
Abstract
This study explored the prevalence and correlates of elder mistreatment among community-dwelling Chinese women in the U.S. Data were from the Population Study of Chinese Elderly in Chicago (PINE), a population-based study of U.S. Chinese older adults aged 60 years and above. Of the 1,833 older women, 289 (15.8%) reported suffering from elder mistreatment. Higher educational levels, lower overall health status, and worsening health over the past year were positively correlated with elder mistreatment, while a greater number of children and grandchildren were negatively correlated with elder mistreatment. Considerable efforts should be put into designing tailored interventions to reduce elder mistreatment in U.S. Chinese women.
Introduction
According to the report from the National Research Council, elder mistreatment refers to intentional actions that cause harm or create a serious risk of harm (whether or not harm is intended) to a vulnerable elder by persons in a trust relationship to the elder or failure by a caregiver to satisfy the elder’s basic need or to protect the elder from harm (Bonnie & Wallace, 2003). Elder mistreatment often encompasses physical abuse, psychological abuse, sexual abuse, elder neglect, and financial exploitation. Elder mistreatment is a health and human rights issue. The National Elder Mistreatment Study found that approximately 11.4% of U.S. older adults experienced some type of elder mistreatment in the past year (Acierno et al., 2010). In another nationally representative elder mistreatment study of 3,005 older adults using the Hwalek–Sengstok Elder Abuse Screening Test (H-S/EAST) and the Vulnerability to Abuse Screening Scale (VASS), 9% of the participants suffered from verbal mistreatment, 3.5% were affected by financial mistreatment, and 1% experienced physical mistreatment (Laumann, Leitsch, & Waite, 2008). Elder mistreatment may result in adverse health outcomes such as physical and cognitive function decline, depression, loneliness, and increased risk of mortality (Dong, Beck, & Simon, 2009; Dong, Simon, De Leon, Fulmer, Beck, & Hebert et al., 2009). It is also linked to increased hospitalization (Dong & Simon, 2013a), emergency care use (Dong & Simon, 2013b), and nursing home placement (Lachs, Williams, O’Brien, & Pillemer, 2002).
Women may be more vulnerable to elder mistreatment. Although women on average have longer life expectancies than men, later life is often fraught with an array of morbidity and co-morbidity that may be related to elder mistreatment. In addition, compared with their male counterparts, older women may be more financially dependent on others and need more care and support, which further dispose them to higher risk of elder mistreatment. Prior studies on elder mistreatment suggested that women were overrepresented as victims of elder mistreatment (Acierno, Hernandez-Tejada, Muzzy, & Steve, 2009; Lachs & Berman, 2011). For instance, in a study of 4,156 older New Yorkers, 7.6% of the participants, among which 64.2% were women, experienced one type of mistreatment (Lachs & Berman, 2011). Moreover, emerging evidence demonstrated that older women tended to experience multiple types of elder mistreatment, and the mistreatment was associated with increased odds of reporting bone or joint problems, chronic pain issues and lung problems, and mental health issues such as depression and anxiety (Fisher & Regan, 2006). Despite the scope of elder mistreatment in older women, a prior study showed that less than half of the victims had disclosed the abuse experience to other people (Zink, Fisher, Regan, & Pabst, 2005). Mitigating violence against older women is a policy priority both internationally and nationally. The Violence against Women Reauthorization Act of 2013 includes funding to combat elder mistreatment, with special attention given to culturally specific and underserved populations. Despite the increasing research interest and public policy awareness, there are large knowledge gaps in our understanding of the issue of elder mistreatment in minority women.
The nature and experience of elder mistreatment in women may vary significantly by racial/ethnic groups. Influenced by traditional patriarchal values and beliefs, women in Chinese society tend to be subordinate to men socially and economically. The historically unequal gender norms and power relations may predispose Chinese women to higher risk of elder mistreatment. Cultural values may also affect the perception of elder mistreatment among Chinese older women. A qualitative study of elder abuse among Chinese Canadians found that disrespect was considered as a key form of elder mistreatment, suggesting the importance of integrating cultural and societal factors into understanding the issue of elder mistreatment (Tam & Neysmith, 2006). In Chinese culture, family relationship has been found to be strongly associated with older adults’ well-being (Chen, Simon, Chang, Zhen, & Dong, 2014). Thus, an unfavorable relationship with family members or family conflicts may cause harm to older adults’ well-being, triggering the occurrence of elder mistreatment. In addition, due to the societal stigma surrounding elder mistreatment and the intention of protecting family honor and dignity, Chinese older women may be less likely to disclose mistreatment experiences (Moon, Tomita, & Jung-Kamei, 2002). The vulnerability of Chinese older women necessitates an improved understanding of the issue of elder mistreatment in Chinese women.
Chinese Americans constitute the largest segment of the Asian American population in the United States. The number of U.S. Chinese older adults aged 60 years and older is estimated at 540,000, among whom 54.2% are women (U.S. Census Bureau, 2010). Due to significant language and cultural barriers, as well as a higher likelihood of social isolation, Chinese older women may be at greater risk of elder mistreatment. However, there is a paucity of research on the issue of elder mistreatment in U.S. Chinese older women. The objectives of this study are to (a) investigate the prevalence of elder mistreatment in U.S. Chinese older women, and (b) explore the correlates of elder mistreatment in U.S. Chinese older women.
Method
Population and Settings
The Population Study of Chinese Elderly in Chicago (PINE) is a community-engaged, population-based epidemiological study of U.S. Chinese older adults aged 60 and older conducted in the greater Chicago area. Briefly, the purpose of the PINE study was to collect community-level data of U.S. Chinese older adults to examine the key cultural determinants of health and well-being. The project was initiated by a synergistic community–academic collaboration among the Rush Institute for Healthy Aging, Northwestern University, and many community-based social service agencies and organizations throughout the greater Chicago area.
To ensure study relevance to the well-being of the Chinese community and increase community participation, the PINE study implemented extensive culturally and linguistically appropriate community recruitment strategies strictly guided by a community-based participatory research (CBPR) approach (Dong, Chang, Simon, & Wong, 2011). The formation of this community–academic partnership allowed us to develop appropriate research methodology in accordance with the local Chinese cultural context, in which a community advisory board (CAB) plays a pivotal role in providing insights and strategies for conducting research. Board members were community stakeholders and residents enlisted through more than 20 civic, health, social, and advocacy groups, community centers and clinics in the city and suburbs of Chicago. The board works extensively with the investigative team to develop and examine study instruments to ensure cultural sensitivity and appropriateness.
Study Design and Procedure
The research team implemented a targeted community-based recruitment strategy by first engaging community centers as our main recruitment sites throughout the greater Chicago area. More than 20 social service agencies, community centers, health advocacy agencies, faith-based organizations, senior apartments, and social clubs served as the basis of study recruitment sites. Community-dwelling older adults aged 60 years and older and self-identified as Chinese were eligible to participate in the study. Of 3,542 eligible older adults approached, 3,159 agreed to participate in the study, yielding a response rate of 91.9%. Details of the PINE study design are published elsewhere (Dong, Wong, & Simon, 2014).
To ensure cultural and linguistic sensitivity, trained multicultural and multilingual interviewers conducted face-to-face home interviews with participants in their preferred language and dialects, such as English, Cantonese, Toishanese, Mandarin, or Teochew dialect. Data were collected using state-of-science innovative web-based software which recorded simultaneously in English, Chinese traditional and simplified characters. Based on the available census data drawn from the U.S. Census 2010 and a random block census project conducted in the Chinese community in Chicago, the PINE study is representative of the Chinese aging population in the greater Chicago area (Simon, Chang, Rajan, Welch, & Dong, 2014). The study was approved by the Institutional Review Boards of the Rush University Medical Center.
Measurements
Basic demographic information included age (in years), sex (female and male), education (years of education completed), annual personal income (US$0-US$4,999, US$5,000-US$9,999, US$10,000-US$14,999, US$15,000-US$19,999, or more than US$20,000), marital status (married, separated, divorced, or widowed), number of children, living arrangement (living alone, living with one person, living with two to three persons, or living with four or more persons), and language preference (English, Toishanese, Cantonese, Mandarin).
Overall health status was measured by “In general, how would you rate your health?” on a 4-point scale (1 = poor, 2 = fair, 3 = good, 4 = very good). Quality of life was assessed by asking “In general, how would you rate your quality of life?” also on a 4-point scale ranging from 1 = poor to 4 = very good. Health changes over the last year were measured by “Compared to one year ago, how would you rate your health now?” on a 3-point scale (1 = worsened, 2 = same, 3 = improved).
Elder mistreatment was measured using a 10-item self-report instrument, derived from the H-S/EAST and the VASS (Hwalek & Sengstock, 1986; Schofield & Mishra, 2003). Participants were asked if they had (a) family conflicts at home, (b) felt uncomfortable with someone in the family, (c) felt that nobody wants them around, (d) been told by someone that they gave too much trouble, (e) been afraid of someone in the family, (f) felt that someone close tried to hurt or harm them, (g) been neglected or confined, (h) been called names or put down, (i) been forced by someone to do things, and (j) had belongings taken without permission. Prior studies have shown good face and construct validity of the VASS and the H-S/EAST measurements (Neale, Hwalek, Scott, Sengstock, & Stahl, 1991; Schofield & Mishra, 2003). The modified VASS has been administered to Chinese elderly populations both in mainland China and in the United States (Dong, Beck, & Simon, 2009; Dong, Simon, & Gorbien, 2007). The scale demonstrated good reliability in this study sample, with Cronbach’s alpha of .80 (Chang, Todd, Simon, & Dong, 2014).
Data Analysis
We used descriptive statistics to summarize demographic information of the participants. Chi-square statistics were used to compare the socio-demographic and health-related characteristics between groups with and without any elder mistreatment. Pearson’s correlation coefficients and Spearman’s rank correlations were calculated to determine the relationship of the socio-demographic and health-related variables with elder mistreatment. All statistical analyses were undertaken using SAS, Version 9.2 (SAS Institute Inc., Cary, North Carolina).
Results
Sample Characteristics
The sample comprised 1,833 older women. The average age of the older women was 72.9 years (SD = 8.6), and the average education was 7.8 years (SD = 5.1). A substantial percentage of (15.8%) older women reported experiencing any mistreatment. More specifically, feeling uncomfortable with someone in the family was the most common form of elder mistreatment (9.9%), followed by having family conflicts at home (6.6%) and being called names or put down (6.4%). In addition, 4.9% of the study participants felt that nobody wanted them to be around, and 3.3% of the participants had been told that they gave too much trouble.
Characteristics of the study participants with elder mistreatment are presented in Table 1. Compared with women without any elder mistreatment, women who experienced elder mistreatment were more likely to be less than 80 years old (86.5% vs.77.3%, p < .01), with an educational level of more than 13 years (32.0% vs. 14.1%, p < .001), separated or divorced (8.1% vs. 3.5%, p < .001), with zero to one child (18.4% vs. 12.8%, p < .001), having poor overall health status (30.5% vs. 18.7%, p < .001), having poor quality of life (4.5% vs. 2.2%, p < .001), and having worsened health status (52.6% vs. 41.7%, p < .001).
Characteristics of PINE Study Participants With Any Mistreatment in Older Women.
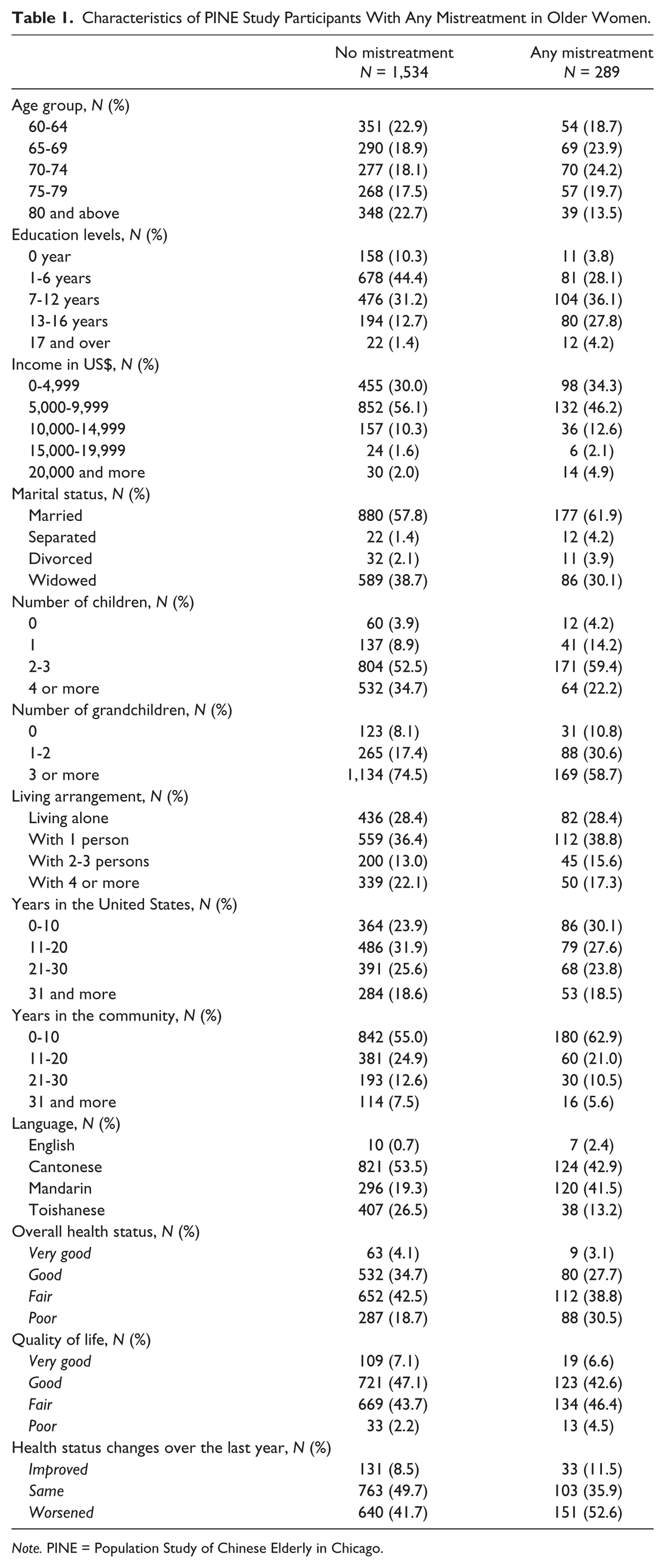
Note. PINE = Population Study of Chinese Elderly in Chicago.
Prevalence of Elder Mistreatment by Socio-Demographic and Family Composition Characteristics
The prevalence of elder mistreatment by age, education, income, language preference, marital status, living arrangement, number of children, and number of grandchildren is presented in Table 2. The prevalence of elder mistreatment is lowest among older women aged 80 years and above (10.1%). In addition, the prevalence of mistreatment increased as education levels increased, with older women with more than 17 years of education having the highest prevalence of elder mistreatment (35.3%). The prevalence of mistreatment was highest among older women at the highest income level (31.8%). As for the prevalence of elder mistreatment by language preference, older women speaking English had the highest prevalence of elder mistreatment experience (41.2%), followed by Mandarin (28.9%), Cantonese (13.1%), and Toishanese (8.5%).
Prevalence of Elder Mistreatment by Socio-Demographic and Family Composition Characteristics.
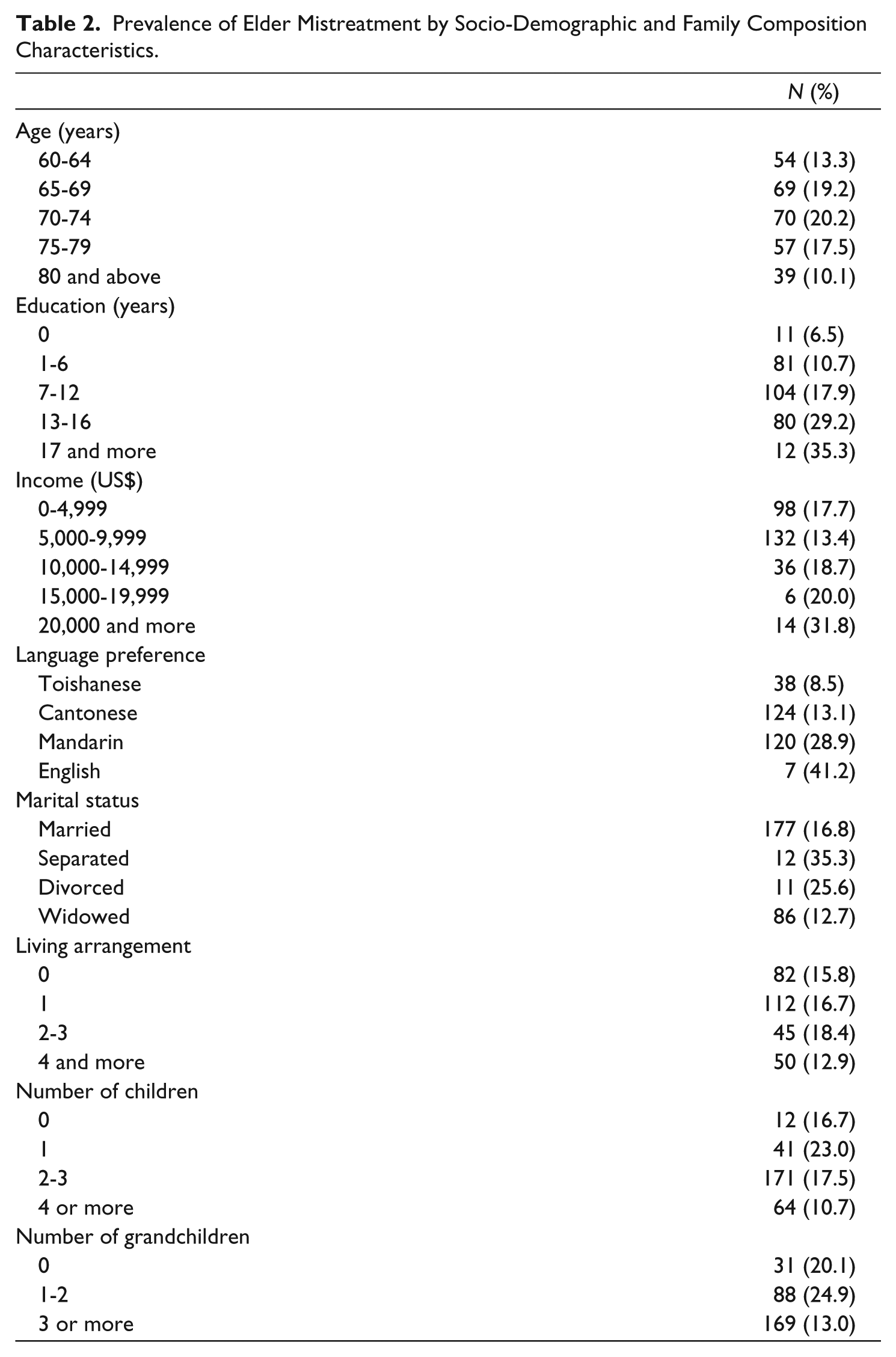
Older women who were separated (35.3%) or divorced (25.6%) reported having higher rates of elder mistreatment than married older women (16.8%) and widowed older women (12.7%). Older women living with two to three persons had the highest prevalence of mistreatment (18.4%) as compared with other living arrangement groups. In addition, older women with only one child had the largest proportion of elder mistreatment victims (23.0%). Similarly, older women with one to two grandchildren had a higher prevalence of elder mistreatment (24.9%) than older women with no grandchildren (20.1%) or those with three or more grandchildren (13.0%).
Correlation of Socio-Demographic and Health-Related Factors With Elder Mistreatment
The correlation of socio-demographic and health-related factors with elder mistreatment is presented in Table 3. A higher level of education (r = .19, p < .001), lower health status (r = .09, p < .001), and worsening health changes over the past year (r = .07, p < .01) were significantly and positively correlated with elder mistreatment. However, number of children (r = −.09, p < .001) and number of grandchildren (r = −.10, p < .001) were negatively correlated with elder mistreatment.
Correlates Between Elder Mistreatment and Socio-Demographic and Health-Related Characteristics in Older Women.
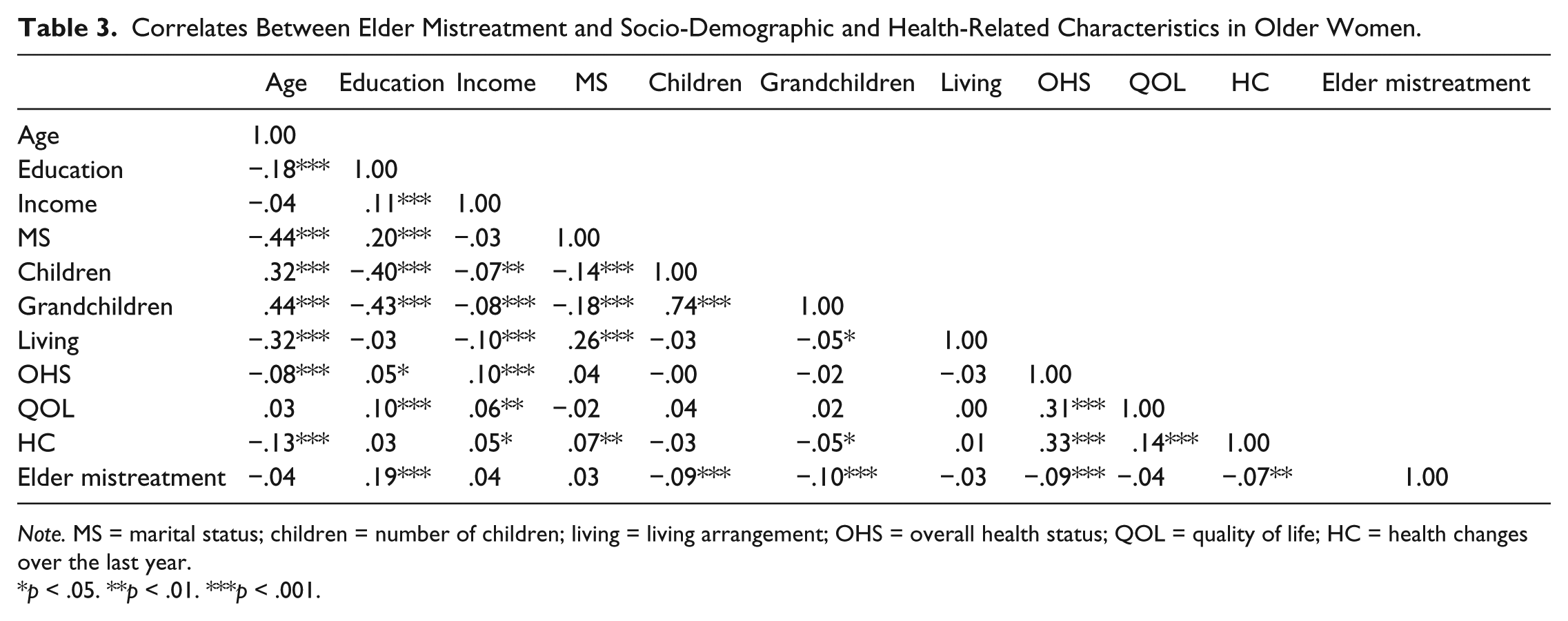
Note. MS = marital status; children = number of children; living = living arrangement; OHS = overall health status; QOL = quality of life; HC = health changes over the last year.
p < .05. **p < .01. ***p < .001.
Discussion
This study suggests that elder mistreatment was common in U.S. Chinese older women. The prevalence of elder mistreatment was higher among women who had higher levels of education, higher levels of income, lived with two to three persons, were separated or divorced, spoke English or Mandarin, had only one child, or had one to two grandchildren. Elder mistreatment was significantly and positively correlated with a higher level of education, lower health status, and worsening health changes over the past year, while negatively correlated with number of children and number of grandchildren.
Our study sheds light on the issue of elder mistreatment in U.S. Chinese older women. As the first large quantitative study of elder mistreatment in U.S. Chinese older women, this study contributes to a more comprehensive understanding of elder mistreatment in minority older women. In addition, our CBPR approach added rigor to the study methodology. With full community engagement and interviews conducted in the participant’s preferred dialect, participants may have been more comfortable, more trusting of research assistants, and more willing to express emotions and acknowledge their feelings.
Consistent with prior studies, this study suggests that elder mistreatment was prevalent in older women, with 15.9% of the participants indicating suffering from some form of mistreatment. In Chinese culture, older women tend to assume the role of “kin-keepers” that maintain the relationship between generations. We suspect that such gender roles may be beneficial to women’s well-being while exposing them to more frequent elder mistreatment. In particular, intergenerational relationships may be more fragile in immigrant households, where there are pronounced cultural and language gaps between generations. The prevalence of elder mistreatment in the present study is lower than the prevalence reported among older women in rural China (36.0%; Wu et al., 2012). The discrepancy may be due to older women in rural China being subjected to substantially different social and economic influences. The prevalence of elder mistreatment found in this study is also significantly lower than that reported in the clinical setting. In a study of 412 older adults in an urban medical center in China, 42% of women reported experiencing elder mistreatment (Dong et al., 2007). Yet the comparison may be biased by the inclusion of a larger proportion of frail and dependent older women in the clinical setting.
Education appears to be significantly and positively correlated with any elder mistreatment in older women in the present study. Our finding is at variance with previous studies that suggest elder mistreatment is more prevalent among older adults with lower educational levels (Dong & Simon, 2013c; Oh, Kim, Martins, & Kim, 2006). This discrepancy may be due in part to the large proportion of immigrant older women in our cohort. Regardless of educational levels, U.S. Chinese older women are confronted with significant language and cultural barriers resulting from immigration. Hence, the traditional notion that higher levels of education may be a protective factor for elder mistreatment may not be true in minority older women. An alternative explanation may be that older women with higher education levels are more likely to identify and acknowledge the elder mistreatment experience. In addition, older women with higher education levels may possess more financial assets that place them at a higher risk of elder mistreatment.
In the study, number of children was negatively correlated with any elder mistreatment. In particular, the group of older women with only one child had the highest prevalence of elder mistreatment. Older women with only one child tend to rely on the adult child as their sole source of social support. The absence of sibling support may aggregate caregiving stress and increase the likelihood of caregivers directing abusive behaviors at their elders. Our finding on the association of the number of children with elder mistreatment should be given considerable attention, given that the number of older women with one child constitutes a growing population of Chinese older women in the United States. Recently, in response to the growing elder mistreatment—especially elder neglect—resulting from the One-Child policy and social-economic changes, China passed an “Elderly Rights Law” that allows older adults to sue their children for neglect. We suspect that the One-Child policy may also influence the caregiving pattern and the well-being of older women in U.S. Chinese families. Given that type and level of contact between the elders and children were not collected, the relationships between the elders and the number of children should be cautiously interpreted.
In our study, elder mistreatment was more commonly reported in older women who were divorced or separated. This finding may contradict prior studies that found that married older adults were more likely to be mistreated (Pillemer & Finkelhor, 1988; Podnieks, Pillemer, Phillip, Shillington, & Frizzel, 1990). Due to the absence of data on the duration and frequency of elder mistreatment, we are unclear whether the mistreatment occurred before or after a woman left a marital relationship. Understanding the association between marital status and elder mistreatment could have important implications on interventions to prevent violence against women. Often battered women are encouraged to leave the abusive relationship. However, leaving the perpetrator may not guarantee the safety of victims. The high prevalence of elder mistreatment in divorced or separated women may indicate the possibility that elder mistreatment may occur or continue after older women leave abusive relationships. Safety planning in terms of when and where to leave is of significance for elder mistreatment interventions (Brandl & Raymond, 1997). This study sets the groundwork for future studies to explore the relationship between marital status and elder mistreatment.
Interestingly, this study reveals that the prevalence of elder mistreatment differed by language preference, with older women who spoke English or Mandarin having a higher prevalence of elder mistreatment than older women who spoke Cantonese or Toishanese. The Chinese population is inherently diverse, which manifests largely in its linguistic plurality. The motivation of immigration as well as the social and economic characteristics among U.S. Chinese older women vary substantially by language preference. The majority of Cantonese- or Toishanese-speaking older women entered the United States to join family members. They tend to live in the Chinatown area and are more likely to be surrounded by family members and relatives. Since the 1990s, with a growing number of Mandarin-speaking populations studying or working abroad, the number of older adults speaking Mandarin has increased in the United States. Compared with the Cantonese- or Toishanese-speaking older women, older women speaking Mandarin or English are more likely to live in suburban areas, where very few culturally appropriate services are provided. Consequently, English- or Mandarin-speaking Chinese older women may suffer from a relatively high level of social isolation, which may be associated with elder mistreatment. This finding highlights the importance of research and investigations targeting Chinese older women to take language preference into consideration.
This study demonstrates that health status may be an important indicator for elder mistreatment. The association between elder mistreatment and health status in older women has been elucidated by a wide range of prior studies. In a study of 1,245 women aged 50-79 years old, exposure to mistreatment had greater effects on mental health than other chronic medical conditions such as hip impairment or visual impairment (Mouton, 2003). Yet, there may be possible inverse associations between elder mistreatment and health status, such that poor health status may increase rates of elder mistreatment. In both cross-sectional and longitudinal studies, lower physical and cognitive function and the decline of physical and cognitive function were associated with increased risk of elder mistreatment (Dong & Simon, 2010; Dong, Simon, Beck, & Evans, 2013; Dong, Simon, & Evans, 2012; Dong, Simon, Rajan, & Evans, 2011). Future studies should clarify the interplay between health status and elder mistreatment in older women.
The present study should be interpreted with limitations. First, this study did not explore the prevalence of subtypes of elder mistreatments in older women. Prior studies suggest that older women are particularly susceptible to psychological and sexual mistreatment (Laumann et al., 2008; Teaster & Roberto, 2004). In addition, financial exploitation may have more devastating effects on older women due to the higher possibility of experiencing financial hardship in older women. Future studies should improve the understanding of subtypes of elder mistreatment in Chinese older women. Second, this study did not explore the frequency, duration, and severity of elder mistreatment. In addition, given that perpetrator characteristics may be associated with elder mistreatment, a dyadic approach should be applied in future studies to better examine the experience of elder mistreatment in U.S. Chinese older women. Furthermore, risk factors such as depression and previous victimization may be important in explaining elder mistreatment in older women. Therefore, future research should conduct a more comprehensive analysis that includes these important risk factors. Last but not least, this is a cross-sectional study, so we could not postulate on potential temporal associations. Longitudinal studies should be conducted to explore the risk factors and outcomes associated with elder mistreatment in U.S. Chinese older women.
This study has important research, practice, and policy implications. First, the prevalence of elder mistreatment in Chinese older women indicates the need for researchers to improve understanding of gender-based mistreatment in minority older adults. Particular attention should be given to develop culturally competent and gender-sensitive instruments for detecting elder mistreatment in minority older women (Fulmer, Guadagno, & Connolly, 2004). In addition, considerable efforts should be placed on how to translate the research findings into interventions. Second, physicians should acknowledge cultural and gender norms associated with elder mistreatment in Chinese older adults and pay special attention to detecting elder mistreatment in older Chinese women. Third, community organizations should increase efforts on improving knowledge pertaining to elder mistreatment in older women. Gender-based interventions such as women’s counseling groups should be designed to provide support and empowerment to the victims. Last but not least, the Violence Against Women Reauthorization Act should continue efforts to address elder mistreatment in minority older women.
Conclusion
This study demonstrates that elder mistreatment was prevalent in U.S. Chinese older women. The prevalence of elder mistreatment differed by socio-demographic and family composition characteristics. In addition, elder mistreatment was positively correlated with a higher level of education, lower health status, and worsening health changes over the past year, while negatively correlated with number of children and number of grandchildren. This study emphasizes the need to improve knowledge on elder mistreatment and design tailored interventions on elder mistreatment in minority women.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Institute on Aging grants (R01 AG042318, R01 MD006173, R01 CA163830, R34MH100443, R34MH100393, P20CA165588, R24MD001650, and RC4 AG039085), Paul B. Beeson Award in Aging, the Starr Foundation, American Federation for Aging Research, John A. Hartford Foundation, and the Atlantic Philanthropies.