
Abstract
Being able to perceive the risk of further violence can be an essential step toward seeking help, leaving the abuser, and eventually reducing the risk of revictimization. The current study looks at the individual and contextual risk factors related to perception of risk and, subsequently, their influence on the decision of 83 battered women to leave the abusive partner after 1 year as well as on revictimization. Results indicated that perceiving more risk is a predictive factor in the decision to leave the partner. A dangerous side of gratitude emerged about future revictimization. Results are discussed for clinical implications.
Introduction
According to the World Health Organization (WHO), it is estimated that one in two women worldwide experience physical or sexual violence in their lifetime, and one in four women report some form of intimate partner violence (IPV; WHO, 2014). The effects of IPV are long-lasting and even life-threatening, and include economic costs and mental health issues such as depression and post-traumatic stress disorder (Baldry et al., 2017; Bonomi et al., 2006; Campbell, 2002; Cohen et al., 2007; Coker et al., 2002; Watkins et al., 2014). Revictimization, here defined as recurrent abuse from the same partner toward the same survivor, is a feature of IPV (Halpern et al., 2009; Renzetti et al., 2017; Walker, 1979). To prevent revictimization, intervention by the criminal justice system, as well as other intervention and protective actions are needed, but they do not necessarily eliminate such risk (Capaldi & Langhinrichsen-Rohling, 2012; Maxwell et al., 2001). Most IPV survivors face the decision of whether to terminate the abusive relationship to prevent being revictimized. Leaving or staying with an abusive partner has different implications and costs associated with each choice; making this decision is difficult and even dangerous (Choice & Lamke, 1997). In other fields, such as medicine, risk perception is essential to inform decision as to which actions to take to change potential risk-related behaviors and to avoid possible adverse future outcomes (Brewer et al., 2004). The same approach can be applied in IPV cases, with survivors needing to perceive the risk to take actions that could help reduce future revictimization. In the current study, we tested a risk prediction model and assessed its effect on decisions aiming at reducing revictimization such as leaving the partner (Brewer et al., 2004; Dichter & Gelles, 2012; Heckert & Gondolf, 2004). An additional goal was to detect which individual and contextual risk factors are likely to increase survivors’ risk perception ability.
Risk Perception in Survivors of IPV
A risk is a “statistical odds of danger; the chance or probability that an event will occur” (Hilton & Harris, 2005, p. 18). According to Harding and Helweg-Larsen (2009), when referring to IPV, the term “risk assessment” is the most frequently used. In other fields, such as health and medicine, the term “risk perception” is preferred. These two terms address the same fundamental concept indicating a subjective feeling of being at risk for an event to occur, and they could be used interchangeably (Harding and Helweg-Larsen, 2009). However, in our opinion, in human behavior, where future adverse outcomes are partially related to individual conditions or decisions, the two terms do not imply the same theoretical explanation: assessing risk does not imply perceiving risk (Baldry & Sebire, 2016). According to the behavior motivation hypothesis (for a review and meta-analysis, see Brewer et al., 2004, 2007), risk perception is one’s ability to link risks and understand how they could lead to revictimization. The theory suggests that a high perception of risk for a negative event will lead to adoption of or change in behavior to reduce the risk (Brewer et al., 2004). But how this perceived risk involves the implementation of a protective behavior is unclear. IPV survivors first need to perceive the risk. Risk assessment, instead, can be defined as “the process of identifying risk and protective factors” (Hart, 2008, p. 7), and it is used by professionals (e.g., police, social workers, judges), who may miss or overlook the dynamic and individual factors that influence survivors’ capacity or willingness to perceive themselves as at risk for revictimization.
Survivors’ risk perception, rather than risk assessment, is a useful model to understand survivors’ intended or future behavior to leave the violent partner and hopefully reduce revictimization. Risk perception is an individual ability, influenced by individual and interpersonal and contextual factors (Cattaneo et al., 2007). It is essential to identify which risk factors are best able to influence risk perception to understand what will motivate someone at risk to ultimately decide to leave the abusive partner. To reduce the risk of revictimization, survivors should be given the resources and support needed to increase risk perception and ultimately end a violent relationship. Risk factors influencing risk perception can be individual, interpersonal, or contextual according to the ecological framework explained by Cattaneo et al. (2007) drawing from the work by Bronfenbrenner (1977, 1986) and Heise (1998). In a study on risk perception, Harding and Helweg-Larsen (2009) interviewed 56 IPV survivors, looking at different risk factors associated with risk perception and decisions to leave the abusive partner. They found that sexual coercion was associated with risk perception, whereas physical assault, psychological abuse, and injury were not. Contact with the police and leaving the abusive partner were both associated with increased risk perception only when the relationship continued, but not when the decision was taken to end it. The authors also found that risk reduction was associated with the intent to end the relationship.
Dichter and Gelles (2012), in their correlational study with 164 women in a hospital emergency department and community-based organizations, did not investigate individual risk factors, such as personality or other psychological dimensions, but rather focused on relationship type and cohabitation status. Interpersonal risk factors, such as previous sexual violence and lethality threats, and contextual risk factors, such as police intervention and social support, were analyzed against risk perception (feeling safe and risk of revictimization). Results showed that survivors’ risk perception was associated with past lethality threats and sexual violence, but not with individual risk factors nor with police arresting perpetrators. Higher levels of social support were positively associated with lower risk perception.
Other factors related to risk perception were investigated by Chu (1992) and Kluft (1990), who theorized that dissociative and numbing symptoms reduce women’s ability to perceive danger, and thus, increase risk of revictimization among women with these symptoms. But others (Helweg-Larsen et al., 2008; Helweg-Larsen & Shepperd, 2001) report that depression, as well as negative mood and anxiety, may enhance risk perception in dating violence survivors who have a generally pessimistic attitude and tend to see the risk as higher. These contradictory findings may be due to the role played by psychological distress, which could mediate the relationship between the risk factors and the capacity to respond to a threatening situation such as IPV (Gidycz et al., 2006).
At the interpersonal level, Helweg-Larsen and Shepperd (2001) identified prior experiences of abuse as being associated with risk perception. Brown et al. (2005) also found that previous experience of sexual victimization is related to a higher perceived risk of future sexual victimization. Similarly, in a study on dating violence among college students, Helweg-Larsen et al., (2008) reported that those students who had previously experienced dating violence reported higher levels of risk perception of future violence than those who had not. Therefore, factors such as longer relationship duration and/or a longer and more severe history of abuse in the relationship (Cattaneo et al., 2007) should lead to increased accuracy. Lack of informal support (by friends, relatives or colleagues) also plays a role in both risk perception and the decision to leave the abusive partner. Isolation as a mechanism of IPV makes the victim increasingly dependent on the perpetrator, both for basic physical needs and for information and emotional sustenance (Herman, 1992). At the contextual level, Cattaneo et al. (2007) found that seeking formal support from the police and social services predicts survivors’ risk perception, but not future revictimization (for review see Cattaneo & Goodman, 2005).
What needs to be determined is the causal relationship between survivors’ risk perception and subsequent decisions to leave abusive partners. Sonis and Langer (2008) found that survivors who had left their abusive partner were at decreased risk of future violence, whereas Robinson and Tregidga (2007) found that terminating the relationship was associated with an increased risk of revictimization. As a matter of fact, leaving the relationship could be dangerous because it may precipitate further violence by abusive partners who wish to maintain control over victims. Some authors suggest that, in some cases, the point of greatest risk of violence is when victims decide to leave their partner (Fleury et al., 2000); assaults may increase in severity following this decision (Anderson & Saunders, 2003). In addition, according to a review by Vezina and Hebert (2007), women who stay in a romantic relationship in which they are victimized are more likely to report stronger feelings for their partner, hold more traditional attitudes about gender roles, and offer more justification for their partners’ violence compared with women who leave violent relationships. Individual risk factors may play a role in the development of positive feelings of survivors toward their abusive partners (Gordon et al., 2004). One of these positive feelings is gratitude toward the partner, which has scarcely been investigated in this field.
Gratitude
Within the field of gratitude research, there is a lack of agreement about the nature of the gratitude (Wood et al., 2010). Several researchers have conceptualized gratitude as an emotion (Wood et al., 2008) directed toward appreciating the helpful actions of other people, or as part of a wider life orientation toward noticing and appreciating the positive in the world (Geraghty et al., 2010). In recent years, a large body of evidence has emerged suggesting that gratitude is strongly related to all aspects of wellbeing. Wood et al. (2016) conclude that “low gratitude is strongly, uniquely, and possibly causally related to clinically impaired functioning and impaired clinically relevant processes” (p. 137). Nevertheless, concerns have been raised about a potential dark side of gratitude; gratitude could be harmful, as when a victim feels gratitude toward her abusive partner, regardless of what he has done, which “might motivate her to remain in the relationship and continue to tolerate the abuser” (Wood et al., 2016, p. 144; see also Carr, 2016). In certain circumstances, the abuser may also foster ingratiation in the victim in several ways with this express intent. For instance, the abuser may encourage false dependence by the victim (e.g., “you could not survive without me”; Wood et al., 2016, p.144). This variable, however, has not been taken into account in previous studies of IPV; consequently, the evidence base is not yet sufficient to assess the negative effect of gratitude in relationships.
The current study, therefore, focused on the relationship of individual and contextual risk factors, including risk perception and the decision to leave the abusive partner, to the risk of physical and psychological revictimization. The study also investigated the influence of other individual/personality or psychological factors on survivors’ risk perception and decision to leave the abusive partner, including feelings of gratitude toward the (ex)partner.
Research Questions
The current study addressed the following research questions:
Method
Procedure and Participants
The study was reviewed and approved by the Ethical Commission of the Department of Psychology, Università degli Studi della Campania “Luigi Vanvitelli.” We conducted face-to-face interviews at T1 and phone interviews at T2. Due to the personal contact of the first author with the National Network of Women’s Shelters in Italy, we were able to invite participation by IPV survivors in seven shelters located in three different cities in Italy (Caserta, Rome, and Milan), to ensure better national representativeness. These cities are located in south, central, and north Italy, respectively, and have differing populations and cultural characteristics. Milan is more urban and vanguard than Caserta, whereas Rome, the country’s capital, represent a mix of the vanguard, tradition, and opportunity. Survivors who sought help at the emergency room (ER) of one of the main hospitals in Milan, which has an ER specialized in dealing with female victims of physical and sexual violence, were also recruited to participate in the study.
We explained the purpose of the study and the study procedures to all potential participants (all women) via a leaflet and directly on site at the shelters and the ER. Women who agreed to participate signed a consent form allowing the use of data for research purposes only and permitting us to contact them a year after the first interview for follow-up. We told the women that the study had no clinical or counseling purposes, and we reassured them that we had no role in any decision they would take (e.g., report to the police, leave the partner), but that we could provide them with further referrals if required or needed. We expected this to enhance participant retention in the study, especially in light of the 12-month gap between the initial interview and the follow-up and also because no financial incentive for participation was offered.
Of the original 319 women survivors who participated at T1, 83 (26%) participated at T2. Their mean age was 42.21 years (SD = 9.58). Attrition analysis with the drop-out sample showed significant differences with regard to gratitude toward the partner, F(1, 316) = 4.86, p = .028, partial η2 = .02 (drop-out sample M = 2.13, SD = 1.17; final sample M = 1.80, SD = 1.11). Significant differences also emerged with regard to risk perception, F(1, 316) = 3.91, p = .049, partial η2 = .01 (the drop-out sample M = 3.61, SD = 1.17, the final sample M = 3.31, SD = 1.20). No significant differences were found with regard to level of depression symptoms, psychological and physical victimization, length of the relationship, and employment status at T1 between completers and those who dropped out of the study after the first interview.
All T1 interviews were conducted in a quiet room. T2 phone interviews were pre-arranged a few days in advance, to schedule the best time and day during which each woman would feel comfortable speaking on the phone about sensitive issues regarding their relationship. All interviews were conducted by one of the authors and a trained and debriefed research assistant. The average T1 length was 40–45 min; average length of T2 interviews was 20–30 min.
Measures
All variables were included in a structured questionnaire, slightly different for some measures of the two versions, T1 and T2.
Demographic information (T1)
Participating women provided information about their age, nationality, place of residence, employment status, education, presence of children, and type of relationship with the abusive partner, whether they ever previously left the partner, whether they had reported the violence to the police/authorities, whether they lived with the batterer at the time they contacted the shelter or accessed the ER, and length of relationship.
Risk perception (T1)
Participating women were asked to rate their perception of risk that their partner would be violent toward them in the future, by answering the following questions: (a) For risk perception of psychological violence, “What do you think the chances are that you will be threatened, verbally insulted by your partner in the next 6 months?” (b) For risk perception of physical violence, “What do you think the chances are that you will be pushed, shoved, or hit or kicked by your partner in the next 6 months?” and (c) To measure risk perception of future lethal violence, “What do you think the chances are that you will be attacked by your partner to a deadly point in the next 6 months?” To all questions, participating women answered on a 5-point Likert-type scale ranging from 1 (not at all likely) to 5 (very likely). All scores were added together to form the risk perception score (α = .76).
Gratitude toward the partner (T1)
Three items from the original Gratitude Questionnaire (GQ-6; McCullough et al., 2002) adapted to measure gratitude toward the intimate partner were used: “I have so much to be thankful for with my partner,” “Regardless of what has happened, I am grateful to my partner because the relationship with him made me grow as a person,” and “There are more things for which I am grateful to my partner than negative ones.” Answers provided on a 6-point Likert-type scale ranged from 1 (strongly disagree) to 6 (strongly agree) and were added together to obtain the partner gratitude score (α = .72).
Depression Scale (T1 and T2)
The CES-D (Radloff, 1977) 20-item self-report scale was used to measure current level of depression symptoms. For each item, participating women could rate from 0 (“not at all or less than only once”) to 3 (“5–7 days” or “nearly every day over a 2-week period”) whether they experienced any of the symptoms listed. Total scores were added together, ranging from 0 to 60, with a cut-off score of 16 for the total CESD-scale for clinical significance (α = .93 at T1, α = .94 at T2).
Informal and formal support (T1)
Informal and formal support was assessed by asking participating women three questions, with a “yes” or “no” answer: whether they received help and support from their family (parents and/or relatives), whether they got in touch with a shelter, and whether they had reported the abuse to the police.
IPV (T1 and T2)
IPV was measured with the Revised Conflict Tactics Scales (CTS2) for physical and psychological violence consisting of 20 items (Straus et al., 1996). Eight items measured psychological violence and 12 measured physical violence. The full list of items is provided in Table 2 with results from T1 and T2. Per the scale developers’ instructions, for each item, answers were provided on a 7-point Likert-type scale ranging from 0 = never, 1 = once in the past year, 2 = twice in the past year, 3 = 3–5 times in the past year, 4 = 6 or more times in the past year, 5 = 11–20 times in the past year, 6 = more than 20 times in the past year, and an additional last point 7 = not in last year but it did happen before. Scores from the two subscales were added together for physical violence (α = .87 at T1; α = .84 at T2), and for psychological violence (α = .69 at T1; α = .61 at T2).
Leaving decision (T2)
During the T2 interview, participating women answered “yes” = 1, or “no” = 0 with regard to whether they had by then left the partner referred to at T1.
Data Analysis
To address our research questions, we performed univariate and multivariate analyses using SPSS 20.0. First, we conducted descriptive, independent and paired samples t-tests to explore changes of prevalence of physical and psychological violence between T1 and T2. We then performed hierarchical regression analysis to determine the relationship between relevant contextual, interpersonal and individual/psychological risk factors and risk perception at T1, and subsequently, binary logistic regression to predict odds of having left the abusive partner and psychological and physical revictimization after 12 months, based on risk factors at T1.
Results
Sample Description
In more than half of the cases (59%), participating women were employed in full- or part-time work at T1, 79.5% of them reported that they had formal support by a shelter, and 45.8% reported that they had informal support from relatives (see Table 1).
Demographic description of the participants (N = 83).
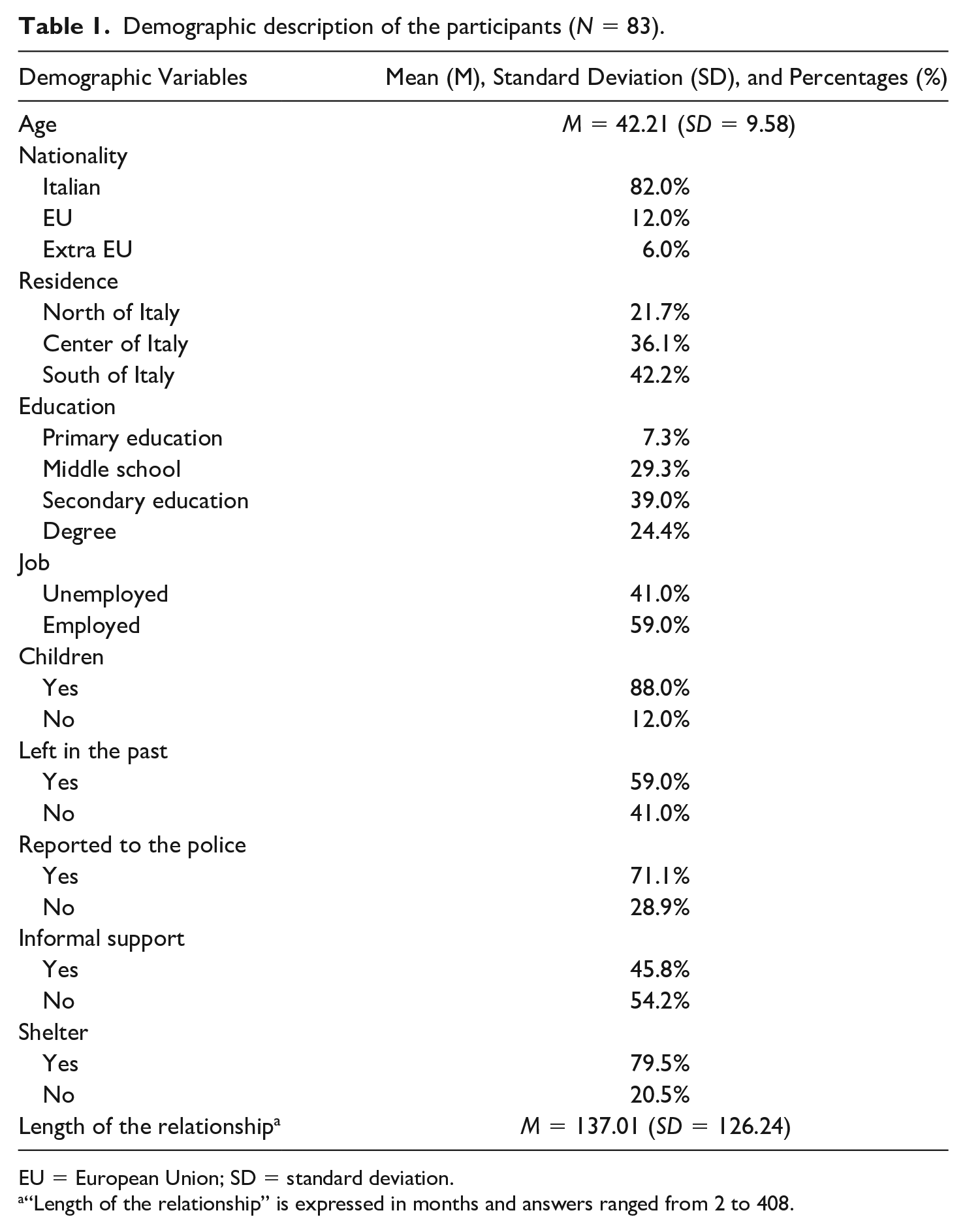
EU = European Union; SD = standard deviation.
“Length of the relationship” is expressed in months and answers ranged from 2 to 408.
The 83 participating women, being a clinical sample, all reported a significant degree of different forms of physical and psychological violence that had taken place during the year prior to the T1 interview (see Table 2). In most cases (71.1%), the participating women had reported to the police; in 59% of all cases, they had left the abusive partner in the past, but had returned to him; and 89.4% had at least one child under 18 years old. After 12 months, T2, 86.7% reported having left the abusive partner; 19.3% reported having been physically revictimized; and 44.6% having been psychologically victimized between T1 and T2. These last two differences are both significant: for a total score of psychological violence, T1 (M = 3.47, SD = 1.51), and T2 (M = 0.86, SD = 1.37), t(82) = 11.59, p < .001; and a total score of physical violence, T1 (M = 2.03, SD = 1.59) and T2 (M = 0.26, SD = 0.88), t(82) = 8.87, p < .001. Furthermore, significant reductions were also found for depression symptoms, T1 (M = 25.41, SD = 13.62) and T2 (M = 19.45, SD = 13.63), t(82) = 3.82, p < .001.
Women Experiencing IPV in the Previous 12 Months at (T1) and (T2) (N = 83).
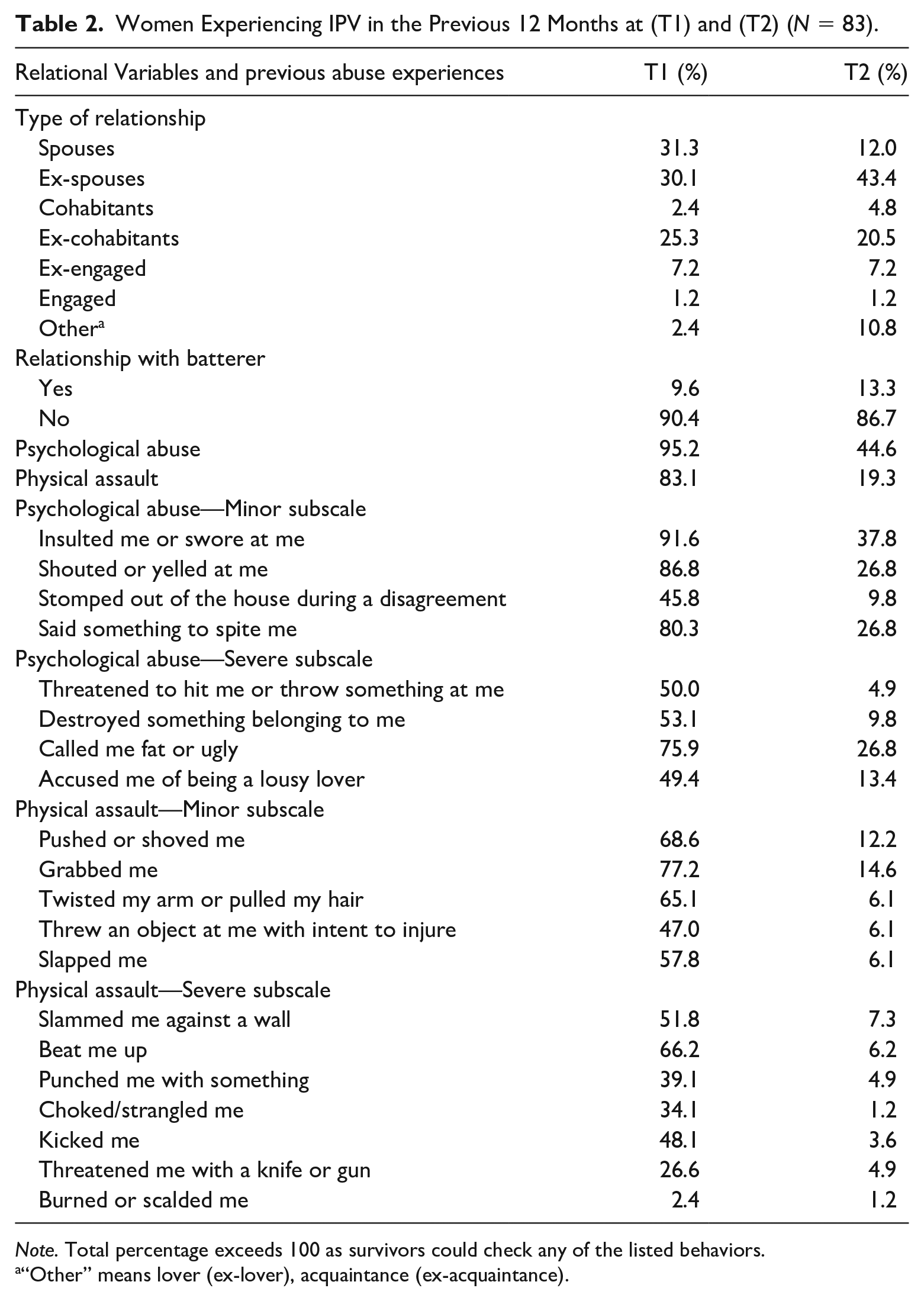
Note. Total percentage exceeds 100 as survivors could check any of the listed behaviors.
“Other” means lover (ex-lover), acquaintance (ex-acquaintance).
Independent t-test sample comparisons were performed on risk perception at T1 between survivors who had left their abusive partner on a previous occasion (M = 3.22, SD = 1.23) and those who had not (M = 3.44, SD = 1.16), with no significant difference, t(81) = 0.81, p = .42. No significant differences, t(81) = −0.86, p = .39, on risk perception at T1 were found between survivors who had a job (M = 3.41, SD = 1.18) and those who did not (M = 3.18, SD = 1.23). No significant differences, t(81) = −0.98, p = .33, on risk perception at T1 were found between survivors who had reported to the police (M = 3.40, SD = 1.20) and those who had not (M = 3.11, SD = 1.20). No significant differences, t(81) = −0.81, p = .42, on risk perception at T1 were found between survivors who had reported having had informal support by parents, friends, or relatives (M = 3.43, SD = 1.24) and those who had not (M = 3.21, SD = 1.17). Significant differences, t(81) = −2.32, p = .02, were instead found between survivors who had asked for formal support from a service (e.g., a shelter; M = 3.46, SD = 1.18) and those who had not (M = 2.73, SD = 1.14).
Hierarchical Regression
To answer the first research question, hierarchical regression analysis was conducted to explain the relationship between different risk factors and risk perception at T1 (see Table 3). For risk perception, survivor’s job, contacts with police, and shelter support were entered in the first step of the analysis with shelter’s support being statistically significant (β = .266, p < .05). In the second step of the analysis, the two subscales for psychological and physical IPV were entered into the model, together with length of relationship, previous separation from the partner, and informal support. No significant increase emerged. In the last step of the analysis, individual variables were entered into the model, significantly increasing the total variance of risk perception, ΔR2 = .092, F(2, 72) = 4.38, p < .05, with survivor’s job (β = .237, p < .05) and depressive symptoms (β = .284, p = .01) being statistically significant. The full model explained 24% of the total variance of risk perception, F(10, 72) = 2.28, p < .05. In other words, individual variables, such as survivor’s job and depressive symptoms are the predictors that better explain an increase in risk perception.
Hierarchical Regression Model on Risk Perception in IPV Survivors.

Note. N = 83. For survivor’s employment, answers ranged from 0 = “no” to 1 = “yes”; for contacts with police, answers ranged from 0 = “no” to 1 = “yes”; for shelter support, answers ranged from 0 = “no” to 1 = “yes”; for psychological and physical violence, answers ranged from 0 = “low levels of chronicity of violence” to 6 = “high levels of chronicity of violence”; length of the relationship is expressed in months and answers ranged from 2 to 408; for left the partner in the past, answers ranged from 0 = “no” to 1 = “yes”; for informal support, answers ranged from 0 = “no” to 1 = “yes”; for depression, answers ranged from 0 = “low levels of depressive symptoms” to 60 = “high levels of depressive symptoms”; for partner gratitude, answers ranged from 1 = “low levels of gratitude toward partner” to 6 = “high levels of gratitude toward partner.”
p < .10. *p < .05.
Multiple Logistic Regression
To predict the decision whether or not to leave the abusive partner after 12 months, a logistic regression was performed using the same predictive risk factors measured at T1 at the contextual, interpersonal, and individual levels to answer our second research question (see Table 4). The full model significantly predicted the decision to leave the abusive partner (omnibus χ2(11) = 23.01, p < .05). The model accounted for between 24% and 45% of the total variance, with 97.2% of the women who left the abusive partner predicted successfully.
Logistic Regression and Odds Ratios Predicting Decision to Leave the Abusive Partner After 12 Months (T2) and Risk Factors at T1 (N = 83).
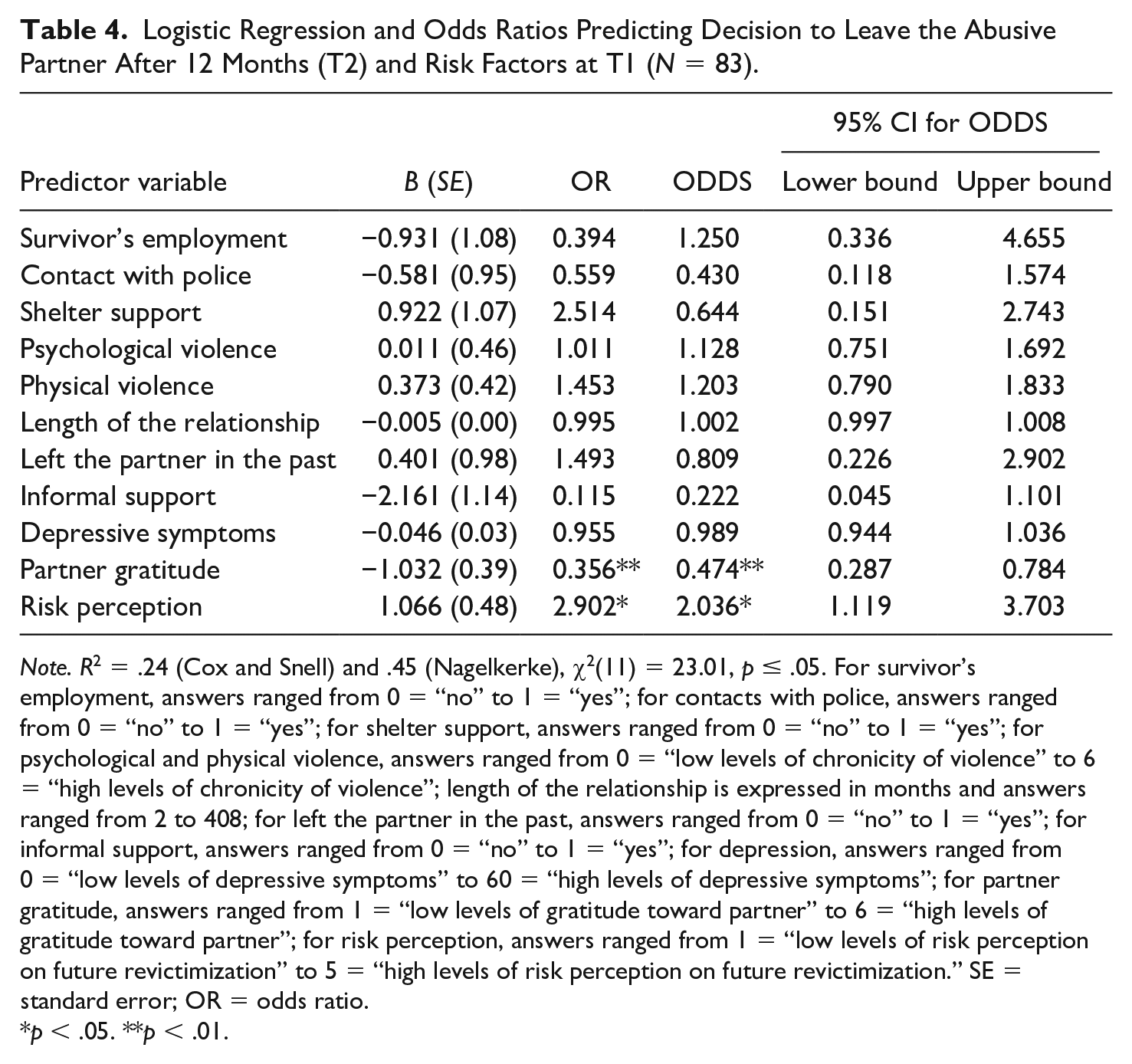
Note. R2 = .24 (Cox and Snell) and .45 (Nagelkerke), χ2(11) = 23.01, p ≤ .05. For survivor’s employment, answers ranged from 0 = “no” to 1 = “yes”; for contacts with police, answers ranged from 0 = “no” to 1 = “yes”; for shelter support, answers ranged from 0 = “no” to 1 = “yes”; for psychological and physical violence, answers ranged from 0 = “low levels of chronicity of violence” to 6 = “high levels of chronicity of violence”; length of the relationship is expressed in months and answers ranged from 2 to 408; for left the partner in the past, answers ranged from 0 = “no” to 1 = “yes”; for informal support, answers ranged from 0 = “no” to 1 = “yes”; for depression, answers ranged from 0 = “low levels of depressive symptoms” to 60 = “high levels of depressive symptoms”; for partner gratitude, answers ranged from 1 = “low levels of gratitude toward partner” to 6 = “high levels of gratitude toward partner”; for risk perception, answers ranged from 1 = “low levels of risk perception on future revictimization” to 5 = “high levels of risk perception on future revictimization.” SE = standard error; OR = odds ratio.
p < .05. **p < .01.
The values of the coefficients reveal that an increase of a unit of gratitude toward the partner decreases by half the odds of deciding to leave the abusive partner (ODD = 0.474, 95% confidence interval [CI] = [0.287, 0.784]), and that each unit increase in the risk perception score is associated with a double increase in the odds of deciding to leave the abusive partner (ODD = 2.036, 95% CI = [1.119, 3.703]). In other words, two individual factors, risk perception and gratitude toward the (ex)partner, predicted the decision to stay or leave the partner after 12 months. In particular, a high level of risk perception of revictimization affects the likelihood of not staying with the abusive partner. In contrast, gratitude acts as a risk factor, as an increase of feeling gratitude increases the likelihood of staying with the batterer after 12 months.
To predict psychological and physical revictimization after 12 months, our third research question, additional logistic regression analyses were performed using the same predictive risk factors measured at T1 at the contextual, interpersonal, and individual levels (see Table 5). For psychological violence (T2) the model did not predict revictimization after 12 months. For physical violence (T2), the full model significantly predicted revictimization after 12 months (omnibus χ2(11) = 27.65, p < .01). The model accounted for between 28% and 45% of the total variance, with 37.5% accurate predictions for the revictimized survivors group. The values of the coefficients reveal that an increase of a unit of depressive symptoms increases by one the odds of physical revictimization (ODD = 1.06, 95% CI = [1.01, 1.11]), and that each unit increase in the score of gratitude toward the partner is associated with a double increase in the odds of physical revictimization (ODD = 2.12, 95% CI = [1.31, 3.40]). Regarding psychological and physical revictimization, the data revealed that no variables predicted psychological violence after 12 months, while for the physical violence, victim’s depressive symptoms and gratitude toward the (ex)partner increase the likelihood of physical violence revictimization after 12 months.
Logistic Regression and Odds Ratios Predicting Psychological and Physical Revictimization After 12 Months (T2) and Risk Factors at T1.

Note. N = 83. For psychological violence, R2 = .19 (Cox and Snell) and .25 (Nagelkerke), χ2(11) = 17.04, p = .11; for physical violence, R2 = .28 (Cox and Snell) and .45 (Nagelkerke), χ2(11) = 27.65, p < .01. For survivor’s employment, answers ranged from 0 = “no” to 1 = “yes”; for contacts with police, answers ranged from 0 = “no” to 1 = “yes”; for shelter support, answers ranged from 0 = “no” to 1 = “yes”; for psychological and physical violence, answers ranged from 0 = “low levels of chronicity of violence” to 6 = “high levels of chronicity of violence”; length of the relationship is expressed in months and answers ranged from 2 to 408; for left the partner in the past, answers ranged from 0 = “no” to 1 = “yes”; for informal support, answers ranged from 0 = “no” to 1 = “yes”; for depression, answers ranged from 0 = “low levels of depressive symptoms” to 60 = “high levels of depressive symptoms”; for partner gratitude, answers ranged from 1 = “low levels of gratitude toward partner” to 6 = “high levels of gratitude toward partner”; for risk perception, answers ranged from 1 = “low levels of risk perception on future revictimization” to 5 = “high levels of risk perception on future revictimization.” SE = standard error; OR = odds ratio; CI = confidence interval.
p < .05. **p < .01. ***p = .001.
Discussion
This study focused on three primary research objectives. First, we wanted to address which individual and contextual risk factors are likely to affect the risk perception of women survivors of IPV. In accordance with Cattaneo et al. (2007), we used an ecological approach to examine the extent to which personal factors, such as a victim’s mental health at the time of the assessment (depression), prior experiences of abuse, victim’s employment, length of the relationship, and previous separations, and relational factors, such as informal support at the interpersonal level and formal support (shelter and police) at the system level are likely to predict the accuracy of a victim’s risk perception. At the individual level, the results of this study revealed that, in line with previous research (Helweg-Larsen et al., 2008), depressive symptoms were associated with greater personal risk perception, while, in line with other studies (e.g., Harding & Helweg-Larsen, 2009; Helweg-Larsen & Shepperd, 2001), psychological and physical abuse were not associated with individual risk perception. Being able to perceive and assess the risk of revictimization accurately is one of the possible steps toward hopefully ending violence by also terminating the violent relationship. In the year before the first interview, 9 out of 10 and 8 out of 10 women reported at least one form of psychological or physical abuse, respectively. After 1 year, when we went back to interview them, the proportion dropped significantly: just over 4 out of 10 for psychological abuse and 2 out of 10 for physical abuse. Several factors might have contributed to this change. Most important is that all these women had already made contact with either a shelter or the dedicated ER, which also has a dedicated support service for women victims of IPV. This is a positive and encouraging result.
We went a step further and looked at contextual as well as individual risk factors and women’s capacity to perceive their risk. Among the factors taken into account, some did not seem to affect risk perception; these include having a job and, surprisingly, feeling depressed. The measure used for “depression” was not a clinical tool, but rather a set of indicators associated with feeling depressed. It could be that women feeling down and demotivated have negative feelings toward the future and the abusive partner, and perceive everything negatively, including the risks of what could happen to them. We examined the effects of risk perception and other contextual and individual/psychological risk factors, such as gratitude, in 83 women IPV survivors on the decision to leave or remain in their abusive relationship and being physically and psychologically revictimized after 1 year from the first contact. Looking at the longitudinal results, many contextual and individual/psychological risk factors seem to play no significant role, but the few that significantly predicted decisions to leave or stay increased by two-fold the likelihood that women would decide to leave their abusive partner within the year. These results are in the same direction as those reported by Heim et al. (2018), even though these authors used a shorter time span for their follow-up and examined different factors.
An interesting result that is especially relevant for its clinical and psycho-social implications is the role played by gratitude. Gratitude here was measured not as a general trait but rather as gratitude toward the (abusive) partner. We know that gratitude has a positive influence on the wellbeing of victims of intimate partner stalking (Baldry et al., 2016), and low gratitude impairs relevant psychological processes (Wood et al., 2010). But similar to Wood et al. (2016) and Carr (2016) who asked whether gratitude could also be harmful, we found that those women who were grateful to their partner, regardless of the fact that he had been abusive, were up to four times more likely to be psychologically abused and two times more likely to be physically abused. This is evidence of what we call the dangerous side of gratitude.
Limitations
This study has some limitations that should be addressed in future studies. The most important are the relatively small sample size, the significant attrition rate, and the limited number of women interviewed at T2 who had then left their partner. Caution should be used, therefore, for generalizing these results. Longitudinal studies with larger samples are needed. Samples are also needed that include women who have experienced less severe and lower prevalence of many forms of violence.
Practical Implications
This study has important practical implications in that it adopts an ecological explanatory mode to examine what affects women’s decisions to leave or stay with an abusive partner and run the risk of revictimization. Individual factors involved in these decisions include risk perception and gratitude. Intervention programs and counseling services should work to increase women’s ability to perceive risk and take actions beyond gratitude, identifying and discussing risk with clients who access services. Feeling grateful toward an abusive partner is not dangerous per se; it is possible that these women have had various positive experiences with their abusive partners, such as having children, which elicit positive and rewarding emotions. Feelings of gratitude become risky when they interfere with perceiving other, negative aspects, leading women, for example, to forget the abusive behavior, forgive the abusive partner, and continue to live with someone who is dangerous.
Footnotes
Acknowledgements
The authors thank the shelters and the hospital for their support and for their assistance in the data collection and all the survivors who participated in the study. Vincenza Cinquegrana thanks Prof. Anna Costanza Baldry for her continuous support, encouragement, and guidance on this project and in her development as a young professional. Her untimely death has left an unbridgeable gap in all of us.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.