
Abstract
More knowledge is needed about the etiology and treatment needs of adolescent sex offenders. The current study compared adolescents who had offended against children (defined as below the age of 12 and at least 5 years younger than the adolescent), adolescents who have offended against peers or adults, and adolescents who had victims in both age groups. Based on Seto and Lalumière’s meta-analytic findings, participants were compared on theoretically derived factors, including childhood sexual abuse, atypical sexual interests, sexual experience, social competence, psychiatric history, and general delinquency factors (past criminal history, substance abuse history, and offense characteristics). The study sample consisted of 162 court-referred male adolescent sexual offenders aged 12 to 17 years. Of the six identified domains, groups significantly differed on five of them; the exceptions were variables reflecting social competence. The results further support the validity of distinguishing adolescent sex offenders by victim age.
Much of the research and clinical literature on sexual offending has focused on adults. However, adult models, assessment tools, and treatment approaches may not be applicable to adolescents. Adolescents account for 26% of all known sex offenders and 36% of sex offenders with child victims in the United States (U.S. Department of Justice, 2009). Self-report data also suggest substantial adolescent involvement in unreported sexual crimes (Zolondek, Abel, Northey, & Jordan, 2001). Less than half of adolescents who have sexually offended will reoffend in any way, with the average general recidivism rate being 43% (Caldwell, 2010). Fortunately, most adolescent sex offenders will not go on to sexually offend as adults; sexual recidivism rates for this population range from 2% to 20%, with an average sexual reoffending rate of 11% (Caldwell, 2002).
To better address sexual recidivism and gain a fuller perspective of sexual offending trajectories, it is necessary to first understand the causes of adolescent sexual offending (see Pullman & Seto, 2012; Seto & Lalumière, 2010). Can adolescent sexual offending be adequately explained by established models of adolescent delinquency from developmental criminology and psychology (see Ryan, Leversee, & Lane, 2010)? Or are adolescent sex offenders different from other adolescent offenders, requiring their own explanations? The generalist view is that adolescent sex offenders commit their crimes as part of a more general pattern of antisocial and criminal behavior (see France & Hudson, 1993). This view suggests that adolescent sex offenders are more similar to other adolescent offenders than they are different, and implies that they share risk factors such as antisocial personality traits, association with delinquent peers, and substance use, and thus would have similar clinical needs (see Quinsey, Skilling, Lalumière, & Craig, 2004).
In contrast, the specialist view suggests adolescent sex offenders differ from other adolescent offenders in theoretically meaningful ways, and thus require different explanatory models, assessment tools, and treatment approaches. Representing this view, the National Adolescent Perpetrator Network (1993), an organization of professionals working with adolescent sex offenders, concluded that “ . . . sexually abusive youth require a specialized response from the justice system which is different from other delinquent populations” (p. 86).
To test the generalist and specialist explanations, Seto and Lalumière (2010) conducted a meta-analysis of 59 studies comparing adolescent sex and non-sex offenders on theoretically important factors. The results suggested that there was likely a mixture of offender types in their sample, wherein some adolescent sex offenders were generalists and others were specialists. There were significant differences in some domains, as predicted by specialist explanations: sexual abuse history, atypical sexual interests, early exposure to sex or pornography, exposure to sexual violence. There was no support, however, for previously proposed explanations such as poor parent−child attachment, social incompetence, and offense-supportive attitudes and beliefs about women, children, or sex.
There were sufficient studies to consider the role of victim age for sexual abuse history and for antisocial tendencies, but not for the other domains in the Seto and Lalumière (2010) meta-analysis. Consistent with research on adult sexual offending, adolescents who had sexually offended against children were more likely to have sexual abuse histories and tended to score lower on measures of antisocial tendencies than adolescents who had sexually offended against peers or adults. We believe victim age likely moderated some of the observed similarities and differences between the adolescent sex offender and non-sex offender groups in the meta-analysis, based on previous research that has found that adolescents who sexually assault children present with different psychological profiles than those who assault peers or adult women (see van Wijk, van Horn, Bullens, Bijleveld, & Dereleijers, 2005).
Victim Age
Classification based on victim age is one of the most widely used methods to examine types of adolescents who sexually offend. This typology parallels the adult sex offender literature that distinguishes between rapists and child molesters (Fanniff & Kolko, 2012). This particular typology has been successful with both adult and adolescent samples of sex offenders, leading to the identification of key etiological factors, unique risks and needs for each subtype, and targeted prevention and treatment efforts (Fanniff & Kolko, 2012).
Adolescents who sexually offend against peers/adults do so within a broader propensity to violate the rights of others (Bullens, van Wijk, & Mali, 2006; Butler & Seto, 2002; Ronis & Borduin, 2007). Their sexually harmful behavior is enabled by their generally exploitative, coercive, and impulsive personalities (Witt, Jackson, & Hiscox, 2002). Adolescents with peer victims have been found to have longer arrest records and more extensive contact with the criminal justice system compared with those with child victims (Aebi, Vogt, Plattner, Steinhausen, & Bessler, 2012; Hunter, Figueredo, Malamuth, & Becker, 2003). Peer victimizers also tend to use more aggression and violence during the commission of their crimes and are more likely to be under the influence of drugs or alcohol compared with those who offend against children (Gunby & Woodhams, 2010; Hunter et al., 2003). Adolescents with peer victims are also more likely to commit a non-sexual crime in conjunction with their sexual offense (Hunter et al., 2003). These findings are consistent with the generalist perspective of sexual offending and suggest that general delinquency factors can also explain sexual offending against peers.
Conversely, adolescents who sexually offend against children consistently score lower on measures of delinquency compared with those who offend against peers/adults (Seto & Lalumière, 2010). Instead, these adolescents are more likely to exhibit internalizing problems. For example, Whitaker et al. (2008) found that adolescents with child victims had significantly higher rates of anxiety, depression, social deficits, and sexual problems compared with those with peer/adult victims. Gunby and Woodhams (2010) also found that adolescents with child victims experienced greater levels of social isolation, as evidenced by having fewer age appropriate friends, having lower self-esteem, and by having been frequently bullied. Although these results do not fully support a specialist explanation of sexual offending against children, by adolescents, they certainly move us away from a fully generalist perspective and provide a basis for further investigation.
The Current Study
The current study compared adolescents who sexually offended against children with adolescents who offended against peers or adults, to determine the extent to which these two victim age groups differ on theoretically important factors related to the generalist and specialist perspectives. There were too few offenders with only adult victims to further distinguish those who offend against peers or adults. Offenders with both child and peer/adult victims were examined separately as a third group of mixed victim offenders. Based on Seto and Lalumière’s (2010) findings, all three groups were compared on special explanation factors, specifically sexual abuse history, atypical sexual interest, and social competence. The groups were also compared on general delinquency factors. It was predicted that adolescents who offend against peers/adults would be more antisocial and delinquent than those who offend against children, who would in turn be more likely to have greater sexual abuse histories, atypical sexual interests, and social deficits. It was further predicted that mixed offenders will display a unique pattern of scores compared with the peer/adult and child victim groups.
Method
Participants
The study examined a Canadian sample of 162 male adolescent sex offenders aged 12 to 17 who were referred to a Family Court Clinic between 1988 and 2010 and who agreed to allow their clinical data to be used for research purposes. Three cases were removed from all analyses due to missing victim age information. The sample was divided into three groups: Participants who committed a sexual offense against a child, defined as below the age of 12 and at least 5 years younger than the offender, were assigned to the “Child Victim” group (n = 88). Participants who committed a sexual offense against a peer or adult were assigned to the “Peer/Adult Victim” group (n = 49). This group combined adolescents with peer victims and those with adult victims because only one participant had exclusively adult victims; the rest either had exclusively peer victims or a combination of both peer and adult victims. This grouping was also driven by the fact that peer victims and adult victims both show signs of sexual maturation, unlike most child victims. Any participant who offended against both a child and a peer/adult was assigned to the “Mixed Victim” group (n = 22).
The mean age of the total sample was 15.2 years (SD = 1.3) and the mean education level for the total sample, as measured by their highest grade completed, was 8.8 (SD = 1.2). The mean age and education did not significantly differ across groups, F(2,146) = 0.84, p = .53, and F(2,146) = .62, p = .54, respectively.
The sexual offending characteristics of the sample are described in Table 1. These include the total number of victims, the mean age of victims, whether the offender ever had a male victim and whether the offender ever had an unrelated victim. The mixed victim group was significantly more likely to have ever offended against a male, χ2(1, n = 71) = 27.33, p ≤ .001, compared with the child or peer/adult victim groups. The child victim group was significantly less likely to have an unrelated victim compared with the peer/adult and mixed victim groups, χ2(1, n = 157) = 14.35, p ≤ .001.
Frequencies and Omnibus Chi-Squared Tests of Sexual Offense Characteristics.

Note. Group values with different subscripts are significantly different from each other.
Measures
A coding form was developed based on the type of information typically available in the clinical files. Files usually included mental health assessments, a summary of the youth’s criminal history, and other collateral information (i.e., parent interviews, teacher reports, child protection assessments). The complete coding form includes a large variety of clinical variables, covering multiple domains; however, only the domains relevant to our study hypotheses are outlined below. All of the study variables were based on self-report plus any available collateral information (e.g., abuse history might be mentioned by the youth, their parent, or noted in previous assessment reports).
Abuse history
This domain includes a history of sexual, physical, and/or emotional abuse. Variables coded include the offender’s age at the time of the abuse, the relationship between the abuser and victim, and the number of abusive incidents that occurred. Sexual abuse included any contact between the adolescent if he was under the legal age of consent and an adult. It also included any sexual behavior that was clearly coercive or violent committed by a same-aged peer or older sibling.
Sexual history
The variables included under this domain include the youth’s sexual orientation, age of onset of puberty, and whether the youth ever experienced consenting sexual intercourse with a similar-aged partner. In addition, information regarding the age the offender first learned about sex and mainstream pornography use was also collected.
Atypical sexual interests
Atypical sexual interests incorporate a range of unconventional sexual interests and behaviors, particularly those involving prepubertal children, coercive sex, or inflicting physical pain or suffering. The variables used to assess the presence of atypical sexual interests include the use of atypical pornography (e.g., child, coercive sex, bestiality) and disclosure of atypical sexual fantasies. In addition, adolescents underwent phallometric testing where changes in penile circumference were measured in response to sexually explicit audio and visual stimuli.
The specific phallometric testing procedures used with adolescents are the same as those used with adult sex offenders (for a detailed description, see Kingston, Seto, Firestone, & Bradford, 2010). Prior to the year 2000, phallometric testing was done on all adolescent sex offenders. Post-2000, several exclusion guidelines were introduced: (a) adolescents 16 years or younger (unless there was a history of repeated sexual offenses, for example, repeated molestation of prepubescent child or sexual offenses against multiple victims); (b) adolescents with cognitive impairment and/or developmental delay, regardless of their age; and (c) if the sexual offense occurred during the course of a major mental illness (e.g., bipolar episode). However, these guidelines were not always followed, for example, if phallometric testing was specifically requested by the court or by legal counsel. There was no difference in the year of assessment or the proportion of participants with missing data across the three adolescent groups, suggesting there was no confound between group and availability of phallometric test results.
In cases where phallometric testing was done, the specific stimuli used were determined by the adolescent’s physician. Generally, these included slides (i.e., male and female nudes differing in age) and non-violent audiotapes (i.e., non-physical coercion, child-initiated sex). Relative responses were calculated using ratios; cutoff scores greater than 1 on a Pedophilia Index (arousal to children relative to adults) and Rape Index (arousal to depictions of coerced sex relative to consenting sex) were used to make a clinical opinion about whether the adolescent showed a problematic sexual arousal pattern.
The variable “any psychosexual disorder label” (n = 48) is also included under the atypical sexual interest domain. This construct reflects diagnostic labels related to any atypical sexual interest that were given at the time of assessment. It includes labels of possible pedophilia (n = 29), possible sexual sadism (n = 3), and psychosexual problem not otherwise specified (n = 16). It is important to note that pedophilia cannot be diagnosed in individuals under the age of 16 (Diagnostic and Statistical Manual of Mental Disorders [4th ed., text rev.; DSM-IV-TR]; American Psychiatric Association [APA], 2000) and is being used in this context primarily as a descriptive label assigned by clinicians. Therefore, the psychosexual disorder variable is not independent of other variables as it was informed by sexual victim characteristics and phallometric test results (see Seto, Murphy, Page, & Ennis, 2003).
Social competence
Social competence is defined as an individual’s ability to successfully interact with members of their social network, including potential sexual and romantic partners. Variables coded in this domain include the presence of close friendships, if they have ever had a girlfriend/boyfriend, social isolation, loneliness, difficulty socializing in general, and difficulty initiating relationships with members of the opposite sex. Of the six variables listed, “difficulty initiating relationships with members of the opposite sex” could be less applicable to non-heterosexual respondents. However, the majority of participants (93%) identified females as their preferred gender, so this item bias did not have a major impact on the results.
Psychiatric history
Psychiatric history refers to any contact with mental health services prior to the commission of the index offense. Variables included in this domain include previous psychiatric assessment, psychiatric hospitalization, any DSM-IV-TR diagnosis, a diagnosis of attention deficit hyperactive disorder (ADHD), and a diagnosis of conduct disorder (CD; APA, 2000).
Psychiatric diagnoses reflecting severe externalizing behavior problems given at the time of the assessment, after the commission of the index offense, were collapsed into one variable: disruptive behavior disorders. This variable included oppositional defiant disorder (ODD; n = 5), conduct disorder (n = 44), and antisocial personality traits (n = 6). Antisocial personality disorder (ASPD) cannot be diagnosed in individuals under the age of 18 according to the DSM, but the antisocial personality traits label was assigned by clinicians and reflected ASPD symptoms and a severe form of conduct disorder
Delinquency indicators and criminal history
General delinquency includes antisocial traits and behaviors that are strongly correlated with each other and are predictive of future criminality (Quinsey et al., 2004). Delinquency indicators included early conduct problems, truancy, history of cruelty to animals, and general alcohol and drug use. Criminal history was also coded using number of previous non-sexual offenses (non-violent or violent) and number of previous sexual offenses. Index offense characteristics were also used to assess general delinquency. These included whether the offense was planned, if it was committed under the influence of drugs or alcohol, and whether a weapon was used. The extent of physical injury (mild, moderate, or severe) inflicted upon the victim was also coded.
Procedure
All participants underwent a mental health evaluation through a Family Court Clinic and a sexological assessment conducted through a Sexual Behavior Clinic. Informed consent to use the clinical information for research purposes was obtained at that time. The consent procedure was opt-in; only adolescents who gave consent and had been referred to the clinic after committing a sexual offense against either a child or peer/adult were included in the study. It is impossible to establish how many adolescents who presented for assessment declined to be included, as we had no permission to look at their files. No other exclusion criteria were used.
Ethics approval was obtained for a retrospective review of all eligible files. The archival clinical data were coded and inputted into an electronic database. No participants were contacted during the course of this study.
Inter-rater reliability of our coding was calculated for all variables using 10 of the clinical files. Some variables were modified or dropped from the analysis due to low inter-rater reliabilities. Self-reported criminal offenses were removed from past offense history to increase the reliability of the criminal history variables, evidence of early conduct problems was dichotomized as absent or present, and social isolation and difficulty socializing with members of the opposite sex were excluded from the analyses. After these changes, agreement ranged from 70% to 100% for all variables. Cohen’s kappa coefficient was also calculated, with values ranging from 0.58 to 1.0, indicating adequate to excellent inter-rater reliability (Landis & Koch, 1977).
Results
The three groups were compared on all domains using chi-square analysis or one-way ANOVA. Omnibus chi-square tests were performed and if there was a significant difference, planned comparisons were conducted to determine which offender groups were driving these observed differences. Planned comparisons were as follows: (a) child victim versus any peer or adult victim (peer/adult victim and mixed victim combined) and (b) peer/adult victim versus mixed victim. Effect sizes were calculated for categorical variables using Cramer’s V (ϕ
c
). All significant coefficients fell between .20 and .38 indicating small to moderate effect sizes (Cohen, 1988). Effect sizes for continuous variables are also reported using partial eta-squared values (
Abuse History
Rates of sexual, physical, and emotional abuse were compared across the three groups (Table 2). A significant difference was found for sexual abuse, and sub-group comparisons showed that the mixed victim group was sexually abused at a significantly higher rate compared with both the child and peer/adult victim groups, χ2(1, n = 71) = 3.77, p = .05. Physical abuse rates were similar across the groups. However, the trend was consistent with past findings (e.g, Worling, 1995b) because the peer/adult victim group had the highest rate of physical abuse (44.9%). No significant difference was found across groups in emotional abuse history. While the mixed victim group had the highest rate of sexual abuse (63.6%), they also had the lowest rate of emotional abuse (13.6%).
Frequencies and Omnibus Chi-Squared Tests of Abuse History, Sexual History, and Atypical Sexual Interest Variables.
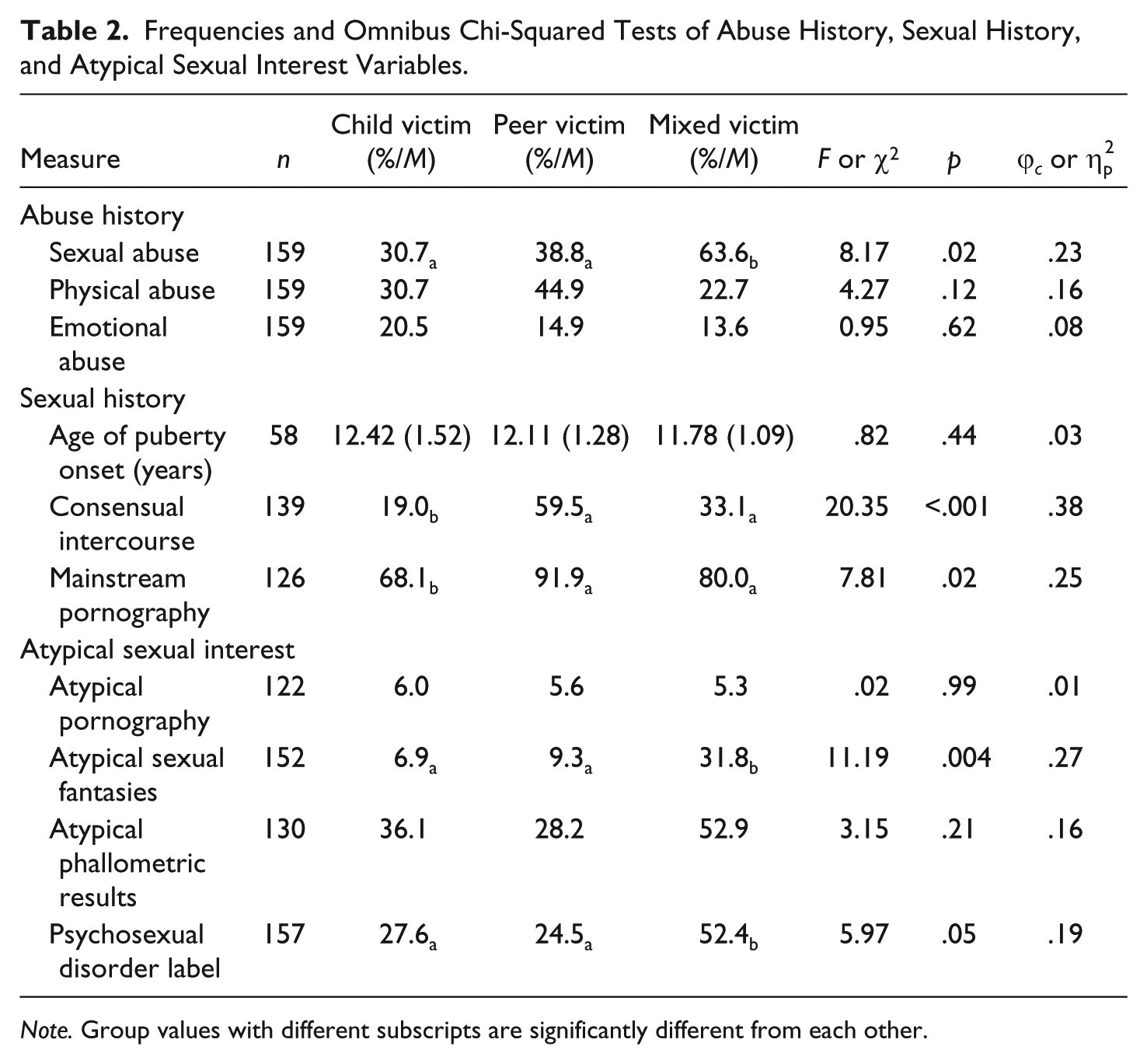
Note. Group values with different subscripts are significantly different from each other.
Sexual History
Sexual history comparisons are summarized in Table 2. The age of onset of puberty was not significantly different across groups. However, groups did significantly differ in terms of engaging in consensual intercourse and mainstream pornography use. The child victim group was significantly less likely than the peer/adult victim and mixed victim groups to have ever been exposed to mainstream pornography, χ2(1, n = 126) = 6.77, p = .009, or to have ever had consenting sexual intercourse, χ2(1, n = 139) = 16.45, p < .001.
Atypical Sexual Interest
Four variables contributed to the atypical sexual interest domain (Table 2). No significant difference was found across groups for atypical pornography use; however, this was likely due to the low rates of exposure to this type of content. There was also no significant difference across groups for atypical phallometric results. Significant differences were found across groups for both atypical sexual fantasies and psychosexual disorder labels. Sub-group comparisons for atypical sexual fantasies showed that the mixed victim group was significantly more likely to endorse having these types of fantasies compared with the child or peer/adult victim groups, χ2(1, n = 65) = 5.25, p = .022. Similarly, the mixed victim group was also significantly more likely to have been given a psychosexual disorder label at the time of assessment compared with the child or peer/adult victim groups, χ2(1, n = 70) = 4.36, p = .037.
Social Competence
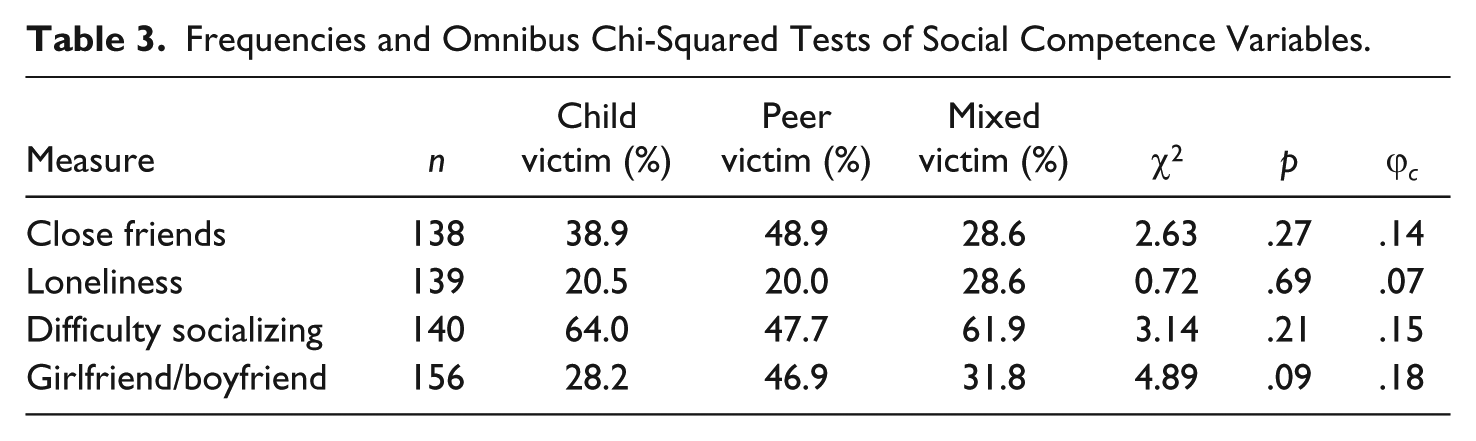
Four variables contributed to the social competence domain, including having close friends, reports of loneliness and difficulty socializing, and ever having a girlfriend/boyfriend. There were no significant differences across the three victim age groups on any variables in this domain (Table 3).
Frequencies and Omnibus Chi-Squared Tests of Social Competence Variables.
Psychiatric History
Out of the five variables that contributed to the psychiatric history domain, three were significantly different across groups: psychiatric hospitalization, ADHD diagnosis, conduct disorder diagnosis (Table 4). Most of these differences were driven by the child victim group: The child victim group was significantly less likely, compared with the peer/adult or mixed victim groups, to have ever been psychiatrically hospitalized, χ2(1, n = 159) = 15.65, p < .001. In addition, the child victim group was also significantly less likely to have ever been diagnosed with conduct disorder, χ2(1, n = 159) = 10.53, p = .001. Conversely, the significant difference found for ADHD diagnosis was driven by the mixed victim group. The mixed victim group was significantly more likely to have been given an ADHD diagnosis, χ2(1, n = 71) = 5.97, p = .015, compared with the child and peer/adult victim groups.
Frequencies and Omnibus Chi-Squared Tests of Psychiatric History Variables and Diagnoses at the Time of Assessment.
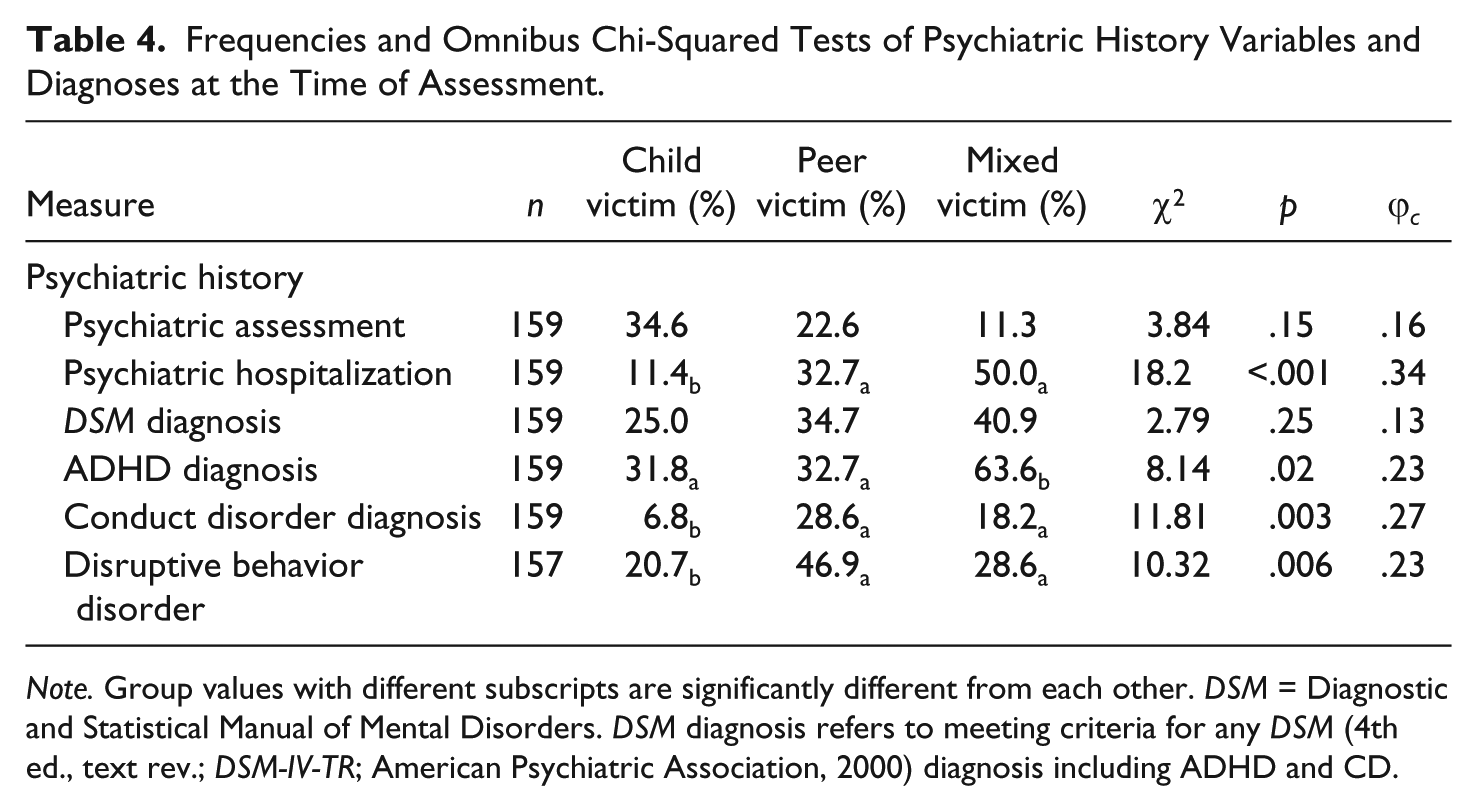
Note. Group values with different subscripts are significantly different from each other. DSM = Diagnostic and Statistical Manual of Mental Disorders. DSM diagnosis refers to meeting criteria for any DSM (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000) diagnosis including ADHD and CD.
Rates of disruptive behavior disorders were also compared across groups (Table 4). This refers to any diagnosis of ODD, CD, or antisocial personality traits made after the commission of the index offense. A significant difference was found across groups with the child victim group being significantly less likely than the peer/adult and mixed victim groups to have been diagnosed with any disruptive behavior disorder, χ2(1, n = 157) = 7.95, p = .005.
Delinquency Indicators and Criminal History
Significant differences across groups were found for all delinquency indicators (Table 5). Groups also significantly differed on two of the index offense characteristic variables. The peer/adult group was significantly more likely to commit the index offense under the influence of alcohol or drugs, χ2(1, n = 68) = 5.09, p = .024, compared with the child and mixed victim groups. The child victim group was significantly less likely than the peer/adult and mixed victim groups to cause any physical injury to their victims, χ2(2, n = 151) = 15.54, p < .001.
Frequencies and Omnibus Chi-Squared Tests of Delinquency Indicators, Criminal History, and Index Offense Characteristics.

Note. Group values with different subscripts are significantly different from each other.
Significant differences were also found when comparing criminal history across groups (Table 5). All of these differences were driven by the child victim group, who consistently had significantly fewer criminal charges compared with the peer/adult or mixed victim groups. No significant difference was found across groups for the number of previous sexual charges; however, this is likely because of the low base rate of prior sexual offending in samples of adolescent sex offenders (Caldwell, 2010).
Supplementary Analyses
Supplementary analyses were conducted to compare the mixed victim group with the child and peer/adult groups after taking victim number into account. By definition, an adolescent in the mixed victim age group had to have at least two victims, whereas adolescents in the child or peer/adult victim groups could have a single victim. Thus, some of the differences between the mixed victim group and other groups might be attributable to the fact that the mixed victim group offenders had more victims, rather than victims of different age categories. Because our variables were categorical, victim number could not be simply statistically covaried in our analyses.
This exclusion criterion led to a substantial decrease in sample size as only 45% of the sample had two or more sexual victims (n = 73). It is therefore not surprising that most comparisons were not statistically significant. The important thing to note, however, is that the pattern of results was largely similar. The mixed victim group still tended to have the highest rates of sexual abuse (63.4%) compared with the child victim (48.5%) and peer/adult victim (50.0%) groups. The child victim group also continued to have less experience engaging in consensual sexual intercourse and less exposure to mainstream pornography compared with the peer/adult victim and mixed victim groups. Similarly, the child victim group continued to have fewer criminal charges compared with the peer/adult victim and mixed victim groups, the latter two groups being quite similar to each other.
Overall, there was only one major difference in the supplementary analysis. Once the number of victims was controlled for by removing all single victim offenders, the child victim group tended to have higher rates of psychosexual disorder labels given at the time of assessment compared with the peer/adult victim and mixed victim groups (45.1% vs. 25.4% and 29.6%). The child victim group also tended to be more likely to exhibit atypical phallometric results compared with the other two groups (43.4% vs. 24.5% and 32.1%). These results suggest that the mixed victim group looked more sexually atypical because they had more sexual victims, on average, rather than the fact they had mixed victim ages.
Discussion
The current study further supports the validity of distinguishing adolescent sex offenders by victim age. Results partially support the hypothesis that adolescent sexual offending against children is better explained by special explanation factors rather than general delinquency factors. Consistent with our prediction, offenders with child victims were less sexually experienced than offenders with any peer or adult victims. This was not a function of age or opportunity, because all groups had similar mean ages. Instead, this result suggests that compared with adolescents who offend against peers, those who offend against children are more likely to do so because they lack the sexual and social maturity to form intimate relationships with peers.
Other adolescents, however, may not be interested in intimate relationships with peers. Offenders with child victims tended to be the most sexually atypical, as a group, compared with the other victim age groups. This is demonstrated by the child victim group having the highest rates of atypical phallometric results, and psychosexual disorder labels given at the time of assessment after controlling for number of victims. Additional comparisons revealed that the child victim group consistently scored lower on all measures of general delinquency indicators compared with the peer/adult victim groups. This is consistent with Seto and Lalumière’s (2010) meta-analysis, which found that adolescents with child victims scored lower on delinquency risk variables. These results also support arguments made within the adolescent offender literature that the behaviors of adolescents who sexually offend against children cannot be simply explained as a manifestation of general delinquency tendencies.
Results were more consistent with the general delinquency explanation for adolescents who sexually offend against peers or adults. Offenders with peer/adult victims inflicted more physical harm upon their victims and were the most likely to be under the influence of substances at the time of the offense. These results are consistent with previous studies by Hunter et al. (2003) and Gunby and Woodhams (2010), who also found that adolescents who sexually victimized peers were more aggressive and more likely to be under the influence of substances during the sexual offense. Offenders with peer/adult victims had the most severe behavioral problems, evidenced by higher rates of general substance use, higher rates of conduct disorder prior to the index offense, and higher rates of any disruptive behavior disorder at the time of assessment. These findings are consistent with other research examining adolescents who have offended against peers/adults. For example, Whitaker et al. (2008) found adolescents with peer victims exhibited more externalizing problems than those with child victims.
Mixed Victim Age Group
Adolescents with both child and peer/adult victims displayed a different pattern of scores, suggesting they are indeed a distinct group of offenders. Compared with the other two groups, adolescents with both victim types were significantly more likely to have been sexually abused and to endorse having atypical sexual fantasies. The mixed victim group was similar to offenders with only peer/adult victims in terms of sexual history by having higher rates of exposure to mainstream pornography and higher rates of previous intercourse compared with the child victim group. They also matched the peer/adult victim group on delinquency indicators such as truancy, use of physical violence during the offense and all measures of past criminal history, and on psychiatric history variables such as previous psychiatric hospitalization and conduct disorder diagnosis. The mixed victim group also had significantly higher rates of ADHD diagnosis and cruelty to animals compared with both the child victim and peer/adult victim groups. The pattern of results remained similar after controlling for victim number.
Taken together, these results suggest that both general delinquency and special explanation factors contribute to the onset of this mixed victim age type of sexual offending. It further implies that adolescents with both victim age types have the most treatment needs. These speculations are tempered by the small number of mixed offenders in this study. These results are a first step in filling the large knowledge gap regarding this group of adolescent sex offenders.
Limitations
As with most offender research, there is a sampling bias when recruiting participants from a criminal justice institution. In regard to the current study, it is possible that only adolescents with relatively severe sexual behavior problems were referred to the Family Court Clinic, whereas those with less severe problems were referred elsewhere or not sent for mental health evaluations.
We conducted our analyses only on variables that were coded with acceptable inter-rater reliability. We do not know, however, the inter-rater reliability and validity of clinical judgments in the files, such as psychiatric diagnosis. Low reliability or validity would constrain our ability to detect significant differences between the victim age groups. There was also a potential confound with our phallometric testing variable; only some adolescents were assessed phallometrically after a change in clinic guidelines in 2000 (those with repeated sexual offenses, multiple victims, or by request of the referral source), whereas all adolescents who were willing underwent testing prior to 2000. This confound would affect the psychosexual disorder label variable as well because phallometric testing results were incorporated in consideration of these labels. However, the groups did not differ in terms of missing phallometric data or average year of phallometric assessment, suggesting this confound did not have a major impact.
Another limitation was the sample size. We addressed the potential confound of victim number by comparing mixed victim age offenders with offenders who had at least two child victims or at least two peer or adult victims. The resulting comparisons did not have sufficient statistical power to detect differences that the unadjusted analysis suggested, though the pattern of results was similar. Replication of this research using larger victim age groups would illuminate group differences without the confound of victim number.
Last, we did not control for multiple comparisons. We note, however, that many of the significant differences were significant at a p value less than .005, and we were particularly interested in the pattern of results, which were generally consistent with our hypotheses and with past research.
Future Directions
We believe this study extends the argument made by Seto and Lalumière (2010) that research and practice with adolescents who sexually offend should consider victim age. Victim gender would also be an important consideration. Victim age and gender are often confounded, with child victim groups offending against both males and females and peer/adult victim groups mostly offending against females (Worling, 1995a). Mixed victim offenders fall somewhere in the middle in terms of victim gender composition.
Future research could also examine the extent of victim age (or gender) cross-over. Vess and Skelton (2010), for example, found that 17% of their sample of adult sex offenders against children had reoffended against an adult victim, whereas 37% of offenders against adults reoffended against children. Though the sexual recidivism rates of adolescent sex offenders are low, some adolescents do reoffend, either as adolescents or as adults (Caldwell, 2010). Knowing the extent of victim age and gender cross-over in large samples of adolescents who sexually offend could shed needed light on questions about etiology, risk assessment, and intervention. For example, adolescent and adult sex offenders with child victims are often prohibited from having unsupervised contacts with children while under supervision. Identifying the correlates of victim age cross-over might indicate that similar prohibitions are warranted for some offenders with only peer or adult victims.
The current results may also contribute to future studies examining adolescent trajectories of sexual offending into adulthood. Recent findings suggest that victim age is related to recidivism risk among adolescents and may moderate whether an offender will continue to offend post-adolescence (Hendriks & Bijleveld, 2008; van den Berg, Bijleveld, & Hendriks, 2011). For example, Lussier, van den Berg, Bijleveld, and Hendriks (2012) found that adolescents with child victims were more likely to be adolescent-limited offenders whereas adolescents with peer victims were more likely to reoffend as adults. They also found that factors related to the generalist explanation of sexual offending, including school failure and involvement with delinquent peers, increase the odds of an adolescent becoming a stable, high-rate offender. Understanding the interplay between victim age and recidivism may help direct future interventions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.