
Abstract
This investigation utilizes structural equation modeling (SEM) to build and test a comprehensive model of specific and global risk perception. A sample of 325 undergraduate females responded to measures of previous victimization, problematic alcohol use, and maladaptive coping. They also rated perceived risk in multiple hypothetical dating vignettes. The results revealed strong relationships between problematic alcohol use and both decreased specific and increased global risk perception. In addition, previous victimization and maladaptive coping were related to increased global risk perception and specific risk perception, respectively. These findings carry implications for theories of risk perception and point to new approaches for research.
Data from the U.S. Department of Justice indicate that in 2011, nearly 1.1 million women reported incidents of rape, sexual assault, or intimate partner violence (U.S. Department of Justice, Office of Justice Programs, Bureau of Justice Statistics, 2012). College-age females are among the most at-risk population. This may be due to limited experience with social interactions, dating, and alcohol consumption (Carmody, Ekhomu, & Payne, 2009; Koss, Gidycz, & Wisniewski, 1987). In one longitudinal study, Humphrey and White (2000) found that the periods of greatest vulnerability for sexual victimization occurred during adolescence (ages 14-18) and the first year of college. The authors found that 69.8% of their sample reported at least one instance of victimization by the end of college and concluded that individuals with multiple previous victimizations were at the greatest risk for subsequent assault. These findings have been replicated across several studies (Classen, Palesh, & Aggarwal, 2005; Fisher, Cullen, & Turner, 2000). Revictimization appears to be independent of the age of the initial assault, or whether females were assaulted in childhood (Milner et al., 2010), adolescence (Humphrey & White, 2000), or adulthood (Classen et al., 2005). One explanation for the relationship between previous sexual assault history and subsequent victimization is a decreased ability to perceive risky or dangerous situations.
Components of Risk Perception
One component of risk perception involves accurately perceiving threat cues in a given situation or interaction (sometimes referred to as specific risk perception). Following this logic, if a specific situation is accurately recognized as risky, the potential victim will take steps to avoid or escape the situation earlier, and the probability of assault will decrease. Risk perception is thus viewed as one protective factor against victimization. Therefore, deficits in risk perception do not imply responsibility to the victim. Alternatively, failing to perceive risk in a specific situation may substantially increase the likelihood for assault by delaying the avoidance or escape response (Messman-Moore & Brown, 2006).
Another component of risk perception involves evaluating broad social, economic, and environmental conditions that create an increased risk for assault for the individual and her peers (sometimes referred to as global risk perception). Evidence suggests that global risk perception is also compromised in women with a history of sexual assault (Messman-Moore & Brown, 2006; Naugle, 1999). Given their close association, it is likely that deficits in each of these components are related to an increased vulnerability for revictimization.
Norris, Nurius, and Graham (1999) investigated both specific and global risk perception simultaneously. The authors presented a sample of undergraduates with one of three dating scenarios (representing a first, fifth, or typical date) and collected risk ratings based on the women’s perceptions of threat in the scenario. They found that females with a history of sexual assault required a greater number of clear and unambiguous risk factors to feel guarded in risky situations. The authors noted, however, that general knowledge about risk factors did not translate into taking personal precautions. These data suggest that while females may be aware of the global factors that increase the chances of being sexually assaulted, they may not recognize the factors as personally relevant in certain contexts (Norris et al., 1999).
Other studies examining sexual assault risk perception have concluded that women with a history of sexual assault evidence a unique response to threat, including attenuated physiological (heart rate) responses (Soler-Baillo, Marx, & Sloan, 2005) and lagged performance during sexual assault prevention training (Yeater & O’Donohue, 2002). The variability of sexual assault risk perception in this population can be linked to a number of behavioral and psychological factors, which need to be examined in a comprehensive theoretical framework.
Alcohol Use and Risk Perception
One important behavioral factor in sexual assault risk perception is alcohol consumption. Sexual assault is more likely to be completed against females who are under the influence of alcohol compared with those who are not (Resnick et al., 2012; Ullman, 2003). It is estimated that at least half of all sexual assaults among young adult populations involve alcohol use by the victim, perpetrator, or both (Abbey, 2002; Abbey, Zawacki, Buck, Clinton, & McAuslan, 2004; Kilpatrick, Resnick, Ruggiero, Conoscenti, & McCauley, 2007; Mohler-Kuo, Dowdall, Koss, & Wechsler, 2004; Testa & Parks, 1996). Among females with a history of sexual assault, alcohol use has been linked to additional negative outcomes, including revictimization (Gidycz et al., 2007), posttraumatic stress disorder (PTSD; Messman-Moore, Ward, & Brown, 2009), and other substance abuse disorders (Kilpatrick, Acierno, Resnick, Saunders, & Best, 1997; Ullman & Najdowski, 2009).
Alcohol use is sometimes tied to coping behavior because of its functional role in avoiding unpleasant internal and external stimuli (Resnick et al., 2012). The tendency toward alcohol and other substance use is often conceptualized as a negative feedback loop resulting in greater use of the substance to dull unwanted emotional and cognitive experiences. However, the physiological effects of alcohol use (e.g., impaired judgment, slowed motor responses) also strongly contribute to deficits in perceiving and responding to environmental threats. Consequently, problematic alcohol use and frequent intoxication lead to revictimization (Ullman, Filipas, Townsend, & Starzynski, 2005; Ullman & Najdowski, 2009). Indeed, women who evidence a pattern of binge drinking (i.e., consuming four or more alcoholic beverages in one sitting, typically within a 2-hr period; National Institute on Alcohol Abuse and Alcoholism [NIAAA], 2013) are less likely to perceive sexual assault risks when intoxicated (Davis, Stoner, Norris, George, & Masters, 2009). Increased intoxication has also been associated with limited recognition of ambiguous risk cues (Testa, VanZile-Tamsen, Livingston, & Buddie, 2006). Thus, problematic alcohol use should independently predict deficits in risk perception.
Coping Style and Risk Perception
Coping style is a complex psychological construct that may contribute to deficits in risk perception (Nurius, Norris, Young, Graham, & Gaylord, 2000). In general, coping refers to a series of cognitive and behavioral strategies used to manage perceived stressors in the environment (Folkman & Moskowitz, 2004). The use of adaptive strategies, such as relying on social support, appears to protect against negative outcomes following assault (Bryant-Davis, Ullman, Tsong, & Gobin, 2011). In contrast, maladaptive strategies (e.g., denial, self-distraction, self-blame, and behavioral disengagement) strengthen the numbing or avoidant responses, potentially decreasing risk perception and thereby increasing vulnerability for future assault. Recently, Najdowski and Ullman (2011) identified a large sample of females who experienced previous sexual assault. Individuals who were revictimized used more maladaptive strategies than those who were not. Maladaptive coping can also prevent recovery following sexual assault (Najdowski & Ullman, 2009).
The trauma response may help explain these findings. Extreme trauma may lead to numbing or dissociative reactions, which prevent accurate appraisal of threat cues (Chu, 1992; Cloitre, Scaralone, & Difede, 1997). Indeed, evidence from several studies indicates that females with more severe histories of sexual assault are less able to identify threat (Meadows, Jaycox, Stafford, Hembree, & Foa, 1995) and take longer to detect danger during exposure to threat cues (Wilson, Calhoun, & Bernat, 1999). Similar impairments in risk perception have been observed in other well-controlled studies (e.g., Messman-Moore & Brown, 2006).
Modeling Sexual Assault Risk Perception
Despite the findings outlined above, a consistent relationship between sexual assault history and impaired risk perception has not been found (for a thorough review, see Gidycz, McNamara, & Edwards, 2006). For example, Hickman and Muehlenhard (1997) found that among college women, a personal history of rape did not affect women’s ratings of future risk. Similarly, VanZile-Tamsen, Testa, and Livingston (2005) concluded that among a large sample of community females, previous victimization status did not affect risk perception in situations involving acquaintance assault. There are a number of possible explanations for these mixed results. Many studies have only focused on specific pathways leading to revictimization, but the complex relationships among these variables have not been examined simultaneously in context. Moreover, risk perception is seldom explored in terms of specific and global risk perception, thereby limiting the conclusions that may be drawn. In consideration of these issues, a more sophisticated approach to modeling the mechanisms behind risk perception is warranted.
Several structural approaches, such as path modeling, confirmatory factor analysis (CFA), and structural equation modeling (SEM), have become more widely utilized in recent years due to their utility in explaining complex relationships among variables simultaneously, and the ease with which these explanations may be compared with one another. Leaders in the field of female sexual assault research have called for a greater use of these approaches (Macy, 2008; Nurius & Norris, 1996; VanZile-Tamsen et al., 2005).
The present study adds to the literature by providing a comprehensive theoretical picture of how behavioral and psychological factors relate to a female’s risk perception. The first series of analyses presented here demonstrates the use of a standardized vignette approach that yields ratings of risk, which increase parametrically with the number of empirically derived risk factors included at each level. The second series of analyses uses a model-building approach to fit an a priori structural model to the observed data in an effort to clarify how previous victimization, problematic alcohol use, and maladaptive coping influence specific and global risk perception.
Method
Participants
Our sample included 325 undergraduate females at a large southeastern public university who were identified as heterosexual. The age range of this sample was 18-46 years (M = 21.26, SD = 4.56); a majority of the sample identified themselves as Caucasian (65.2%), with smaller proportions identified as Hispanic (16.0%), Black (8.9%), multiracial (4.3%), Asian/Pacific Islander (3.4%), and undisclosed (2.2%). The sample was mostly single (57.8%), though a large proportion reported being in a committed relationship (33.3%). The remaining participants reported being either married (7.1%) or divorced/separated (1.8%).
Measures
In addition to a demographic questionnaire, participants also completed a battery of self-report inventories.
MacLeod Assessment of Risk Knowledge (MARK)
The MARK is comprised of six written vignettes depicting three levels of sexual assault risk (i.e., low, moderate, and high). Each vignette describes a hypothetical dating scenario in which both individual and environmental factors contribute to an increased risk of sexual assault. There are two vignettes at each risk level. They were created to accurately describe typical dating scenarios using individual and contextual factors that have been empirically associated with a higher risk of sexual assault (Cue, George, & Norris, 1996; Norris et al., 1999). The individual factors include perpetrator characteristics (e.g., belief in male sexual entitlement), while the contextual factors include situational variables (e.g., man paying for a date). A total of eight discrete variables were selected and inserted into the vignettes, such that each risk level contained a parametrically increased danger for the reader. The individual and contextual factors were added to the vignettes using direct and comprehensible language to offer realistic depictions of the factors. We chose to focus on heterosexual dating scenarios with familiar partners specifically, given the frequency of victimization that occurs within this context, rather than assault by a stranger (Black et al., 2011). Vignettes were written in the first-person perspective and were comparable in length (154-189 words per vignette).
Participants were presented with each of the six vignettes, one at a time. In an effort to reduce order effects, we randomized the order of the MARK vignettes. Participants were asked to imagine themselves in each scenario and then respond to five questions concerning their likely response. The items following each vignette were based on a 7-point Likert-type scale (1 = not at all and 7 = very much). The first three items directly assessed specific risk perception (e.g., How likely do you think he would make unwanted physical contact with you?), and the remaining two items assessed global risk perception (e.g., What is the likelihood you would find yourself in this type of situation?). Examples of low- and high-risk vignettes are included in the appendix. The full MARK is available from the corresponding author upon request.
Specific and global rating items were summed within each vignette to provide a single value for each set of responses. Higher scores on the Specific Risk Perception and Global Risk Perception scales are indicative of greater levels of the corresponding variable. For ease of interpretation, total scores were standardized (z score transformed) to identify over- and under-reporting of risk. All rating items were presented in the same order for all participants.
Sexual Experiences Survey–Short Form Victimization (SES-SFV)
The SES-SFV (Koss et al., 2007) is a 10-item self-report instrument designed to measure a continuum of unwanted sexual experiences that, at the extreme, indicate legal definitions of rape and attempted rape prior to age 14, from age 14 and above, and within the last 12 months. The items measure the frequency of occurrence of specific sexual experiences on a Likert-type scale of 0 (none) to 3 (three or more), and the frequency of sexual coercion used by the perpetrator on a continuum from verbal persuasion to physical force. The SES-SFV has demonstrated an internal consistency reliability coefficient of .69 and a 1-week test–retest reliability coefficient of .93 (Koss et al., 2007; Koss & Gidycz, 1985). SES-SFV scoring yields five separate groups, which were collapsed into three for the present study due to an imbalance in group size. The non-victim group (Group 1) included individuals who did not endorse any previous history of sexual assault. The sexual coercion/contact group (Group 2) included individuals who endorsed items corresponding to previous experience with sexual assault, but not forcible penetration. The rape/attempted rape group (Group 3) included individuals who endorsed items corresponding to previous experience of sexual assault in which penetration was present or was attempted. The relative sizes of Group 1 (N = 135), Group 2 (N = 93), and Group 3 (N = 97) were consistent with those reported in previous research (Yeater, Treat, Viken, & McFall, 2010).
Impact of Events Scale (IES)
The IES (Horowitz, Wilner, & Alzarez, 1979) is a 15-item self-report measure that assesses the subjective impact of a given traumatic life event in the areas of intrusive and avoidance symptoms. Participants who indicated a history of sexual assault according to the SES-SFV were administered the IES to assess the impact of the sexual assault, or the most recent assault if there were multiple experiences. The purpose of this instrument was to assess subjective ratings of the impact of victimization and to use it as an indicator of previous victimization. The IES has been used with a wide range of events; in the area of rape and sexual trauma, it has been shown to possess good internal consistency (Intrusion subscale α = .79, Avoidance subscale α = .82).
Brief COPE
The Brief COPE (Carver, 1997) is a 28-item scale of coping strategies assessed through self-report with Likert-type items to indicate the frequency of use (1 = I haven’t been doing this at all, 4 = I’ve been doing this a lot). The Brief COPE has been widely used for stressed populations and has adequate internal consistency (all but one subscale α ≥ .60) and test–retest reliability (rs = .46-.86). The scoring procedure for the Brief COPE yields 14 subscales, including Behavioral Disengagement, Denial, Self-Distraction, Self-Blame, Substance Abuse, Active Coping, Positive Reframing, Planning, Humor, Acceptance, Religion, Emotional Support, Instrumental Social Support, and Venting. Although efforts to identify a higher order factor structure have produced divergent results, recent work has demonstrated that behavioral disengagement, denial, self-distraction, self-blame, and substance abuse represent distinct factors within this inventory (Litman, 2006; Mitchell, 2013). For this investigation, alcohol use items were removed from this factor due to their relation to the latent variable of problematic alcohol use.
Alcohol Use Disorders Identification Test (AUDIT)
The AUDIT (Babor, Higgins-Biddle, Saunders, & Monteiro, 2001) was developed by the World Health Organization to screen for excessive drinking behaviors. It contains 10 items, with responses based on a 5-point Likert-type scale. It has been adapted for self-report administration and has demonstrated good construct validity and good test–retest reliability (r = .86).
Procedure
All data were collected online through a university-based study participation website. Participants were directed to the study website through enrollment in undergraduate psychology courses. After logging onto the system, selecting to participate in the investigation, and providing informed consent, participants responded to a demographic survey and completed the MARK. The individual vignettes were randomized to reduce order effects. During this period, participants also responded to the self-report battery. The order of questionnaires was consistent for all participants. Validity items drawn from other measures (e.g., “I have not seen a car in 6 months”) were embedded in the survey to ensure appropriate effort in responding. Upon completion, participants received a debriefing document and contact information for the research team. A university internal review board approved and monitored all study procedures. All participants received course credit based on the duration of their participation.
Results
Table 1 provides descriptive and reliability statistics for study variables for the first series of analyses used to confirm the psychometric properties of the MARK. Visual inspection of frequency distributions revealed an approximately normal distribution of ratings at each risk level, which was confirmed by kurtosis and skewness values within acceptable limits based on the sample size (Yanagihara & Yuan, 2005). The internal consistency estimates ranged from good to very good, suggesting consistent risk responses within each vignette.
Descriptive Statistics for All Study Variables (N = 325).
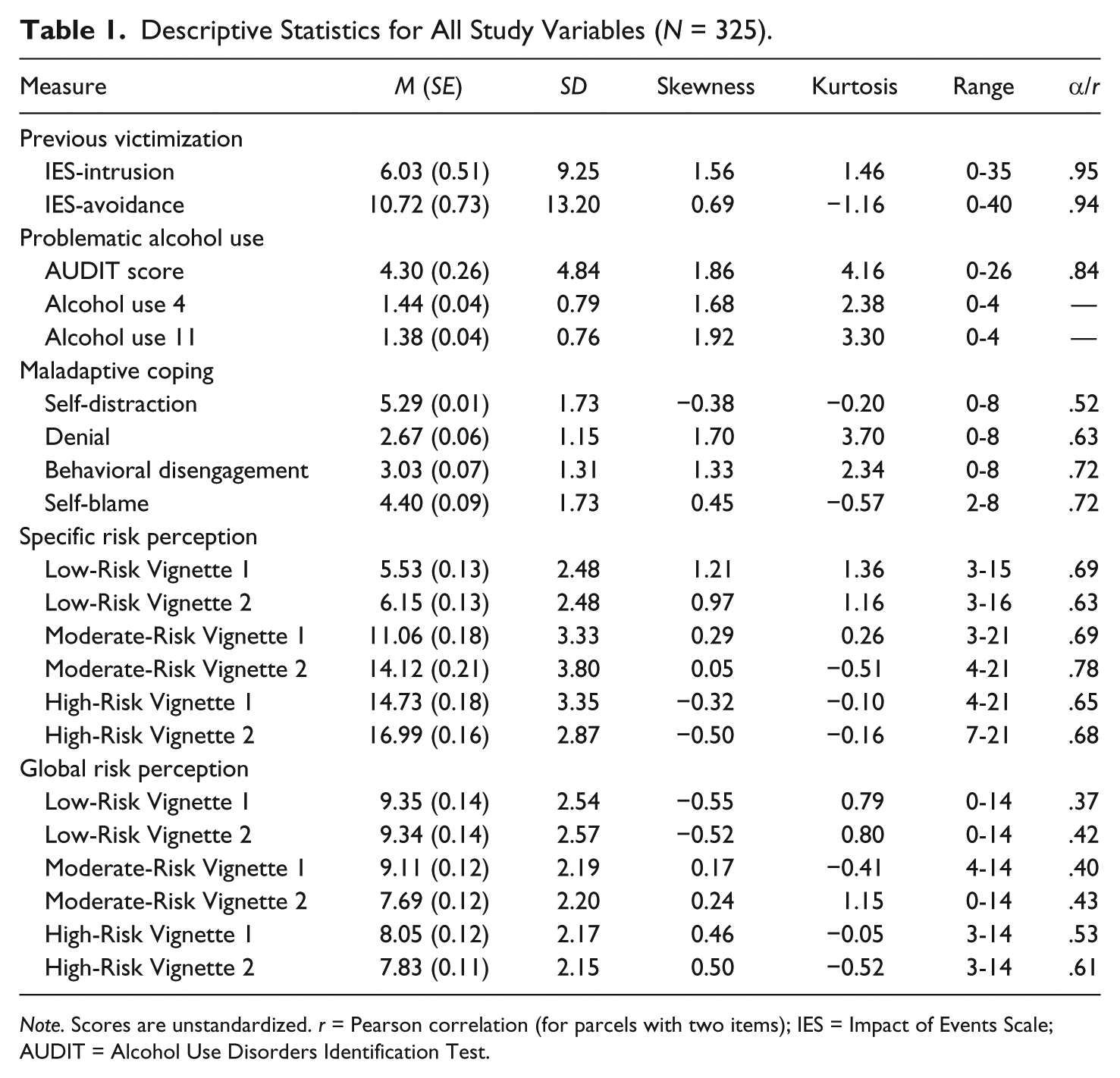
Note. Scores are unstandardized. r = Pearson correlation (for parcels with two items); IES = Impact of Events Scale; AUDIT = Alcohol Use Disorders Identification Test.
We utilized a 3 (risk level) × 2 (vignette) within subjects repeated measures MANOVA to examine the changes in specific and global risk perception ratings. Main effects and interaction terms were tested using the multivariate criterion of Wilks’s Lambda (Λ). Planned pairwise comparisons examined differences within specific and global risk perception ratings across risk levels. The results revealed a significant main effect for risk level, Λ = 0.09, F(8, 305) = 381.27, p < .001, multivariate η2 = .91, with significant differences in specific risk ratings, F(2, 624) = 824.26, p < .001, η2 = .73, and decreases in global risk ratings, F(2, 624) = 42.01, p < .001, η2 = .12. Planned comparisons confirmed increased specific risk and decreased global risk ratings across low-, moderate- and high-risk levels (all ps < .01). The main effect for vignette and the risk by vignette interaction failed to reach significance. Table 1 provides descriptive statistics for the MARK Specific and Global Risk scales at each level of risk. These findings demonstrate that, as expected, the MARK vignettes yielded parametric increases in risk ratings concordant with the increased number of risk factors.
Initial Structural Model Specification
Conclusions regarding the influence of previous victimization, problematic alcohol use, and maladaptive coping on female’s risk perception are drawn from epidemiological and cross-sectional research. Existing theories of risk perception among females typically address specific variables in this complex process. As such, no single theoretical model currently exists that attempts to explain the nature of these relationships concurrently. Because our intention was not to test a distinct theory, we approached this analysis largely from a model-building perspective, taking into account information from several theoretical and empirical accounts prior to model specification and during model modification. Indeed, an ancillary goal of this approach was to identify a suitable model for future investigation.
In SEM, two levels of analysis are conducted simultaneously. These two levels achieve the goals of measuring unobserved (latent) phenomena and describing the strength of the relationships among them. Our primary objective in specifying the initial model was to account for the relationships that have been empirically supported (e.g., between increased alcohol use and decreased risk perception). Our secondary objective in specifying the initial model was to identify additional relationships that may help account for additional variance in the explanation of both specific and global risk perception (e.g., the combined effects of problematic alcohol use and maladaptive coping strategies). In this investigation, the measurement model was specified through consideration of established indicators of the respective variables. The structural model was specified to achieve the objectives described above and to maximize the variance explained by the full model. We chose to allow exogenous latent variables to covary to depict these factors as related, but not causal. Specification was completed prior to fitting the initial model to the data. This initial model is presented in Figure 1. The presentation of findings follows the recommendations by Hoyle and Isherwood (2013).
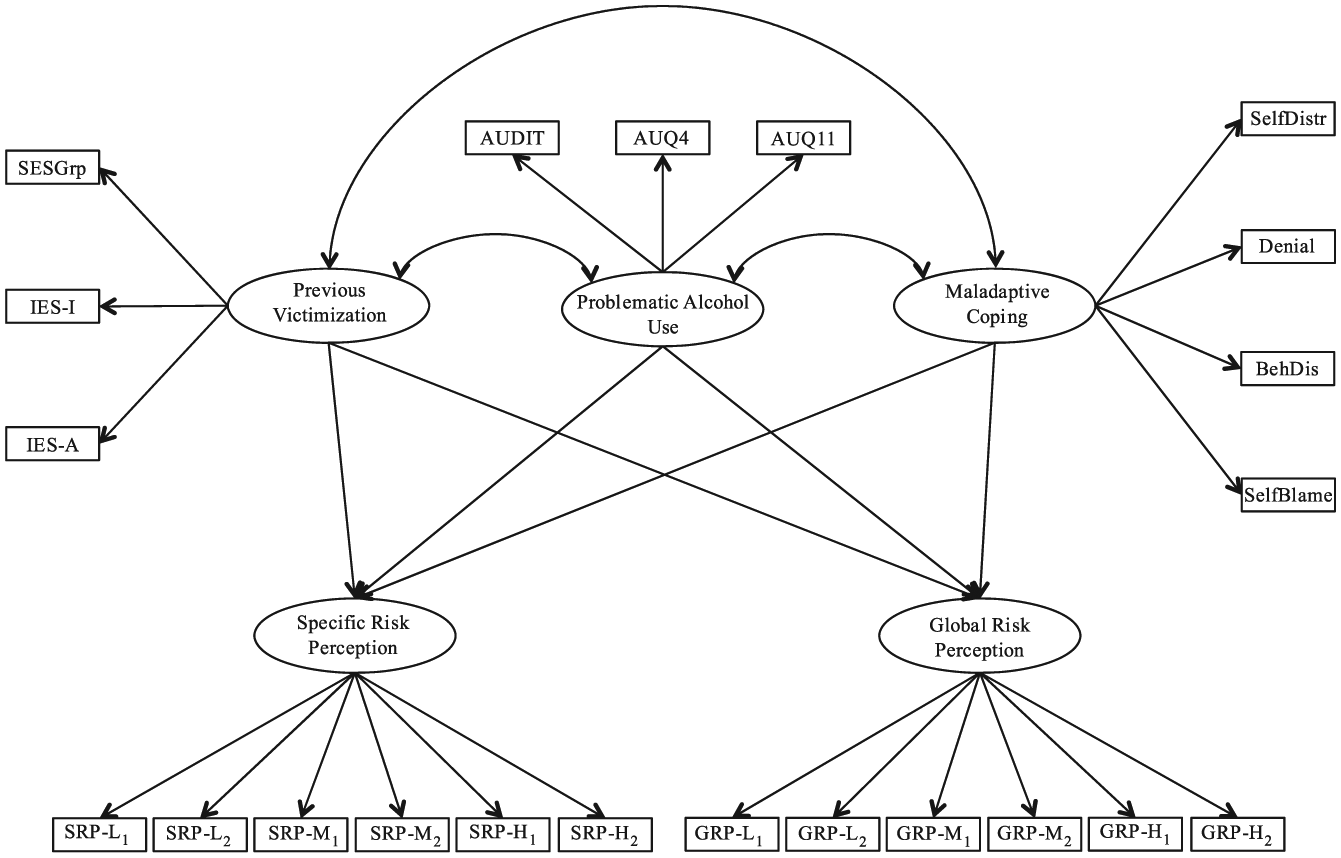
Initial model of sexual assault risk perception.
The structural analysis described here was executed using Mplus version 7.11 (Muthén & Muthén, 2013). Prior to analysis, all variables were inspected for missing values and non-normality. The final data set contained 13 cases with missing at random (MAR) data. These data were replaced using full information maximum likelihood (FIML) procedures. Univariate measures of skewness and kurtosis were examined. Any variable yielding values greater than 1.96 were considered for transformation (Tabachnick & Fidell, 2013). Due to their significant positive skewness, the AUDIT, IES-Intrusion, and IES-Avoidance scales were log transformed. The skewness values of the resulting variables were within acceptable limits.
Latent variables were indicated by both item- and parcel-level observed variables. Item-level variables included two alcohol use questions from the Brief COPE, which were used as indicators of problematic alcohol use, due to their focus on alcohol consumption. Parcel-level indicators comprised the remainder of the observed variables. This model also contained both categorical and continuous factor indicators. The use of both types of variables is appropriate when not redundant (i.e., when a single item is not used both within a parcel and as an item-level indicator). Table 2 provides zero-order correlations of the study variables.
Zero-Order Correlations Among Study Variables.
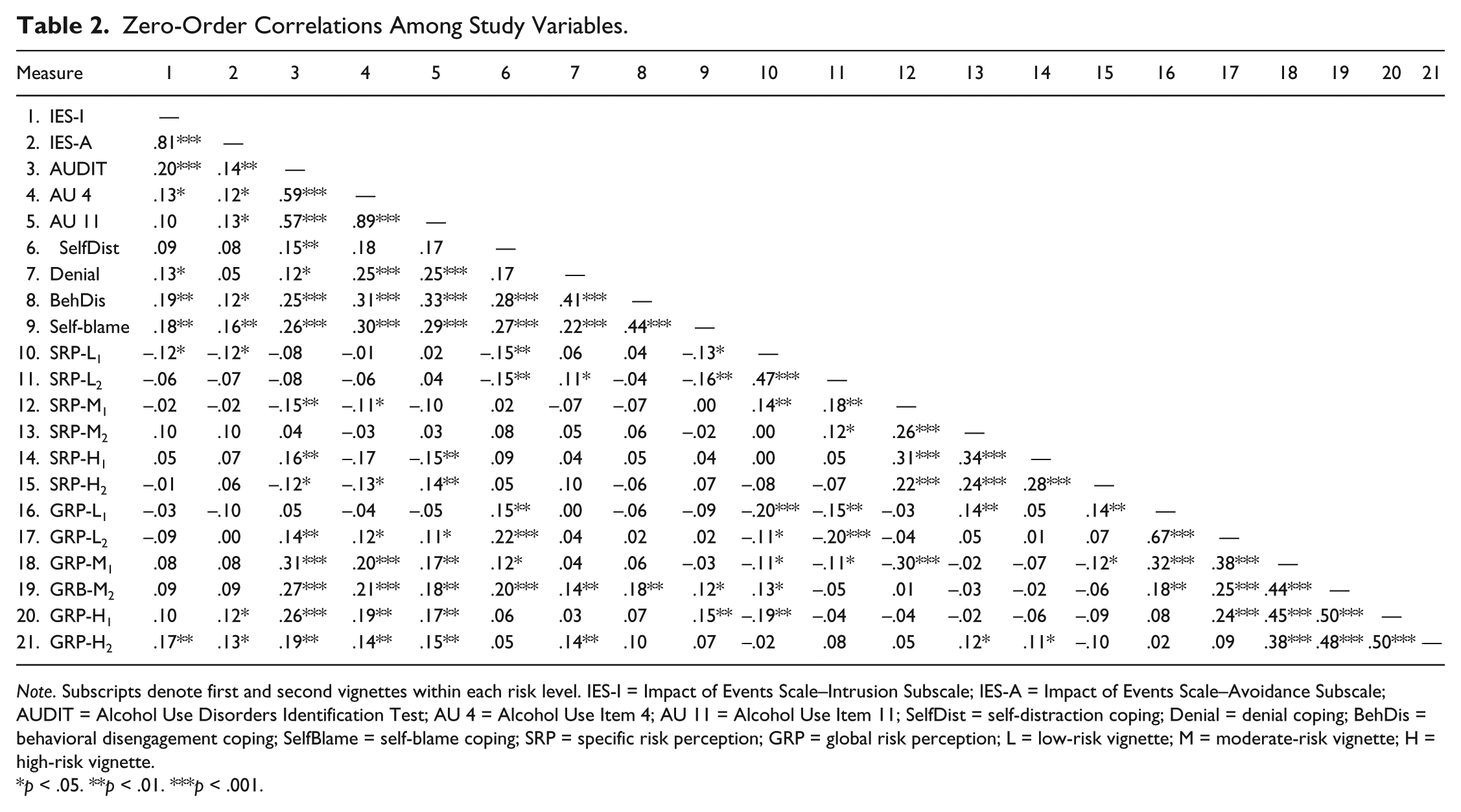
Note. Subscripts denote first and second vignettes within each risk level. IES-I = Impact of Events Scale–Intrusion Subscale; IES-A = Impact of Events Scale–Avoidance Subscale; AUDIT = Alcohol Use Disorders Identification Test; AU 4 = Alcohol Use Item 4; AU 11 = Alcohol Use Item 11; SelfDist = self-distraction coping; Denial = denial coping; BehDis = behavioral disengagement coping; SelfBlame = self-blame coping; SRP = specific risk perception; GRP = global risk perception; L = low-risk vignette; M = moderate-risk vignette; H = high-risk vignette.
p < .05. **p < .01. ***p < .001.
All parameter estimates were completed using unweighted least squares mean- and variance-adjusted χ2 (UWLSMV or Robust ULS) estimation, which is capable of parameter estimation involving both continuous and categorical variables, is appropriate for small samples, and is less impacted by non-normality. All path estimates presented were standardized. Following parameter estimation, the omnibus model fit was assessed through multiple fit indices using the following guidelines for adequate fit provided by Hu and Bentler (1999): comparative fit index (CFI) > .90, Tucker–Lewis index (TLI) > .90, and root mean square error of approximation (RMSEA) ≤ .06, p of Close Fit (PCLOSE) > .50. The χ2 test of model fit was also examined and reported; however, because this index is often heavily influenced by sample size, it is not discussed in depth. All models fit to the data were identified. No adjustments to convergence criteria were made.
The fit of the initial model was marginally inadequate: χ2(199) = 565.09, p < .001, CFI = 0.659, TLI = 0.602, RMSEA = 0.075, 90% confidence interval (CI) = [0.068, 0.083], PCLOSE = 0.00. Based on these results and an examination of factor indicators, we re-specified the endogenous variable indicators to improve the measurement model of the specific and global risk perception latent variables. Specifically, we examined factor-loading estimates to determine which observed variables poorly represented the underlying construct. This process led us to remove (fix to 0) the Specific and Global Risk Rating scales from both low-risk vignettes. These observed variables were weak indicators likely due to the homogeneity of ratings across all subjects. Further examination did not suggest a poorly specified measurement in other latent variables. Non-significant pathways between previous victimization and specific risk perception, as well between maladaptive coping and global risk perception, were fixed to 0 for the subsequent model.
This model yielded an improved, but still inadequate fit: χ2(127) = 221.48, p < .001, CFI = 0.891, TLI = 0.869, RMSEA = 0.040, 90% CI = [0.038, 0.058], PCLOSE = 0.538. As an exploratory measure, we consulted modification indices produced with parameter estimation to identify misspecified pathways. These indices suggested that allowing measures of specific and global risk to covary would significantly improve the model fit. These changes to the model are conceptually appropriate, given that each set of ratings for these scales was based on the same vignette and, thus, shared variance. We then re-ran this model to obtain parameter estimates and factor loadings. Figure 2 presents the final model with standardized factor loadings and parameter estimates.
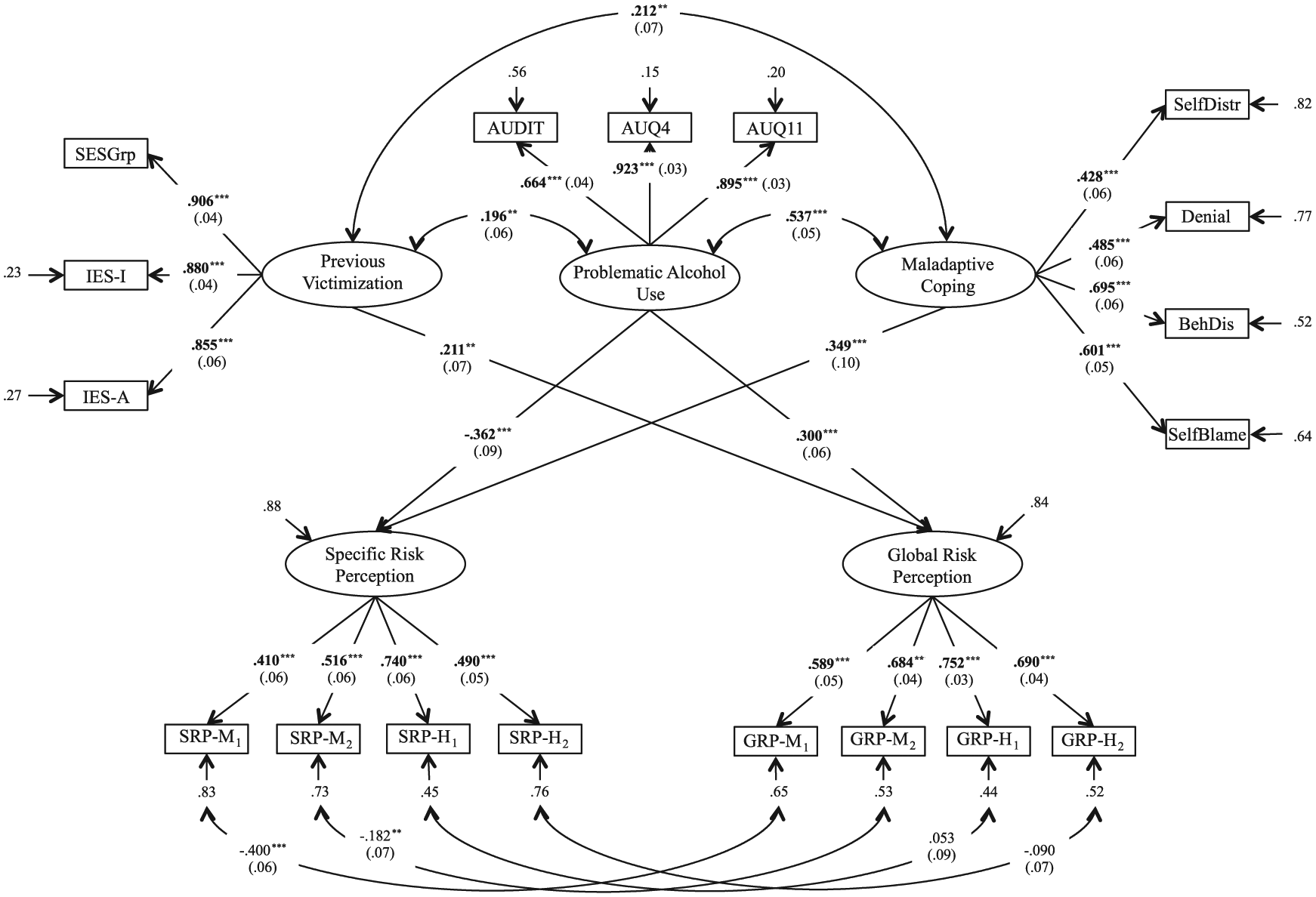
Final model of sexual assault risk perception.
This final model provided the best omnibus model fit: χ2(123) = 182.20, p < .001, CFI = 0.932, TLI = 0.915, RMSEA = 0.038, 90% CI = [0.026, 0.050], PCLOSE = 0.952. Inspection of this model revealed several key findings that are consistent with data reported in the literature, as well as some relationships not previously examined. Primarily, whereas previous victimization did not predict specific risk perception, β = 0.01, ns, it did predict global risk perception, β = 0.21, p < .01, 95% CI = [0.07, 0.39]. Similarly, maladaptive coping was positively related to specific risk perception, β = 0.35 p < .001, 95% CI = [0.16, 0.60], but was unrelated to global risk perception, β = 0.11, ns. Problematic alcohol use was related to both types of risk perception, but in opposing directions. Specifically, greater problematic alcohol use was associated with decreased specific risk perception, β = −0.36, p < .001, 95% CI = [−0.54, −0.13], but increased global risk perception, β = 0.30, p < .001, 95% CI = [0.18, 0.46]. As expected, the relationships among previous victimization, problematic alcohol use, and maladaptive coping each reached significance (all ps < .01), adding support to the reciprocal nature of these variables.
Discussion
The goal of this study was to develop and test a structural model of the relationships between previous victimization, problematic alcohol use, and maladaptive coping style on both specific and global risk perceptions among heterosexual college females. While the initial model did not adequately fit the data, the subsequent re-specifications yielded a very good parameter estimation and model fit. A number of the findings from the final model have important theoretical ramifications for the field.
Previous research is equivocal in establishing whether individuals with a history of previous victimization evidence deficits in risk perception. Figure 2 illustrates the significant relationships in the model that are discussed here. Our data suggest that while previous victimization is associated with a global sense of increased risk, it does not translate into a heightened perception of risk for sexual assault in specific situations.
Problematic alcohol use is directly associated with previous victimization. Furthermore, problematic alcohol use mediated opposing effects on specific and global risk perceptions. That is, higher alcohol use was associated with decreases in specific risk perception, but increases in global risk perception. This pattern suggests that as an individual’s use of alcohol increases, the individual perceives less risk in specific situations, yet perceives a greater general sense of risk. These findings are consistent with the previous literature and support the conclusion that alcohol use is critical to understanding the risk perception process.
Finally, maladaptive coping was directly associated with increases in specific risk perception, but it was unrelated to global risk perception. While maladaptive coping is typically associated with a number of negative outcomes in terms of psychological adjustment, our data indicate that in isolation, maladaptive coping does not lead to decreases in specific risk perception. However, maladaptive coping is associated with increased alcohol use, which in turn, is associated with decreases in specific risk perception. Therefore, an interaction among these variables seems to be highly likely given the documented vulnerability for revictimization within this population (Macy, Nurius, & Norris, 2007).
The results from this study carry a number of interesting implications for theory, research, and prevention. Although generally consistent with the literature, these findings support the conclusion that previous victimization itself is not directly related to decreases in specific risk perception; rather, it is the combination of previous sexual assault, higher levels of alcohol use, and maladaptive coping that is important for understanding these deficits. The theoretical implications are therefore most clearly understood as descriptive, as opposed to explanatory. We expect this model will offer new information toward building a comprehensive model of sexual assault risk perception and victimization among college females.
Moreover, while females with a history of sexual assault may engage in increased alcohol use and other maladaptive coping strategies that lead to decreases in their ability to recognize dangerous situations, it is likely that they still directly recognize their vulnerability on a global level. That is, appraising risk in social situations (global) and predicting the likelihood that assault would occur (specific) may be orthogonal processes. Therefore, prevention programs may be able to leverage or capitalize on this general awareness of risk to help support awareness of specific risk factors in heterosexual social interactions. This can be accomplished through psychoeducation and by role-play of avoidance and escape strategies. Finally, helping at-risk individuals avoid victimization should therefore involve not only addressing their ability to recognize and respond to risk but also decrease their patterns of alcohol use and increase positive coping behaviors.
Future Directions
The MARK is a promising tool for assessing risk perception among females. In light of the initial evidence we presented here, the continued development of this instrument is important. Although the empirically derived risk factors help establish content validity, the demonstration of convergent and divergent validity would extend the utility of this instrument. Indeed, within the final model, we observed factor loadings slightly below optimal levels. Future studies should focus on optimizing the measurement models of latent variables. Similarly, because we did not have the opportunity to re-assess risk perception across a discrete time period, evidence of the MARK’s temporal stability is an important goal for future investigations.
Given the cross-sectional nature of this investigation and the reliance on self-report data, these findings should be corroborated through longitudinal methodology and multiple modalities of measurement over time. Because the data were collected at one point in time, we are unable to determine if the target characteristics were present before instances of sexual assault or if they developed following victimization. These issues carry significant consequences for model specification, particularly alternative models to the one presented here. Future investigations addressing these limitations should also focus on the role of protective factors (e.g., appropriate vigilance, situation selection) and specific male characteristics (e.g., presence of sexual aggression) in both risk perception and revictimization. Understanding what actions individuals may take to avoid sexual assault is crucial to determine how potential interventions, like those described above, should be developed and delivered.
Footnotes
Appendix
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.