
Abstract
The prevalence of domestic violence and abortion in India is high, yet little is known about the relationship between these experiences. Data from two linked data sets, India’s 1998-1999 National Family Health Survey (NFHS-2) and a follow-up survey in 2002-2003, were analyzed. The analysis examines how the experience of physical violence affects the subsequent uptake of abortion, and how the experience of abortion affects subsequent experience of physical, sexual, and verbal violence. Women who experienced physical violence have significantly higher odds of reporting a subsequent induced abortion, whereas women who had an induced abortion have significantly higher odds of reporting subsequent sexual and verbal violence. There was no significant relationship between domestic violence and spontaneous abortion.
Introduction
Male to female domestic violence is increasingly being recognized as an important public health problem, with significant consequences on women’s mental, physical, sexual, and reproductive health (Chandra, Satyanarayana, & Carey, 2009; Garcia-Moreno, Jansen, Ellsberg, Heise, & Watts, 2006; Gazmararian et al., 2000). The World Health Organization (WHO) reported that domestic violence is the most common form of violence in women’s lives, and estimates revealed that the lifetime prevalence of partner violence ranged from 13-61%, with most countries surveyed falling between 23% and 49% (Garcia-Moreno et al., 2006). A plethora of evidence suggests that high levels of reported male to female domestic violence exist in South Asia, specifically in India due to the existence of social institutions that often legitimize spousal abuse (Jejeebhoy, 1998; Jeyaseelan et al., 2007; Kaur & Garg, 2010). The most recent estimates for the national prevalence of domestic violence are obtained from the National Family Health Survey (NFHS-3) conducted in 2005-2006. The survey placed national domestic violence prevalence (physical, sexual, and verbal) at 37%, with regional estimates ranging from 59% in North India to 31% in Western India (International Institute for Population Sciences [IIPS] & Macro, 2009). Women who report domestic violence experience a range of negative reproductive health outcomes (reproductive tract infections, irritable bowel syndrome, unplanned pregnancies, lack of contraceptive use) and pregnancy health outcomes (high levels of anemia, low birth weight babies, pre-term delivery, and neonatal death; Ackerson & Subramanian, 2008; Martin et al., 1999; Ntaganira et al., 2008; Salam, Alim, & Noguchi, 2006; Sarkar, 2008; Stephenson, Koenig, & Ahmed, 2006; Wilson-Williams, Stephenson, Juvekar, & Andes, 2008).
There is also a demonstrated link between domestic violence and abortion in developed country settings (Glander, Moore, Michielutte, & Parsons, 1998; Goodwin, Gazmararian, Johnson, Gilbert, & Saltzman, 2000; Leung, Leung, Chan, & Ho, 2002; Wiebe & Janssen, 2001). However, the majority of studies were cross-sectional or unable to determine causality, and utilized clinic-based samples in developed country settings. This article examines the association between domestic violence and abortion, and fills a gap in the literature for three distinct reasons: It utilizes longitudinal data to determine links; it utilizes a population-based sample; and it is set in a resource-poor setting, rural India. In the current analysis, we use population-based data to examine the link between physical, sexual, and verbal domestic violence and abortion (spontaneous or induced) in four Indian states (Bihar, Jharkhand, Maharashtra, and Tamil Nadu) among married rural women of reproductive age (age 15-49). Specifically, the study explores the direction of causality between domestic violence and abortion by looking at two research questions:
The results demonstrate the need for the integration of domestic violence screening into abortion services in India.
Background
The United Nations estimated that the abortion rate in India is 3.1 abortions per 1,000 women (United Nations, 2007). Two types of abortions were considered in this study: spontaneous abortion (miscarriage) and induced abortion. The causal pathways linking domestic violence with these two types of abortions are highly correlated, although some differences do apply. Spontaneous abortion is a naturally occurring or a spontaneous loss of the fetus prior to 20 weeks gestation, and may be caused by infection, hormonal problems, or problems with the mother’s reproductive organs or immune response. On the other hand, induced abortion is a non-naturally occurring loss of the fetus performed by the woman or another actor, and terminated by a variety of different methods. In India, the Medical Termination of Pregnancy Act of 1971 made induced abortion legal when performed by a legally registered physician with specialized training under a wide range of circumstances (Patel, Bennett, Halpern, Johnston, & Suchindran, 2009). These circumstances include saving the life of the woman, preserving mental and physical health, in cases of rape or incest, contraceptive failure, and for economic or social reasons (Hirve, 2004). Despite the liberal abortion law that has existed in India for over three decades, access and quality of services is low in most parts of the country, especially in rural areas (Hirve, 2004). The quality of abortion services in public hospitals, as well as private clinics, is compromised due to poor technique, counseling, and patient confidentiality (Hirve, 2004). In addition, stigma regarding abortion, general lack of knowledge about reproductive health, and limited access to abortion services often result in women seeking and obtaining criminal abortions. Criminal abortions range from somewhat safe abortions conducted by medical doctors who simply are not certified to perform abortions to fatally unsafe abortions conducted using foreign objects and traditional methods (Mathai, 1997). It is estimated that in India between 9% and 20% of maternal deaths are related to unsafe induced abortions (Patel et al., 2009).
The association between domestic violence and induced abortion has received much attention in developed settings. Although abortion may be a direct consequence of physical trauma due to physical assault or an indirect consequence of stress in abusive relationships, women with unplanned or unintended pregnancies who are in abusive relationships have been found to have a higher uptake of induced abortion (Wiebe & Janssen, 2001). A study in Hong Kong found that the lifetime prevalence of domestic violence among patients seeking abortion was 27.3%, with 13.5% having a recent history of physical abuse (Leung et al., 2002). A study in North Carolina found that 7.8% of women interviewed during pre-abortion screening were victims of emotional or physical violence during their current pregnancy (Wiebe & Janssen, 2001). The authors suggested that termination of pregnancy might be related to relationship abuse and subsequent unintended pregnancy through partner’s control of contraception, as well as women’s fears that a child born through an abusive relationship would be a victim of subsequent parental violence (Wiebe & Janssen, 2001). One study found that relationship issues were the predominant reasons for pregnancy termination given by women with a history of domestic violence, and abused women were also significantly less likely to inform their partner of pregnancy or to have partner support for or involvement in the abortion decision (Glander et al., 1998). As part of the Pregnancy Risk Assessment Monitoring System (PRAMS) population surveillance project, women were asked about exposure to physical violence and pregnancy intent. It was found that women with unwanted or mistimed pregnancies reported higher rates of physical violence than women with intended pregnancies. The odds of experiencing physical violence were 4.1 times higher among women with unintended pregnancies (Goodwin et al., 2000). Therefore, mistimed or unwanted pregnancies as related to physical violence help to explain the causal pathway between violence and induced abortion. A limited number of studies in developing countries also found associations between domestic violence and induced abortion. For example, in Uganda where abortion is illegal, domestic violence was found to be a risk factor for unwanted pregnancy and induced abortions among women seeking post-abortion care (D. K. Kaye, Mirembe, Bantebya, Johansson, & Ekstrom, 2006). Another study from Uganda found that 38.9% of women interviewed stated domestic-violence-related issues as the main reason for inducing abortion (D. Kaye, 2001).
There is also limited research from developing areas regarding the link between spontaneous abortions and domestic violence. A cross-sectional study in Bangladesh found a higher odds of unwanted pregnancy (odds ratio [OR] = 1.46) and miscarriage (OR = 1.81) among physically abused women (Silverman, Gupta, Decker, Kapur, & Raj, 2007). A study in Cameroon found that women who were exposed to physical and sexual spousal violence were more likely to experience spontaneous fetal loss (Alio, Nana, & Salihu, 2009). The authors explained the causal pathway by stating that the experience of sexual violence affects a woman’s psychological well-being. This in turn results in withdrawal from public life and seeking prenatal care, which leads to negative birth outcomes (Alio et al., 2009). Pathways to explain domestic violence and spontaneous abortion in the South Asian setting include poorer general health found among abused women, poor nutrition as a potential aspect of abuse, poor or delayed antenatal care received by abused women, and injuries during pregnancy that directly or indirectly compromise fetal health (Silverman et al., 2007). It is also possible that the inability of a woman to have a child to term could result in domestic violence (Jejeebhoy, 1998; Silverman et al., 2007; Wilson-Williams et al., 2008); however, the cross-sectional analyses of most studies were unable to determine whether the abuse caused spontaneous abortion, or if the loss of the child resulted in abuse. A qualitative study in India found that a large proportion of women who experienced fetal loss associated the miscarriage or stillbirth with a violent assault inflicted upon them by their husbands (Jejeebhoy, 1998).
As discussed above, India exhibits significant levels of domestic violence against women. In addition, domestic violence has been shown to be associated with both spontaneous and induced abortions. However, the majority of data are obtained from clinic-based samples in developed regions using cross-sectional analyses. This study seeks to build upon the minimal work of domestic violence and abortion in India by exploring causality between domestic violence and abortion among rural Indian women from four states: Bihar, Jharkhand, Maharashtra, and Tamil Nadu.
Data and Methods
Study Setting
This article analyzed data from four economically and culturally distinct states of India, namely Bihar and Jharkhand in the North, Maharashtra in the West, and Tamil Nadu in the South. These four states represent India as a whole in this analysis, because they vary widely across a range of indicators related to socioeconomic and women’s status, age at marriage, literacy, and parity. In addition, prevalence of domestic violence varies among the four states of interest. Bihar has the highest prevalence at 59%, whereas Maharashtra has the lowest prevalence at 31%. Jharkhand and Tamil Nadu also have relatively high domestic violence prevalence, at 37% and 42%, respectively (IIPS, 2009).
Data
This longitudinal study used two linked data sets (NFHS-2 and NFHS-2 follow-up survey). The NFHS-2, the Indian equivalent of the Demographic and Health Survey, was India’s second national survey carried out in 1998-1999. The NFHS-2 sample covered 99% of India’s population residing in its 26 states and included three questionnaires, including a woman’s questionnaire that collected information concerning the following: sociodemographic characteristics; fertility behavior and intentions; use, knowledge, and quality of family planning methods; abortion history and type of abortion; maternal and child health care; reproductive health; and domestic violence (IIPS & Macro, 2000). Overall response rates for sampled women were high (96%) and ranged from 94-100% in the states included in the present study (IIPS & Macro, 2000). Following completion of the NFHS-2 survey, a prospective follow-up study of original NFHS-2 respondents was conducted by the IIPS, India, and the Johns Hopkins Bloomberg School of Public Health. The sampling frame for the NFHS-2 follow-up survey, conducted in 2002-2003, consisted of all rural respondents interviewed in the original 1998-1999 study in four Indian states: Bihar and Jharkhand (which had been part of Bihar at the time of the NFHS-2 survey) in the North, Maharashtra in the West, and Tamil Nadu in the South. Therefore, the two data sets were linked based on the individual respondents, of rural women from the four aforementioned states. High rates of reinterview were achieved in all four states, ranging from 76% in Maharashtra to 94% in Tamil Nadu. The reinterviewed and non-reinterviewed samples of women were generally similar in characteristics, indicating no significant selectivity in our reinterviewed sample (IIPS & Macro, 2000).
The final sample was restricted to currently married women at the time of the 1998-1999 NFHS-2 interviews, because these are the women at risk of domestic violence by their husband. Respondents who reported being sterilized at the time of baseline survey were excluded from analysis as they could not be pregnant and thus at risk of an abortion in the inter-survey period. By limiting the sample to only those women who were not sterilized, the sample will be younger and possibly less likely to experience domestic violence. In India, female sterilization is known to be synonymous with contraception and is generally used to limit the number of children; therefore, older rather than younger women are sterilized. In addition, sterilization has been shown to be associated with experience of violence (Rao, 1997; Stephenson, Koenig, Acharya, & Roy, 2008; Stephenson et al., 2006). However, to look at the link between domestic violence and abortion, the sample needed to be limited to only those women actually at risk of abortion or non-sterilized women. The final sample size is thus 4,025 rural women age 15-39 at baseline (NFHS-2 survey), and age 18-44 at follow-up (follow-up survey).
Both the NFHS-2 and the follow-up surveys included questions on domestic violence. The NFHS-2 measures only physical domestic violence; specifically, respondents were asked if they had been physically beaten in the 12 months prior to the survey. The follow-up survey included a more detailed battery of questions on violence than were included in the NFHS-2, and collected data on physical, sexual, and verbal violence. To assess physical intimate partner violence (IPV), respondents were asked whether their husband had ever pushed, pulled, or held them down; hit with fist; kicked or dragged; tried to strangle; or attacked them with a knife or weapon. Sexual IPV was assessed by asking the respondents if their husband had used physical force to have sex with them. And verbal IPV was assessed by asking if their husband had verbally abused them, defined as verbal insults. For each type of IPV (physical, verbal, sexual), the respondents were asked if they had experienced that type of IPV in the past 12 months.
The follow-up survey included multiple questions on abortion. Specifically, respondents were asked if they had had an abortion in the inter-survey period (between the NFHS-2 and the follow-up survey), the specific timing of the abortion (in months and years), and the type of abortion (spontaneous or induced).
Data Analysis
Two analyses were conducted to (a) assess if physical domestic violence led to increased odds of experiencing an abortion (spontaneous or induced) and (b) assess if the experience of an abortion (spontaneous or induced) led to an increased odds of experiencing physical, sexual, or verbal domestic violence. Data were analyzed using STATA 10.0.
The first analysis fits a multinomial regression model to a categorical abortion outcome; the main exposure variable was reported physical violence. To ensure the correct temporal ordering of events, the measure of physical domestic violence was taken from the baseline NFHS-2 survey, and the measure of abortion was taken from the follow-up survey. The categorical abortion outcome was defined as not having an abortion, having an induced abortion, or having a spontaneous abortion in the inter-survey period (anytime between baseline NFHS-2 survey and the follow-up survey). The main exposure, physical domestic violence in the past 12 months prior to baseline, was measured as a dichotomous variable, no = 0 and yes = 1.
The second analysis considered three separate binary outcomes: reporting of recent physical, sexual, or verbal violence in the 12 months prior to the follow-up survey. Separate logistic models are fitted to each outcome. The main exposure for each model was the report of an abortion during the inter-survey period but at least 12 months prior to the follow-up survey. The measure of abortion for this analysis is also taken from the follow-up; however, the follow-up also recorded the timing of the abortion (in months and years). Thus, for this analysis, abortions are restricted to those that occurred in the inter-survey period, but more than 12 months prior to the follow-up survey, and the measures of violence are those in the last 12 months. This ensures that the recorded abortion occurred before the recorded violence. The three outcomes of domestic violence were measured as dichotomous variables: experience of physical violence in the 12 months prior to the follow-up survey (0 = no, 1 = yes), experience of sexual violence in the 12 months prior to the follow-up survey (0 = no, 1 = yes), and experience of verbal violence in the 12 months prior to the follow-up survey (0 = no, 1 = yes). Abortion was measured as a categorical variable: defined as not having an abortion between the baseline NFHS-2 survey and 12 months prior to the follow-up survey, having an induced abortion between the baseline NFHS-2 survey and 12 months prior to the follow-up survey, or having a spontaneous abortion between the baseline NFHS-2 survey and 12 months prior to the follow-up survey.
All models controlled for age and education level (of both respondent and partner), respondents’ age at marriage, spousal age difference, parity, ever use of contraceptives, standard of living index, and justification of beating scale. In addition, the second analysis also controlled for baseline experience of physical violence. Scales were created to measure the respondent’s standard of living and attitudes toward justification of wife beating. The standard of living index was measured as low, medium, or high according to the respondent’s answers regarding living in a home with electricity, toilet facility, a refrigerator, source of drinking water, and ownership of car, motorcycle, radio, or television. Justification of wife beating is measured on a scale from 0-6—low to high—according to the respondents justifying beating if the wife is unfaithful, if her family does not provide money at marriage, shows disrespect to her husband, goes out without telling her husband, neglects the house or children, or does not cook properly.
Results
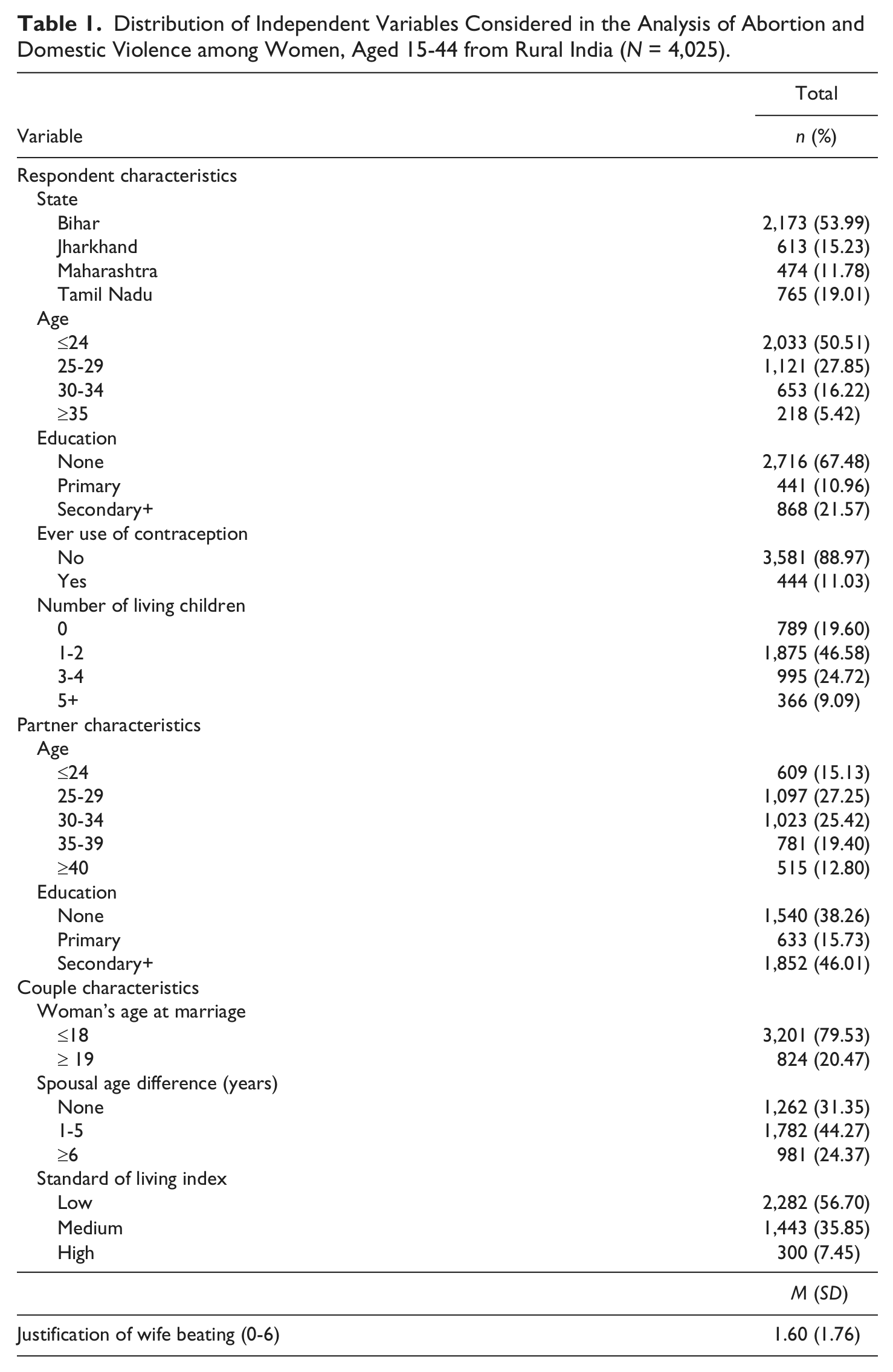
Table 1 displays the independent variables considered in the analyses. The largest proportion of respondents lived in Bihar (53.99%) and the fewest in Maharashtra (11.78%). Fifty percent of the respondents were less than 25 years old, and 67.48% of the respondents reported no education (rather than primary or secondary education). The large majority of respondents had never used any form of contraceptives (88.97%), and in relation had at least one child (80.40%). Respondents’ husbands were more educated and older than their wives. Less than 40% of husbands had no education and 46.01% had at least a secondary education. Partners’ age was fairly evenly distributed with 15.13% below age 25, 25.42% aged 30-34, and 12.80% above age 40. In turn, the majority of women were in a marriage with an age difference of at least one year (68.65%). Almost 80% of respondents were married before age 19. In addition, 56.70% of the couples had a low standard of living index, 35.85% a medium standard of living index, and 7.45% a high standard of living index. The mean of the Justification of Wife-Beating scale was low at 1.60, ranging from 0-6.
Distribution of Independent Variables Considered in the Analysis of Abortion and Domestic Violence among Women, Aged 15-44 from Rural India (N = 4,025).
According to the baseline survey, 29.02% of the respondents reported experiencing physical violence (Figure 1). In the follow-up survey, a smaller percentage, or 20.99%, of the respondents reported experiencing physical violence. Verbal domestic violence was the most frequently reported, where 34.43% of the respondents reported verbal violence in the follow-up survey. Sexual domestic violence is the least reported by the respondents in the follow-up survey (11.68%). These proportions are particular to our sample of women who were not sterilized at baseline and cannot be generalized to the whole of India. Questions regarding abortion in the inter-survey period were asked by specific type of abortion, and 5.09% of women reported a spontaneous abortion, whereas 3.28% reported an induced abortion. In addition, 4.77% of the respondents reported a spontaneous abortion and 3.11% of the respondents reported an induced abortion in the inter-survey period but at least 12 months prior to the follow-up survey.

Domestic violence and abortion patterns from baseline and follow-up survey among women, aged 15-44 from rural India (N = 4,025).
Women who reported physical violence in the 12 months prior to the baseline survey were significantly more likely to report an induced abortion (Relative Risk Ratio [RRR] = 2.13, confidence interval [CI] = [1.06, 4.24]) (Table 2). Women aged 25-29 were less likely to have an induced abortion, compared with women less than 25 years old (RRR = 0.44, CI = [0.24, 0.81]), whereas women who had a partner aged 25-29, compared with women below age 25, were more likely to report an induced abortion (RRR = 2.51, CI = [1.08, 5.85]). While women’s education was not found to be statistically significant, a partner’s educational level of secondary+ was associated with a lower likelihood of an induced abortion (RRR = 1.54, CI = [1.21, 3.41]). Women with at least one child were more likely to report having an induced abortion; in fact, the likelihood of having an induced abortion increases as parity increases (parity 1-2 RRR = 1.98, CI = [1.04, 3.78]; parity 3-4 RRR = 3.62, CI = [1.66, 7.91]; parity 5+ RRR = 6.07, CI = [2.37, 15.51]). A woman’s justification of physical abuse lowered the likelihood of having an induced abortion (RRR = 0.88, [CI = 0.79, 0.99]).
Multinomial Regression for Abortion Among Women Aged 15-44 in Rural India (N = 4,025).
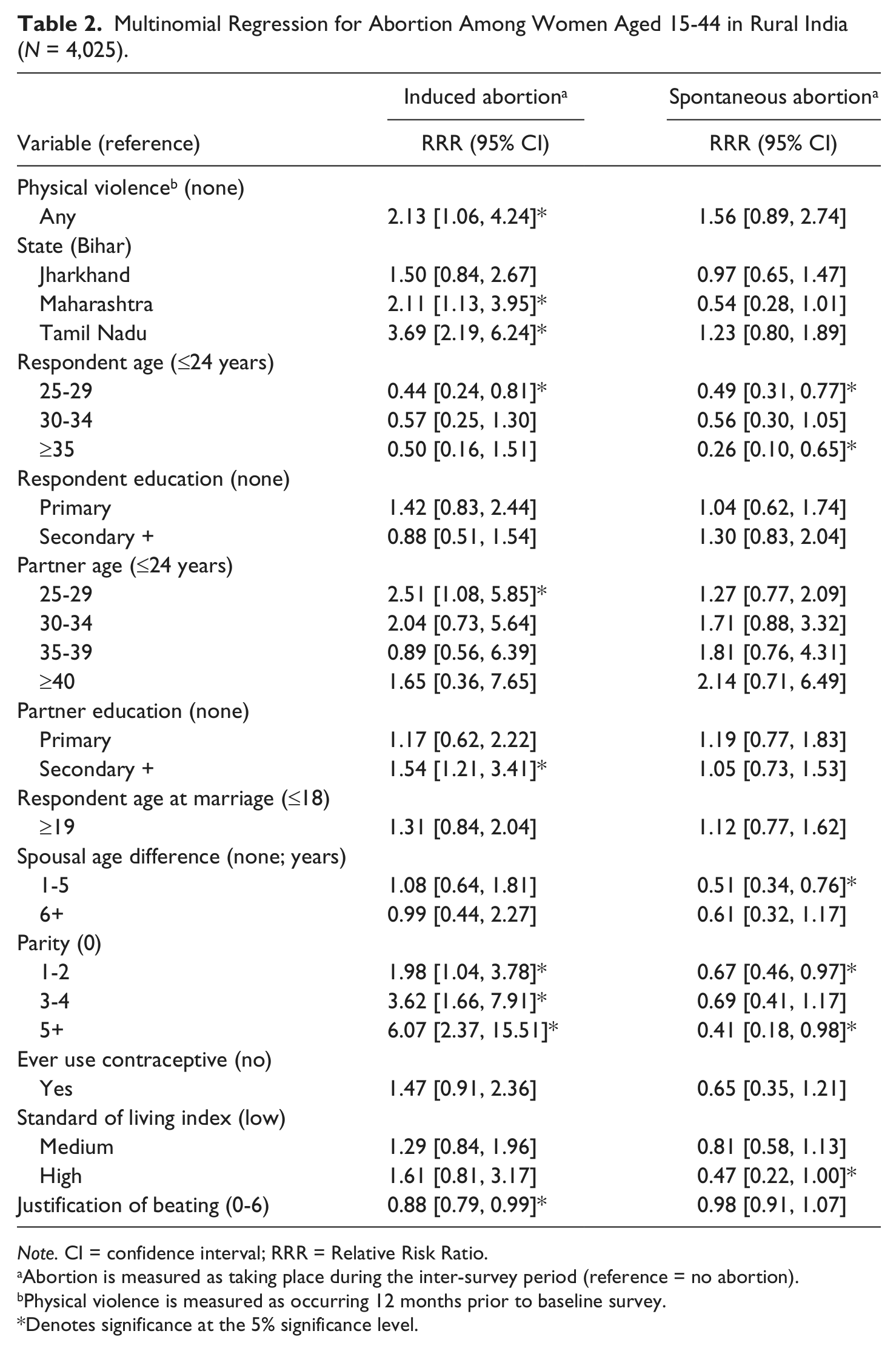
Note. CI = confidence interval; RRR = Relative Risk Ratio.
Abortion is measured as taking place during the inter-survey period (reference = no abortion).
Physical violence is measured as occurring 12 months prior to baseline survey.
Denotes significance at the 5% significance level.
There was no statistically significant relationship between physical abuse and spontaneous abortion among women in our sample. However, compared with women below age 25, women aged 25-29 (RRR = 0.49, CI = [0.31, 0.77]) and women aged at least 35 (RRR = 0.26, CI = [0.10, 0.65]) had a significantly lower likelihood of spontaneous abortion. Women with a spousal age difference between 1 and 5 years were less likely to have a spontaneous abortion (RRR = 0.51, CI = [0.34, 0.76]) than women with no spousal age difference. In contrast to the induced abortion finding, women who had at least one child were significantly less likely to report a spontaneous abortion (parity 1-2 RRR = 0.67, CI = [0.46, 0.97]; parity 5+ RRR = 0.41, CI = [0.18, 0.98]). Women with a high standard of living index were less likely to have a spontaneous abortion than women with a low standard of living index (RRR = 0.47, CI = [0.22, 1.00]).
The results of the logistic regression models revealed that women who had an induced abortion were more likely to face subsequent sexual (OR = 2.17, CI = [1.34, 3.51]) and verbal (OR = 1.54, CI = [1.04, 2.29]) violence from their husbands after controlling for background characteristics (Table 3). It is important to note that the three models were analyzed with and without the variable, experience of physical violence and baseline, and there was no meaningful change in significance or affect size in the relationship between induced abortion and each violence outcome. Specifically, the link between induced abortion and physical violence was non-significant before the variable physical violence at baseline was added. Therefore, experience of violence at baseline by itself does not explain violence at follow-up. There was no significant relationship found between women who experienced induced abortion and physical violence.
Logistic Regression Models for Experience of Physical, Sexual, and Verbal Domestic Violence Among Women Aged 18-44 in Rural India (N = 4,025).
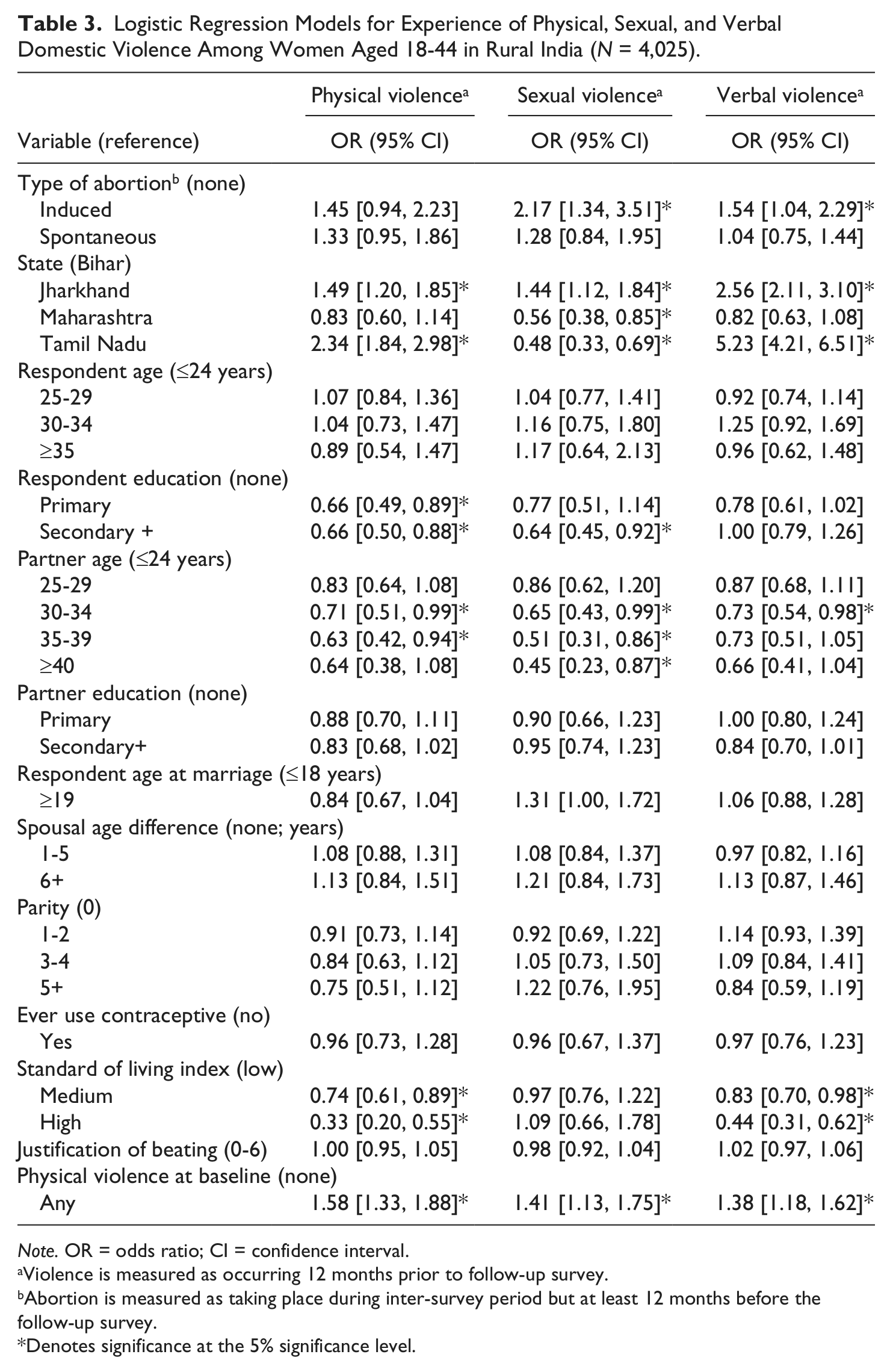
Note. OR = odds ratio; CI = confidence interval.
Violence is measured as occurring 12 months prior to follow-up survey.
Abortion is measured as taking place during inter-survey period but at least 12 months before the follow-up survey.
Denotes significance at the 5% significance level.
Relative to women in Bihar, women in Jharkhand were more likely to report physical (OR = 1.49, CI = [1.20, 1.85]), sexual (OR = 1.44, CI = [1.12, 1.84]), or verbal (OR = 2.56, CI = [2.11, 3.10]) violence. However, women in Tamil Nadu were less likely to report sexual violence (OR = 0.48, CI = [0.33, 0.69]) but more likely to report physical (OR = 2.34, CI = [1.84, 2.98]) or verbal (OR = 5.23, CI = [4.21, 6.51]) violence. Conversely, women in Maharashtra were less likely to report sexual violence (OR = 0.56, CI = [0.38, 0.85]). Respondents whose husbands were between the ages of 30 and 34 were less likely to face all forms of violence after an abortion compared with women with husbands less than 25 years old (physical OR = 0.71, CI = [0.51, 0.99]; sexual OR = 0.65, CI = [0.43, 0.99]; verbal OR = 0.73, CI = [0.54, 0.98]). Respondents’ education was also a significant factor; specifically, women with at least a secondary education were less likely to face physical or sexual violence post-abortion (physical OR = 0.66, CI = [0.50, 0.88]; sexual OR = 0.64, CI = [0.45, 0.92]). Women with a medium standard of living index were less likely to face physical (OR = 0.74, CI = [0.61, 0.89]) or verbal (OR = 0.83, CI = [0.70, 0.98]) violence after an abortion. Women with a high standard of living were less likely to face physical (OR = 0.33, CI = [0.20, 0.55]) or verbal (OR = 0.44, CI = [0.31, 0.62]) violence. Last, women who reported experiencing physical violence in the baseline survey were more likely to report physical, sexual, and verbal violence in the follow-up survey (physical OR = 1.58, CI = [1.33, 1.88]; sexual OR = 1.41, CI = [1.13, 1.75]; verbal OR = 1.38, CI = [1.18, 1.62]).
Discussion
This study fills a gap in the literature by exploring the direction of causality between domestic violence and abortion (spontaneous and induced) using a population-based sample in a resource-poor setting. The results found that there was no link between domestic violence and spontaneous abortion; however, the statistically significant displayed link between domestic violence and induced abortion was complex. The pathways between violence and induced abortion are multidirectional: Induced abortion leads to an increase in sexual and verbal violence, whereas physical violence leads to a woman seeking an abortion.
This study demonstrated a relationship between physical violence and induced abortion: Women exposed to spousal physical domestic violence have significantly higher odds of having an induced abortion. Studies in Hong Kong and the United States have shown similar relationships with physical violence and abortion, thus our finding is notable and a first in the Indian setting (Leung et al., 2002; Wiebe & Janssen, 2001). The results also demonstrate the effect of having an induced abortion on a woman’s risk of violence: Specifically, an increased odds of sexual and verbal violence. The causal pathways between abortion and subsequent violence require further investigation; it is possible that in a society with a high emphasis placed on fertility and childbearing that an abortion may lead to violence as it is seen as in opposition to a woman’s expected role. It is widely known that there is a preference for a male child in India; however, how this preference plays a role in the link between domestic violence and abortion is unknown (Das Gupta et al., 2003). A woman carrying a female child rather than a male may lead to a sex-selective abortion and subsequent violence; for example, Silverman showed that infant girl mortality was significantly greater among mothers who were experiencing violence but non-significant for infant boys. Also, it is possible that women who opt for an abortion live in households in which violence, or the threat of violence, is already present; the act of abortion may thus act as a trigger for violence. Thus, women who experienced physical violence were more likely to then go on and experience an induced abortion; and, women with a reported induced abortion were more likely to then go on and experience sexual and verbal violence. These effects exist after controlling for other known correlates of abortion (age, parity, education, age at marriage; Leung et al., 2002; Mishra, Ramanathan, & Rajan, 1998; Santhya & Verma, 2004; Wiebe & Janssen, 2001). Previous studies that examined the relationship between domestic violence and spontaneous abortion found significant associations, which were not found in our study.
Previous studies have also suggested that the higher rate of abortions among abused women may be an attempt to protect future children from abuse (Mishra et al., 1998). It is possible that for women who experience physical violence (rather than sexual or verbal violence), the threat of repeating this violence on their children is more plausible. Similarly, women who reported that being beaten was justifiable (for reasons such as being unfaithful, showing disrespect to the husband, going out without permission, and not cooking properly) were less likely to report having an induced abortion. Women who justify violence and are thus more tolerant of violence may be less concerned about the repetition of violence on future children.
Further research is needed to understand the circumstances in which exposure to violence leads to increased abortion, and how a woman’s decision to have an abortion makes her a victim of domestic violence. There needs to be better screening of domestic violence integrated into existing family planning services that include measures to screen women for different types of violence, including physical, sexual, and verbal violence. The results also demonstrate a need to increase contraceptive knowledge among women to prevent unwanted pregnancies among women who are facing domestic violence. One potential limitation to this study is that both domestic violence and abortion measures are self-reported by the women. However, previous studies have shown that domestic violence is culturally accepted in this setting, therefore the likelihood of underreporting may be low (Kaur & Garg, 2010). Measures of abortion are also self-reported; however, the questions asked separately regarding spontaneous and induced abortions do allow the differentiation of types of abortions. It is likely that misclassification bias existed, because lack of knowledge regarding the legal right to an induced abortion and stigma may have resulted in more reported spontaneous abortions than induced abortions. However, this would result in bias away from toward the null. The availability of in-depth data from two time points is a considerable advantage of this study, and has allowed the identification of relationships between abortion and domestic violence that are often overlooked in resource-poor settings.
Conclusion
This study contributes toward an understanding of the effect of domestic violence on a woman’s decision to undergo an induced abortion. It establishes temporal relationships between domestic violence and abortion, a first in an Indian setting. Domestic violence education and screening need to be incorporated into abortion services in rural India. Given that physical violence is significantly associated with higher odds of abortion, physicians and other health care providers need to be trained to recognize signs of physical or sexual violence in women. Integrating domestic violence screening at family planning clinics could be an important venue for education and assistance regarding spousal abuse, and providing referral services for abused women to abortion clinics if necessary. Rural India relies on networks of community health workers for primary health care as well as family planning; thus, community-based outreach programs to educate women who are victims or potential victims of violence would be beneficial in women noticing signs of violence and seeking help. Future research should explore the circumstances of domestic violence that leads to women seeking abortions in the Indian setting. This would further help inform national policy for domestic violence screening in different health care settings, as well as establishing abortion services for victims of abuse, and counseling on domestic violence for women who receive abortions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.