by prison staff. To measure sexual violence during the past six months, 11 indicators were used. They included (1) been sexually assaulted, (2) touched in threatening ways, (3) unwanted touch, (4) forced to touch somebody else, (5) forced to have sex, (6) forced to have oral sex, (7) forced to have anal or vaginal sex, (8) inserted fingers or objects without consent, (9) forced to insert fingers or objects in another person, (10) attempted sexual assault, and (11) forced to perform sexual acts to avoid future harm. Respondents were identified as victims of sexual victimization by residents if they responded affirmatively to any of the 11 items that referred to other residents and identified as victims of sexual violence by staff if they reported any of the 11 incidents perpetrated by staff members.
Importation Covariates
Preprison Attributes. The following sociodemographic characteristics have been traditionally included as importation variables: race (distinguishing among Black, White, and other), ethnicity (Hispanic = 1), age (in years), and the highest level of education (7-point scale: grade school only, some high school, high school graduate/general educational development, technical or trade school, some college, bachelor's degree, and graduate studies).
Criminal History. Offense types were distinguished between violent crimes (battery, assault, murder and/or manslaughter) and sexual offenses (rape and/or sexual assault). Respondents were asked, “What type of offense are you doing time for now: drug offense, property offense (like theft, burglary, car theft), fraud or embezzlement, rape or sexual assault, violent offense (like battery, assault, murder, manslaughter), and other.” Multiple responses were allowed. If there were multiple responses, a singular offense type was assigned using the following rule: sexual offense was assigned first, if identified; followed by a violent offense, if identified; followed by property offense, if identified.
Deprivation Covariates
Time Served. A continuous variable that measures the time in years served in prison or jails since turning 18 years of age.
Number of Visits. Consistent with Lahm (2015), the number of visits was included as a deprivation covariate. It was measured by the number of visits received from friends and family members during the past six months. This was an open-ended numeric question. Two outliers were trimmed at the 90th percentile (75).
Perception of Crowdedness. Crowdedness was measured by the subjective response to the question: “How crowded has your housing unit been,” with the following response options: not at all crowded, slightly crowded, somewhat crowded, and very crowded. Perception of crowdedness is a binary variable with 1 equaling “very crowded.”
Vulnerability Covariates
Mental Illness. Mental illness was based on an affirmative response to the following question: “Have you ever been treated for any of the following problems: depression, schizophrenia, posttraumatic stress disorder (PTSD), bipolar disorder, anxiety disorder.” These were all dichotomous questions, measured using a lifetime reference frame. Mental illness distinguished between no mental illness, serious mental illnesses (ever been treated for schizophrenia and/or bipolar disorder), and other mental illnesses (ever been treated for anxiety, depression, and/or PTSD).
Current Depressive Symptoms. Four symptoms were used to assess current depressive symptoms. Respondents were asked how often, in the past six months, they had feelings of hopelessness, helplessness, loneliness, and difficulty caring about anything (symptoms of potential vulnerability). Items were measured using 4-point unipolar scales ranging from never to every day. Depressive symptom scores ranged from 0 to 15 and were computed by summing the responses to the four items (based on 0 = never, once a month, or a few times a month; 1 = once a week; 2 = a few times a week; and 3 = every day). The scale showed good internal consistency (α = .81).
Life-Course Covariate
Childhood Abuse (Latent Class Indicators). Ten binary variables were used to measure child physical abuse (five items), sexual abuse (four items), and emotional abuse (one item). These items were adapted from the National Violence Against Women and Men Survey (Tjaden & Thoennes, 2000). Each question was referenced to when the resident was a minor (younger than the age of 18 years) and alluded to “relatives, friend, or anyone else” as perpetrators of the harm. Physical abuse was based on responses to questions about the following acts: “choked or attempted to drown,” “hit with some object that left welts or caused bleeding,” “burned with a match, cigarette, hot liquid, or any other hot object,” “threatened or harmed with a knife or gun,” or “beat up.” For sexual abuse, residents were asked whether anyone had done any of the following to them as a minor: “touched, felt, or grabbed in a way that felt sexually threatening,” “tried or succeeded in having you touch their genitals,” “coerced sex by force or threat of harm,” or “coerced oral or anal sex by force or threat of force.” Emotional abuse was measured by a positive response to the question of whether anyone had ever “abandoned you” as a minor. Dichotomous indicators of physical abuse, sexual abuse, and abandonment were also created based on the responses to the 10 childhood abuse experiences (coded as 1 if any of the items integrated into each typology was answered positively).
Analytical Strategy
Analyses were conducted in several steps. First, descriptive statistics were computed for all study variables. Next, LCA was used to identify groups of respondents based on their child abuse experiences. A one-profile model was fitted and then the number of classes progressively increased up to 10, assessing whether adding each additional profile resulted in conceptually and statistically superior solutions. Models were tested iteratively, and multiple fit statistics were used to select the optimal model. These indicators included log-likelihood (LL), the Akaike information criterion (AIC), and the Bayesian information criterion (BIC). In interpreting these indicators, lower BIC and AIC values and higher LL values reflect better model fit. Based on simulation studies indicating that AIC tends to over-extract the number of classes, BIC was prioritized over AIC when determining the optimum number of classes (Chen et al., 2017; Nylund et al., 2007). In addition to the fit statistics, consideration was given to class size (avoiding rare classes comprising <5% of the sample), the substantive meaningfulness of the classes, and the parsimony of the models. SAS was used for data cleaning and management, and Stata for LCA model testing.
To examine the extent to which the importation/deprivation, vulnerability, and life-course covariates were linked to in-prison victimization, a series of logistic regression models were estimated. There was no indication of collinearity among variables (variance inflation factor [VIF] range = 1.05-2.24). Item nonresponse across all study variables ranged from 0% to 2.3% (M = 0.8%, SD = 0.6%). To avoid the loss of statistical power resulting from a reduced analytical sample and given the evidence that the data were missing completely at random (Little
Results
Sample Description
Table 1 provides the descriptive statistics for all study variables. In-prison victimization was relatively common, with slightly over one in five residents reporting physical and sexual abuse from other residents within the past six months (22.4% and 23.0%, respectively). Physical and sexual victimization from staff members was indicated by roughly one in 11 residents (9.1% and 8.6%, respectively). During a six-month period, six in 10 women reported no victimization of any type measured (59.9%). Experiences of victimization during childhood were widespread, with approximately half of the residents reporting physical and sexual harm (53.8% and 46.7%, respectively), and over one-third experiencing abandonment (35.9%) before turning 18 years.
Characteristics of the Sample (N = 564).
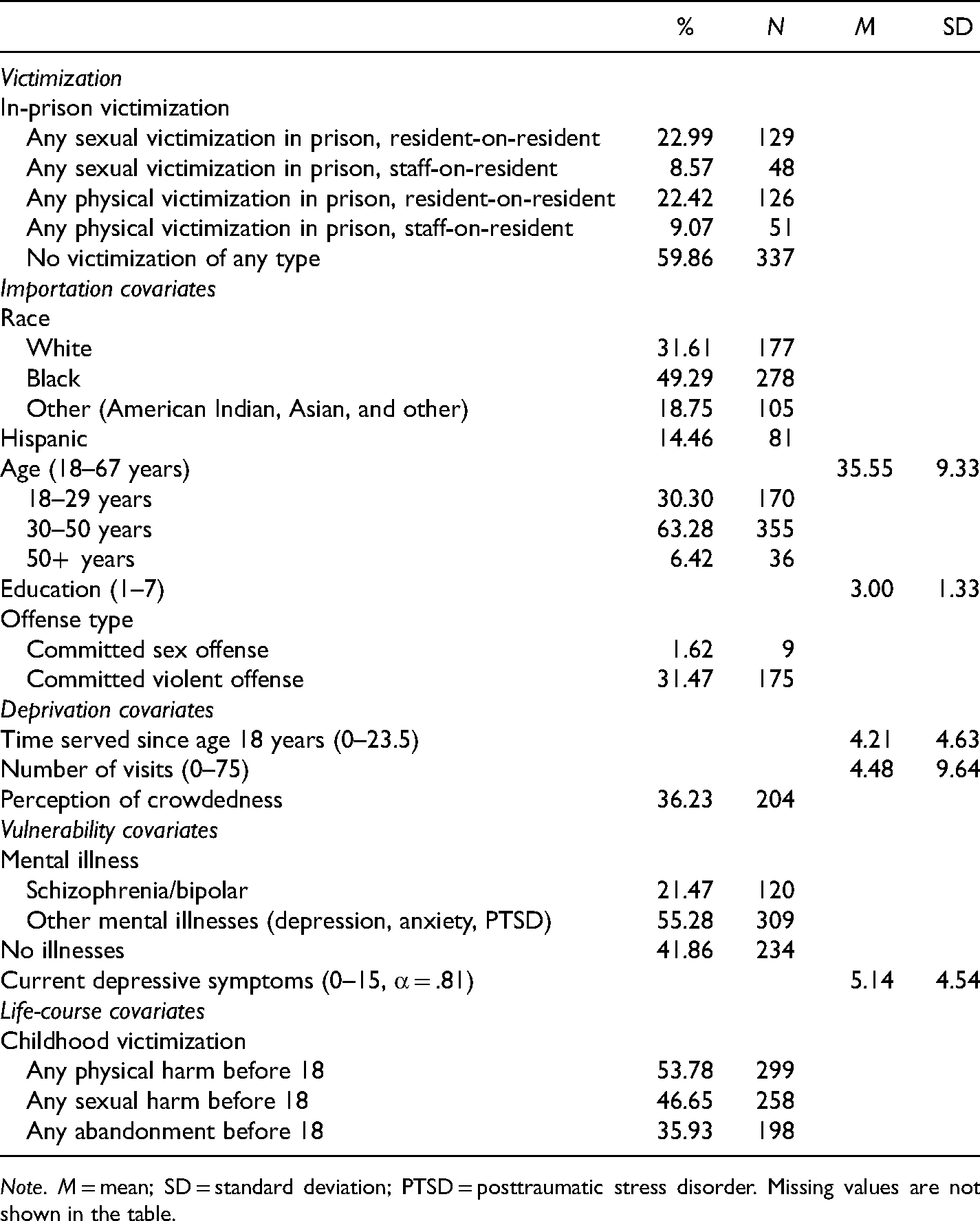
Note. M = mean; SD = standard deviation; PTSD = posttraumatic stress disorder. Missing values are not shown in the table.
Residents’ age ranged from 18 to 67 years (M = 35.55 years, SD = 9.33 years) and the average level of education among women was high school. Nearly half of the residents identified as Black (49.3%) and 14.5% were Hispanic. Approximately one in three participants had been charged with a violent offense (31.5%). On average, residents had received four visits from friends and family members during the past six months, with a typical resident having received only one (mdn = 1). Current depressive symptom scores ranged from 0 to 15, with an average of 5.14 (SD = 4.54). Treatment for mental illnesses in the past was frequent, with roughly one in five residents reporting ever receiving treatment for schizophrenia and/or bipolar disorder (21.5%), and slightly over half (55.3%) had prior treatment for other disorders (depression, anxiety, and/or PTSD). Time served since the age of 18 years ranged from <1 to 23.5 years, with the typical resident having spent roughly three years incarcerated (Mdn = 2.75; M = 4.21; SD = 4.63). Nearly four in 10 residents reported being housed in a very crowded unit (36.2%).
Latent Class Profiles
LCA models were estimated for one to 10 classes. The LCA fit indices are shown in Table 2. Overall, the fit indices favored the four-class solution, which had the lowest BIC value. AIC values progressively decreased from the one- to the four-class model and then flattened, which also supported the selection of this solution. These four classes are distinguished from each other by the occurrence of child abuse experiences. Figure 1 displays the conditional item probability profile for the four-class model, which was used to interpret the emerging profiles. Based on the observed patterns, the classes were labeled as (1) low abuse, (2) low sexual abuse and moderate/high nonsexual abuse, (3) high sexual abuse and low/moderate nonsexual abuse, and (4) high abuse.
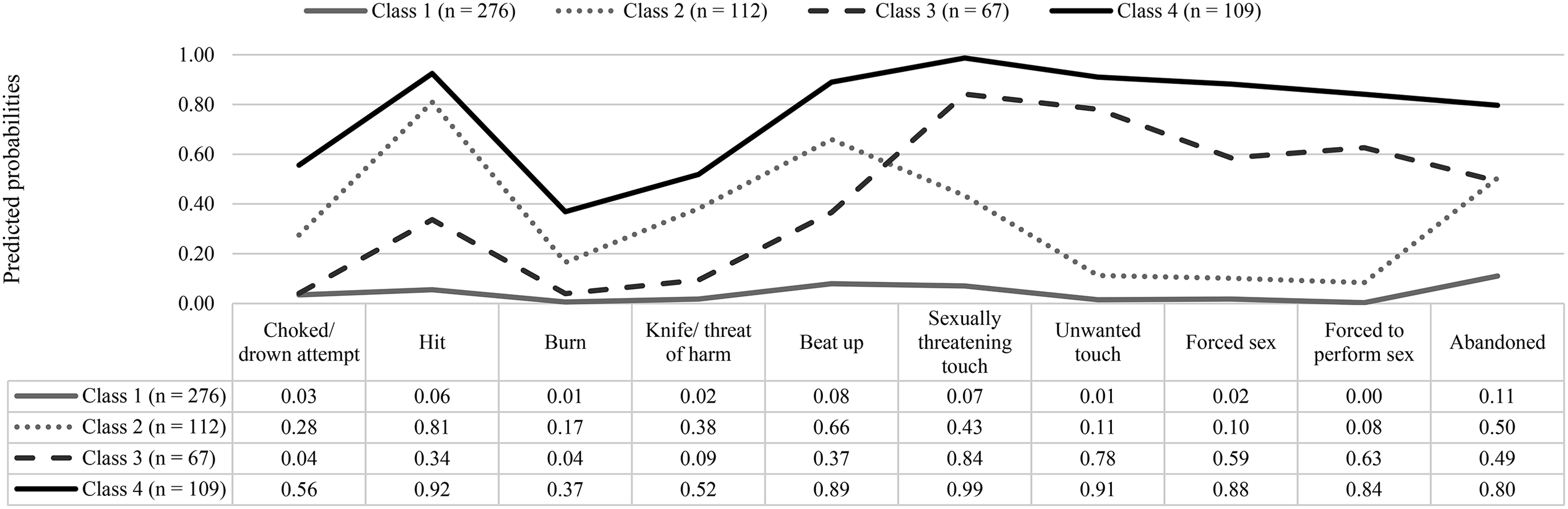
Predicted probabilities of childhood abuse experiences by class (N = 564).
Fit Indices for LCA Models with 1–10 Classes.

Note. DF = degrees of freedom; AIC = Akaike information criteria; BIC = Bayesian information criterion. Bolded values indicate chosen model.
Class 1, low abuse, was the largest class (48.9% of the sample) and was characterized by low probabilities of childhood abandonment, physical abuse, and sexual abuse. Compared with the other profiles, class 1 had the lowest scores on every domain (<15% in all cases). Class 2 (19.9% of the sample) was labeled low sexual abuse. Residents in this class had moderate and high scores across indicators of physical abuse (17%–81%) and abandonment (50%). Class 3 was the smallest group (11.9%). This class was labeled as high sexual abuse, given its high probabilities of childhood sexual abuse (59%–84%) and abandonment (49%), with low to moderate experiences of childhood physical harm (4%–34%). Class 4 (19.3%), high abuse, had the highest probabilities of all forms of childhood abuse, including physical abuse (37%–92%), sexual abuse (84%–99%), and abandonment (80%).
Correlates of In-Prison Victimization
To assess which factors were associated with in-prison victimization, a series of logistic regression models were estimated with the four measures of in-prison victimization as the outcome variables. The predictors on these models included sociodemographic and crime type information (importation—model 1) and prison conditions (deprivation—model 1), indicators of mental health (current and past) (vulnerability—model 2), and childhood harm (life-course—models 3 and 4). Table 3 provides the results of the models predicting physical victimization perpetrated by other residents, including odds ratios (ORs), standard errors, and 95% confidence intervals (CIs). The two variables that consistently predicted physical victimization by another resident were current depressive symptoms and perception of crowdedness. These variables were significant in all the models where they were included and were linked with increased risk of physical victimization.
Logistic Regression Results, Physical Victimization Resident-on-Resident (N = 564).
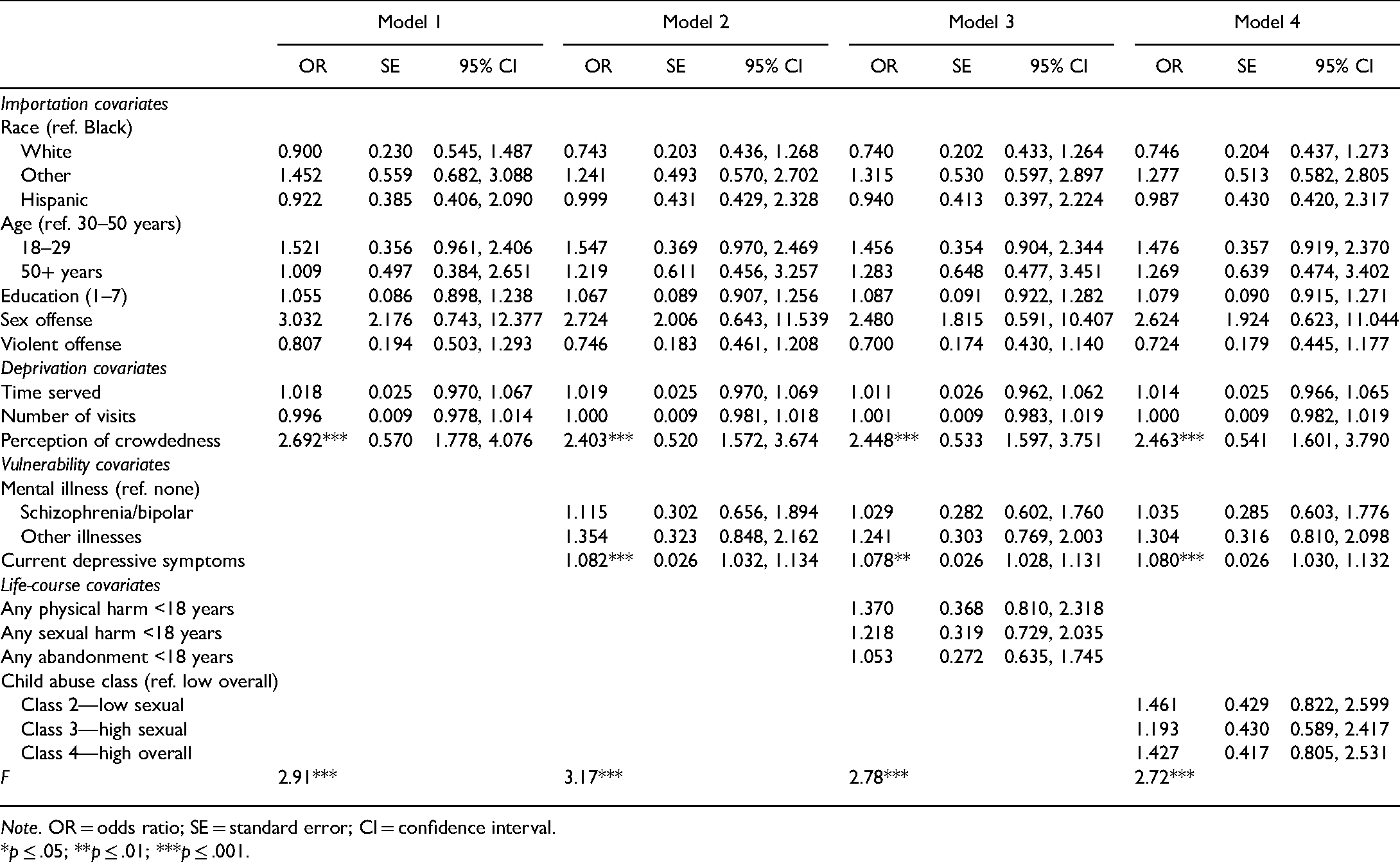
Note. OR = odds ratio; SE = standard error; CI = confidence interval.
*p ≤ .05; **p ≤ .01; ***p ≤ .001.
The models examining physical victimization by staff members are presented in Table 4. Across the models, White residents were significantly less likely to report physical victimization by prison staff than Black residents, and Hispanic women were less likely to report this form of victimization than their non-Hispanic counterparts. Conversely, the odds of physical victimization were higher for other racial groups (OR = 2.899, p = .018, 95% CI = 1.197, 7.024), although this variable became nonsignificant once mental health variables were included in the models (models 2–4). Residents convicted for violent offenses were consistently less likely to report physical victimization by prison staff. Consistent with the models examining physical victimization by residents, current depressive symptoms and perception of crowded units increased the risk of physical victimization perpetrated by staff members.
Logistic Regression Results, Physical Victimization Staff-on-Resident (N = 564).

Note. OR = odds ratio; SE = standard error; CI = confidence interval.
*p ≤ .05; **p ≤ .01; ***p ≤ .001.
Table 5 summarizes findings from the regression model predicting sexual victimization by another resident. In them, age, childhood abuse, current depressive symptoms, and perception of crowdedness emerged as significant correlates. Specifically, the odds of sexual victimization were significantly higher among the youngest group (18–29 years) when compared to the middle-age group (30–50 years). In contrast, members of the low sexual abuse class and the high abuse class were more likely to report sexual victimization by another resident (model 4, OR = 2.250, p = .005; 95% CI = 1.279, 3.956 and OR = 2.136, p = .009, 95% CI = 1.206, 3.784). The relevance of childhood abuse and the robustness of the findings are supported by the significance of the dichotomous indicators of childhood physical and sexual abuse (model 3, OR = 1.697, p = .047; 95% CI = 1.007, 2.859 and OR = 1.766, p = .027, 95% CI = 1.068, 2.922). Similar to the models examining physical victimization, the results from these models reveal that current depressive symptoms and perception of crowdedness are consistently linked to sexual victimization perpetrated by other residents.
Logistic Regression Results, Sexual Victimization Resident-on-Resident (N = 564).

Note. OR = odds ratio; SE = standard error; CI = confidence interval.
*p ≤ .05; **p ≤ .01; ***p ≤ .001.
The models analyzing sexual victimization by prison staff, displayed in Table 6, indicate that current depressive symptoms and time served were the only significant predictors. Scoring higher on current depressive symptomatology and having been incarcerated longer significantly raised the odds of sexual victimization perpetrated by a staff member.
Logistic Regression Results, Sexual Victimization Staff-on-Resident (N = 564).

Note. OR = odds ratio; SE = standard error; CI = confidence interval.
*p ≤ .05; **p ≤ .01; ***p ≤ .001.
Discussion
Many different personal and prison characteristics have been used to predict in-prison violence (Steiner et al., 2017). Most often the choice of risk factors has been grounded in criminological theories about deprivation within prison environments (Goffman, 1961; Sykes, 1958) and the importation of personal values, beliefs, and norms of behavior from the community (Irwin & Cressey, 1962). A few studies have explored the role of vulnerability as identified by von Hentig (1948), particularly mental illness and symptoms of psychological distress (Blitz et al., 2008; Caravaca-Sánchez & Wolff, 2016; Wolff et al., 2009; Wood, 2013; Wood & Buttaro, 2013). Research on the etiological transmission of harm over the life cycle has been pverlooked, with a few exceptions (Aizpurua et al, 2021; Caravaca-Sánchez & Wolff, 2016; Wolff et al., 2007). Moreover, these studies have traditionally been insensitive to well-known gender-based differences in victimization (Tjaden & Thoennes, 2000). This study challenged the notion that victimization is unique to the setting or, more specifically, that victimization inside prison is predicted by factors unrelated to factors that predict victimization in the community. To test this expectation of environmental similarity, two robust predictors of victimization from the community-based victimization literature were selected: childhood abuse and mental illness/psychological distress and used to predict in-prison physical and sexual victimization of women.
First, as expected, nearly half or more of incarcerated women reported some form of childhood physical and sexual abuse and roughly four in 10 reported an experience of in-prison sexual or physical victimization over a six-month period. Childhood harm fell into four distinct typologies, with some incarcerated women experiencing little or no childhood harm, others had either high or low nonsexual harm exposure coupled with low or high sexual harm, and another group experienced high levels of all types of harm. Childhood harm significantly predicted in-prison resident-on-resident sexual victimization, consistent with our expectation and the broader victimization literature (Classen et al., 2005). However, the relationship was not straightforward. Compared to low overall childhood harm, low sexual and high abuse childhood harm classes predicted resident-on-resident (not staff-on-resident) sexual victimization. By contrast, high sexual childhood harm was not predictive of sexual victimization inside prison during a six-month period. Particular types of childhood abuse (physical and sexual) were also predictive of resident-on-resident sexual victimization. All these associations remained significant controlling for current depressive symptoms. Also, contrary to expectation, in-prison physical victimization (perpetrated by residents or staff) and staff-on-resident sexual victimization were not correlated with childhood harm, measured either by class or binary types of harm.
Second, while the effect of childhood harm was inconsistently predictive of in-prison victimization, higher levels of current depressive symptoms were strongly associated with physical and sexual victimization perpetrated by another resident and staff. This finding is consistent with the broader literature on the mental health consequences of victimization (Choudhary et al., 2012; Cortina & Kubiak, 2006; Hedtke et al., 2008; Johansen et al., 2013; Kilpatrick, et al., 1985). Victimization is a highly stressful event and is often associated with psychological symptomatology, inclusive of depression and depressive symptoms (Chermack et al., 2006; Choudhary et al., 2012; Johansen et al., 2013). In addition, the fear of revictimization may elevate depressive symptoms (especially feelings of helplessness) among those recently victimized (Boney-McCoy & Finkelhor, 1995). Either way, current depressive symptoms may be an emotional response to a recent experience of victimization. On the other hand, current depressive symptoms may be a precursor to victimization as depressive symptoms may signal lowered defenses and increase vulnerability to attack (Acierno et al., 1999; Briere & Jordan, 2004).
Third, a new contribution to the literature is the consistently positive association found between the perception of crowdedness and physical and sexual victimization. This is new not because overcrowding has not been examined in previous studies of violence and victimization. To the contrary, the link between prison crowding and violence and victimization has received considerable attention, and the results are conflicting. Although some researchers have found no association between prison crowding and victimization (Kuo et al., 2014; Lahm, 2009), others have found a positive association between prison crowding and violence (Baggio et al., 2020; Gaes & McGuire, 1985; Glazener & Nakamura, 2018; Nacci et al., 1977), and others have challenged the significance and importance of this association altogether (Franklin et al., 2006). Rather, what makes our finding new is that perceptions of overcrowding consistently predict victimization. Researchers have traditionally measured prison overcrowding as population density at the facility or system level. By contrast, such as Kuo et al. (2014), we measured crowdedness subjectively at the individual level but, unlike Kuo et al., we measured it with a simple direct question asking how crowded the resident felt her unit was, whereas Kuo et al., asked five scaled questions that were more oblique and conflated with assessments of physiological and psychological wellness.
One possible explanation for the link between the perception of crowdedness and victimization concerns the impact of stress, created by overcrowded conditions, on individual behavior and wellness. Paulus et al. (1978) argued that overcrowding was positively associated with mortality rates because prison overcrowding produced high stress that essentially put residents’ nerves on edge (creating psychological impairment). That is, people, when pressurized by stress associated with living too closely to others, may be more aggressively reactive, elevating behaviors of violence (increasing the likelihood of victimization, including self-harm) and depressively inactive (elevating feelings of powerlessness in ways that create risks for victimization). Not surprisingly, there is considerable affirmative evidence showing an inverse relationship between levels of perceived personal control or autonomy and prison misconduct and feelings of helplessness and depression (Goodstein et al., 1984; Ruback et al., 1986; Wright, 1991, 1993). The role of perceptions regarding environmental conditions and victimization warrants more careful investigation in future studies.
Overall, our findings, supportive of the vulnerability and life-course explanations for victimization, suggest that predictors of victimization are similar across settings. Depressive symptoms and childhood harm are common risk factors for women victimized in the community and in prison. Even characteristics of the environmental setting, such as population density, may be similarly perceived by women in different settings if they trigger generalized stress responses conditioned by childhood harm. And, as such, the relevant question for all women independent of setting is: What makes a particular woman a target for harm?
By reducing some of the noise in this literature and integrating explanations across the literature on victimization, three strong predictors were identified. Yet, much remains unknown in part because the available data are limited. To advance the knowledge base, more individualized data are needed on both childhood and adulthood harm. First, measuring harm as a binary variable conceals meaningful attributes of childhood harm, such as frequency, severity, age of onset, and perpetrator type, that heighten the risk of victimization (Classen et al., 2005). Future research, at a minimum, should include the full (revised) ACE survey, inclusive of questions on family dysfunction. In addition, the definition and measurement of in-prison victimization should be expanded to include bullying, voyeurism, indecent exposure, stalking, and sexual exploitation, and a measure of emotional abuse inclusive of dimensions identified in the abusive behavior inventory (Postmus et al., 2016; Shepard & Campbell, 1992). These additions would provide a more accurate measure of in-prison harm.
Second, even with extant data, more could be learned by adding interaction effects and using second-generation multivariate methods that, instead of analyzing variables separately, analyze all variables simultaneously (see Henry, 2020). Exploring interaction effects among childhood harm and adult outcomes is an important next step, especially given the consistently strong associations found between childhood adversity and adverse adult outcomes, including substance abuse, mental illness, incarceration, and low educational attainment (Anda et al., 2006). Moreover, while the directionality of the co-occurrence of depression and victimization cannot be disentangled with cross-sectional data, the mediation effect of childhood harm and depression on the association between childhood abuse and adulthood victimization could be explored using path analysis or structural equation modeling. Further exploration of this relationship using a prospective design is warranted. Longitudinal data would yield greater clarity regarding the temporal sequencing of victimization events and symptoms of psychological distress, which could inform efforts to prevent revictimization.
Victimization prevention is an important public policy and public health goal. Reducing the risk of in-prison victimization and treating its consequences during incarceration has the potential to improve individual and public health outcomes (Krug et al., 2002). Yet, for research to be useful in this manner, the evidence should identify instruments of intervention that make theoretical sense and are practical. The links identified in this study among childhood harm and victimization, depressive symptoms and victimization, and perceived overcrowding and victimization suggest practical pathways to both prevent in-prison victimization and effectively treat its consequences. First, by broadening the scope of admission protocols to identify, as potential risk factors, the abuse histories and depressive symptoms of women, prison officials can use the classification process more deliberatively to protect women against victimization. Second, because women with these risk factors may be at heightened risk of harm during incarceration, targeting each of these risk factors for proactive, coordinated intervention is sensible. This might include surveying women periodically about their impressions of crowdedness and psychological wellness in an effort to proactively identify those who are experiencing levels of stress that may adversely affect safety and wellness outcomes. For those identified at risk, trauma-informed treatment that enhances emotional regulation and coping skills, such as seeking safety (Miller & Najavits, 2012), would build the internal capacity of at-risk women so that they can safely survive incarceration, while also helping them to confront their trauma histories in a safe and supported way. Using techniques from dialectical behavioral treatment, emotion-focused therapy, cognitive behavioral therapy, mindfulness-based interventions, and problem-solving therapies, when combined with trauma treatment, serve to build and strengthen the internal resources of incarcerated women in ways that prevent their abusive and depressive pasts from repeating themselves. Third, given the cooccurrence of depressive symptoms and in-prison victimization, it is important that women who are victimized during their incarceration be referred immediately to compassionate mental health treatment that considers childhood harm and depression as part of the healing and recovery process.
There are several noteworthy limitations. One limitation is that our sample was drawn from the only women's prison in a single state and, as such, cannot be generalized to other women's prisons. Whether risk factors differ by prison is an area for future research. Also examining whether similar risk factors predict in-prison victimization of men would be a valuable addition to the literature. A second limitation is that all measures used in this study are based on self-report. While respondents may have inflated or deflated responses, our use of audio-CASI to protect confidentiality served to maximize the accuracy of their responses, minimizing the risk of measurement error. Another limitation is the cross-sectional design of our data. We are unable to disentangle causal relationships among associations without knowing whether victimization occurred before or after the elevation of depressive symptoms. Research based on prospective designs is needed to elucidate the directionality of the relationship between depressive symptoms and victimization. These more targeted studies would rigorously measure depressive symptoms using standard depression scales, such as the Beck depression inventory, Hamilton depression rating scale, or Center for Epidemiologic Studies depression scale. Lastly, isolation is an attribute of prison deprivation. Connection with people on the outside ameliorates social isolation. We proxied social connection using a number of visits, which does not capture the quality of these visits or other forms of connection through phone calls and emails/letters (which are less costly and likely more frequent). As social support may be an important protective factor, measuring it more inclusively is recommended.
Victimization is a prevalent and serious problem inside prisons. This study identifies two often overlooked risk factors of victimization that can be easily identified and targeted for effective, evidence-based intervention. More research is needed on the bidirectional relationship between depressive symptoms and victimization but, meanwhile, it is imperative that proactive steps be taken to build the capacity of at-risk women so that in-prison harm can be minimized. Our research suggests that the presentation of childhood harm risk is different among women who experience in-prison victimization but their current depressive symptoms are similar in elevation. Harm prevention should motivate proactive intervention based on this information alone. But what intervention is best and which techniques are most effective and when requires more careful research. In the future, as research on identifying and understanding risk factors of in-prison victimization continues using experimental and longitudinal designs, parallel intervention research is needed on the pairing and sequencing of interventions for incarcerated women with elevated risks of harm to ensure that the right treatments are paired at the right time in the right way to reduce their exposure to harm during incarceration.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.