
Abstract
This study examined the mediating and moderating impact of fear of victimization on the relationships between forcible and vicarious rape on depression and post-traumatic stress disorder (PTSD) among college women. Forcible and vicarious rape positively affected PTSD and depression symptomology, but fear did not mediate these relationships. Fear moderated the impact of forcible rape on PTSD, but was not a moderator for depression. Findings suggest that there may be “healthy” levels of fear in the aftermath of victimization where having too little fear may leave women unnecessarily vulnerable to victimization, while having too much fear may lead to social isolation and withdrawal.
Keywords
Perhaps because of its violent and extremely invasive nature, rape is among the most feared types of victimization by women (Ferraro, 1996). In fact, evidence suggests that fear of victimization 1 is fear of rape for women (Dobbs, Waid, & Shelley, 2009; Ferraro, 1996; Fisher & Sloan, 2003). Women’s fears may be warranted—rape victims suffer from post-traumatic stress disorder (PTSD), depression, substance use, and suicide ideation and/or attempts at higher rates and for longer periods than victims of other forms of trauma (Campbell, Dworkin, & Cabral, 2009; Resick, 1993). Furthermore, college women appear to be at higher risk for rape than the general population (Fisher, Sloan, Cullen, & Lu, 1998), making them particularly vulnerable to such negative outcomes. Most victims of rape experience fear as a result of the trauma (Hale, 1996; Resick, 1993); however, they likely do not experience fear in exactly the same way (e.g., Ferraro, 1996; Girelli, Resick, Marhoefer-Dvorak, & Hutter, 1986; Wilcox, Jordan, & Pritchard, 2007; Wilcox Rountree, 1998). Some women may suffer from very high levels of fear, while others may experience low levels of fear; some may significantly alter their behaviors in the aftermath of rape, while others may not change their lifestyles or routines at all. Although most scholars accept the notion that “disproportionate” levels of fear (e.g., Hale, 1996; Warr, 2000)—especially high fear—can be particularly harmful, only recently have scholars begun to examine what might constitute problematic or “dysfunctional” fear (Gray, Jackson, & Farrall, 2011; Jackson & Gray, 2009). In addition, very little research has examined whether fear might moderate the impact of rape on negative outcomes such as mental health outcomes. In the current study, we seek to address these issues by examining the interrelationships between rape, fear of victimization, and mental health outcomes (e.g., PTSD and depression) among college women.
Rape and Mental Health Among Women
Rape is an extremely traumatic event and can have devastating outcomes to interpersonal health. In their review of sexual assault and women’s mental health outcomes, Campbell et al. (2009) reported that up to 65% of rape victims develop PTSD and up to 51% meet the criteria for depression in the aftermath of the trauma. Studies indicate that sexual assault trauma can have both short-term and long-term effects with victims suffering negative mental health symptoms for weeks, months, and even years after the assault (Campbell et al., 2009; Frazier, 2000; Girelli et al., 1986; Resick, 1993).
Some scholars have argued that there is “something about rape itself” that makes rape victims, as opposed to victims of other traumatic events, particularly vulnerable to experiencing negative consequences and emotions long after the assault occurs (Ullman & Filipas, 2001, p. 370). Perhaps feelings of life endangerment or distress during the assault engender subsequent fear, anxiety, guilt, self-blame, humiliation, and numbness after the incident (Campbell et al., 2009; Kaysen, Morris, Rizvi, & Resick, 2005). It might also be the aggressive and personally intrusive nature of rape that elicits such problems among victims, explaining why forcible rape is so detrimental to mental health outcomes, such as PTSD and depression (Resick, 1993; Ullman, Filipas, Townsend, & Starzynski, 2007; Zinzow et al., 2010).
Fear may be the most consistent outcome of rape, though, with over 70% of rape victims developing fear and/or anxiety as a consequence of rape (Campbell et al., 2009). However, it is likely that women do not experience fear in exactly the same way (Ferraro, 1996; Girelli et al., 1986; Wilcox et al., 2007; Wilcox Rountree, 1998). Fear may provoke women to avoid certain places or people at certain times of the day (Fisher & Sloan, 2003); take precautionary measures, such as altering their dress or their drinking habits; or withdraw from risky activities altogether (Rader, Cossman, & Allison, 2009). Scholars suggest that fear can lead to defensive behaviors, such as installing alarms and purchasing weapons, that are meant to alleviate fear by making victims feel more secure, while others suggest that both avoidance and defensive behaviors can actually lead to more fear (Liska, Sanchirico, & Reed, 1988; Rader, May, & Goodrum, 2007). In addition, fear may become so restrictive that it leads to further mental health deterioration, and feelings of isolation, helplessness, and depression (Stafford, Chandola, & Marmot, 2007). Previously unexplored, however, is whether different levels of fear among college women mitigate or exacerbate the effect of rape on their mental health outcomes. We consider this possibility in the subsequent sections.
Fear of Victimization
According to Warr (2000), fear is the consequence of one’s perceived risk of victimization. One of the strongest predictors of fear is gender/sex, in that women are more fearful of victimization (Hale, 1996; Warr, 2000). However, as noted above, for women, fear of victimization equates to fear of sexual assault. Ferraro (1996) found that fear of rape “shadows” fear of other forms of victimization among women, and concluded that fear of rape is women’s fear of crime, regardless of their perceived risk of assault. This “shadow thesis” has been supported by other research (e.g., Fisher & Sloan, 2003). In addition, women tend to fear sexual assault by a stranger more than rape by an acquaintance (Hickman & Meuhlenhard, 1997; Wilcox et al., 2007), and are just as fearful when learning of rape vicariously, such as knowing someone who has been raped or hearing about it from others (Hale, 1996). Thus, when examining fear among women, it is important to understand that their fear is predominantly related to their fear of being sexually assaulted, particularly by strangers, and they are more fearful when they have been previously victimized or know of someone who has been raped.
Fear can be both beneficial and problematic (Warr, 2000; Wilcox et al., 2007). On one hand, fear might prevent someone from victimization if they take the necessary precautions to protect themselves. On the other hand, fear can have negative consequences if it is unduly restrictive, constrains behaviors, or changes routines (Fisher & Sloan, 2003; Warr, 2000). For instance, “excessive” or “disproportionate” fear, especially relative to one’s actual risk of victimization, can carry with it both interpersonal consequences (e.g., avoidance behavior, not going out at night, feelings of isolation, or vulnerability) and aggregate consequences (e.g., withdraw from community activities, avoidance of particular places; see Hale, 1996; Skogan, 1986; Warr, 2000). Fear can also affect physical and mental health (Stafford et al., 2007). Extremely high levels of fear might restrict what activities people engage in and where they go—in a sense, leaving them socially paralyzed and socially isolated, which might in turn exacerbate negative mental health outcomes. Being restricted in terms of activities outside the home and/or interacting with others might reduce opportunities to form social ties with others. Stafford and colleagues (2007) suggested that less physical activity and more social isolation can lead to poor physical and mental health; in fact, they found that highly fearful adults in London were 50% more likely than those with low levels of fear to exhibit symptoms of mental disorder and 90% more likely to have symptoms of depression.
Most scholars tend to focus on the negative effects of high levels of fear, but certainly, having too little fear might also be detrimental; if, for example, one has no fear, they may not take simple precautions to guard against crime, thus leaving themselves unnecessarily vulnerable to victimization (Jackson & Gray, 2009; Warr, 2000). Very low levels of fear, then, may put individuals further at risk for victimization, which in turn might increase negative mental health outcomes. To date, the potential mental health benefits of moderate or “healthy” levels of fear have not been thoroughly examined in the literature. Healthy levels of fear may reflect a healthy appraisal of the dangers of social life, as well as a sense of agency when dealing with these threats. Perhaps a “healthy” level of fear is fear that leads to protective behaviors, thus reducing one’s potential level of victimization, but which does not lead to excessive levels or attempts at protection, withdrawal, or significant changes in one’s normal activities. Jackson and Gray (2009) and Gray et al. (2011) term normal or healthy fear as “functional” fear, that which can lead individuals to feel safer, take reasonable precautions to reduce their risk of victimization, and which does not impede or harm their quality of life. These scholars assert that fear can increase problem solving and allow individuals to anticipate and prepare for threatening events.
As most research has focused on the detrimental effects of high fear, we believe the potential impact of other levels of fear—including low and moderate fear—need to be examined more thoroughly to determine whether various fear levels affect mental health problems differently. The primary goal of our research is to examine high, average, and low levels of fear and determine if fear mediates or moderates the relationship between rape and mental health outcomes (depression and PTSD) among college women. In addressing this goal, we examine three research questions.
Drawing from prior research, we anticipate that prior rape victimization and mental health symptoms will be highest when fear levels are high.
We expect that rape will be strongly related to fear, and that including fear in our multivariate models will partially mediate or reduce the relationship between rape and PTSD and depression symptomology.
Specifically, we predict that the impact of rape on PTSD and depression symptomology will be strongest both when levels of fear of victimization are highest and when levels of fear of victimization are lowest.
Data and Measures
The data for our study are the result of the National Women’s Study–Replication (Kilpatrick, Resnick, Ruggiero, Conoscenti, & McCauley, 2007). The sample was recruited using the American Student List (ASL), the largest and most widely used list of college students in the United States (Kilpatrick et al., 2007). The sample was divided into nine geographic regions, and women were called in proportion to the U.S. Census representation of the population of American college women in each region (Paul et al., 2014). Women aged 18 years and older were interviewed using a computer-assisted telephone interviewing (CATI) system. When a residence had more than one woman who met study criteria, the woman with the most recent birthday was selected for interview.
Due to the sensitive nature of the interview, two steps were taken to increase the likelihood that questions could be answered in an open and honest manner. First, the women were asked if they were in a situation where they could be assured of privacy and could answer in an open manner. If not, the interviewer offered to call back at another time when privacy was more likely. Second, the interview was designed primarily with closed-ended questions (Paul et al., 2013).
The sampling frame contained approximately 17,000 individuals and was restricted to women attending 4-year institutions of higher education. There were 253 different colleges and universities included in the sample from 47 different states. Among those women determined to be eligible to participate, 73.5% completed interviews (Paul et al., 2013). The sample includes 2,000 survey respondents.
Dependent Variables
The dependent variables for our study are symptoms of PTSD and depression. PTSD and major depression symptomology were assessed using modules from the original National Women’s Study (Ruggiero et al., 2004). These measures have been found to have acceptable levels of reliability and validity (Kilpatrick et al., 2003). For the current study, PTSD symptomology consisted of 20 items measuring experiences such as loss of interest in activities, repeated nightmares, flashbacks, avoidance behaviors, sleep difficulties, hypervigilance, and angry outbursts (α = .902). Depression symptomology includes 13 items tapping experiences such as an increased or decreased appetite, excessive sleeping, feeling tired and low energy, feelings of worthlessness, difficulty concentrating, thoughts of hurting oneself, and thoughts of death or being better off dead (α = .869). In all models, our dependent variables are logged to reduce skewness.
Rape Variables
Respondents were asked if they had ever 2 been forcibly raped or learned of rape from someone else vicariously. Forcible rape is a dichotomous variable which denotes if women answered affirmatively that one or more of the following had ever happened to them: (a) a man or boy made them have sex by using force or threatening to harm them or someone close to them, (b) someone made them have oral sex by force or by threatening to harm them, (c) someone made them have anal sex by force or by threatening to harm them, and (d) someone put fingers or objects in their vagina or anus against their will by using force or threatening to harm them. Vicarious rape is also a dichotomous variable denoting if the respondent answered affirmatively to one or both of the following: (a) a woman or girl ever directly told you that someone forced her to have sexual intercourse, oral sex, or anal sex when she did not want to, and (b) a woman or girl ever directly told you that someone had sexual intercourse, oral sex, or anal sex with her when she did not want to after she was extremely high or passed out due to alcohol or drug use (r = .279, p < .001).
Fear of Victimization
Because we are interested in women’s fear—whether perceived or acted upon—our measure of fear of victimization taps past and current fear and contains both a perceptual component and a behavioral component. The perceptual component is the result of a factor analysis of three questions: (a) How safe do you think you are in your community (factor loading = .576)? (b) How worried are you personally about being sexually abused or attacked (factor loading = .841)? (c) How worried are you personally about being physically abused or attacked (factor loading = .872)? The behavioral component is also the result of a factor analysis of three questions: Has fear of being physically or sexually attacked caused you to (a) limit places or times you go shopping (factor loading = .823)? (b) limit places or times you will work (factor loading = .786)? (c) limit places you will go by yourself (factor loading = .682)? These factors were standardized and then summed to create one combined measure of fear of victimization. From this overall measure, we also created measures of levels of fear of victimization. Respondents with low levels of fear are those with a score that falls one or more standard deviations below the mean on the fear of victimization measure. Similarly, respondents with high levels of fear of victimization are those with a score that falls one or more standard deviations above the mean. Finally, those with average levels of fear have scores that fall less than one standard deviation above or below the mean.
Control Variables
Because binge drinking and substance abuse are often associated with sexual assaults among college students (Fisher et al., 1998), we include controls for each of these measures. Binge drinking is defined as having five or more drinks at a time at least once per month. Substance abuse indicates that women answered yes to at least one of the negative consequences of substance use assessed by the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) (e.g., charged with driving under the influence [DUI], substance use caused trouble with employer). Because the theoretical processes of interest might differ for new college students as compared with more mature college students, dichotomous controls are included for sophomore, junior, and senior year students. Graduate students are collapsed with seniors, and freshman is the reference category. Nontraditional age indicates that the woman was over 25 years old. Separate questions were asked for race and ethnicity so each respondent has both an ethnicity (Hispanic or non-Hispanic) as well as a race (African American, Asian, or Other race), with White as the reference category. An income variable is included that reflects parents’ or primary guardians’ total household income according to the following categories: 1 = less than US$10,000; 2 = US$10,000-$19,999; 3 = US$20,000-$39,999; 4 = US$40,000-$59,999; 5 = US$60,000-$79,999; 6 = US$80,000-$99,999; 7 = US$100,000-$199,999; 8 = US$200,000 or greater. Mean imputation was used to replace missing data on income. The vast majority of respondents were never married, and a dichotomous variable distinguishes these women from those of other marital or relationship circumstances.
The remaining control variables reflect circumstances of the victimization. We include a dichotomous variable reflecting the experience of multiple rapes in the respondent’s lifetime (more than one rape was coded as “yes”). We also include a dichotomous variable called recent event that indicates that the rape occurred during the current school year.
Method
Our analysis progresses in stages as we address each of our research questions. First, we examine how rape, mental health, and background characteristics are distributed by levels of fear of victimization through the use of chi-square tests and ANOVAs. We then use ordinary least squares (OLS) regression models to examine the predictors of fear of victimization. Our next step is to use OLS regression models to assess to extent to which fear mediates the impact of rape on mental health outcomes. For both PTSD and depression, we run one multivariate model that excludes fear of victimization and another model that includes fear of victimization. If the inclusion of fear of victimization in the second model reduces the effect of the theoretical variables, this suggests that fear of victimization is at least part of the explanation for why victimization affects PTSD and depression. Finally, we examine the extent to which fear moderates the effect of rape on mental health symptomology. In other words, is the relationship between victimization and mental health symptomology different for women with low, moderate, or high levels of fear of victimization? To determine whether the effects of rape on each mental health outcome are statistically different across these three levels of fear, we conduct equality of coefficients tests (Clogg, Petkova, & Haritou, 1995). To ease interpretation of our findings, “fear of victimization” is operationalized as a continuous variable as a mediator and a three-level categorical variable as a moderator. Due to our novel approach of adopting fear of victimization as a moderating variable, we also examine, in an exploratory fashion, the extent to which control variables of interest are moderated by levels of fear.
Results
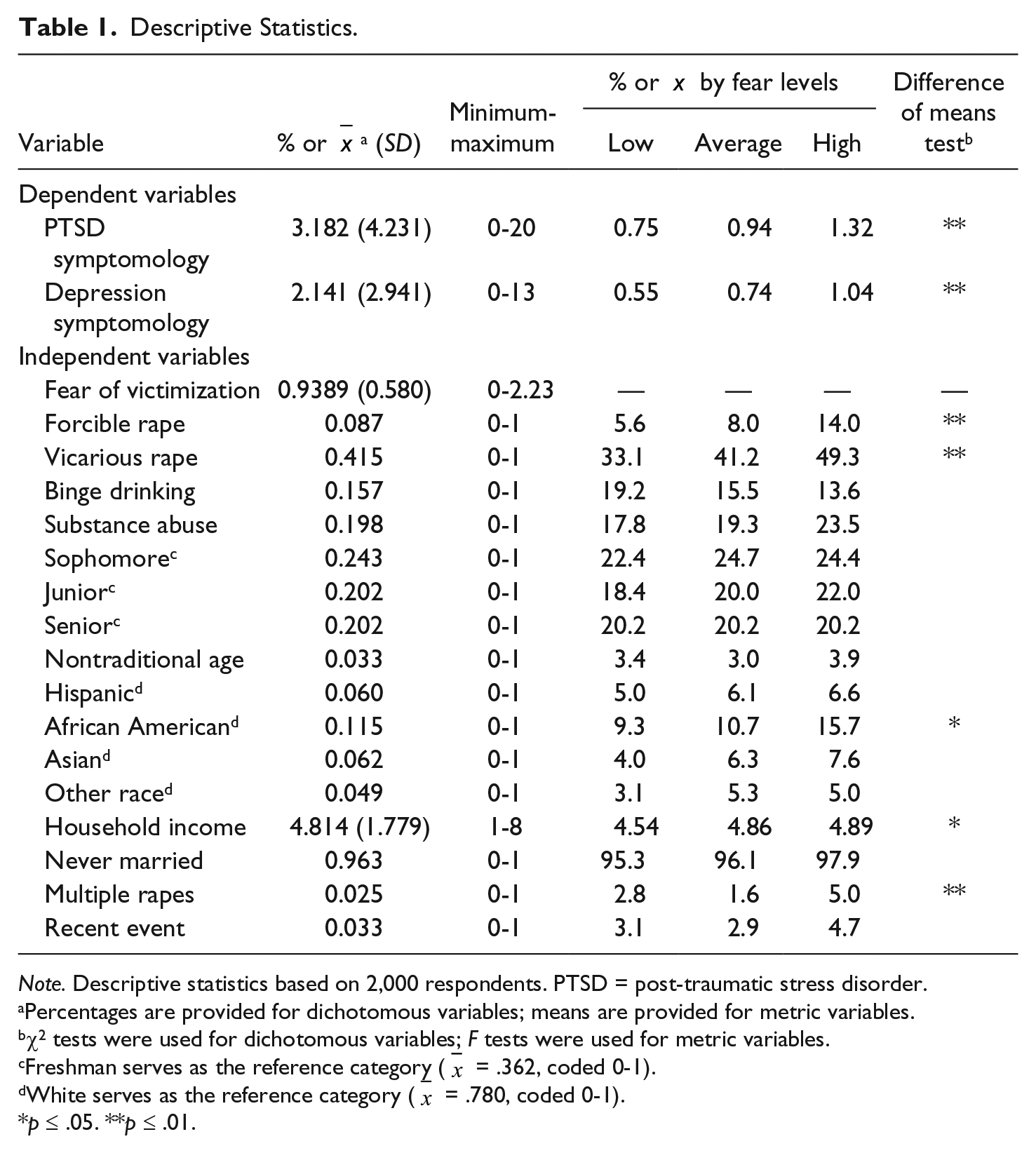
Table 1 presents the descriptive statistics for all variables in our analysis. Regarding our dependent variables, the mean for PTSD symptomology is 3.182 out of a total of 20 possible symptoms. The mean for depression symptomology is 2.141 out of a total of 13 possible symptoms. Regarding the victimization variables, 8.7% of women in the sample reported having been a victim of forcible rape and approximately 42% reported having someone confide in them that they had been raped (vicarious rape). The sample is fairly evenly distributed across year of school, with the largest percentage of women being freshmen (35.3%). Six percent were Hispanic, and the most common racial category is White (77.4%). The vast majority of the females had never been married. Finally, concerning the rape experiences, 2.5% of women experienced multiple rapes and 3.3% reported that their victimization was recent (within the current school year). Only a small minority of the sample (3.3%) were above the age of 25.
Descriptive Statistics.
Note. Descriptive statistics based on 2,000 respondents. PTSD = post-traumatic stress disorder.
Percentages are provided for dichotomous variables; means are provided for metric variables.
χ2 tests were used for dichotomous variables; F tests were used for metric variables.
Freshman serves as the reference category (
White serves as the reference category (
p ≤ .05. **p ≤ .01.
The chi-square tests and ANOVAs in Table 1 address our first research question regarding the distribution of rape experiences, mental health symptomology, and background characteristics by levels of fear. First, those respondents who had experienced forcible rape or vicarious rape were more likely to experience higher levels of fear of victimization. Women who experienced greater PTSD and depression symptomology also reported higher levels of fear of victimization. Regarding socio-demographic variables, African Americans are significantly more likely to report higher levels of fear of victimization. Moreover, the lowest level of fear of victimization was associated with the lowest reported household income. Finally, those expressing the highest levels of fear of victimization were more likely to report having been raped multiple times.
Our second research question concerns the effect of rape on fear and the mediating effect of fear on the relationship between rape and mental health outcomes. Table 2 examines this question with OLS regression models. Model 1 demonstrates that controlling for relevant factors, experiencing forcible rape or vicarious rape is significantly related to fear of victimization. 3 The standardized coefficients (β = .074 and β = .077, respectively 4 ) are nearly similar in size. In other words, one’s own victimization has a similar relationship with fear of victimization as having someone confide in you regarding their victimization. Other factors related to higher levels of fear of victimization include substance abuse problems, being African American or Asian (as compared with Whites), having a higher household income, and having never been married. Reporting binge drinking, in contrast, is negatively related to fear of victimization. Overall, our model explains only about 3% of the variance in reported fear of victimization.
OLS Models Predicting Fear of Victimization and Mental Health Symptomology Outcomes.

Note. The values represent b (SE). OLS = ordinary least squares; PTSD = post-traumatic stress disorder.
Continuous measure.
p ≤ .05. **p ≤ .01.
Table 2 also includes models predicting PTSD symptomology and depression symptomology, and these models allow us to examine the mediating effect of fear on the relationship between rape and these negative mental health outcomes. First, Models 2 and 4 indicate that forcible rape and vicarious rape have a positive, significant impact on PTSD and depression symptomology. Forcible rape has a standardized coefficient of 0.155 and is the most important variable in Model 2. Other important predictors of PTSD include vicarious rape, substance abuse problems, African American, lower levels of household income, and experiencing multiple rapes. The corresponding results for depression symptomology (Model 4) are very similar to those for PTSD. Forcible rape is the most important predictor of depression symptoms (β = .136). Other important predictors include vicarious rape, substance abuse problems, Hispanic ethnicity, African American, lower levels of household income, and experiencing multiple rapes. Overall, these models indicate that negative mental health outcomes are consistently related to not only one’s own rape victimization but also the known victimization of other women. However, Models 3 and 5 indicate that fear does little to mediate these effects. Although the regression coefficients related to victimization are reduced slightly when fear is included, they are still important predictors of PTSD and depressive symptomology. Fear of victimization has a significant direct effect on PTSD symptomology and is the most important variable in the model (β = .161); the same is true for the depression symptomology model (β = 0.154). Overall, the model including fear explains about 14% of the variance in PTSD symptomology and about 11% of the variance in depression symptomology.
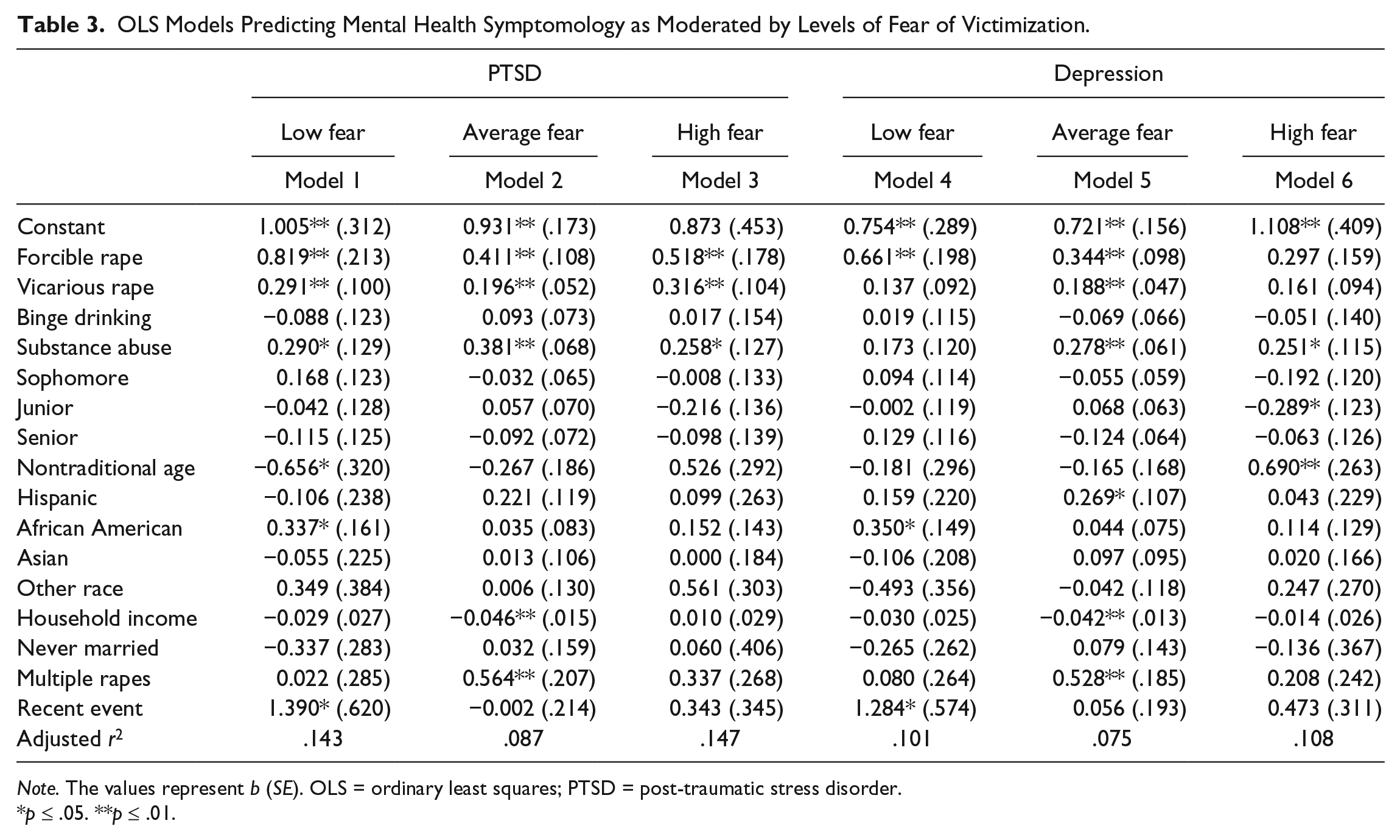
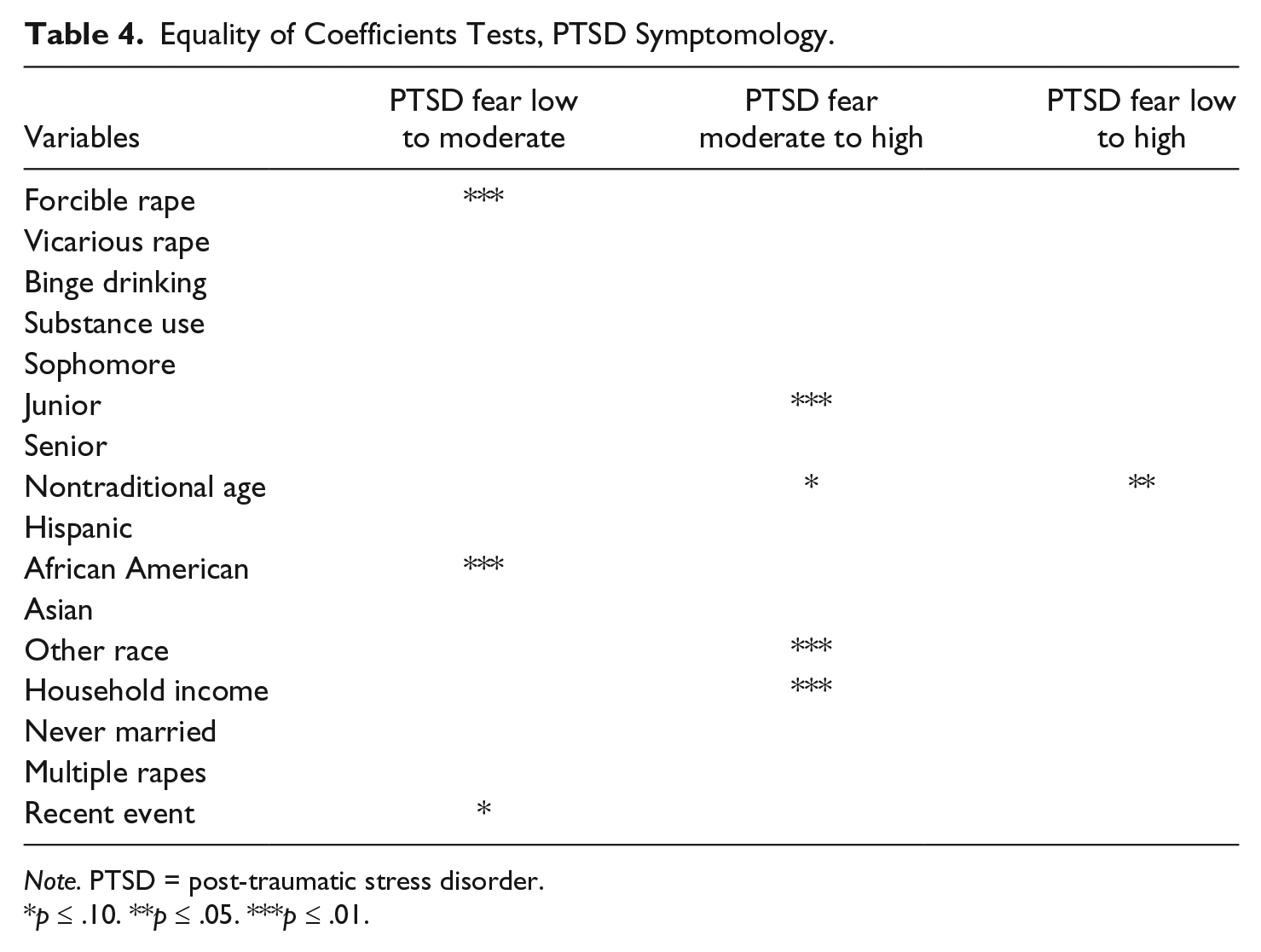
Our final research question addresses the possibility that the effect of rape on mental health outcomes may depend in part on women’s levels of fear of victimization. The regression models in Table 3 examine the role of fear as a moderator. We expected that extremely high or extremely low levels of fear of victimization may result in particularly detrimental mental health outcomes in the aftermath of rape victimization. In comparison, we anticipated that women with average or moderate levels of fear would have less deleterious mental health outcomes as a result. Looking first at PTSD, our prediction seems to hold for respondents victimized by forcible rape. In Models 1 through 3 of Table 3, forcible rape significantly predicts PTSD across all levels of fear. However, forcible rape has stronger relationships with PTSD for women with low levels of fear (b = 0.819) and for women with high levels of fear (b = 0.518) than for women with average levels of fear (b = 0.411). The equality of coefficients test (found in Table 4) indicates that forcible rape has a significantly stronger impact on PTSD for women with low levels of fear as compared with women with mid-range levels of fear.
OLS Models Predicting Mental Health Symptomology as Moderated by Levels of Fear of Victimization.
Note. The values represent b (SE). OLS = ordinary least squares; PTSD = post-traumatic stress disorder.
p ≤ .05. **p ≤ .01.
Equality of Coefficients Tests, PTSD Symptomology.
Note. PTSD = post-traumatic stress disorder.
p ≤ .10. **p ≤ .05. ***p ≤ .01.
Vicarious rape shows a similar pattern with PTSD. It has stronger relationships with PTSD for women with low levels of fear (b = 0.291) and for women with high levels of fear (b = 0.316) than for women with mid-range levels of fear (b = 0.196). However, the equality of coefficients tests in Table 4 indicate that these differences are not significant.
In addition to our predictions, a number of other significant moderation effects are of interest in the models predicting PTSD. First, being African American is more strongly related to PTSD for college women with low levels of fear (b = 0.337) as compared with average levels of fear (b = 0.035, Z = 1.667, p ≤ .10). Second, higher household income is significantly less predictive of PTSD for women with average fear (b = −0.046) as compared with high levels of fear (b = 0.010, Z = −1.667, p ≤ .10). In other words, for women with high levels of fear, higher income does not serve as a protection from PTSD symptoms. Third, a recent forcible rape is more highly related to PTSD for women with low levels of fear (b = 1.390) compared with women with average levels of fear (b = −0.002, Z = 2.122, p ≤ .05). Finally, being a non-traditional aged college student is more of a protective factor against PTSD among women with low levels of fear (b = −0.656) and women with average levels of fear (b = −0.267) compared with women with high levels of fear (b = 0.526). Both of these moderation effects are significant at a significance level of p ≤ .05. This suggests that being older protects against PTSD, but not for college women with high levels of fear.
Continuing to examine moderation effects, in Table 3, we compare the impact of forcible rape on depression symptomology across levels of fear of victimization and find that forcible rape has the strongest relationship with depression for women with low levels of fear (b = 0.661) as compared with women with mid-range levels of fear (b = 0.344) and for women with high levels of fear (b = 0.297). The equality of coefficients tests (found in Table 5) indicate that none of the differences in the impact of forcible rape on depression across levels of fear are significant. Vicarious rape does not show the predicted pattern in its relationship with depression, either. In contrast to our expectations, the strongest relationship between vicarious rape and depression is found for women with mid-range levels of fear of victimization (b = 0.188).
Equality of Coefficients Tests, Depression Symptomology.

p ≤ .05. **p ≤ .01. ***p ≤ .10.
In addition, a number of other significant moderation effects are of interest in the models predicting depression. Table 5 indicates that African Americans with low levels of fear are more likely to express symptoms of depression (b = 0.350) compared with African Americans with moderate levels of fear (b = 0.044, Z = 1.834, p ≤ .10). Second, and similar to PTSD, a recent forcible rape is more strongly related to depression for college women with low levels of fear (b = 1.284) when compared with college women with moderate levels of fear (b = 0.056, Z = 2.028). Third, being a non-traditional aged college student is more predictive of depression for high-fear women (b = 0.690) than women with medium (b = −0.165) and low levels of fear (b = −0.181). Both of these moderation effects are significant at a significance level of p ≤ .05. This suggests that being older is a detriment for college women with high levels of fear, but not for college women with medium or low levels of fear.
Discussion and Conclusion
This study focused on fear of victimization, rape, and negative mental health outcomes among women. There is little question that experiencing the trauma of rape or hearing about such an event firsthand can elicit negative reactions, such as fear and/or adverse mental health symptomology. Although fear of victimization is largely considered a negative consequence of prior victimization, it potentially has advantages as well (Hale, 1996; Warr, 2000). We suggest that moderate levels of fear of victimization are, in some sense, “healthy.” For instance, moderate levels of fear may lead to protective behaviors which can reduce the potential for future victimization, make individuals feel safer, and result in a higher quality of life (Gray et al., 2011; Jackson & Gray, 2009). In this way, healthy fear may empower victims by giving them the sense that they have (or are moving toward) regaining control over their life. Yet, “healthy” levels of fear have generally been ignored in prior studies. The current study sought to better understand women’s fear levels, as well as how their fear may mediate or moderate the impact of their rape experiences on symptoms of PTSD and depression. We believe we found three noteworthy results stemming from our research questions, and we discuss these below.
First, the results of our first research question confirm that fear of victimization is unequally distributed among certain groups of people (e.g., women with higher incomes, women who had experienced multiple rape victimizations) and that negative events (e.g., rape, PTSD, or depression) are strongly related to higher levels of fear among women. This is largely consistent with prior research (Ferraro, 1996; Wilcox et al., 2007). We found that women’s background characteristics (race, income) and prior experiences (prior victimization, experiencing multiple rape victimizations) were related to increased fear levels. Higher levels of depression and PTSD symptomology were found as fear levels increased; the same was true for forcible and vicarious rape experiences. Interestingly, a higher proportion of women reported all fear levels (low, average, high) in the wake of hearing about rape vicariously (33%, 41%, and 49%, respectively) as opposed to physically being raped (5%, 8%, and 14%, respectively). This may partially explain why prior studies have reported that actual rape and vicarious rape elicit very similar effects (e.g., Hale, 1996). Unsurprisingly, having been victimized multiple times was related to higher fear levels.
Our second research question addressed the impact of rape on fear and the mediating effect of fear on the relationship between rape and mental health symptomology. We found that forcible rape and vicarious rape were two of the strongest predictors of fear; however, we found little evidence that fear of victimization, in turn, mediated the effect of rape on negative mental health outcomes. While the explained variance increased in regression models when fear was included as a predictor of PTSD and depression, the substantive effect of forcible rape and vicarious rape changed very little compared with models where fear was not included. This may suggest that there is “something else” about rape—besides the fear it elicits—that more directly affects mental health outcomes among women. Some scholars have suggested that the amount of distress victims feel during the rape event, or the extent to which they fear for their lives during the attack, may be the critical mechanism at work (e.g., Girelli et al., 1986). Others have suggested that the behaviors and attitudes that victims engage in after their victimization (e.g., avoidance behaviors, withdrawal) can further increase their fear levels and subsequent mental health (Liska et al., 1988; Stafford et al., 2007). While this is a distinct possibility, our models did not suggest a strong mediating effect of fear (which included both behavioral and conceptual components)—“healthy” or not. Thus, we believe that other mechanisms bridge rape—both forcible and vicarious—with PTSD and depression. Perhaps it is not the risk factors that are missing from our analyses (we included most of the most relevant correlates of fear and mental health outcomes: for example, multiple rapes, recent event, substance abuse), but the protective factors, such as social support from others, treatment, and services that are offered to or engaged in by the victim in the aftermath of her trauma (Campbell et al., 2009). We hope that future research examines these prosocial and supportive measures as potential mediators of rape experiences.
Finally, although we expected that very high or very low levels of fear (vs. average levels) would be related to more detrimental mental health outcomes in the aftermath of rape victimization, we found little evidence that the effect of forcible rape or vicarious rape on either mental health outcome was moderated by fear. Forcible rape significantly predicted PTSD and depression regardless of fear levels, with only one exception. Looking first at PTSD, the regression coefficients fit the predicted pattern: each form of victimization exerted a weaker impact on negative mental health outcomes at average levels of fear and exerted higher impacts on negative mental health outcomes at both low and high levels of fear. However, only one moderation effect was found to be of moderate significance: The impact of forcible rape is slightly stronger for college women with low levels of fear compared with college women with average levels of fear (Z = 1.708, p ≤ .10). PTSD involves feelings of numbness; avoidance of people, places, or thoughts of victimization; reliving the event; and so forth; perhaps average or healthy fear levels promote appropriate avoidance behaviors, thus reducing the likelihood that memories become “triggered,” but low fear, in contrast, may increase the risk of “triggering” PTSD symptoms especially if women do not take adequate precautions against further victimization. For depression, the impact of forcible rape was also largest at the lowest levels of fear, but it was not significantly different across fear levels (as indicted by the equality of coefficients tests).
It is also possible that mental health outcomes of victims are due to something entirely separate from fear. Some women who experienced sexual assault not only had a low fear of victimization but also had mental health symptomology. This pattern might actually be an indication that the victim feels shame and is blaming themselves for the assault. These women may not feel fear of victimization after their assault, but by placing the blame on themselves instead of the perpetrator, coping with the victimization could be more difficult. Self-blame could be detrimental to the victim’s mental health especially when disclosing an assault may garner negative social reactions that do not support the victim (Ullman, 1996).
Victims often blame themselves after an assault, thinking they could have done more to prevent it from happening or even believing they provoked the assault. Research has connected this type of self-blame after a sexual assault to detrimental mental health outcomes. For example, Breitenbecher (2006) found that the blame college women placed on themselves after a sexual assault due to a character fault (i.e., I am a bad person, I deserved this) was a predictor of mental distress. Self-blame is also detrimental to coping with a sexual assault where victims may turn to avoidance behaviors, or other maladaptive coping strategies, which could also affect mental health (Littleton & Breitkopf, 2006; Najdowski & Ullman, 2009). In addition, self-blame after a sexual assault is also a risk factor for future victimizations (Katz, May, Sorensen, & DelTosta, 2010). As a factor intervening between victimization and mental health symptomology, blaming one’s self by definition lessens blame placed on the perpetrator and, consequently, might be most relevant for women with low fear levels.
The explanations we provide here are speculative, but our primary conclusion in regard to the relationship between forcible rape and mental health is that college women with the lowest levels of fear are most at risk for mental health symptoms as a result of victimization. As the majority of research on fear of victimization has focused on the negative impact of high fear, our understanding about the effects of low fear levels is limited. Our research suggests at least two avenues for future research: First, more research is needed that focuses on the impact of “low” fear levels on various outcomes, and second, low levels of fear likely should be considered distinct from “healthy” fear in future studies. It would also be beneficial to include measures of self-blame or maladaptive coping mechanisms after an assault to examine how they impact mental health outcomes independent of fear levels.
Vicarious rape significantly affected PTSD at all levels of fear (showing the predicted pattern), but affected depression only at average levels of fear. In other words, it appears that vicarious rape is more salient for PTSD—regardless of fear levels—than depression, and when it is related to depression, it is only among females with average fear levels. Thus, the vicarious rape and depression relationship is complicated somehow by fear levels, whereas the vicarious rape and PTSD relationship is not. We cannot account for these findings, but we noted a similar pattern for both household income and multiple rapes for both PTSD and depression. In each case, the variables exert significant effects for college women with average levels of fear of victimization, but are not significant in predicting mental health symptomology for college women professing low or high rates of fear. Additional research would be useful in deciphering why these factors only influence mental health symptomology for college women with moderate levels of fear of victimization.
Two other findings are of interest for future research. First, the recency of victimization increases both PTSD and depression, but only for college women with low levels of fear. We would have predicted that a recent event would have a significant impact on mental health symptoms for victims regardless of levels of fear of victimization. Perhaps having low levels of fear places women at increased risk of further victimization or exposes them to circumstances (e.g., drinking) which trigger mental health symptoms. Second, our research suggests that age is an important variable for research on fear of victimization focusing on college women, just as age is found to be an important factor for fear of victimization in more general samples where older women often have levels of fear that exceed their likelihood of victimization (Hale, 1996; Warr, 2000). In our research, being an older, female college student appears to be a protective factor for women with low levels of fear of victimization, but an aggravating factor for women with high levels of fear. We suggest that older college students are less likely to be in situations (e.g., bars, drinking and/or drug use, late-night partying) that may increase their risk of sexual victimization (Fisher et al., 1998) and they are cognizant of this reality. In other words, the routine activities of non-traditional college women result in less actual risk and less perceived risk, the overall result of which is less detrimental to mental health. Our findings, however, suggest that this potentially protective role is limited to women who do not have irrationally high levels of fear of victimization.
Our research has limitations that should be noted. First, given the nature of the sample, some variables suffer from a lack of variation. Forcible rape is rare, particularly among the group with low levels of fear. In addition, few of the women were never married, experienced multiple rapes, or experienced rape as a recent event. This lack of variation can reduce statistical power in models to detect significant main effects and moderation effects. Also, although we restrict the measurement of the dependent variables to the 6 months preceding the survey, we do not have true longitudinal data that would allow for stronger causal arguments founded on known ordering of cause and effect. However, because only about 3% of the sample experienced a recent rape, we can be confident in most circumstances that victimization preceded our measure of reports of mental health symptomology.
We began this research with the assumption that there are “healthy” levels of fear, as well as dangerous levels of fear. College women with too little fear may fail to take necessary precautions against sexual victimization, whereas women with too much fear might overly restrict their behaviors and routine activities. Overall, our findings suggest that too little fear is indeed a moderating factor that exacerbates the relationship between victimization and mental health symptomology: Forcible rape in particular has a higher impact on PTSD among women with low levels of fear compared with women with average levels of fear. Yet, we found no moderation effects of fear for either forcible or vicarious rape on depression outcomes, and the effect of vicarious rape on PTSD was significant regardless of women’s levels of fear. We did find, however, that fear levels moderated the effects for some background (e.g., race, household income, age) and victimization history (e.g., recency of rape) variables on both mental health outcomes. Our results suggest that more research is needed that focuses on various levels of fear—not just high fear—and that the identification of “healthy” fear of victimization is a theoretical endeavor that deserves additional research both with college women and women more generally.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.