
Abstract
In legal cases regarding child sexual abuse (CSA), children have various options, such as to disclose or deny maltreatment. When interviewed in adulthood, their accounts may be consistent with their childhood responses. Alternatively, denial in childhood could be followed in adulthood by disclosure (“deferred disclosure”), confirming previous suspicions. Or the adults could possibly recant. We conducted a longitudinal study of CSA disclosures and denials (N = 99; Time 1 [T1], 3- to 16-year-olds). T1 CSA disclosures and denials at a forensic unit were compared to the individuals’ responses 20 years later (Time 2 [T2]. 22- to 37-years-old). We found that consistent disclosure was associated with being older at T1 and female. Deferred disclosure was significantly associated with greater T2 trauma-related symptoms. Corroboration and higher CSA severity predicted T2 recantation. Consistent denial was related to less severe CSA. Our findings add to knowledge about CSA disclosures, which affect legal pathways available to child victims.
Introduction
In legal cases of child sexual abuse (CSA), a major point of concern is whether the alleged victim discloses or denies the experience. We conducted a longitudinal study that examined consistency and change in CSA disclosures from childhood to adulthood. Specifically, we examined consistent disclosure, deferred disclosure (i.e., childhood denial of CSA followed by disclosing it in adulthood), recantation (i.e., disclosing CSA in childhood but denying it in adulthood), and consistent denial.
Disclosure of CSA is typically required for a case to move forward in the legal system. Yet failure to disclose CSA during childhood forensic interviews (e.g., denying that it was experienced) occurs (Eisen et al., 2021). By comparing, in the same individuals, childhood and adulthood disclosures of CSA, predictors of consistencies and discrepancies in disclosures and denials could be identified. Such knowledge may help authorities and laypersons (e.g., forensic interviewers, law enforcement officers, prosecutors, and jurors) evaluate CSA cases, with implications for legal response to child maltreatment.
We focused on disclosure and denial of CSA across two timepoints. In our longitudinal study, the first timepoint (Time 1 [T1]) was in childhood during investigative interviews when suspected victims were directly asked (i.e., “Has anyone touched your private parts?”), a question likely to elicit a disclosure from children (Saywitz et al., 1991). The second timepoint (Time 2 [T2]) was 20 years later, when these same individuals, now adults, were interviewed about child maltreatment, and again directly asked about CSA. Our main goal was to investigate factors that predicted disclosure consistencies and changes.
Disclosures, Consistencies, and Discrepancies
Disclosure here concerns how much a person is willing or able to tell another about the experience of CSA. There are many reasons for consistencies or discrepancies in disclosures from childhood to adulthood. For example, in childhood, a survivor may disclose to protect themselves or others from continuing the experience of CSA; adults may disclose because they finally feel safe to do so, or because they understand the immorality of the acts (Lyon, 2007). Children might deny CSA that they are experiencing because they were threatened, told to keep it secret, embarrassed, or protecting the perpetrator (e.g., Herman, 1992); in adulthood, they may have greater perspective and be able to reflect on what happened. However, in childhood, the psychological damage of denying CSA that is being experienced may be related to greater trauma-related symptoms later on (Wu et al., 2021). We thus focused on disclosure and denial.
Disclosure and Denial
It is estimated that under 25% of CSA victims disclose their abuse immediately (London et al., 2005; McElvaney, 2015). Although surveys reveal that only a minority of CSA cases are brought to authorities’ attention (McGuire & London, 2020; Russell, 1983), disclosures within investigative interviews are often necessary to ensure child protection and legal resolution (e.g., Block et al., 2022). A meta-analysis indicated that about 64% of children disclose in forensic interviews, but it also revealed that about 30% of children do not disclose there (Azzopardi et al., 2019).
One important type of non-disclosure is to deny that CSA was experienced. Yet when specifically examining children’s CSA denial, considerable variability exists, even in corroborated cases. When Hershkowitz et al. (2006) examined 100 children in CSA cases, approximately half denied the corroborated sexual abuse. Elliot and Briere (1992) reported that, of 399 suspected CSA victims (8- to 15-years-old), 10% denied despite credible evidence. Even with strong evidence of CSA (e.g., photos), some children deny that it occurred (e.g., Cederborg et al., 2007).
Based on the same sample studied here, Eisen et al. (2021) examined denials in 3- to 16-year-olds who had two T1 forensic interviews due to suspicions of sexual or physical abuse. The denial rate was 39.2% for CSA cases; being younger was associated with CSA denial. Boys compared to girls were also more likely to deny CSA consistently across the two interviews in childhood. The present study advances Eisen et al.’s work. Here, we examined whether adults continue their disclosures or denials 20 years later.
Recantation
Rieser (1991) discusses many reasons why a child may recant, including guilt, family pressure, and lack of support. Empirical studies on recantation are sparse. Of note, in a case file study, Malloy et al. (2007) examined the prevalence of recantation among 2- to 17-year-old intrafamilial CSA victims. A 23.1% recantation rate was observed. Child victims who were more vulnerable to familial adult influences (younger children, those abused by a parent figure and who lacked support from the non-offending caregiver) were more likely to recant. Although recantation could indicate an initial false report, perhaps due to leading questions (e.g., Ceci & Bruck, 1995; London et al., 2005), this alternative hypothesis was not supported in the Malloy et al. study. However, it should be noted that all participants in the Malloy et al. study were involved in dependency court cases related to their abuse, potentially limiting the generalizability of their findings.
In contrast to the Malloy et al. (2007) research, the present study examined possible recantations in adulthood. Greater perspective, years after disclosure, could result in accurate denial of past CSA. However, if the CSA was corroborated at T1 but is denied in adulthood, the recantation may reflect, among other possibilities, socioemotional or cultural factors (e.g., feeling that it is “no one else’s business”).
A Longitudinal Approach: Predictors
One advantage of a longitudinal approach is the comparison, within the same individuals, of disclosure in childhood and adulthood. In child maltreatment cases, children typically want to go home (e.g., from foster care, from court) to their parents, even at risk of further child abuse (Block et al., 2010; Melinder et al., 2013). Attachment to family members, even if abusive, may prompt children to protect them (Crittenden & Ainsworth, 1989). Children thus may be motivated to deny CSA that has occurred (Malloy et al., 2007). In contrast, adults in general should be freer of childhood constraints, including feeling less dependence on parents and close family members.
Based on the extant literature, we attempted to identify predictors of consistencies and changes across our two timepoints. The hypothesized predictors were T1 age, gender, race, CSA severity, and T2 trauma-related symptoms.
Age
Azzopardi et al.’s (2019) meta-analysis revealed that older children are more likely to disclose in forensic interviews. Although they are also more aware of negative consequences of their disclosures (Goodman-Brown et al., 2003; McElvaney et al., 2020), they usually know right from wrong and can articulate what happened. Also, adults are more likely to remember what was discussed in forensic interviews about CSA and other traumas when these conversations took place as older children or adolescents (Wu et al., 2021). Thus, older age at T1 might be associated with greater consistency in disclosures and denials.
Although older children are more likely to disclose CSA, the literature on age and denial or non-disclosure of CSA in forensic interviews is mixed. It suggests, however, that younger children are more likely to be inconsistent in their disclosures or denials of CSA, and are more likely to delay disclosure (e.g., Alaggia et al., 2019; Hershkowitz et al., 2007; Keary & Fitzpatrick, 1994; Leclerc & Wortley, 2015; Wallis & Woodworth, 2020). Young children are easily silenced by promises and threats, may not recognize CSA as wrong, and lack vocabulary to describe the abuse (e.g. Finkelhor, 1984), yet at times they may “leak” the truth (Evans & Lee, 2013), meaning that young children often find it difficult to maintain a deception or unintentionally reveal the abuse. This often leads to inconsistent, accidental disclosures (Alaggia et al., 2019).
Gender
For both genders, factors that inhibit disclosures include considering CSA as a taboo topic, lacking trust that the potential disclosure recipient will respond appropriately, and experiencing negative emotions such as shame, guilt, and embarrassment (Alaggia et al., 2019; Collin-Vézina et al., 2015; Fontes & Plummer, 2010; Jensen et al., 2005). Some men feel the additional challenges of not wanting to be identified as victims and fear being labeled as gay if the perpetrator is also male (Easton et al., 2014; Sorsoli et al., 2008). Perhaps as a result of these additional challenges, males are less likely than females to disclose CSA and are more likely to delay disclosing CSA (e.g., Cashmore et al., 2017; Easton et al., 2014; Stoltenborgh et al., 2011; Wallis & Woodworth, 2020; Widom & Morris, 1997). Males thus may be less likely than females to disclose CSA at all or consistently.
Race
Black children are overrepresented in the child welfare system compared to their representation in the U.S. population (U.S. Department of Health & Human Services, 2022). Likely exacerbated by past racism, negative attitudes tend to exist in many minority communities, including the Black community, toward the child protection system (Cleveland & Quas, 2020), which may result in minority members being hesitant or unwilling to disclose (e.g., Goodman et al., 2003). We had the opportunity to examine this issue as our sample included many Black participants who were questioned, across our two timepoints, about their experience of CSA. Thus, we considered race in our study.
CSA Severity
Perhaps counterintuitively, greater CSA severity is often associated with denial and non-disclosure (Hershkowitz et al., 2007; Leander, 2010; Smith et al., 2000). For example, Leander (2010) reported that survivors of more severe forms of CSA and chronic CSA were more likely to deny CSA experience when asked about it in childhood. Greater severity of CSA is also associated with delay. Hershkowitz et al. (2007) interviewed 30 children suspected of experiencing extrafamilial CSA and found that a greater number of survivors of severe CSA and chronic CSA cases delayed disclosure than survivors of less severe CSA and single-incident CSA cases (see also Smith et al., 2000).
Although severe CSA may at times result in childhood denials and delays in reporting, more severe CSA is also more likely to be remembered years later. In adulthood, severe abuse might make victims more likely to disclose: Goodman et al. (2003) conducted a longitudinal study of children who had testified as victims in criminal prosecutions. More than a decade later, when the victims were interviewed about their lives, they were more likely to disclose CSA if it had been more severe. The traumatic impact on individuals’ lives is likely to be greater when severe CSA was experienced, resulting in stronger memory even into adulthood (Goodman et al., 2018). Here, we examined abuse severity in relation to our study’s four disclosure categories.
Trauma-Related Symptoms
Disclosure is believed to result in better mental health by relieving children and adults from the burden of secret keeping caused, for example, by shame (Easton et al., 2014; Goodman et al., 2017). Concerns exist that denial in childhood can lead to greater trauma-related symptoms later in adulthood (Paine & Hansen, 2002). For example, if CSA was being experienced, lack of childhood disclosure could result in children remaining in an abusive home and not obtaining needed services; CSA disclosure at T2 in adulthood could indicate that the childhood abuse had been occurring at T1. Thus, we examined whether participants who fell in the deferred disclosure category reported higher levels of trauma-related symptoms at T2.
Current Study
Disclosure of CSA is often a process that can continue for years. However, as Alaggia et al. (2019) argue, most empirical studies are cross-sectional or rely on retrospective reporting. There is a dearth of longitudinal studies. The lack of clarity in the literature led to our research questions: How do disclosures of CSA change over time? Are disclosures of CSA in childhood consistently maintained in adulthood, or do adults who had denied CSA in childhood now confirm the earlier suspicions of CSA? For children who claimed CSA at T1, how likely are they to recant? Can we identify significant predicators of disclosure patterns?
Based on the literature reviewed above, several sets of hypotheses were tested: 1. Consistency hypothesis: Older T1 age, being female, and experiencing more severe CSA will be related to more consistent CSA disclosure across T1 and T2. 2. Gender/denial hypothesis: Males will be more likely than females to defer disclosing (deny at T1 and disclose at T2), recant at T2, and consistently deny. 3. Trauma-related symptoms hypothesis: Consistent with Paine and Hansen’s (2002) proposal, we expected that CSA denial at T1 followed by disclosure at T2 (deferred disclosure) would be associated with higher trauma symptoms scores at T2. We did not expect other response categories (e.g., disclosure at T1 or consistent denial, which could indicate lack of CSA) to be significantly related to higher T2 trauma symptom scores.
We also examined the influences of race and post-forensic unit trauma experiences on disclosures and denials.
Method
Participants
Participants were 99 adults (66 women) who had participated in both timepoints of a longitudinal study examining long-term outcomes of childhood maltreatment. At T1, they ranged in age from 3- to 16-years-old (M = 8.17, SD = 3.28). Researchers re-interviewed the participants approximately 20 years later (T2). Participants were then 23- to 37-years-old (M = 28.22, SD = 3.28). The sample was primarily Black (73%), followed by Caucasian (non-Hispanic) (12%), Hispanic/Latinx (11%), and Native American (2%). An additional 2% of participants did not identify with any of the aforementioned options. At T2, the majority of participants reported comparatively low incomes: 82.8% of the sample reported a household income under $35,000/year, and 64.6% reported a household income under $20,000 per year.
Measures
T1
Demographics Questionnaire
This questionnaire, created for the T1 study and completed by forensic unit staff, covers information such as the participants’ gender, age, and race.
Interview Questionnaire
This measure, completed by staff psychologists at the forensic unit, provides information on participants’ disclosures of CSA at T1. The questionnaire permits indication of a child’s disclosure, denial, or non-disclosure of abuse during a psychological or forensic interview. Specifically, a yes versus no option is offered to indicate if the child disclosed or not. Detail is also provided, indicating if a denial or non-disclosure occurred.
Global Adaptive Functioning
The Global Adaptive Functioning (GAF) assesses children’s psychological, social, and educational functioning on a scale from 1 to 100, with lower scores indicating poorer adaptive functioning. It is based on criteria from the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 1995) and is very similar to the Global Assessment Scale (Endicott et al., 1976). It was completed by the forensic unit psychological staff or psychological consultants.
T2
Demographics Questionnaire
This form, created for the T2 study, covers information such as the participant’s age, race, education status, and annual household income.
Trauma Symptom Checklist
The Trauma Symptom Checklist (TSC-40; Elliott & Briere, 1992) is a self-report measure that contains 40 items meant to assess distress in adulthood resulting from traumatic experiences. Items include “fear of men,” “flashbacks (sudden, vivid, distracting memories),” or “feeling that you are not always in your body.” Each item is rated on a 0 (never) to 3 (very often) scale to examine symptom frequency over the previous 2 months. A higher score indicates more trauma symptomatology. Our sample displayed high reliability, α = .93.
Post-Forensic Unit Trauma Index
This measure, created for the T2 study, assesses trauma experiences that occurred after the investigation at the forensic unit. This includes whether the participant experienced corporal punishment, physical abuse, sexual abuse, emotional abuse, neglect, sex trafficking, and/or domestic violence after leaving the forensic unit. A higher score indicates more post-forensic unit trauma experiences. For details about the questions, see Wu et al. (2021) and Quas et al. (2005).
Procedure
The T1 study was approved by the university’s Institutional Review Board (IRB) and several other IRBs of relevance (Eisen et al., 2021). T2 was approved by the university’s IRB.
T1
At T1, children were placed into a forensic unit for an in-patient forensic evaluation due to one or more allegations or suspicions of maltreatment (primarily intrafamilial). These included allegations of sexual abuse as well as allegations of physical abuse and neglect. While at the forensic unit, usually a 5-day stay, children were assessed for all maltreatment types, regardless of the allegations at admission. These exams were conducted by medical staff, psychologists, and other trained professionals. All participants underwent a full medical exam and psychological interview, and participants whose cases were being considered for prosecution also underwent a forensic interview, the “child development interview,” also taking place at the unit.
The psychological interview involved meeting with a psychologist who built rapport with the child and then explicitly asked the child whether they had experienced physical abuse, corporal punishment, neglect, and/or sexual abuse (using child-appropriate language). A specific yes/no question regarding possible CSA was asked. The interviewer first ensured that the children knew where their private parts were and could point to them. The interviewer then asked, “Has anyone touched your private parts?” If the participant indicated “Yes,” the psychologist asked follow-up questions about the participant’s disclosure to ascertain more details about the possible maltreatment. If the child answered “No,” a denial was noted. At the end of the session, the psychologist completed the Interview Questionnaire.
If criminal charges were considered, the child development interview was conducted by a trained social worker from the District Attorney’s office. The interviewer asked a yes/no question about private-part touch. At the end of the forensic interview, the interviewer also completed the Interview Questionnaire. As these interviews took place in the 1990s, science-based protocols were not used. Interviews covered CSA and other maltreatment types.
T2
T2 took place 20 years (M = 20 years; SD = 0.65) after the stay on the forensic unit. All T2 interviews were conducted over the phone, except for three that were conducted in person. Participants were told this study was to better understand the experiences of children and adolescents who had grown up in [city name] in the 1990s and would involve participating in two separate phone call interviews with a researcher (Sessions 1 and 2).
Coding
Coding of Dependent Variables: Consistent Disclosure, Deferred Disclosure, Recantation, and Consistent Denial.
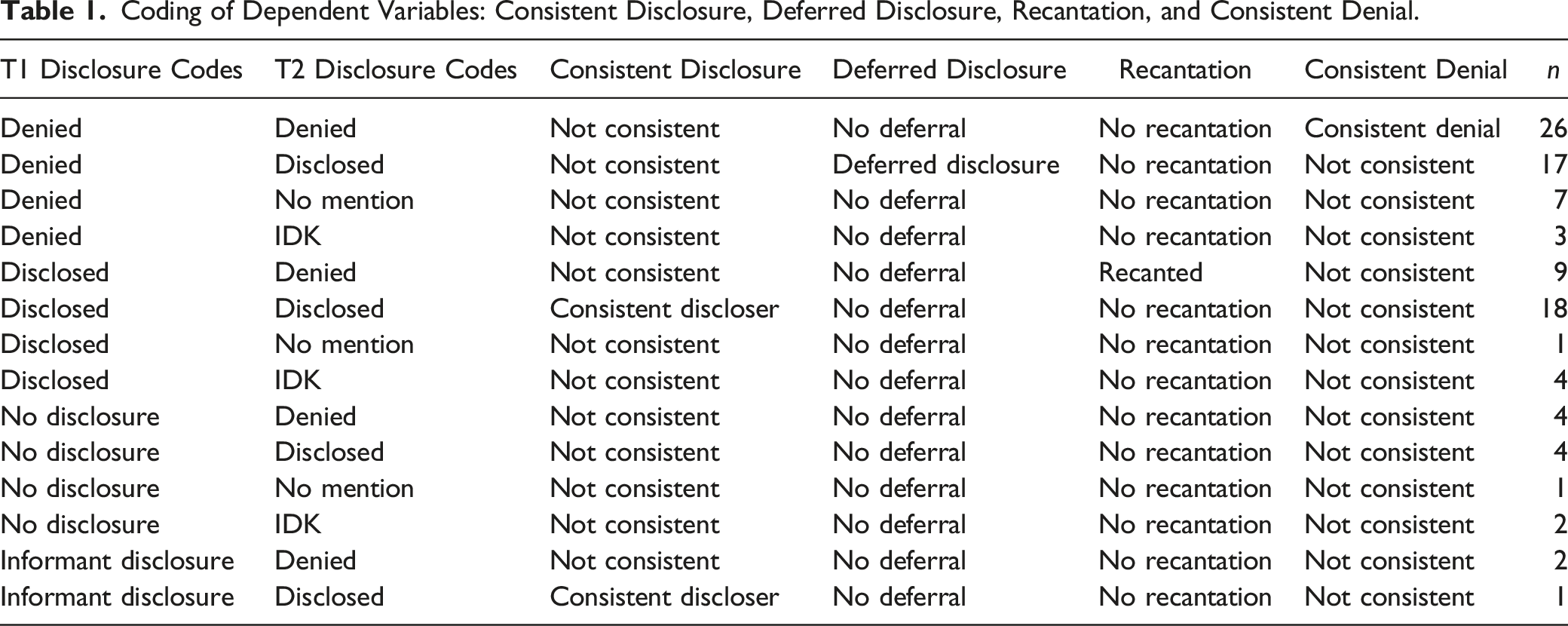
T1 and T2 disclosures and denials were then compared to create dependent variables (Table 1): consistent disclosure, deferred disclosure, recantation, or consistent denial. All four variables were created as binary variables (0 = Not consistent/no deferral/no recantation, 1 = Consistent/deferral/recanted, respectively). This allowed for the inclusion of as many participants as possible and is in line with how other researchers have utilized disclosure variables in their analyses (e.g., Kogan, 2004; McElvaney et al., 2020; Schӧnbucher et al., 2012). All but three participants had been asked if they had experienced sexual abuse at T1. Participants who disclosed CSA at T1 and T2 were deemed consistent disclosers. Participants who denied at T1 and T2 were deemed consistent deniers. Participants who denied CSA at T1 but disclosed CSA at T2 were coded as deferred disclosers. Participants who disclosed CSA at T1 but denied CSA at T2 were coded as recanters. The three not asked at T1 had refused to answer questions and left the interview before the question could be asked. They were coded as T1 non-disclosers (see Supplemental File). We use the term deferred disclosure in this paper to represent participants who explicitly denied CSA at T1 and disclosed CSA at T2 because explicit denial prior to disclosure is not required for delayed disclosure in the extant literature.
Analysis Plan
A power analysis conducted by G*power for continuous independent variables showed a total of at least 40 participants needed for detecting a medium effect (OR = 3.47) with power of .80. Although the power analysis for dichotomous independent variables indicated a need for 161 participants to detect a medium size effect, we were able to establish the replicability of our findings through Structural Equation Modeling (SEM). (Statistics on the representativeness of our sample and details about the SEM and its ability to establish the replicability of our findings are provided in the Supplemental File).
We examined descriptive statistics (e.g., crosstabs, correlations) of disclosure and denial codes at T1 and T2. Next, given binary dependent variables (e.g., 0 = No deferral, 1 = Deferral), we conducted logistic regressions. Across all models, VIF (a measure of multicollinearity among the predictor variables) ranged from 1.00 to 1.26, falling within acceptable levels (Rogerson, 2010). The number of participants varies due to missing data; therefore, n’s per analysis are indicated. All significant effects are reported.
Unless specified otherwise, all regressions use the following model order: In the first model, T1 age in months (continuous), gender (0 = male, 1 = female), and race (0 = Not Black, 1 = Black) were entered. The second model added the T1 CSA severity score. The third model added the T2 post-forensic unit trauma index (z-scored proportion score). The fourth model added the T2 TSC-40 total score. For all regressions, Model 1 examines and then statistically controls for demographics. Models two to 4 are chronologically organized. This ensures that variables (e.g., post-forensic unit trauma in Model 3) that could affect the dependent variable are examined and then statistically controlled before investigating a variable of interest measured in adulthood (e.g., TSC-40). In this way, we can identify unique predictors of the dependent variable (Cohen et al., 2003).
Results
Descriptive Data
Of the 99 participants in our sample (numbers equal percentages, except where indicated), at Time 1, 32 disclosed having experienced CSA, 53 denied CSA, 11 made no disclosure, and 3 made an informant disclosure (disclosed that CSA happened to someone else). In comparison, at T2, 40 participants disclosed experiencing the target CSA, and 41 responded with a target CSA denial. An additional nine participants never mentioned having experienced CSA, and nine participants were unsure as to whether they had experienced CSA.
A crosstabs revealed 18 participants were “consistent disclosers”; at both T1 and T2 they disclosed CSA (56.3% of those who disclosed at T1). However, 17 participants made deferred disclosures, specifically, they had denied experiencing CSA at T1 but disclosed CSA at T2 (32.1% of those who denied at T1). Conversely, nine participants made recantations: They disclosed CSA at T1 but then denied CSA at T2 (28.1% of those who disclosed at T1). A total of 26 participants were “consistent deniers”; at both timepoints they denied experiencing CSA (49.1% of those who denied at T1).
Main Analyses
Means, Standard Deviations (SDs), Range, and Correlations of Key Variables.
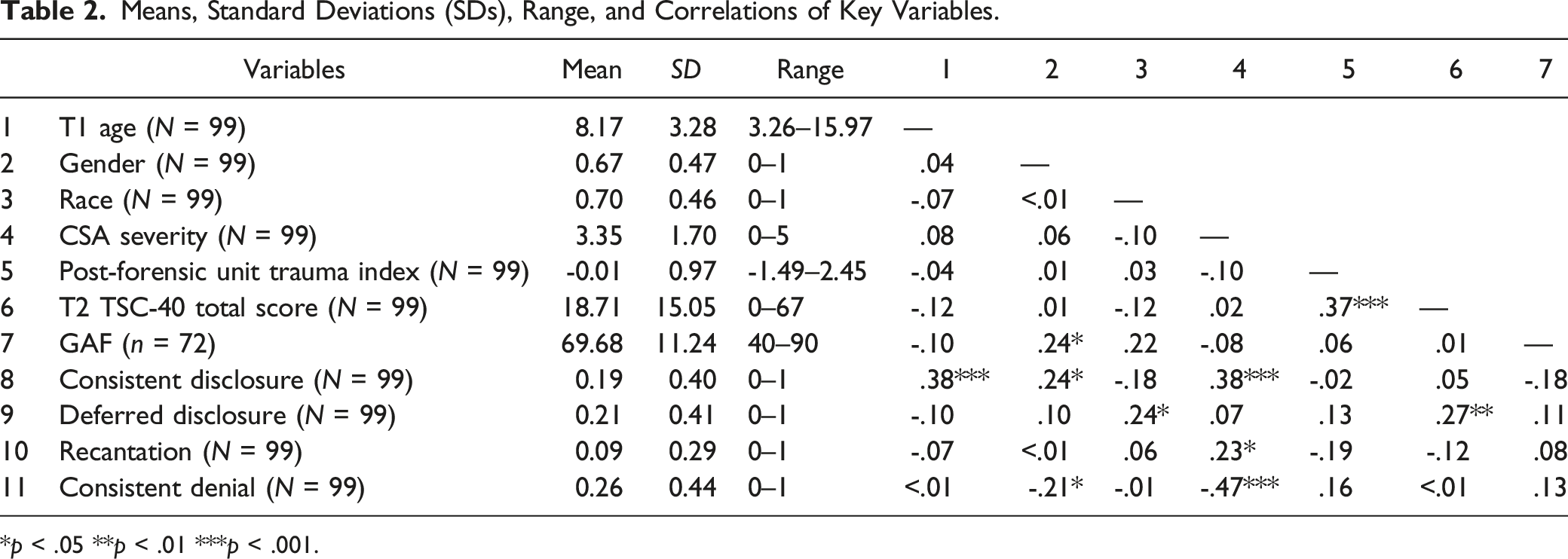
*p < .05 **p < .01 ***p < .001.
Logistic Regression of Consistent Disclosure, Deferred Disclosure, Recantation, and Consistent Denial.
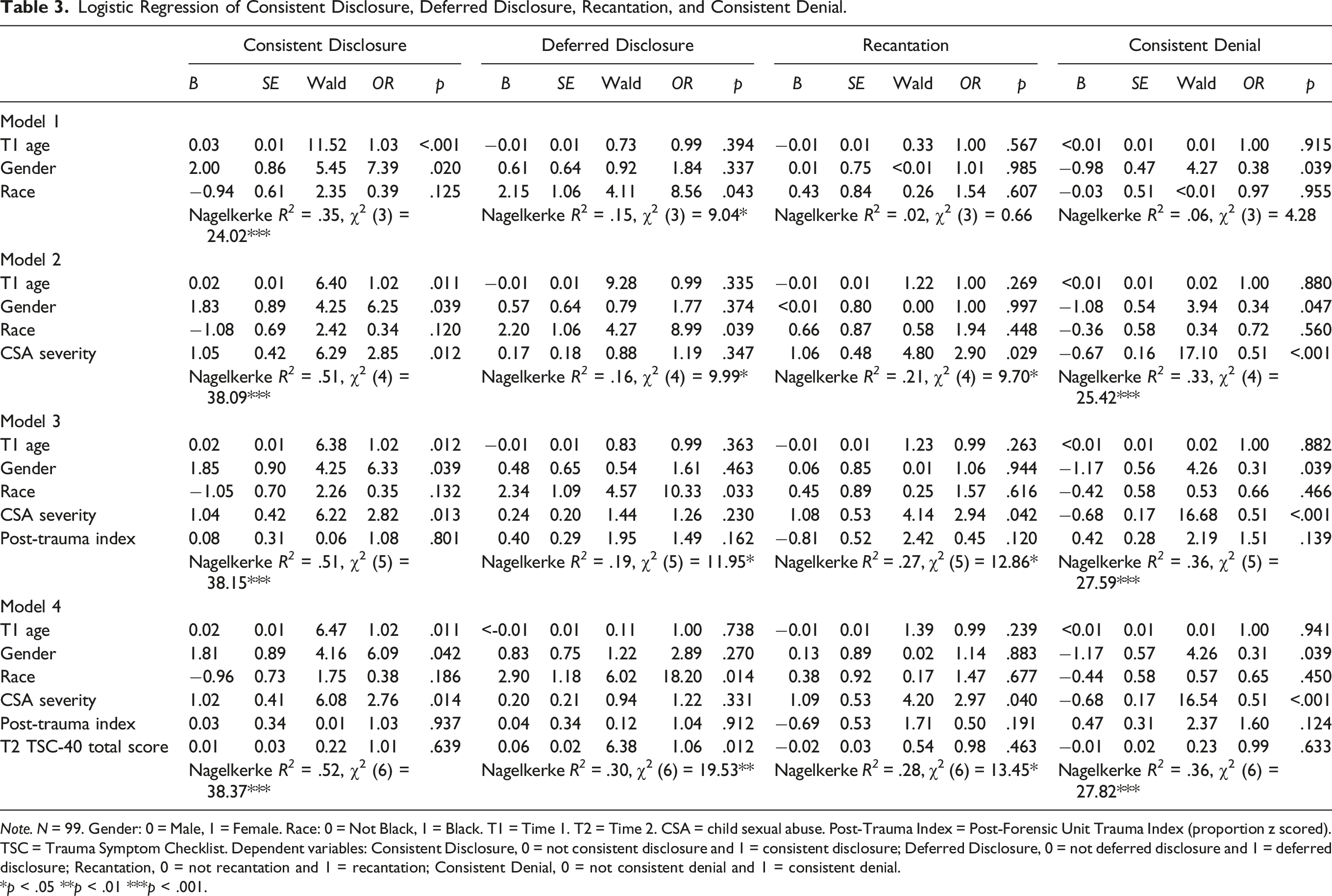
Note. N = 99. Gender: 0 = Male, 1 = Female. Race: 0 = Not Black, 1 = Black. T1 = Time 1. T2 = Time 2. CSA = child sexual abuse. Post-Trauma Index = Post-Forensic Unit Trauma Index (proportion z scored). TSC = Trauma Symptom Checklist. Dependent variables: Consistent Disclosure, 0 = not consistent disclosure and 1 = consistent disclosure; Deferred Disclosure, 0 = not deferred disclosure and 1 = deferred disclosure; Recantation, 0 = not recantation and 1 = recantation; Consistent Denial, 0 = not consistent denial and 1 = consistent denial.
*p < .05 **p < .01 ***p < .001.
Consistent Disclosure
To determine significant predictors of consistent disclosure across the 99 participants, the consistent disclosure dependent variable (coded as 0 = Not consistent and 1 = Consistent) was tested in a binary logistic regression. As shown in Table 3, participants who were older at T1 and females were more likely to be consistent disclosers. Participants with higher T1 CSA severity scores were more likely to disclose consistently from T1 to T2.
Deferred Disclosure
To determine significant predictors of deferred disclosure across the 99 participants, the deferral dependent variable (coded as 0 = No deferral and 1 = Deferral) was tested in a binary logistic regression. Race was significant: Black (compared to non-Black) participants were more likely to deny CSA at T1 and then disclose CSA at T2. The TSC-40 total score was also significant: Adults with more trauma-related symptoms at T2 were more likely to have made a deferred disclosure.
Binary Logistic Regressions of T1 Deniers (n = 53) and T1 Disclosers (n = 32).

Note. Gender: 0 = Male, 1 = Female. Race: 0 = Not Black, 1 = Black. T1 = Time 1. T2 = Time 2. CSA = child sexual abuse. Post-Trauma Index = Post-Forensic Unit Trauma Index (proportion z scored). TSC = Trauma Symptom Checklist. Dependent variables: Deferred Disclosure, 0 = not deferred disclosure and 1 = deferred disclosure; Recantation, 0 = not recantation and 1 = recantation.
*p < .05 **p < .01 ***p < .001.
However, a new result emerged: In the T1 deniers only analysis, CSA severity was significant; more severe CSA predicted deferred disclosure for that subgroup even when demographic variables were statistically controlled. Also, when T1 GAF score (our proxy for T1 behavioral adjustment; n = 72) replaced the post-forensic unit trauma score (non-significant in all analyses), T1 GAF was not significant but the T2 TSC-40 remained a significant predictor of deferred disclosure, Wald = 5.93, OR = 1.07, p = .015. Thus, T1 behavioral adjustment, as captured by GAF, did not explain the finding that T2 TSC-40 was significantly related to deferred disclosure in this subset of participants.
Recantation
The recantation dependent variable (coded as 0 = No recantation and 1 = Recantation) was also tested in a binary logistic regression. CSA severity was the only significant predictor: Adults with higher T1 CSA severity scores were more likely to recant.
The analysis of recantation just described included participants who did not disclose at T1. It could be argued that recantation for them is not a logical possibility. Thus, because T1 disclosure was a prerequisite to be in the recantation category, a separate logistic regression was conducted with all who disclosed at T1 (n = 32). This analysis compared those classified in the T2 recantation category to those who disclosed at T1 but at T2 disclosed/did not disclose (but did not deny)/said “don’t know” or “maybe” (Table 4). Despite loss in statistical power (due to the reduced sample size), the direction of the results was consistent with those of the larger sample.
Consistent Denial
When a binary logistic regression of predictors of consistent denial (coded as 0 = Not consistent and 1 = Consistent) was conducted, CSA severity was significant: Less severe CSA was associated with consistent denial. Although Model 1 was not significant, the logistic regression produced an OR for gender that was significant. Because a gender effect was hypothesized but the logistic regression reduces degrees of freedom, a partial correlation was conducted to examine further whether gender was associated with consistent denial. With age and race partialled, males were significantly more likely than females to consistently deny, partial r (95) = -.21, p = .038.
Corroboration
Corroboration was defined as medical evidence, a confession, or an eyewitness (e.g., a parent or sibling witness). A new analysis was conducted in which the post-forensic unit trauma variable was removed; it was replaced with the variable presence/absence of corroboration (0 = no corroboration and 1 = corroboration; n = 97). Corroboration was not a significant predictor of consistent disclosure, Wald = 2.65, OR = 3.53, n.s.; deferred disclosure, Wald = 2.67, OR = 0.24, n.s.; or consistent denial, Wald = 0.04, OR = 1.18, n.s. However, compared to cases without recantation, cases with recantation were more likely to have been corroborated, Wald = 5.28, OR = 16.16, p = .022 (see Supplemental File for detail).
Discussion
Longitudinal data permitted us to examine consistency and changes in disclosure of CSA between childhood and adulthood. For a considerable portion of our sample, 42.4%, there were changes in disclosure. Specifically, 17.2% of our sample deferred disclosure (denied at T1 and disclosed at T2) and 9.1% of our sample recanted (disclosed at T1 and denied at T2). The other 16.1% made changes in disclosure that did not fit into our coding scheme of deferred disclosure or recantation (e.g., they disclosed at T1 and responded “I don’t know” at T2).
Age
T1 age was positively related to consistent disclosures. Children who were older at T1 were also more likely to consistently provide a T1 and T2 disclosure. One possibility is that older participants at T1 were accurately disclosing the abuse at T1, perhaps realizing the importance of their disclosures for their own safety and well-being (Wu et al., 2021), and continued to accurately disclose abuse at T2. This fits with other research showing that older children and adolescents are more likely than younger children to make purposeful disclosures (Campis et al., 1993; Nagel et al., 1997) and Azzopardi et al.’s (2019) meta-analysis that indicated older age predicts disclosure in forensic interviews. However, another possibility is that older children were more likely to remember what they said initially at T1 and be consistent with it at T2. T1 age did not significantly predict the other disclosure or denial categories.
Gender
Gender differences were found in disclosure of CSA (females disclosed more consistently than males, and males denied somewhat more consistently than females). Counter to our hypothesis, we did not find significant gender differences in deferred disclosure and recantation. This was surprising when one considers how prevalent gender effects are in research on delayed disclosure and empathy toward child victims (Bottoms et al., 2007; Easton et al., 2014; O’Leary & Barber, 2008; Stoltenborgh, 2011; Wallis & Woodworth, 2020). However, of the 33 males in our sample, only seven disclosed CSA at T1 and seven disclosed at T2 (but only two of the males disclosed at both timepoints). Thus, our findings may indicate that males were not willing to disclose (Eisen et al., 2021), as children or adults, which would make it difficult to find any gender differences in delayed disclosure or recantation.
Race
Few race differences were found, except in deferred disclosure. When we examined specifically who in our sample denied in childhood and disclosed in adulthood, Black participants were especially likely to defer disclosure. One possibility is that this reflects these parents’ and children’s lack of trust at T1 in government-related agencies, like child welfare services and the courts, and the medical establishment, such as the doctors and psychologists who were conducting the physical exams and interviews (e.g., Cleveland & Quas, 2020; Fine et al., 2019).
Trust is of vital importance when deciding whether to disclose abuse—lack of trust inhibits abuse disclosures (Brennan & McElvaney, 2020; Capella et al., 2016; Easton et al., 2014; Schönbucher et al., 2012). Further research should examine this issue and, if validated, appropriate training should be conducted to account for relations between racism, trust, and CSA disclosure (Hope et al., 2022).
CSA Severity
Consistent with our prediction, more severe CSA was associated with consistent disclosure, but also with recantation and deferred disclosure, the last only when the smaller T1 denier subsample was considered. For the consistent disclosure group and the deferred disclosure subgroup, these findings are in accord with other research indicating that more severe CSA results in more robust memory (Goodman et al., 2019). Still, it was surprising that adults who allegedly experienced more severe abuse were more likely to recant.
Recantation
By denying that CSA occurred, children who disclosed at T1 and, as adults, recanted at T2 could avoid discussing a potentially distressing experience that often implicated family members. Alternatively, the T1 CSA disclosure could have been false (Ceci & Bruck, 1995; Otgaar et al., 2022), perhaps especially given the leading nature of the T1 interviewing. However, corroborative evidence was more likely for those who recanted than for others, increasing the likelihood that CSA occurred.
Our ability to analyze recantation was limited by the small number (n = 9) of adults who recanted. We carefully examined each of the nine files. The T1 situations for the children were diverse. Several, but not all, had been sexually abused by older siblings, with physical findings of rape or adult eyewitnesses to the rapes. Three of the nine were quite young (4 years old or younger); thus, T2 childhood amnesia or T1 false reporting may have played a role in their T2 recantations. However, some of the children were old enough to have remembered the CSA but likely were avoiding the memory or avoiding acknowledging to us what had happened. For example, at T1, a pregnant 13-year-old said the CSA was perpetrated by her mother’s boyfriend. This 13-year-old gave birth to and raised the child who resulted from the rape. At T2, as an adult, this same victim said she had never been sexually abused, did not remember being at the forensic unit, and said “never” to all trauma symptoms. Further research is needed to determine if the relation between abuse severity and recantation generalizes beyond our sample and if avoidance of discussing abuse is the driving factor behind this relation (e.g., for older children), as more definitive findings could hold important legal implications.
Trauma-Related Symptoms
More trauma-related symptoms at T2 (TSC-40 total score) were not significantly associated with consistent disclosure, recantation, or consistent denial, but deferred disclosure was significantly related to a greater number of trauma symptoms (even with CSA severity controlled). Both Easton (2019) and Ullman and Filipas (2005) found that participants who disclosed soon after the abuse, or at least within a year, reported better mental health (e.g., lower PTSD symptoms) than those who delayed their disclosures. Disclosure of abuse is often an important step in helping child survivors access resources (e.g., therapy), and receive support from friends and family. The two groups that disclosed at T1 likely had access to these resources, which may have improved their mental health, whereas denial of CSA that was occurring apparently contributed later to trauma symptoms for the deferred disclosure group.
We examined the possibility that T1 maladaptive functioning was related to deferred disclosure, perhaps inhibiting participants from disclosing earlier or being related to disclosure in adulthood. However, T1 GAF scores (available for a sufficient number of participants) were not a significant predictor of deferral. At T1, self-conscious emotions such as shame, or the desire to return home or protect the perpetrator might have prevented disclosure (e.g., Block et al., 2010; Easton et al., 2014). Thus, survivors of CSA who deny initially might enter into a vicious cycle in which they feel a barrier to disclosure, and their lack of disclosure in childhood prevents them from accessing early treatment for trauma-related symptoms. Further research is needed to verify the existence of this cycle, and if it exists, to identify ways in which to disrupt it.
Qualitative Remarks
We would be remiss without adding a few anecdotal observations, especially about the deferred disclosure group. Many participants in the deferred disclosure group indicated at T2 that they had denied the CSA at T1 in the hope they could return home despite the maltreatment. Some had been in foster care previously and did not want to return there. Also mentioned were obstacles such as fear of negative consequences, feeling uncomfortable talking about CSA, and not understanding the vocabulary interviewers used to ask about their experiences. One participant touched on several themes when she discussed why, at the forensic unit at age 7, she denied CSA when asked: I was nervous because…I didn’t know what to say. Would it get me in trouble or would it get me taken away from my mom because I didn’t want to go anywhere….They were asking me…have I ever been like sexually abused and things like that. And I didn’t know some of those words so…you know I started crying because I was feeling uncomfortable.
Legal Implications
There is a paucity of longitudinal research that tracks CSA disclosures over time; especially lacking are studies that examine CSA disclosures decades apart. Despite this, researchers and practitioners recognize that disclosure is an iterative process that evolves over time. How this process unfolds can hold heavy legal implications. For example, to the extent that the adults in our study disclosed accurately about their childhood experiences, the percentage of false denials in childhood was 17%. Even with T1 behavioral functioning statistically controlled, deferred disclosure was related to higher levels of adult trauma symptoms. For such individuals, there is a pressing need in childhood for forensic interviewers and legal actors to determine if the denial is true or false, and if the denial is false, to intervene. Denials, even if false, are often believed by adults (Block et al., 2012), who could be informed (e.g., by experts) about the potential dangers of false denials. Moreover, deferred and other non-disclosures in childhood, if followed by disclosure in adulthood, can result in investigations and hearings that take place long after the last incident of abuse. With the recent extensions of the statute of limitations for CSA cases in many states, the fact of denying in childhood affects adults’ perceived credibility, adding to the loss of evidence (e.g., corroborating witnesses) with time.
To the extent that a true recantation occurs, it could mean that an innocent person was indicted and possibly sentenced, or at the least experienced a loss in reputation, which could have severe repercussions for that person’s life. However, the rates of recantation in this study were relatively low, and our findings on corroboration suggest that not all the recantations were “true.” While the present study was limited, as the majority of studies in this area are, by our inability to determine with complete confidence the truth of what occurred (i.e., whether there was CSA or not), the longitudinal nature of this study provides a perspective lacking in the extant literature.
Additionally, this study addresses these issues in a population historically under-represented in this area of research: primarily Black and of low socio-economic status. We found that Black participants and participants with greater adult trauma-related symptoms at T2 were more likely to have deferred disclosure (i.e., denied in childhood). What were the barriers that prevented them from disclosing at T1? Why did they disclose at T2? Further research is needed to better understand these barriers, especially in non-White populations. Such research would be informative for many of the actors in our legal system, from the professionals who conduct forensic interviews with children to the prosecutors responsible for trying cases of CSA.
Limitations
The replicability and generalizability of our findings needs to be established. As with many longitudinal studies, there was attrition, and thus not all T1 participants were included in our T2 sample. Our sample was comprised primarily of Black participants, but CSA is not limited to any single race or ethnicity. Virtually all the children in our sample were involved with child protective services, so abuse had been raised as an issue prior to their inclusion in our study. Some participants had made disclosures of CSA prior to their admittance to the forensic unit (Eisen et al., 2021). Furthermore, all participants had their abuse actively investigated. Many survivors of CSA do not have their abuse reported to authorities, much less investigated, which may have influenced memories and subsequent disclosures at T2.
The T1 forensic interviews did not use science-based protocols as they were conducted prior to the widespread adoption of such protocols. This may have affected T1 disclosure rates.
At both T1 and T2, the interviewers tried to build rapport with the study participants. However, CSA is an uncomfortable topic for many. Some participants may have falsely denied the experience, or downplayed its severity, because they did not want to discuss that part of their life with a stranger. That said, it may be easier to talk confidentially to a sympathetic stranger than to people who matter in one’s life. Finally, we could not always determine the accuracy of the disclosure or denial with certainty.
Conclusion
For many survivors of CSA, willingness to disclose changes between childhood and adulthood. It is essential to understand how the disclosure process changes with age. Also, more research is needed on how cultural factors influence disclosures.
Supplemental Material
Supplemental Material - Childhood Sexual Abuse: A Longitudinal Study of Disclosures and Denials
Supplemental Material for Childhood Sexual Abuse: A Longitudinal Study of Disclosures and Denials by Dana T. Hartman, Yan Wang, Daisy Vidales, Gail S. Goodman, Yuerui Wu, Deborah Goldfarb, Jianjian Qin, and Michell L. Eisen in Child Maltreatment
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the U.S. Children's Bureau (90-CA-1554), National Science Foundation (1424420 ), (2037583), National Institute of Justice (2013-IJ-CX-0104).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.