
Abstract
Identifying rape myths among criminal justice and medical professionals is central to preventing secondary victimization. We present the first preliminary Danish validation of McMahon and Farmer’s updated Illinois Rape Myth Acceptance scale using samples of police and medical trainees. Exploratory and confirmatory factor analyses result in a 14-item, four-factor measure that demonstrates acceptable model fit, satisfactory convergent and discriminant validity, and good internal consistency. Although reported rape myth acceptance is generally low in both samples, some subscale scores vary across professional groups, thereby identifying specific targets for intervention in different occupational contexts. Further tests of the scale are recommended.
Introduction
In recent years, there has been increasing attention to the public and professional treatment of rape victims. Exemplified by the #MeToo movement, there have been widespread calls in many countries to identify and break down potentially damaging social myths that may discourage victims from reporting sexual assault and/or contribute to secondary victimization by the medical and criminal justice systems when they do (Campbell et al., 2001). Similar patterns have been observed in Denmark which has recently struggled with claims of supporting a “rape culture” (Amnesty International, 2019). Massive underreporting of sexual assault, paired with figures showing that nearly half of Danish rape complainants are unsatisfied with the police's handling of their case (Mannov, 2020; Pedersen et al., 2020; Rigspolitiet, 2020), further underlines the importance of this issue. This has led to a number of political initiatives aimed at ensuring that rape survivors are met in the best possible way and calling for better training of professionals in contact with sexual assault victims (Justitsministeriet, 2016). Implicit in these discussions is the suggestion that rape myths, defined as stereotypical beliefs about the circumstances, victims, and perpetrators of rape (Bohner et al., 2009; Burt, 1980), may play a role. Yet, little is actually known about Danish rape myth acceptance (RMA), as only very few examinations have been conducted to date. The ability to systematically measure stereotypical attitudes toward rape, particularly among professional groups likely to have contact with rape victims, is paramount to informing public debate and to evaluating the success of interventions aimed at improving rape victims’ experiences with the system. However, modern validated measures for doing so are lacking in the Danish context. With a view to providing such a measure and contributing to the growing literature exploring the validity and sensitivity of rape myth measurements in different cultural, professional, and linguistic contexts (Bendixen & Kennair, 2017; Fakunmoju et al., 2018; Trottier et al., 2020; Xue et al., 2016), we carry out a preliminary Danish validation of the updated Illinois Rape Myth Acceptance (IRMA) scale (Lonsway & Fitzgerald, 1994; McMahon & Farmer, 2011) using two groups of professional trainees (police and medical students) who may play an important role in future efforts aimed at diminishing risks of secondary victimization. In doing so, we also construct the first Danish profile and comparison of RMA in these groups, establishing an important empirical starting point for initiatives aimed at decreasing professional RMA.
Conceptualizing Rape Myths
Academic interest in identifying and combatting stereotypical attitudes toward rape dates back to the mid-1970’s, when a number of scholars began pointing to widespread views blaming survivors for their own victimization and exonerating rape perpetrators for their actions (Brownmiller, 1975; Schwendinger & Schwendinger, 1974). In 1980, the first formal definition of such beliefs was coined, defining rape myths as “prejudicial, stereotyped, or false beliefs about rape, rape victims, and rapists” (Burt, 1980, p. 217). In the decades since, various modified and refined conceptualizations have been proposed, most of which focus on sexual assault committed by men against women (Gerger et al., 2007; Lonsway & Fitzgerald, 1994). Although there is no universal agreement as to the ideal wording or scope of rape myth definitions, there is today general consensus that the concept encompasses a wide range of “descriptive or prescriptive beliefs about rape (i.e. about its causes, context, consequences, perpetrators, victims and their interaction) that serve to deny, downplay or justify sexual violence … " (Bohner et al., 2009, p. 19). Typically, rape myths are framed as cognitive schemas that act to guide the interpretation and organization of rape-related information, and consciously and/or unconsciously shape social evaluations and decision making processes in relation to sexual assault (Ryan, 2019). Common rape myths include the belief that victims cause the assault by their attire or behavior, that many women are inclined to lie about rape, and that rape happens because men cannot control their sexual desires. As these examples illustrate, much of the existing work on rape myths shows they are highly gendered, framing females as the victims of sexual assault and males as the perpetrators. Although this focus is partly justified by international crime and victimization statistics indicating this pattern (World Health Organization, 2002), there is increasing recognition that sexual assault can be committed by all genders against all genders (Rumney, 2007), and that myths can also exist in relation to this fact. However, work on such myths is less developed.
Over the past 40 years, research into rape myths and their determinants, correlates, and implications have been steadily accumulating. This evidence generally points to variations in RMA across age, gender, and educational level (where men, older people, and lower education relate to the higher endorsement of rape myths). In addition, RMA has been found to be positively correlated with a range of other social attitudes, such as gender role stereotyping, sexism, racism, and endorsement of interpersonal violence (Burt, 1980; Hockett et al., 2016; Lonsway & Fitzgerald, 1994; Suarez & Gadalla, 2010). Furthermore, individuals who endorse rape myths may act accordingly. For instance, research indicates that higher RMA is related to men’s proclivity to commit sexual violence (Yapp & Quayle, 2018), and victims' reluctance to report it (Egan & Wilson, 2012).
Rape Myths and Professional Practice
In addition to demonstrated relationships with individual demography and behavior, research also points to rape myths’ potential organizational and systemic implications. Of particular relevance for this article is evidence suggesting that these myths may have detrimental impacts on how rape complainants are treated within the medical and criminal justice systems, as professionals’ endorsement of rape myths may contribute to secondary victimization and impact the progression of rape cases through the justice system (Campbell, 2005; Maier, 2008). For example, while research generally points to low overall levels of RMA among medical students, some evidence indicates that trainee doctors with higher RMA display increased hesitancy in screening for patients’ sexual victimization history (Milone et al., 2010). Additionally, studies suggest that many sexual assault survivors are faced with victim-blaming questions by the personnel conducting forensic rape examinations and that these staff may fail to realize that their actions are distressing and can result in secondary victimization (Campbell, 2005; Campbell & Raja, 2005).
Within the legal system, there is also considerable evidence suggesting that rape myths are present and influential, despite generally low levels of acceptance (Gray & Horvath, 2018; Page, 2010; Sleath & Bull, 2017). Studies indicate that police officers with higher RMA show inferior interviewing skills, are less likely to believe rape complainants and are less prone to recommend charging the alleged offender (Goodman-Delahunty & Graham, 2011; Page, 2008; Rich & Seffrin, 2012). Furthermore, Shaw et al. (2017) show that rape myths are evident in official police records, suggesting that some officers “invoke traditional rape myths in documenting their investigations” (p. 602). Such myths have similarily been found to influence the prosecution and sentencing of rape cases in the courtroom (Bitsch & Klemetsen, 2017; Dinos et al., 2015; Temkin et al., 2018). Such evidence suggests that it is crucial to explore the extent and content of rape myths in professional groups likely to come into contact with rape survivors. Identifying and combatting these attitudes early in the career, when myths can more easily be targeted through education, may be particularly valuable.
Cultural Variations
To date, the vast majority of research into rape myths, including the development and application of measures, has been conducted in the United States, often using general college samples (Bohner et al., 2009). Yet, emerging evidence comparing American samples to those from other countries (Fakunmoju et al., 2020; Xue et al., 2016), as well as studies exploring cultural background in relation to RMA (Lee et al., 2005), points to variations in the level and types of rape myths endorsed. This highlights the importance of exploring rape myths in different cultures and national settings. In the Scandinavian context, despite high levels of gender equality (World Economic Forum, 2020), research suggests that some criminal justice professionals in Norway and Sweden also hold stereotypical beliefs about victims (Ask, 2010; Bendixen et al., 2014) and might be influenced by rape myths in their judgments about rape cases (Ask & Landström, 2010; Bitsch & Klemetsen, 2017; Bohner & Schapansky, 2018). However, there is relatively little Danish research on rape in general, and rape myths, in particular.
To the best of our knowledge, only one previous study has focused specifically on measuring Danish RMA, showing that a sample of Danish website visitors had more favorable attitudes toward rape victims than Singaporean, US male, and Australian student samples (Elklit, 2002). Two additional studies based on the review of police records found no indications of investigative biases based on rape stereotypes among Danish police (Hansen et al., 2019), and only minimal support for the notion of the “credible criminal” influencing charges and convictions of rape suspects (Nielsen et al., 2018). Although these studies provide a preliminary picture of the Danish landscape, there is a clear need for further investigations using additional samples and contemporary rape myth scales.
Measurement of RMA
Systematic investigations of rape myths require valid and reliable measures. Several standardized measures of RMA have been developed since the concept was first introduced (Burt, 1980; Feild, 1978; Ward, 1988), one of the most widely used of which is the IRMA scale developed by Payne et al. (1999).
In the decades since the development of the traditional RMA scales, increased attention to issues of sexual violence and greater public awareness regarding the social unacceptability of some of the included myths has led to suggestions that rape myths have become more subtle and covert and therefore more difficult to measure reliably with older scales (Gerger et al., 2007; McMahon & Farmer, 2011). In hopes of better capturing modern rape myths, McMahon and Farmer (2011) revised and validated an updated version of the IRMA, which is now most widely used. Whereas the original IRMA consisted of 40 statements (and five filler items) divided into seven subscales, McMahon and Farmer (2011) tested a 22-item version with four subscales, yielding 19 validated items organized into a five-factor second-order model. Myths that generally blame the victim for the assault due to her attire or behavior are captured by the “She asked for it” (SA) subscale, whereas the subscale “It wasn’t really rape” (NRR) includes items questioning whether it is rape if the victim doesn’t have bruises or physically resist the assault. Statements excusing men’s behavior due to uncontrollable sexual urges or alcohol are included in the “He didn’t mean to” (HDM) subscale and the second-order factor “He didn’t mean to (intoxication).” Finally, the subscale “She lied” (SL) expresses doubts about victims’ credibility and truthfulness. All items are rated on a 5-point Likert scale from 1 (strongly agree) to 5 (strongly disagree), with higher scores indicating greater rejection of rape myths. To the best of our knowledge, the original IRMA and its updated version are among the most reliable and psychometrically sound measures of RMA in use today (McMahon & Farmer, 2011).
The IRMA is also notable in that it has been translated and culturally adapted to a number of non-American contexts, including China (Xue et al., 2016), Norway (Bendixen & Kennair, 2017), Nigeria (Fakunmoju et al., 2018), and France (Trottier et al., 2020). These studies support either a five-factor (Trottier et al., 2020; Xue et al., 2016) or a four-factor (Bendixen & Kennair, 2017; Fakunmoju et al., 2018) structure, indicating that while some items and subscales are robust across cultures, the validity of others may be more specific to the social context and/or respondent group. This variation points to the need for additional country and sample-specific validations that are able to shed light on the specificity of RMA, while also allowing for the accumulation and comparison of knowledge generated using validated versions of the same scale. 1 To the best of our knowledge, there are no existing validations of the updated IRMA scale among trainee groups with responsibility for handling rape cases. In light of the literature reviewed above, exploring the validity of this scale in such respondent populations is another important step toward advancing knowledge regarding the scale’s applicability. In the Danish setting, a validated local measure that can capture modern RMA in different occupational groups is particularly needed, as such a measure will be critical to informing and evaluating ongoing political and practical efforts aimed at improving future rape victims’ contact with the medical and criminal justice systems.
Study Aims
The aims of the current study are three-fold. First, with a view to addressing some of the aforementioned gaps in the literature, we derive and test the factor structure of a Danish translation of the updated IRMA scale (McMahon & Farmer, 2011), using a sample of future law enforcement officers. Second, in order to test the robustness of the derived scale (hereafter referred to as IRMA-DK) and explore its psychometric properties in a different occupational group, we validate the scale using an independent sample of future medical professionals. Finally, with the aim of providing evidence to nuance current debate and policy efforts related to improving rape victims’ meetings with the medical and criminal justice systems, we use this measure to establish initial descriptive and comparative profiles of RMA in these two groups. The current study represents the first preliminary validation of a Danish measure of modern RMA.
Methods
Participants
We draw on two samples fielded as part of a larger randomized controlled trial (RCT) testing the effects of an e-learning module on sexual assault. The current study is based on data collected from control group participants between March 2018 and January 2019.
Sample 1 consists of 259 trainees from the Danish police academy who participated in the study in a class setting prior to the start of their normal teaching on sexual assault (95.5% estimated response rate based on course registration numbers). Four of these respondents had missing data for the rape myth measure and were therefore excluded from further analysis, yielding a final sample of 255. Respondents had an average age of 27.56 years (SD = 3.25). Consistent with the overrepresentation of male police trainees generally, the sample was heavily skewed with respect to gender, with 79% of respondents identifying as male, 20% identifying as female, and <1% reporting an “other” gender identity. 2 For the purposes of some analyses, the police trainee sample is randomly split into two halves (hereafter identified as samples 1A and 1B). These were tested for gender and age imbalance and showed none.
Sample 2 consists of 117 medical students from the three largest universities in Denmark who were invited to participate in the study during supplementary teaching offered in association with their core training in either gynecology or forensic medicine (63% estimated response rate based on attendance at the supplementary lectures). Three respondents with missing data on the rape myth measure were excluded from further analysis, rendering a final sample of 114 students with an average age of 26.15 years (SD = 2.39); 66.7% of respondents reported as female and 33.3% as male.
Due to the larger size and higher response rate in the police trainee group, this is treated as our primary sample for the initial validation, while the medical student sample is used to assess the robustness of the validated scale structure.
Although these samples were not initially recruited with the primary purpose of validating the IRMA measure, the data collected as part of a larger study exploring RMA in these groups provided a unique opportunity to conduct a preliminary validation using available data. Doing so provides novel insights regarding the applicability of the scale in these professional trainee groups. However, it is important to emphasize that because these samples are not representative of the general Danish population (e.g., both samples are skewed in terms of age and gender), we consider this a preliminary validation for the IRMA-DK for these specific professional groups. Additional samples would be required for a broader community validation. We return to this issue in the discussion.
Measures
Rape myth acceptance was measured using a Danish translation of McMahon and Farmer’s (2011) updated IRMA scale described earlier. Following previous research, all 22 initial items from the updated IRMA scale are included in our validation (rather than just the final 19 validated items) as other validation studies have found varying results regarding the additional three items (Bendixen & Kennair, 2017; Fakunmoju et al., 2018; Trottier et al., 2020). In order to ease interpretation, we employ a reversed 5-point scale, so that higher scores indicate greater RMA rather than greater rejection of rape myths (1 = strongly disagree to 5 = strongly agree). As in the original scale, both overall (average) index scores and subscale scores measuring specific domains of RMA are computed. Informed by existing guidelines and allowing for potential cultural adaptation of relevant items (Beaton et al., 2000), the scale was first translated to Danish by three independent translators, and subsequently back-translated by three additional translators. Agreement between translators was reached through several committee meetings. The original, translated, and back-translated items are provided in Appendix A.
Procedures
Participants were invited to participate following the distribution of written material 1–2 weeks prior to data collection and a short in-person introduction by a member of the project team. Students were informed that participation was voluntary and that responses were anonymous. No incentives or compensation were offered for participation. The study was reported to the regional ethics committee of Central Denmark prior to commencing data collection (inquiry 281/2017) and all participants provided informed consent. Data collection preceded formalized teaching on sexual assault. The RMA scale was administered through an online link as part of a larger web-based survey assessing knowledge and attitudes toward rape. The survey was completed individually in a classroom setting, via computer, tablet, or mobile phone. Following data collection, the participants were debriefed regarding the aims of the study and were given the opportunity to ask questions and reflect on their survey responses as a starting point for their subsequent teaching on sexual assault.
Analytic Strategy
We adopt a three-stage analytic approach. In order to address our first study aim, we first derive and test the factor structure of the IRMA-DK scale in a split sample of police recruits (samples 1A and 1B). Next, in order to address our second aim and explore the robustness of the scale validated in stage 1, we test the IRMA-DK structure and psychometric properties in an independent sample of medical students (sample 2). Finally, in order to address the third study aim of exploring potential group differences in RMA for these two occupational groups, we conduct a series of between-group comparisons, controlling for gender. Details of each analysis and their corresponding results are presented below.
Results
Stage 1: Deriving and Testing the IRMA-DK Scale in the Police Trainee Samples
The phase 1 validation of the IRMA-DK consists of two steps. In the first step, we carry out exploratory factor analysis (EFA) on sample 1A, in order to establish factor loadings for McMahon and Farmer’s (2011) original 22 IRMA items. Based on previous validations, we expect that not all original items will be adequately valid and reliable indicators for the RMA sub-dimensions they were initially designed to measure. The EFA allows us to investigate this empirically and identify a final set of items for the Danish validation. Next, using structural equation modeling, we run a confirmatory factor analysis (CFA) on sample 1B, in order to test the hypothesized scale structure developed in Step 1. Randomly partitioning the police sample in this way allows us to perform EFA on sample 1A without it affecting the validity of the CFA hypothesis tests in sample 1B. The EFA and CFA were run in Stata 16 software (StataCorp, 2019) using the “factor” and “SEM” packages, respectively. Due to violations of univariate and multivariate normality assumptions, we employ principal factor extraction for the EFA and robust maximum likelihood estimation (MLM) for the CFA, both of which are recommended for use with nonnormal distributions (Brown, 2015; Fabrigar & Wegener, 2012). 3
Exploratory Analyses
Descriptive statistics for the initial pool of 22 items are shown in Table 1, grouped according to the hypothesized structure of McMahon and Farmer’s (2011) updated IRMA scale.
Univariate Item Statistics for the Initial Pool of McMahon and Farmer’s (2011) 22 IRMA Items (Original English).
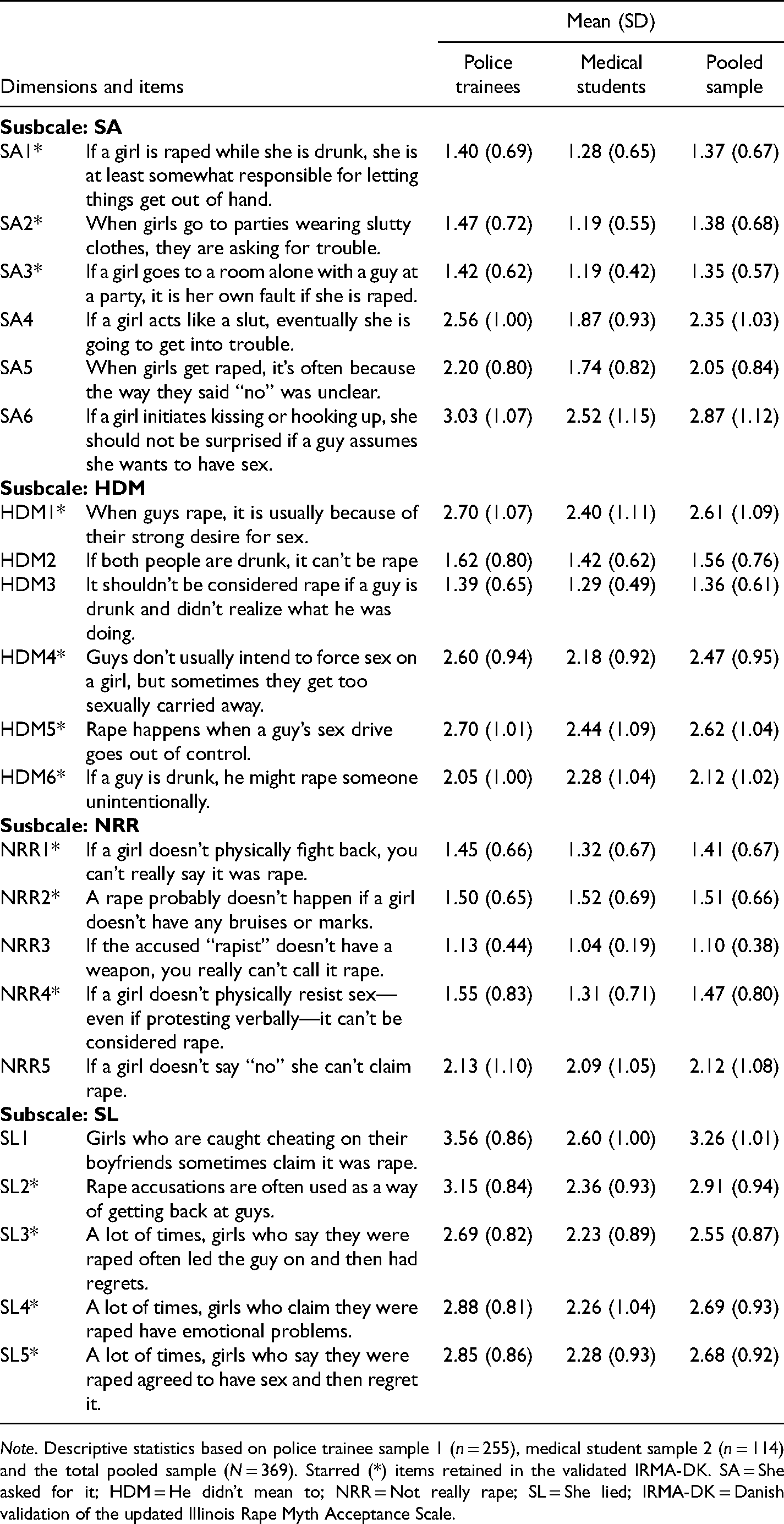
Note. Descriptive statistics based on police trainee sample 1 (n = 255), medical student sample 2 (n = 114) and the total pooled sample (N = 369). Starred (*) items retained in the validated IRMA-DK. SA = She asked for it; HDM = He didn’t mean to; NRR = Not really rape; SL = She lied; IRMA-DK = Danish validation of the updated Illinois Rape Myth Acceptance Scale.
EFA of the initial 22-item pool (principal factors; oblique-oblim rotation) yielded factor loadings consistent with the four dimensions “She asked for it”, “She lied”, “Not really rape”, and “He didn’t mean to” originally identified by McMahon and Farmer (2011) (see Appendix B). 4 An examination of the individual factor loadings for each item indicated that most had a conventionally strong (> 0.55) or acceptable loading (> 0.45) on their designated factor (Comrey & Lee, 1992), indicating sufficient convergent validity. However, seven items (SA4, SA5, SA6, HDM2, HDM3, NRR5, and SL1) fell below the 0.45 threshold and had uniqueness estimates > 0.70, indicating that a rather large share of their variation could not be accounted for by any of the factors. These items were thus dropped from the measurement model. In order to increase discriminant validity, one additional item (NRR3) with a factor loading of 0.46 and a secondary cross-loading of 0.26 was also removed.
A second EFA on the remaining 14 items (identified with stars in Table 1) indicated an improvement to the four-factor model, with 10 strong and four acceptable item loadings, the smallest being 0.48 (see Appendix C). On the basis of these results, the 14-item four-factor model was selected as the starting point for subsequent confirmatory analyses of the IRMA-DK scale. 5
Confirmatory Analyses
Table 2 reports the estimates from a Robust ML (MLM) CFA in the second half-sample of police trainees (sample 1B).
6
In order to evaluate model fit, we examined the inferential goodness-of-fit statistic
Estimates From Confirmatory Factor Analysis of the Final Four-Factor, 14-Item IRMA-DK Model in Police Trainee Sample 1B.
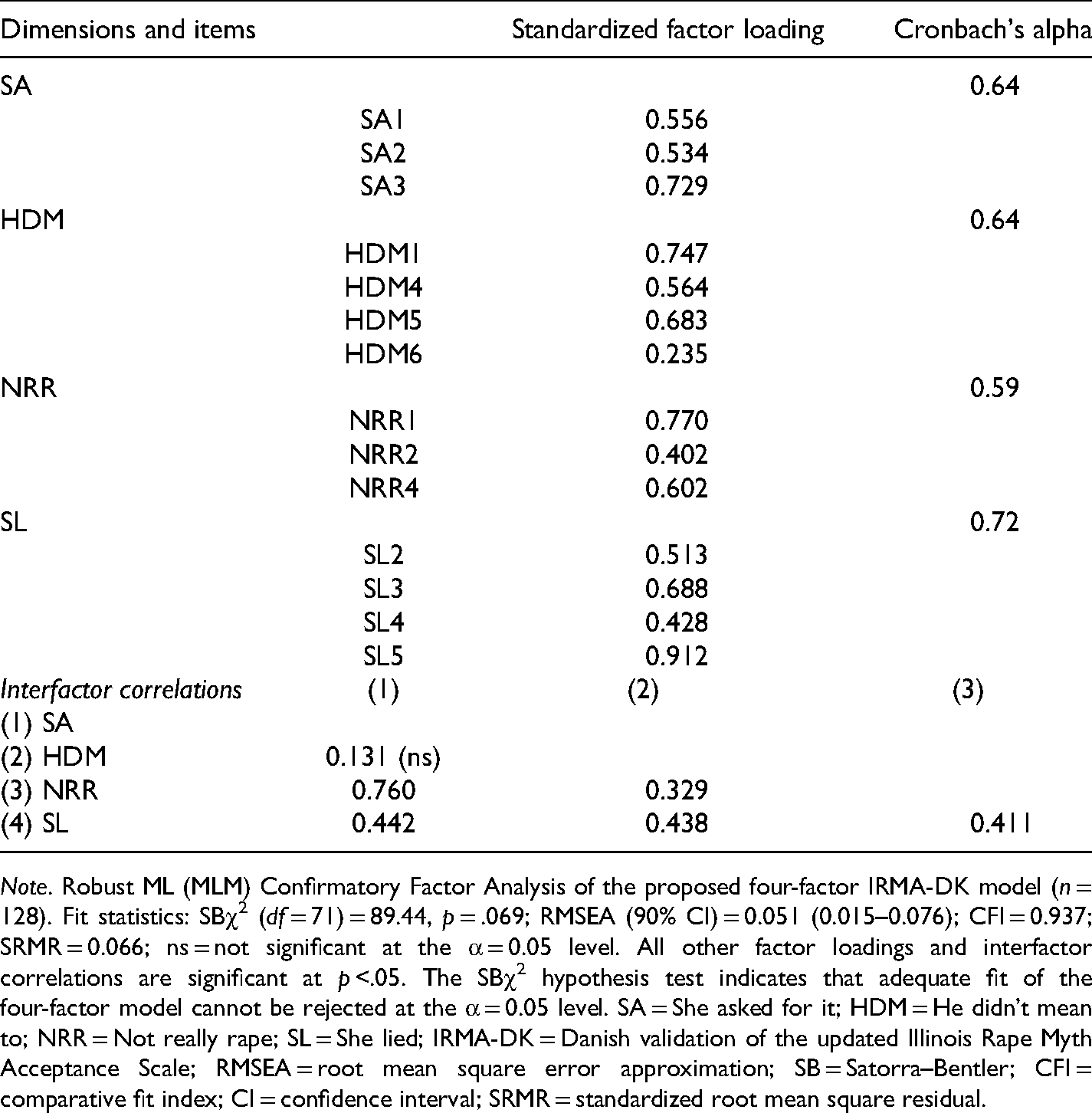
Note. Robust ML (MLM) Confirmatory Factor Analysis of the proposed four-factor IRMA-DK model (n = 128). Fit statistics: SBχ2 (df = 71) = 89.44, p = .069; RMSEA (90% CI) = 0.051 (0.015–0.076); CFI = 0.937; SRMR = 0.066; ns = not significant at the α = 0.05 level. All other factor loadings and interfactor correlations are significant at p <.05. The SBχ2 hypothesis test indicates that adequate fit of the four-factor model cannot be rejected at the α = 0.05 level. SA = She asked for it; HDM = He didn’t mean to; NRR = Not really rape; SL = She lied; IRMA-DK = Danish validation of the updated Illinois Rape Myth Acceptance Scale; RMSEA = root mean square error approximation; SB = Satorra–Bentler; CFI = comparative fit index; CI = confidence interval; SRMR = standardized root mean square residual.
To further assess the suitability of the four-factor model, we also ran supplementary analyses comparing the fit indices for this model against those of two alternative specifications: a one-factor model where all items load from the same underlying dimension, and a three-factor model in which the “She asked for it” and “Not really rape” dimensions are collapsed (due to their relatively high interfactor correlation). For both of the competing models the
Stage 2: Confirmation of the IRMA-DK Factor Structure in the Medical Student Sample
In order to test whether the IRMA-DK scale structure developed using the police sample could be confirmed in a different occupational trainee group, a final CFA was performed using the medical student sample (sample 2). As shown in Table 3, both inferential and descriptive indices again indicate an acceptable-to-good model fit (SB
Validation Sample: Estimates From Confirmatory Factor Analysis of the Final Four-Factor, 14-Item IRMA-DK Model in Medical Student Sample 2.
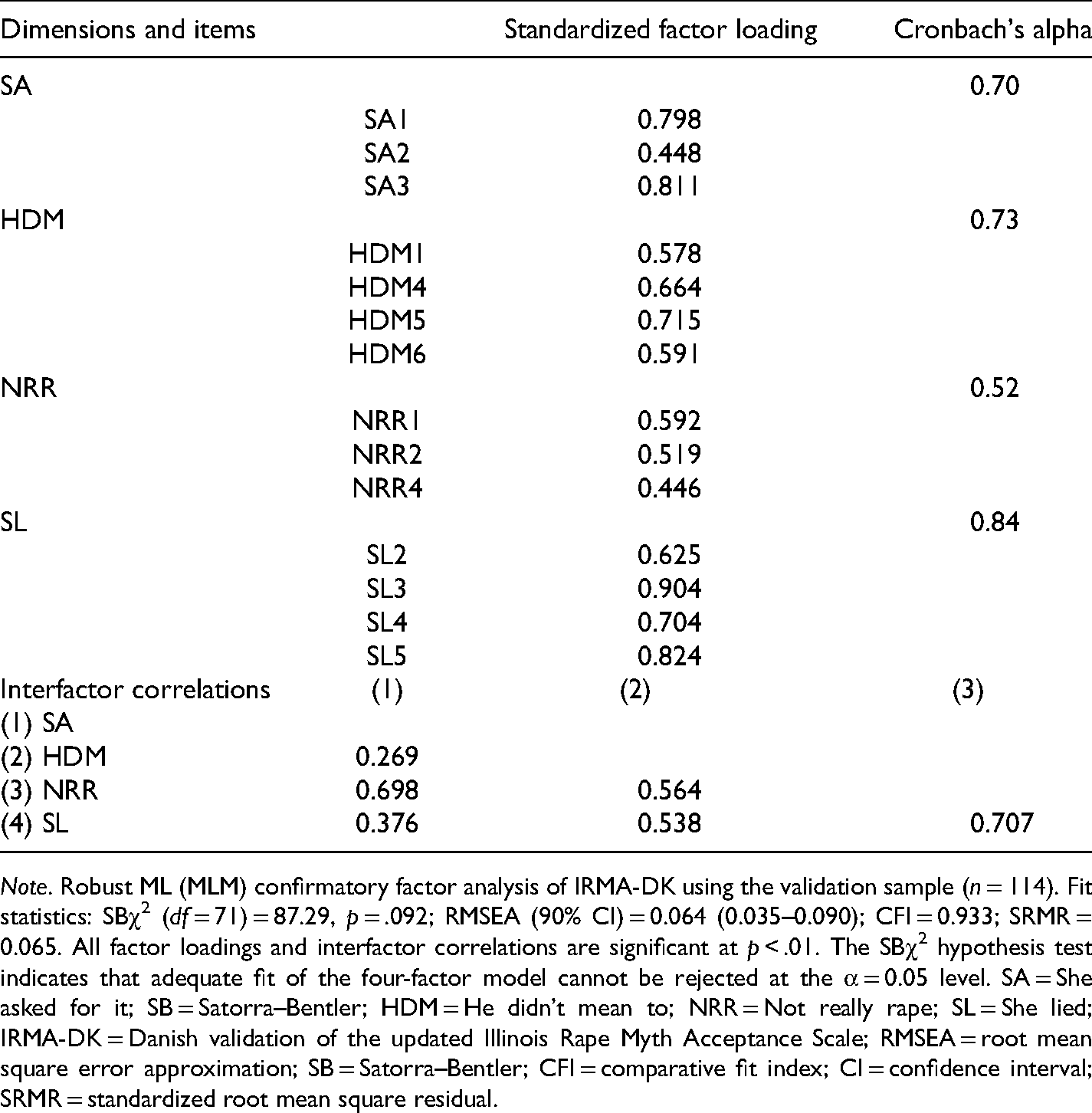
Note. Robust ML (MLM) confirmatory factor analysis of IRMA-DK using the validation sample (n = 114). Fit statistics: SBχ2 (df = 71) = 87.29, p = .092; RMSEA (90% CI) = 0.064 (0.035–0.090); CFI = 0.933; SRMR = 0.065. All factor loadings and interfactor correlations are significant at p < .01. The SBχ2 hypothesis test indicates that adequate fit of the four-factor model cannot be rejected at the α = 0.05 level. SA = She asked for it; SB = Satorra–Bentler; HDM = He didn’t mean to; NRR = Not really rape; SL = She lied; IRMA-DK = Danish validation of the updated Illinois Rape Myth Acceptance Scale; RMSEA = root mean square error approximation; SB = Satorra–Bentler; CFI = comparative fit index; CI = confidence interval; SRMR = standardized root mean square residual.
Taken together, the Stages 1 and 2 validation results outlined above suggest that the proposed 14-item IRMA-DK scale provides a valid preliminary measure of RMA for both police trainees and medical students. That being said, while the CFA on the medical student sample generally indicated solid convergent and discriminant validity, results from the police trainee sample suggest that there is room to improve the internal reliability of some subscales, and that the item “if a guy is drunk, he might rape someone unintentionally” may be a poor indicator of the “He didn’t Mean to” dimension.
Stage 3: Between-Group Differences in RMA
With a view to addressing our final study aim, in the third and last stage of the analysis, the 14-item validated scale was used to explore endorsement and between-group differences in RMA among police trainees and medical students. Mean differences in total and subscale scores are investigated using independent samples t tests with Bonferroni corrected p values run in IBM SPSS Statistics software version 25 (IBM Corporation, 2017). Due to previously established gender differences in RMA (Ryan, 2019) and considerable variation in the gender breakdown of our two occupational groups, any significant group differences are also explored using ordinary least squares (OLS) regression controlling for gender.
Descriptive analyses of total IRMA-DK scores showed relatively low levels of RMA among both police trainees (M = 2.17, SD = 0.41) and medical students (M = 1.87, SD = 0.48). 7 Although the average RMA score for the police trainees was significantly higher than that of the medical students (t [187,467] = 5.761, p < .001, d = 0.67), both groups generally disagreed with the included rape myths, with average total scores falling well below three on the 5-point scale. As illustrated in Figure 1, average scores for both groups also fell on the “disagree” side of the scale for all four subscales, with the lowest scores observed for the “She asked for it” dimension followed closely by “It wasn’t really rape.” Significant differences between the educational groups were nonetheless observed for two of the four subscales; namely, the “She asked for it” (t [258,540] = 4.003, p < .001, d = 0.44) and “She lied” (t [176,075] = 7.418, p < .001, d = 0.87) subscales. In line with previous studies (Sleath & Bull, 2015; Venema, 2018), myths relating to victim credibility, as captured by the subscale “She lied,” seem to be especially relevant for the police trainees.
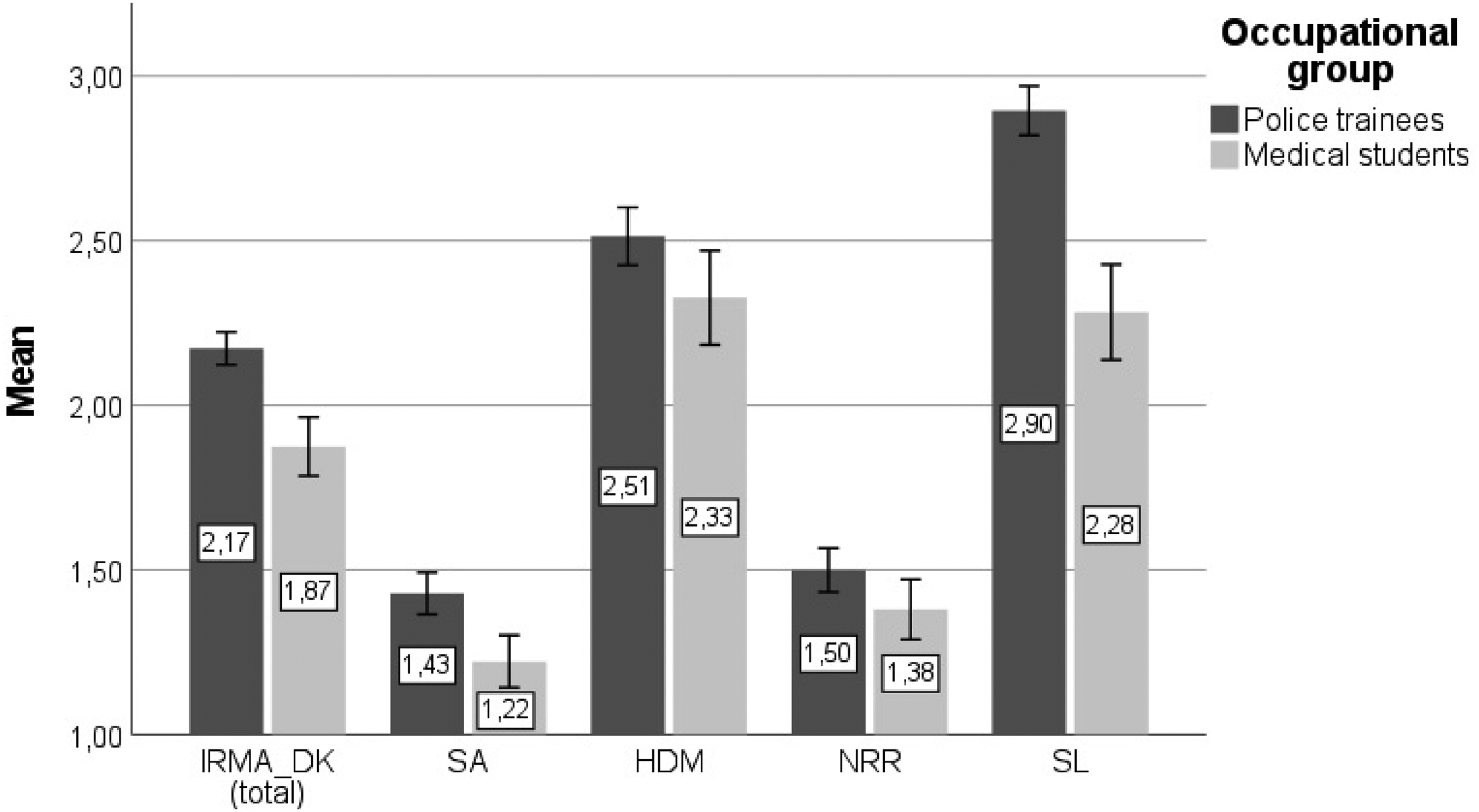
Total and subscale IRMA-DK scores for police trainees and medical students.
Looking at gender differences within the two groups, we unexpectedly observe no significant differences in average RMA for male and female police trainees (male M = 2.18, SD = 0.394 vs. female M = 2.13, SD = 0.436, t [252] = −0.729, p = .467, d = 0.11), or medical students (male M = 1.94, SD = 0.467, female M = 1.84, SD = 0.488, t [112] = −1.081, p = .282, d = 0.22). Although this finding is contrary to previously established gender differences in RMA, it might be in line with longstanding theories about occupational socialization processes that can act to eliminate or reduce gender differences (Gomez-Mejia, 1983). In order to explore this further, a hierarchical linear regression analysis was conducted, with gender as a predictor of RMA in the first step, and professional group added in the second step. The results of this analysis are presented in Table 4, and show that gender was a significant predictor of total IRMA-DK score in the first model, with men scoring higher than women. In model 2, professional group, but no longer gender, was a significant predictor, with medical students showing significantly lower RMA than police trainees when controlling for gender. This indicates that the previously established differences between the occupational groups were not due to differences in their gender distributions. Further regression analyses on the SA and SL subscales showed that all significant differences between medical students and police trainees persisted when controlling for the effects of gender. This suggests that occupational group may be a stronger predictor of RMA than gender.
Hierarchical Regression Analysis Predicting Total IRMA-DK Score.

Note. N = 369; R2 = 0.04 for Step 1; R2= 0.10 for Step 2. Bias corrected and accelerated CIs and standard errors based on 1,000 bootstrap samples. IRMA-DK = Danish validation of the updated Illinois Rape Myth Acceptance Scale; CI = confidence interval.
Discussion
Improved international understanding of the nature and scope of RMA among medical and criminal justice actors requires psychometrically sound local measures. Our results suggest that the 14-item IRMA-DK scale provides a valid and reliable measure of RMA among Danish police trainees and medical students. The four-factor measurement structure derived and tested in the police sample demonstrated acceptable-to-good model fit, satisfactory convergent and discriminant validity, and good internal consistency, albeit with possible room for improvement on some subscales. These findings were confirmed in an independent sample of medical students, where the measure demonstrated similar and even slightly improved psychometric properties.
The factor loadings of the retained IRMA-DK items are similar to those reported by McMahon and Farmer (2011), although the second-order factor of “He didn’t mean to—intoxication” could not be established in this sample. Other recent validation studies have similarly failed to identify this second-order factor (Bendixen & Kennair, 2017; Fakunmoju et al., 2018; Xue et al., 2016), indicating that it could be culturally or cohort specific.
Eight items from the original 22-item IRMA were removed during the validation process. These exclusions might point to outdated rape myths and highlight the dynamic nature of these beliefs, as well as the need to update RMA measures over time, especially in the post #MeToo era. Although a comprehensive comparison of the final item structure of other translated IRMA scales is beyond the scope of this article, it is worth noting that while previous validations have shown varying results regarding item composition (Bendixen & Kennair, 2017; Fakunmoju et al., 2018; Trottier et al., 2020), they generally share similar factor structures and good psychometric properties. Thus, while the individual versions may neither be exactly equivalent nor the results they produce directly comparable, they all contribute to the accumulation of knowledge about RMA as a universal concept manifested in diverse contexts.
In addition to contributing to a growing international literature on the measurement of RMA, the findings presented here also provide important new insights into the extent of RMA in two Danish trainee groups likely to have contact with rape victims. Consistent with previous research, both groups showed low average levels of RMA as measured by the IRMA-DK, thus generally disagreeing with the included myths (Milone et al., 2010; Sleath & Bull, 2017). Even so, a number of group differences were observed. Compared to medical students, the police trainees scored significantly higher on total IRMA-DK, and on the two subscales “She asked for it” and “She lied,” differences which persisted when controlling for gender. The between-group differences observed here might reflect underlying variations in the attitudinal profiles of individuals with different occupational preferences (those drawn to law enforcement vs. medicine) (Lippa, 2010). However, these differences (as well as the observed within-group gender similarities) could also be an expression of early occupational socialization (Gomez-Mejia, 1983). Although this cannot be determined in the current study, these findings highlight the need to consider the potential role of such processes as they relate to RMA in different trainee and professional groups.
With respect to the specific patterns of RMA observed in each group, police trainees scored highest on the rape myths related to victim credibility, captured by the “She lied” subscale, in accordance with previous research (Jordan, 2004; Page, 2010; Sleath & Bull, 2015; Venema, 2018). Although it can be argued that lie detection is an inherent part of police work (Docan-Morgan, 2007), creating special attention to potentially false statements, such results have also been interpreted as evidence of a general culture of skepticism in the treatment of rape victims within the criminal justice system (Jordan, 2004; Sleath & Bull, 2015). Even though our police trainees do not appear to endorse rape myths at a high level, special attention to myths expressing skepticism is warranted, especially in light of the previously mentioned report from the Danish police, showing that alarming numbers of rape complainants reported feeling that their reports were not taken seriously (Rigspolitiet, 2020).
Contrary to previous research (Sleath & Bull, 2015; Venema, 2018), both the police trainees and medical students reported the lowest acceptance of the subscale “She asked for it,” which could either indicate that these myths are not prevalent in the Danish context, or that widespread attention in the media and general discussions about rape, has rendered them especially prone to social desirability bias. As it was not possible to control for social desirability bias in this study, we cannot exclude the possibility that the low rates of agreement with some of the rape myths explored here could reflect socially desirable reporting. However, given that previous IRMA validations have shown that social desirability does not appear to predict rape stereotypes or impact the predictive value of RMA, this may not be a serious concern (Bendixen & Kennair, 2017). Future investigations may nonetheless benefit from the development of more implicit attitude measurements and the comparison of findings generated using different measurement approaches (Ryan, 2019).
Limitations
Although this study provides the most detailed information on Danish RMA in these professional groups to date, a number of limitations must also be recognized. Most notably, the cross-sectional nature of the research did not allow for examination of the test–retest reliability of the IRMA-DK scale for our samples, nor its predictive validity. Further, the confines of the RCT in which this validation study was embedded prevented us from exploring additional predictors of RMA and group differences including, for example, benevolent and hostile sexism, adversarial sexual beliefs, or ethnicity. This unfortunately excluded the possibility of exploring convergent validity, which should be a priority for future work aimed at further validating this measure.
Practical constraints at the educational institutions participating in the study also required different sampling procedures for the two occupational groups, which may have produced a sampling bias among the medical students, such that those with a particular interest in the topic and potentially more positive attitudes toward victims might have been more likely to attend the data collection sessions, as compared to both nonparticipating medical students and the police sample, who instead participated as part of their standard teaching activities. These potential selection issues should also be addressed in future studies using the IRMA-DK.
Another limitation concerns the trainee samples used. Although this validation has produced a measure suitable for use among future medical and criminal justice professionals (a highly relevant group for forward-looking efforts to improve rape victims’ contact with the system via education), the generalizability of the validated scale must still be demonstrated. The current study provides a first step toward developing a solid Danish measure of rape myths, but more work is needed. For example, future studies should endeavor to validate the scale in a more representative community sample. The generally low levels of RMA observed in both of the occupational groups explored here may or may not mirror patterns within a general community sample. Furthermore, future studies should test the scale structure among other professional trainee groups and especially among more senior and specialized medical and criminal justice professionals. This may be particularly relevant, given that occupational group predicted RMA in the current study.
Implications
Despite its limitations, the current study adds valuable knowledge to the growing body of literature indicating that cultural and linguistic adaptations of RMA measures are possible and valuable. It further highlights that while particular rape myths might be culturally or professionally specific and dynamic, the overall concept and dimensionality of rape myths seems to extend beyond cultures and languages. In the Danish context, this study provides a preliminary psychometric validation supporting the IRMA-DK as a valid and reliable measure of modern RMA for the professional groups explored. Furthermore, it is the first to map RMA in Danish trainee samples who will likely go on to interact with rape victims and shape their experiences with the medical and criminal justice systems. These findings offer crucial empirical evidence to nuance public debate regarding rape myths within the Danish criminal justice and medical systems, and the IRMA-DK provides a concrete tool that can be used to evaluate applied intervention efforts with these groups in the future. Although the generally low levels of RMA identified in this study is a comforting finding, the results still highlight the need for attention to specific myths and point to potential focus areas that can usefully be targeted for education and intervention. Our results also hint at potential differences in occupational culture and the importance of tailoring early training to address the specific stereotypical views of different professional groups. The hope is that this work will inspire future research aimed at confirming the validity of IRMA-DK in additional samples, at linking these attitudes to professional conduct and, ultimately, to informing intervention efforts aimed at improving rape victims’ meetings with the system.
Footnotes
Appendix A: Translated IRMA Items
Original English, Danish, and Back-translated Items From McMahon and Farmer’s (2011) Revised IRMA.
Appendix B: Exploratory Factor Analysis Using Sample 1A on Initial 22 items
Loadings From an Exploratory Factor Analysis (Principal Factors) of the Initial 22 McMahon and Farmer (2011) IRMA Items in Police Trainee Sample 1A.
Appendix C: Exploratory Factor Analysis Using Sample 1A on Final 14 items
Loadings From an Exploratory Factor Analysis (Principal Factors) of the Final 14 IRMA-DK Items in Police Trainee Sample 1A.
Appendix D: Fit Statistics of Final IRMA-DK
Fit Statistics for Confirmatory Factor Analyses of Final 14 IRMA-DK Items in Police Trainee Sample 1B.
Acknowledgment
The authors would like to thank the Center for Rape Victims at Aarhus University Hospital and the TrygFonden Centre for Child Research for their collaboration on this research, as well as the Danish police academy and the medical schools at Aarhus University, the University of Southern Denmark, and Copenhagen University for facilitating the data collection process.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by TrygFonden (grant number 113539).
Ethical Approval
This study was registered with the Central Denmark Regional Commitee for Health Research Ethics prior to commencing data collection (inquiry 281/2017). Following a concerete asessement, and in line with Danish law, the committee determined that a full ethical approval was not required. The research was conducted in full accordance with the Danish Code of Conduct for Research Integrity.
Informed Consent
All participants provided informed consent.